
Full Regression of Peyronie’s Disease Plaque Following Combined Antioxidant Treatment: A Three-Case Report


Abstract
:1. Introduction
2. Case Presentations
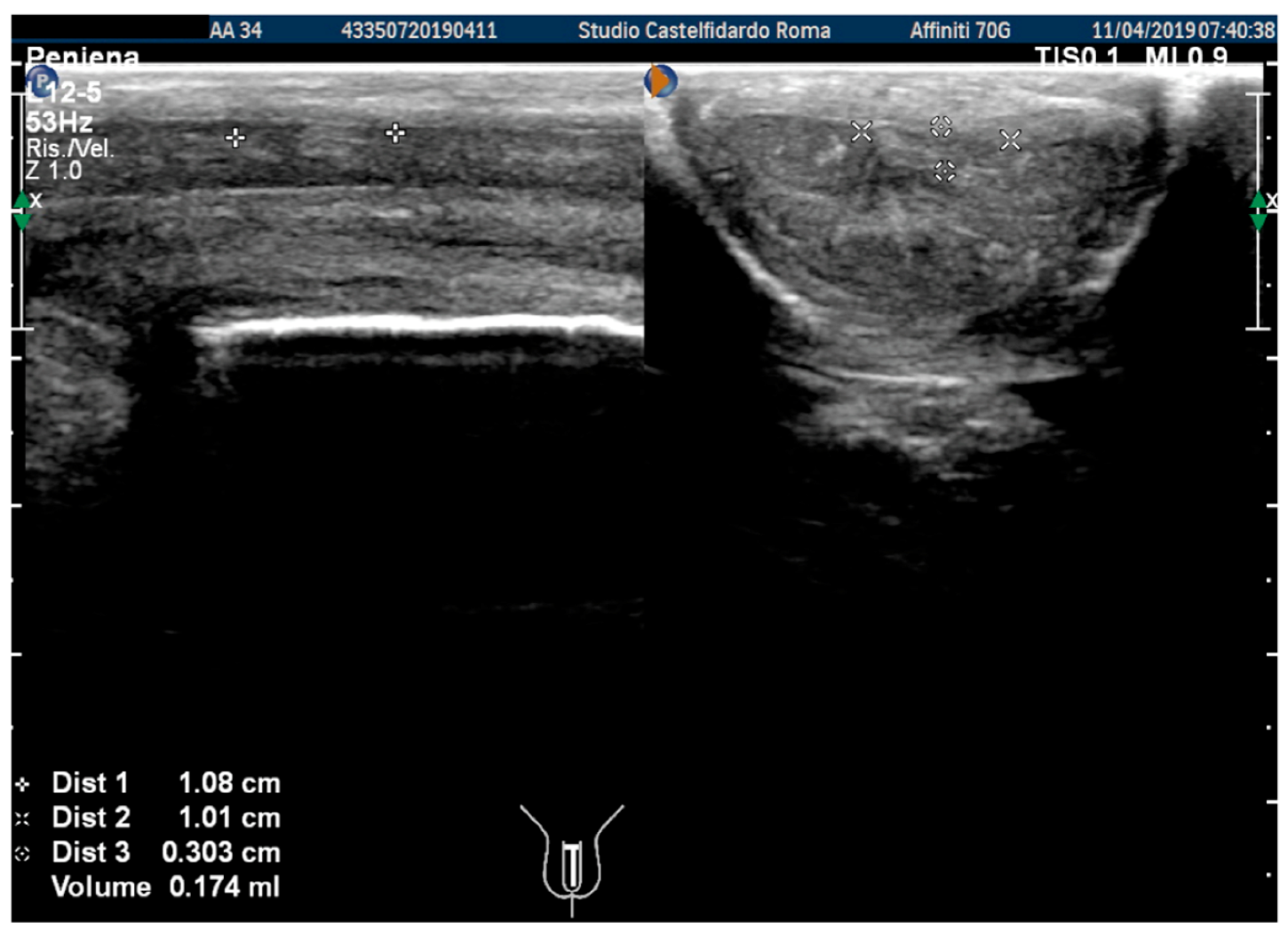
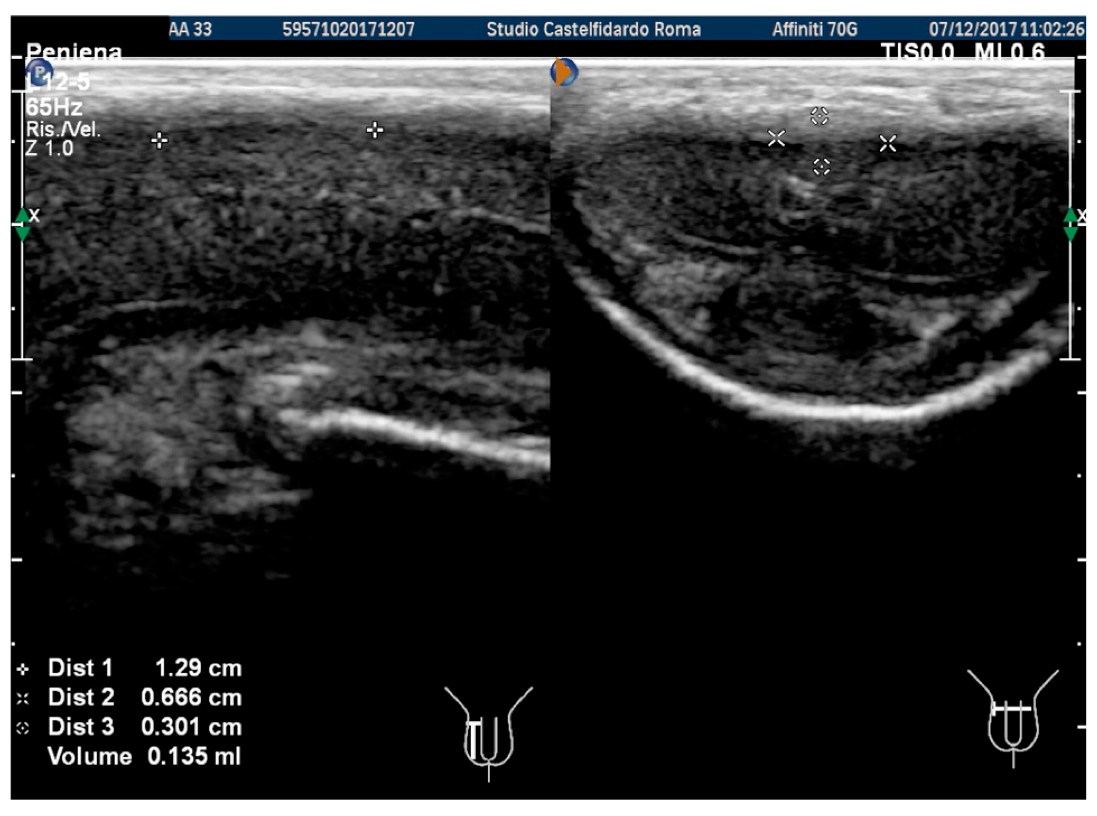
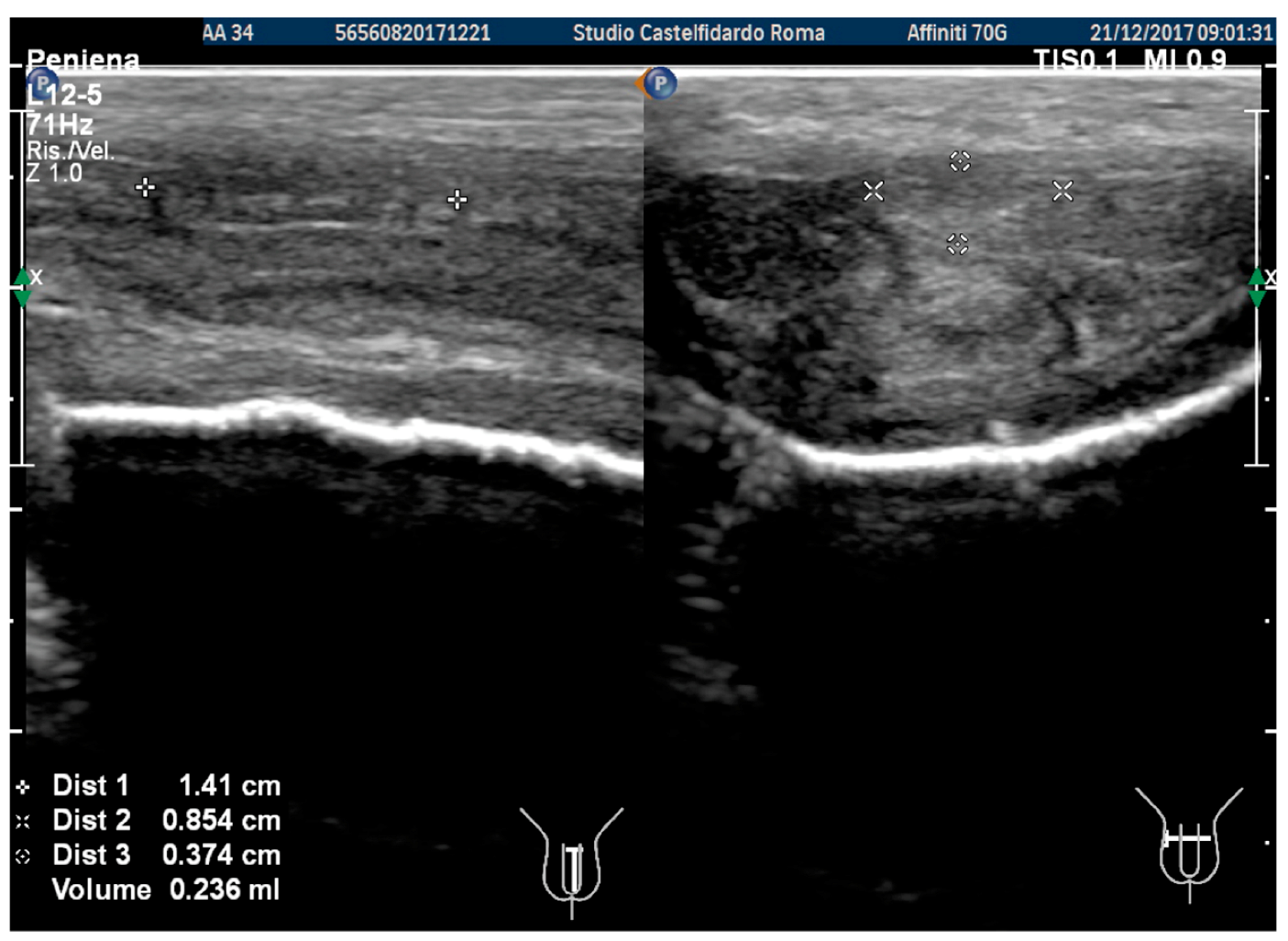
2.1. Case 1
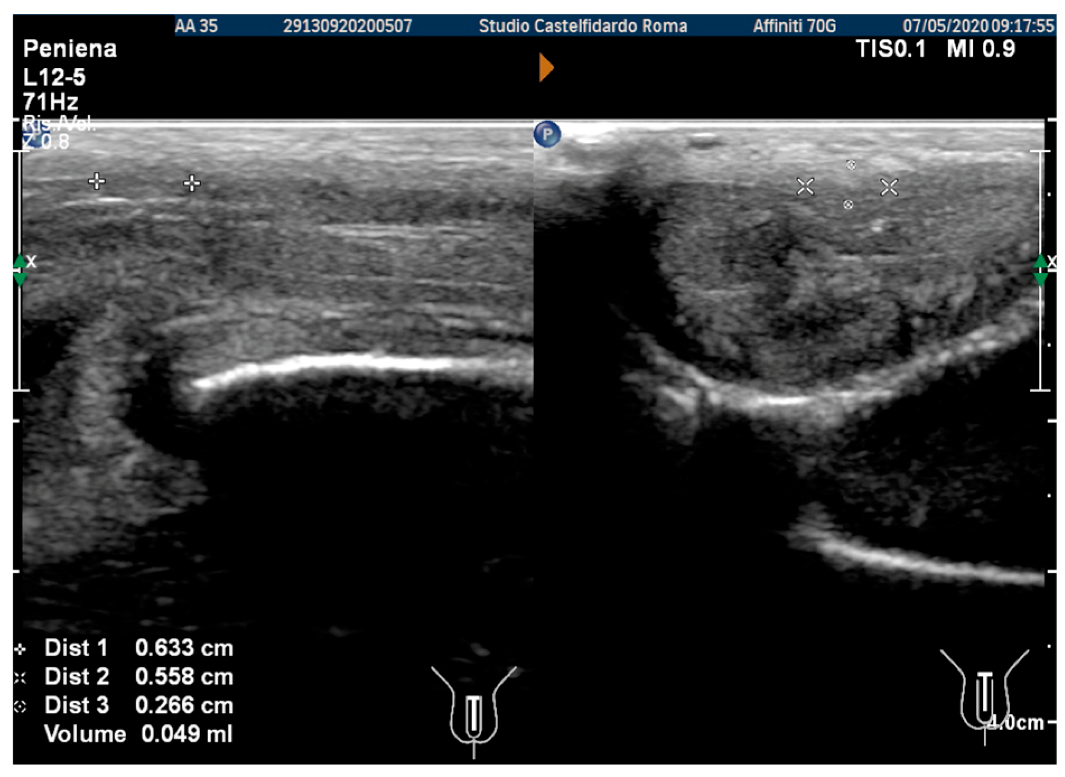
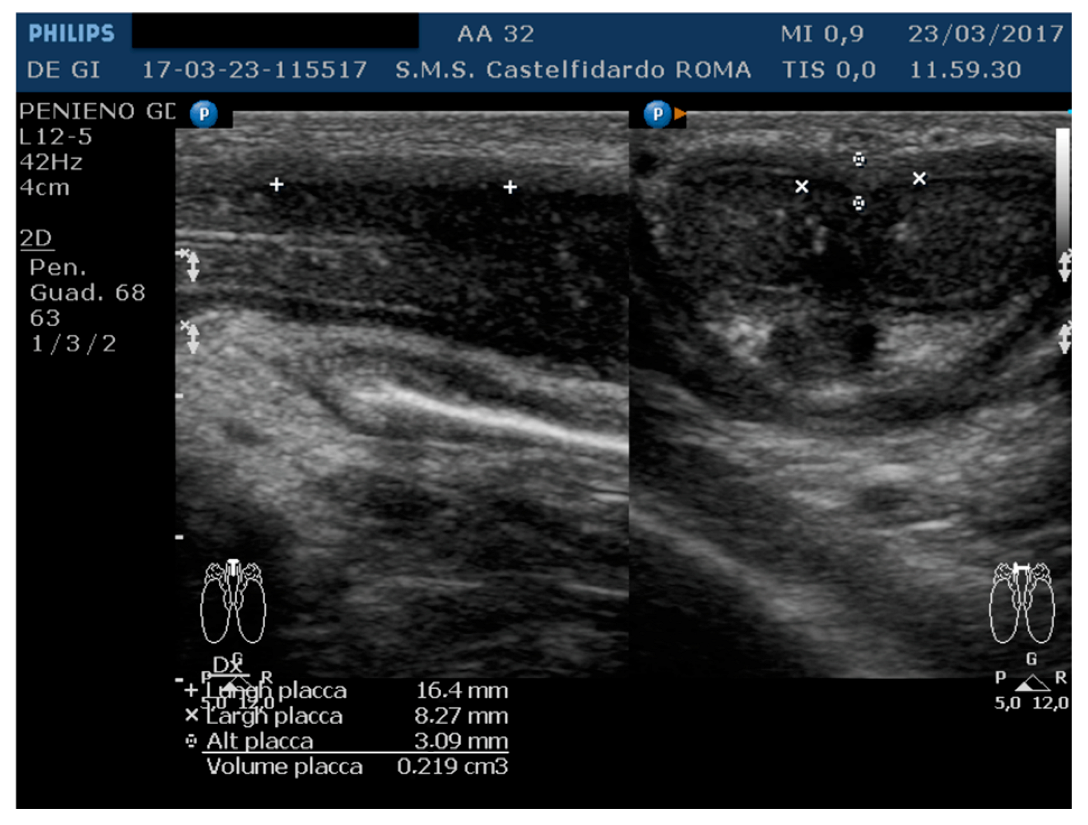
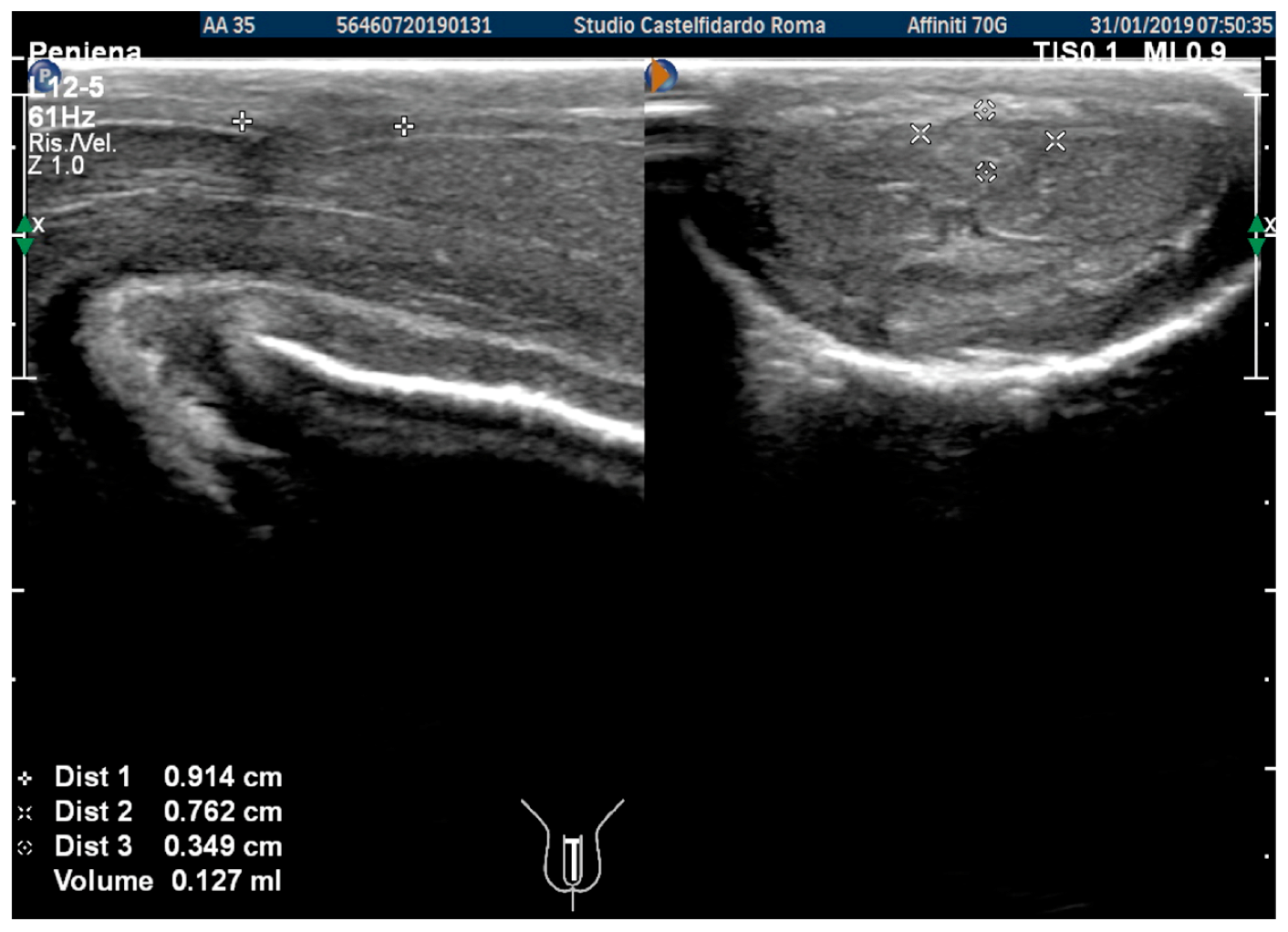
2.2. Case 2
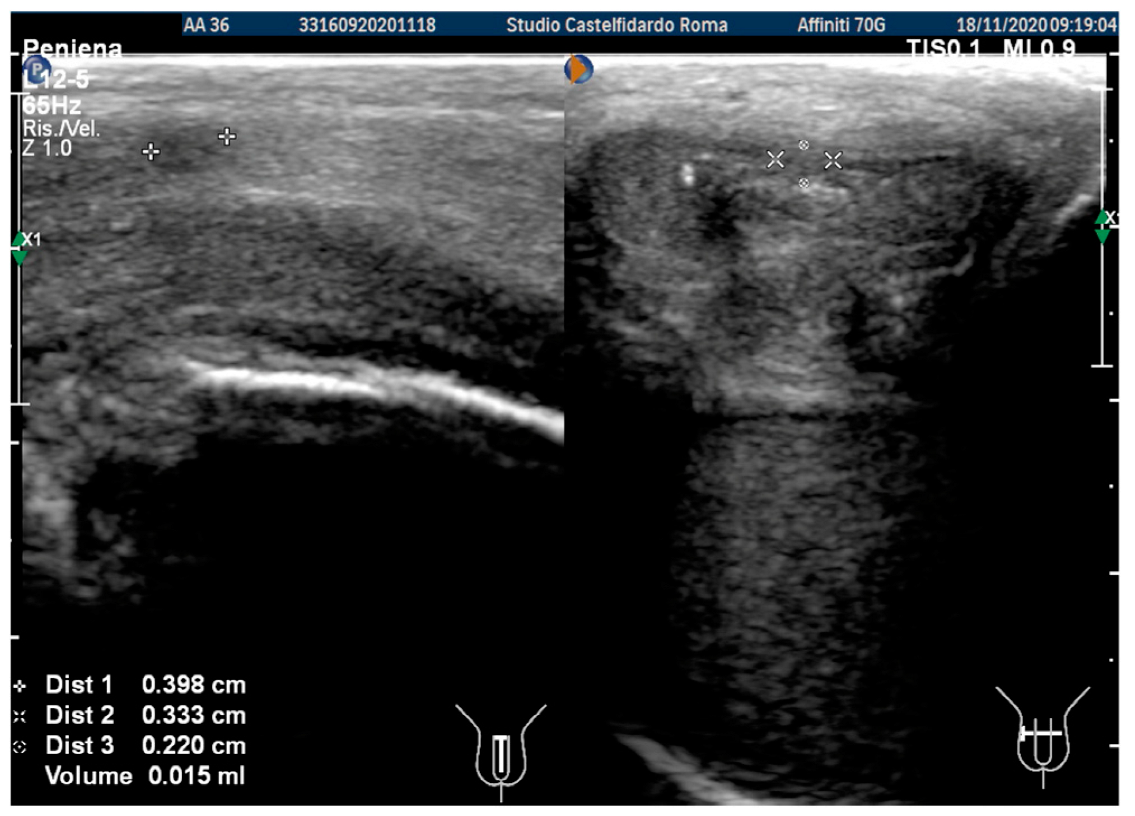
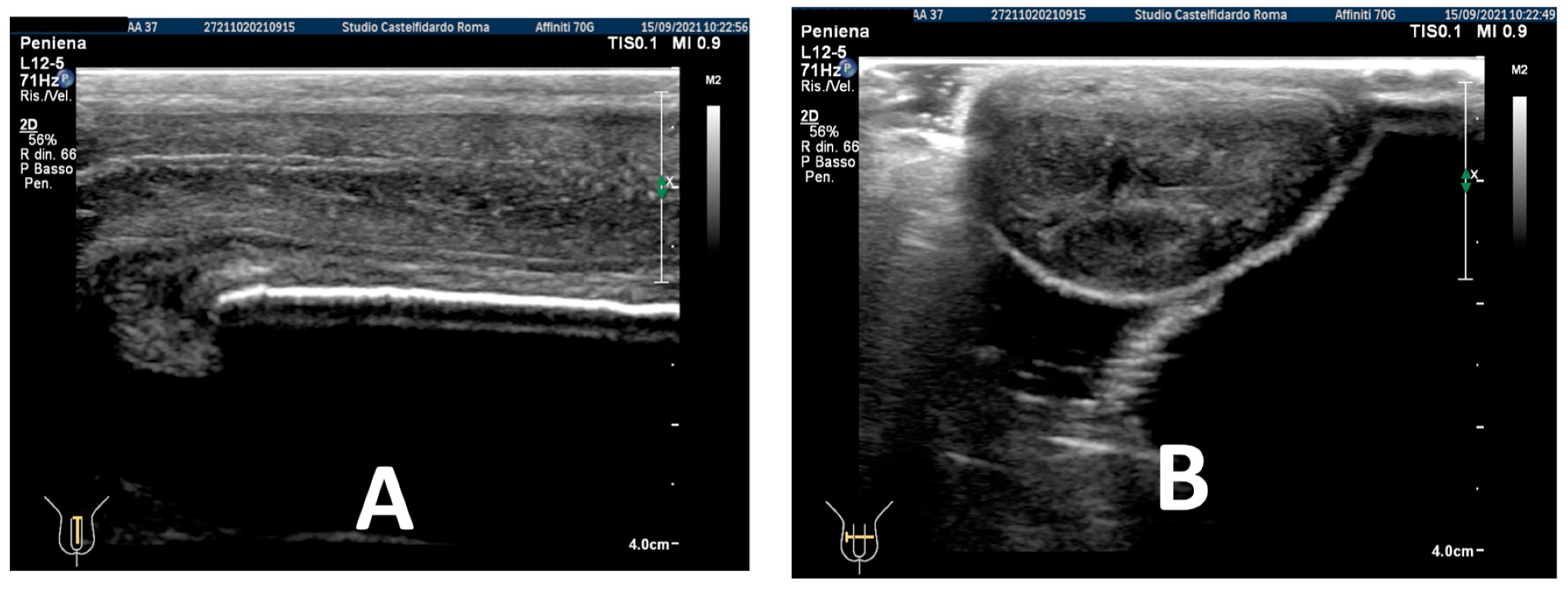
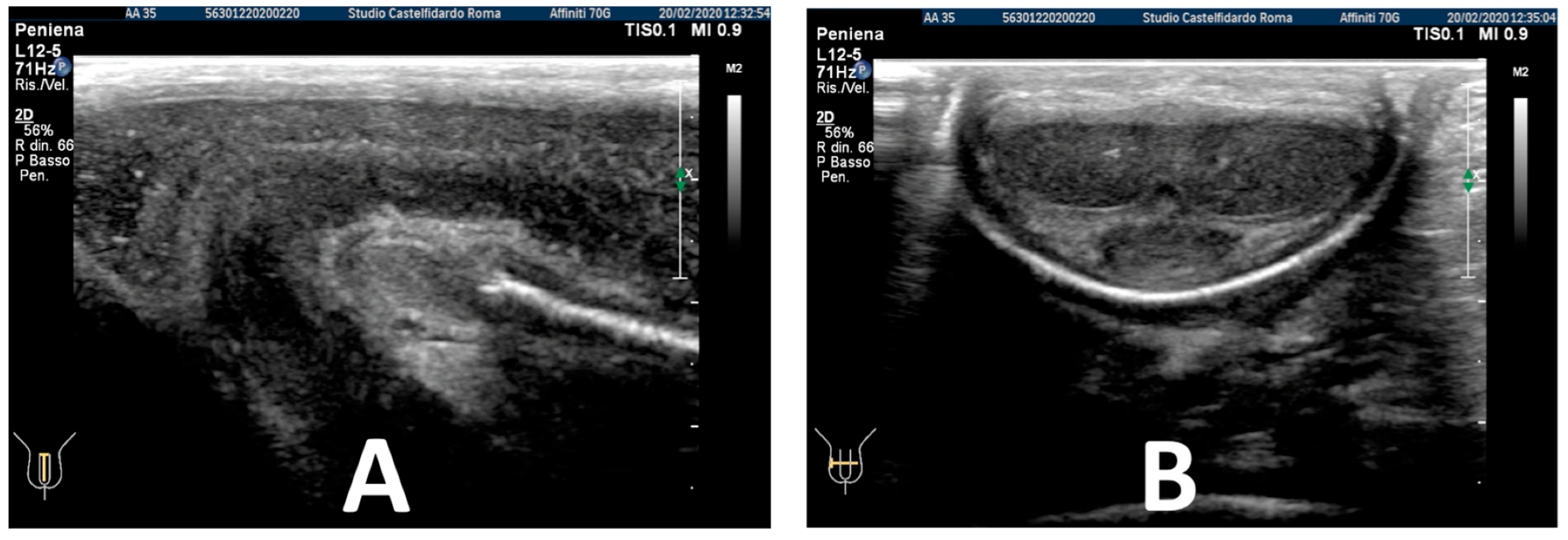
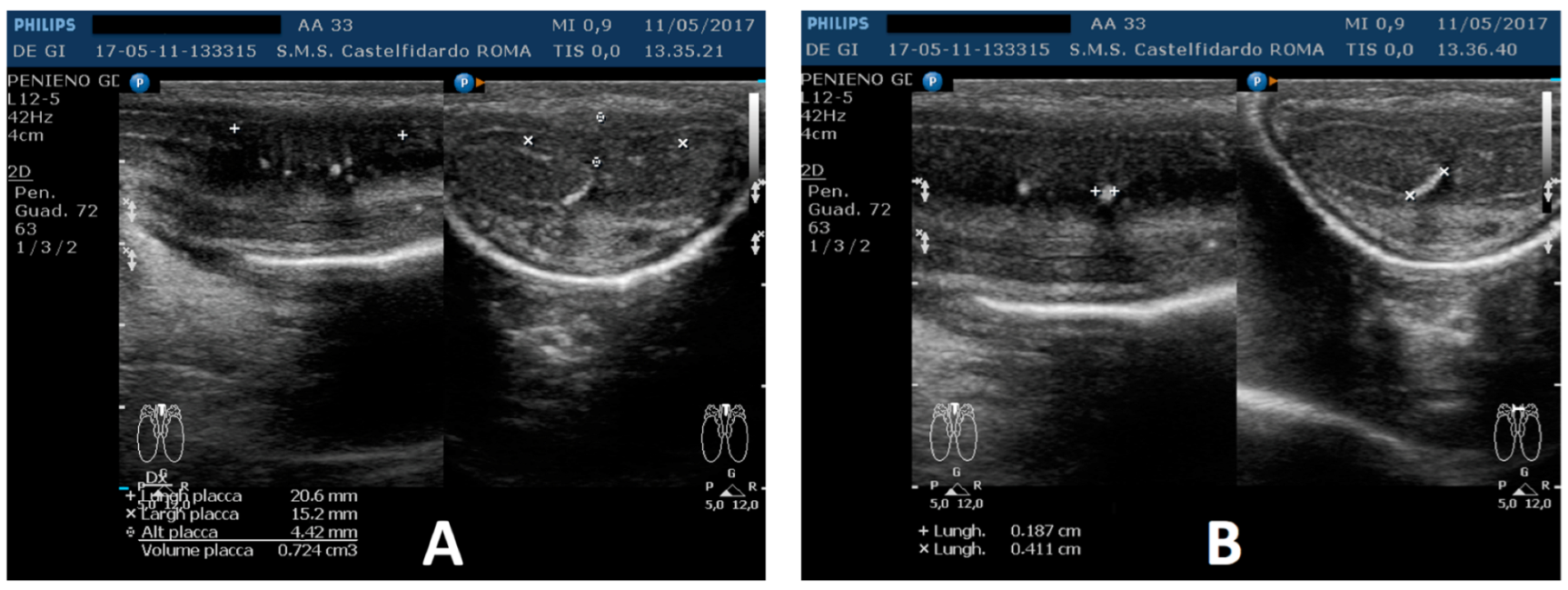
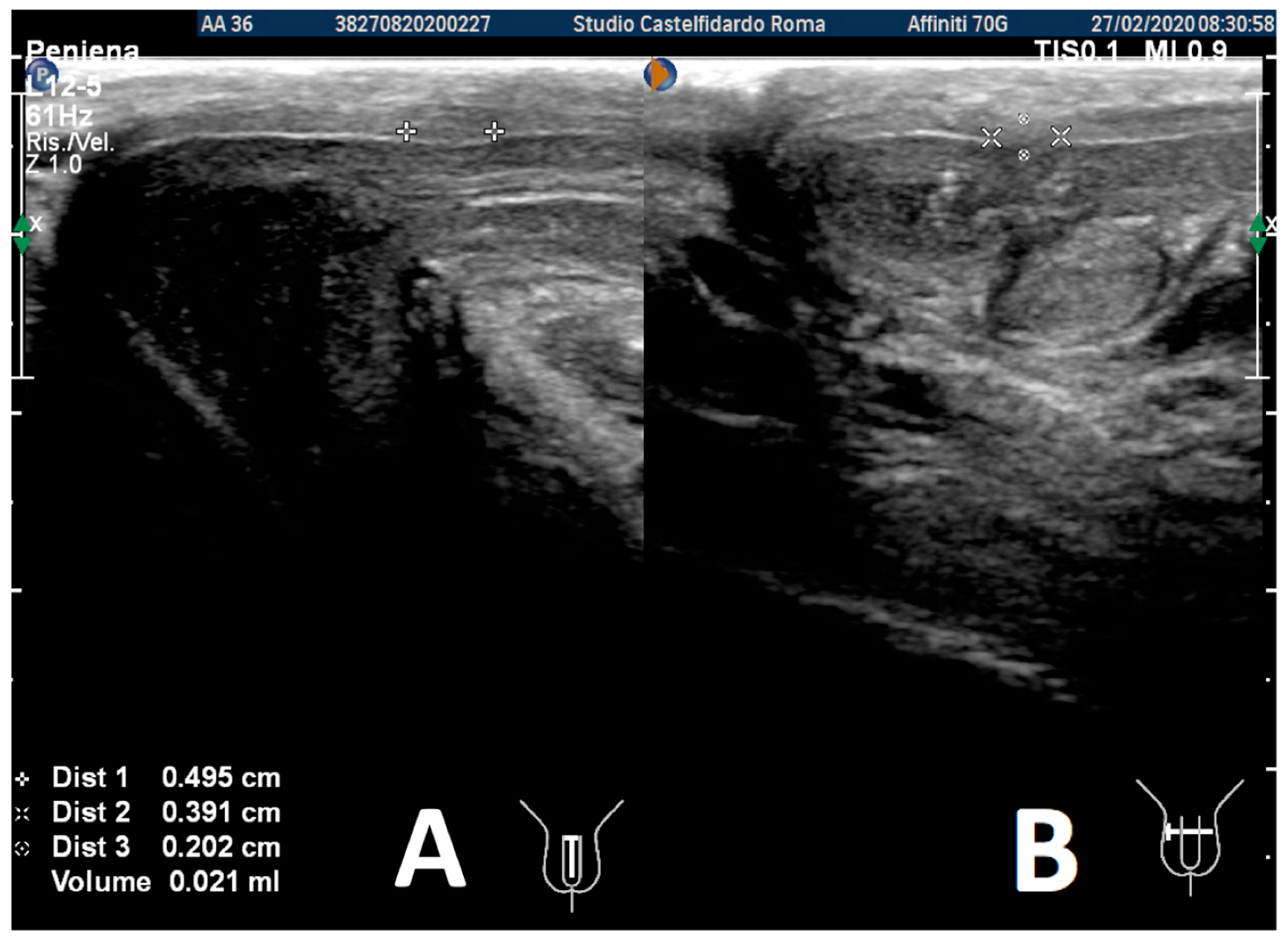
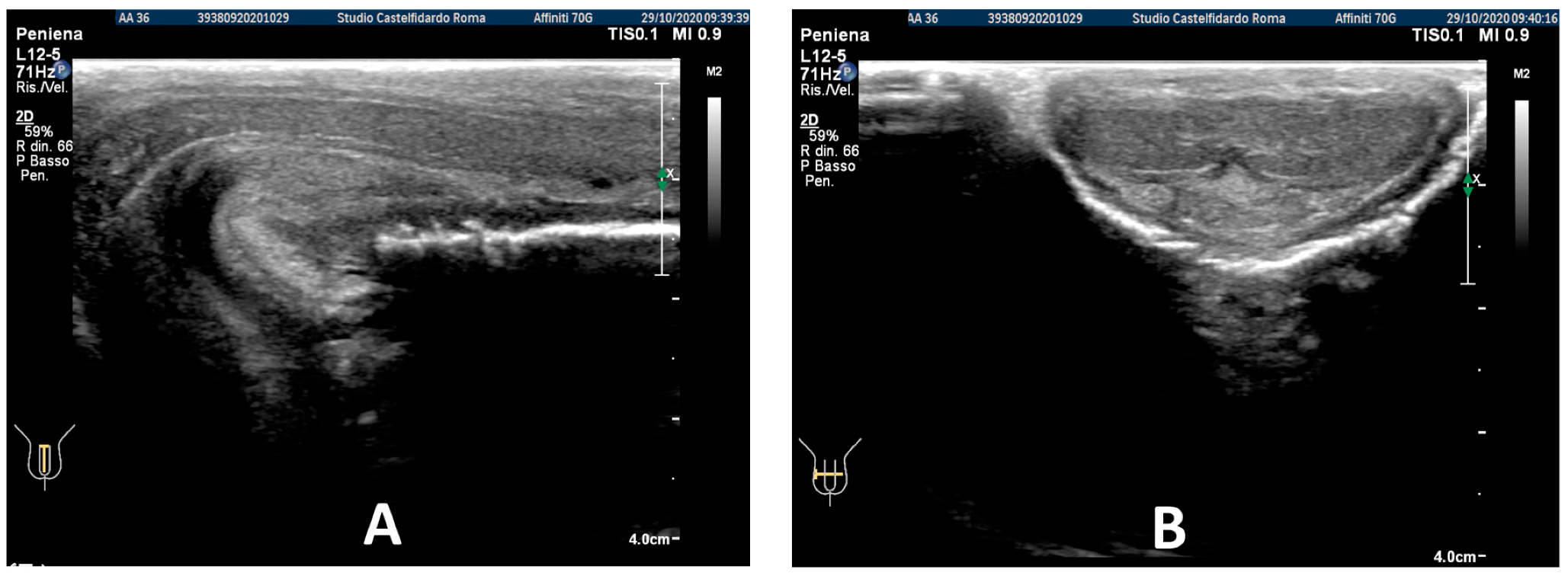
2.3. Case 3
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weidner, W.; Schroeder-Printzen, I.; Weiske, W.H.; Vosshenrich, R. Sexual dysfunction in Peyronie’s disease: An analysis of 222 patients without previous local plaque therapy. J. Urol. 1997, 157, 325–328. [Google Scholar] [CrossRef]
- Pryor, J.P.; Ralph, D.J. Clinical presentations of Peyronie’s disease. Int. J. Impot. Res. 2002, 14, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.J.; Diblasio, C.; Kendirci, M.; Hellstrom, W.; Guhring, P.; Mulhall, J.P. The chronology of depression and distress in men with Peyronie’s disease. J. Sex. Med. 2008, 5, 1985–1990. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, U.; Sommer, F.; Klotz, T.; Braun, M.; Reifenrath, B.; Engelmann, U. The prevalence of Peyronie’s disease: Results of a large survey. BJU Int. 2001, 88, 727–730. [Google Scholar] [CrossRef] [PubMed]
- DiBenedetti, D.B.; Nguyen, D.; Zografos, L.; Ziemiecki, R.; Zhou, X. A Population-based study of peyronie’s disease: Prevalence and treatment patterns in the United States. Adv. Urol. 2011, 2011, 282503. [Google Scholar] [CrossRef] [PubMed]
- Segundo, A.; Glina, S. Prevalence, Risk Factors, and Erectile Dysfunction Associated with Peyronie’s Disease Among Men Seeking Urological Care. Sex. Med. 2020, 8, 230–236. [Google Scholar] [CrossRef]
- Devine, C.J., Jr.; Somers, K.D.; Ladaga, L.E. Peyronie’s disease: Pathophysiology. Prog. Clin. Biol. Res. 1991, 370, 355–358. [Google Scholar]
- Jarow, J.P.; Lowe, F.C. Penile trauma: An etiologic factor in Peyronie’s disease and erectile dysfunction. J. Urol. 1997, 158, 1388–1390. [Google Scholar] [CrossRef]
- Devine, C.J., Jr.; Somers, K.D.; Jordan, G.H.; Schlossberg, S.M. Proposal: Trauma as a cause of Peyronie’s lesion. J. Urol. 1997, 157, 285–290. [Google Scholar] [CrossRef]
- Somers, K.D.; Dawson, D.M. Fibrin deposition in Peyronie’s disease plaque. J. Urol. 1997, 157, 311–315. [Google Scholar] [CrossRef]
- Sikka, S.C.; Hellstrom, W.J. Role of oxidative stress and antioxidants in Peyronie’s disease. Int. J. Impot. Res. 2002, 14, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulis, G.; Romano, G.; Paulis, L.; Barletta, D. Recent Pathophysiological Aspects of Peyronie’s Disease: Role of Free Radicals, Rationale, and Therapeutic Implications for Antioxidant Treatment-Literature Review. Adv. Urol. 2017, 2017, 4653512. [Google Scholar] [CrossRef] [PubMed]
- El-Sakka, A.I.; Salabas, E.; Dinçer, M.; Kadioglu, A. The pathophysiology of Peyronie’s disease. Arab. J. Urol. 2013, 11, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Levine, L.A.; Larsen, S. Diagnosis and Management of Peyronie Disease. In Campbell-Walsh Urology, 11th ed.; Wein, A.J., Kavoussi, L.R., Partin, A.W., Peters, C.A., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2015; pp. 722–748. [Google Scholar]
- Chung, E.; Ralph, D.; Kagioglu, A.; Garaffa, G.; Shamsodini, A.; Bivalacqua, T.; Broderick, G. Evidence-based management guidelines on Peyronie’s disease. J. Sex. Med. 2016, 13, 905–923. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.N.T.; Anaissie, J.; DeLay, K.J.; Yafi, F.A.; Sikka, S.C.; Hellstrom, W.J. Safety and efficacy of collagenase Clostridium histolyticum in the treatment of acute-phase Peyronie’s disease. J. Sex. Med. 2017, 14, 1220–1225. [Google Scholar] [CrossRef] [PubMed]
- Eri, L.M.; Thomassen, H.; Brennhovd, B.; Håheim, L.L. Accuracy and repeatability of prostate volume measurements by transrectal ultrasound. Prostate Cancer Prostatic Dis. 2002, 5, 273–278. [Google Scholar] [CrossRef]
- Lee, J.S.; Chung, B.H. Transrectal ultrasound versus magnetic resonance imaging in the estimation of prostate volume as compared with radical prostatectomy specimens. Urol. Int. 2007, 78, 323–327. [Google Scholar] [CrossRef]
- Paulis, G.; Cavallini, G.; De Giorgio, G.; Quattrocchi, S.; Brancato, T.; Alvaro, R. Long-term multimodal therapy (verapamil associated with propolis, blueberry, vitamin E and local diclofenac) on patients with Peyronie’s disease (chronic inflammation of the tunica albuginea). Results of a controlled study. Inflamm. Allergy Drug Targets 2013, 12, 403–409. [Google Scholar] [CrossRef]
- Favilla, V.; Russo, G.I.; Privitera, S.; Castelli, T.; Madonia, M.; La Vignera, S.; Morgia, G. Combination of intralesional verapamil and oral antioxidants for Peyronie’s disease: A prospective, randomised controlled study. Andrologia 2014, 46, 936–942. [Google Scholar] [CrossRef]
- Paulis, G.; Barletta, D.; Turchi, P.; Vitarelli, A.; Dachille, G.; Fabiani, A.; Gennaro, R. Efficacy and safety evaluation of pentoxifylline associated with other antioxidants in medical treatment of Peyronie’s disease: A case-control study. Res. Rep. Urol. 2016, 8, 1. [Google Scholar] [CrossRef]
- Gallo, L.; Sarnacchiaro, P. Ten-year experience with multimodal treatment for acute phase Peyronie’s disease: A real life clinical report. Actas Urol. Esp. 2019, 43, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Paulis, G.; De Giorgio, G. Complete Plaque Regression in Patients with Peyronie’s Disease after Multimodal Treatment with Antioxidants. A Report of 2 Cases. Am. J. Case Rep. 2022, 23, e936146. [Google Scholar] [CrossRef] [PubMed]
- Kwon, K.D.; Choi, M.J.; Park, J.M.; Song, K.M.; Kwon, M.; Batbold, D.; Suh, J.K. Silencing histone deacetylase 2 using small hairpin RNA induces regression of fibrotic plaque in a rat model of Peyronie’s disease. BJU Int. 2014, 114, 926–936. [Google Scholar] [CrossRef] [PubMed]
- Ji, Q.; Zhang, L.; Jia, H.; Xu, J. Pentoxifylline inhibits endotoxin-induced NF-kappa B activation and associated production of proinflammatory cytokines. Ann. Clin. Lab. Sci. 2004, 34, 427–436. [Google Scholar]
- Karlsen, A.; Paur, I.; Bøhn, S.K.; Sakhi, A.K.; Borge, G.I.; Serafini, M.; Blomhoff, R. Bilberry juice modulates plasma concentration of NF-kappaB related inflammatory markers in subjects at increased risk of CVD. Eur. J. Nutr. 2010, 49, 345–355. [Google Scholar] [CrossRef]
- Búfalo, M.C.; Ferreira, I.; Costa, G.; Francisco, V.; Liberal, J.; Cruz, M.T.; Sforcin, J.M. Propolis and its constituent caffeic acid suppress LPS-stimulated pro-inflammatory response by blocking NF-κB and MAPK activation in macrophages. J. Ethnopharmacol. 2013, 149, 84–92. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, R.; Wang, Y.; Peng, R.; Wu, Y.; Yuan, Y. Ginkgo biloba extract mitigates liver fibrosis and apoptosis by regulating p38 MAPK, NF-κB/IκBα, and Bcl-2/Bax signaling. Drug Des. Dev. Ther. 2015, 9, 6303–6317. [Google Scholar]
- Tian, M.Y.; Fan, J.H.; Zhuang, Z.W.; Dai, F.; Wang, C.Y.; Hou, H.T.; Ma, Y.Z. Effects of silymarin on p65 NF-κB, p38 MAPK and CYP450 in LPS-induced hoof dermal inflammatory cells of dairy cows. BMC Vet. Res. 2019, 15, 127. [Google Scholar] [CrossRef]
- McCauley, J.F.; Dean, R.C. Diagnostic utility of penile ultrasound in Peyronie’s disease. World J. Urol. 2020, 38, 263–268. [Google Scholar] [CrossRef]
- Hatzimouratidis, K.; Eardley, I.; Giuliano, F.; Hatzichristou, D.; Moncada, I.; Salonia, A.; Wespes, E. EAU guidelines on penile curvature. Eur. Urol. 2012, 62, 543–552. [Google Scholar] [CrossRef]
- Parmar, M.; Masterson, J.M.; Masterson, T.A., 3rd. The role of imaging in the diagnosis and management of Peyronie’s disease. Curr. Opin. Urol. 2020, 30, 283–289. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Age/Years | Concomitant Diseases | Localization of the Penile Plaque | Plaque Measurements ( Length × Width × Thickness) and Volume of the Plaque (A) Prior and (B) After Therapy | Typology of the Curvature (A) Prior and (B) After Therapy | Penile Pain VAS Scale (Score 1 to 10) (A) Prior and (B) After Therapy | IIEF Questionnaire Score (A) Prior and (B) After Therapy | Duration of Therapy Up to Plaque Regression | Description of the Administered Multimodal Therapy |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 34 years | Congenital lateral-left penile curvature (10-degrees) | Middle third | (A) 10.8 × 10.1 × 3.03 mm volume = 174 mm3 | (A) 40-degree left curvature | (A) score 2 | (A) score 26 | 2 years and 5 months | orally: Silymarin 400 mg + Ginkgo biloba 250 mg + Propolis 600 mg + Bilberry 160 mg + Vitamin E 800 IU/once a day, for 29 months. + topically: Propolis creme/twice a day/for 29 months. * The patient refused peri-plaque penile injections |
| (B) No plaque detected | (B) 10-degree left penile curvature (previous condition = congenital lateral left penile curvature) | (B) score 0 (after 12 months) | (B) score 26 | ||||||
| 2 | 32 years | lichen sclerosus, chronic prostatitis | Proximal third | (A) 16.4 × 8.27 × 3.09 mm volume = 219 mm3 | (A) 10-degree left curvature | (A) score 3 | (A) score 26 | 2 years and 9 months | orally: Silymarin 400 mg + Ginkgo biloba 250 mg + Propolis 600 mg + Bilberry 160 mg + Vitamin E 800 IU/once a day, for 33 months. + topically: Propolis creme/twice a day/for 33 months. + peri-plaque penile injections: Pentoxifylline 100 mg (30 G needle) every 15 days for 6 months, and then monthly for 12 months, and then 1 injection every other month. for 12 months (total = 30 injections) |
| (B) No plaque detected | (B) None | (B) score 0 (after six months) | (B) score 28 | ||||||
| 3 | 33 years | None | Middle third | (A) 20.6 × 15.2 × 4.42 mm volume = 724 mm3 + some small calcifications, the largest of which measured 1.9 × 4.1 mm | (A) 30-degree dorsal penile curvature | (A) score 2 | (A) score 26 | 3 years and 5 months | orally: Silymarin 400 mg + Ginkgo biloba 250 mg + Propolis 600 mg + Bilberry 160 mg + Vitamin E 800 IU/once a day, for 41 months. + topically: Propolis creme/twice a day/for 41 months. + peri-plaque penile injections: Pentoxifylline 100 mg (30 G needle) every 15 days for 6 months, and then monthly for 12 months, and then 1 injection every other month. for 12 months (total = 30 injections) |
| (B) No plaque detected | (B) None | (B) score 0 (after six months) | (B) score 27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paulis, G.; De Giorgio, G. Full Regression of Peyronie’s Disease Plaque Following Combined Antioxidant Treatment: A Three-Case Report. Antioxidants 2022, 11, 1661. https://doi.org/10.3390/antiox11091661
Paulis G, De Giorgio G. Full Regression of Peyronie’s Disease Plaque Following Combined Antioxidant Treatment: A Three-Case Report. Antioxidants. 2022; 11(9):1661. https://doi.org/10.3390/antiox11091661
Chicago/Turabian StylePaulis, Gianni, and Giovanni De Giorgio. 2022. "Full Regression of Peyronie’s Disease Plaque Following Combined Antioxidant Treatment: A Three-Case Report" Antioxidants 11, no. 9: 1661. https://doi.org/10.3390/antiox11091661