
A Systematic Review on the Role of Vitamin C in Tissue Healing



Abstract
:1. Introduction
2. Materials and Methods
- (i)
- Cochrane Library (searched 26 April 2022)
- (ii)
- Ovid Embase (searched 5 April 2022)
- (iii)
- Ovid MEDLINE (searched 26 April 2022)
- (iv)
- PubMed (searched 5 April 2022)
Inclusion and Exclusion Criteria
3. Results
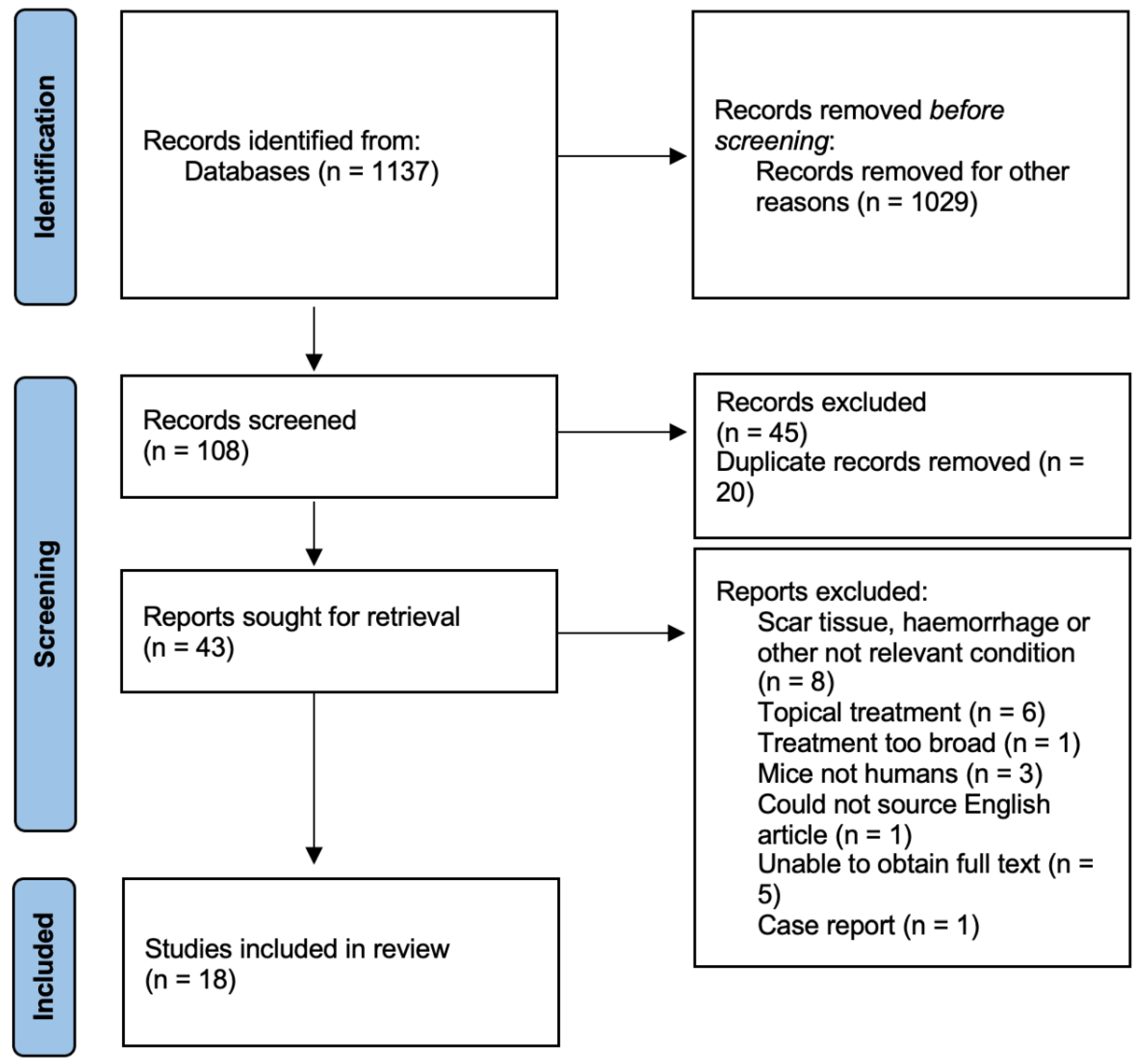
3.1. Study Selection
3.2. Description of Included Studies
3.3. Vitamin C Studies
3.3.1. Pressure Ulcers
3.3.2. Dental Extractions, Implants and Gingivitis
3.3.3. Foot Ulcers
3.3.4. Fractures
3.4. Studies with Combined Treatments
3.4.1. Pressure Ulcers
3.4.2. Foot Ulcers
3.4.3. Burns
3.4.4. Unspecified Trauma
3.4.5. Hernia Repair
3.4.6. Tattoo Resection
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| EAR | Estimated average requirement |
| PRP-FG | Platelet-rich plasma-fibrin glue |
| PUSH | Pressure Ulcer Scale for Healing |
| RCT | Randomized controlled trial |
| RDI | Recommended dietary intake |
References
- Collins, N. Nutrition 411: Revisiting vitamin C and wound healing. Ostomy Wound Manag. 2013, 59, 12–14. [Google Scholar]
- Nishikimi, M.; Fukuyama, R.; Minoshima, S.; Shimizu, N.; Yagi, K. Cloning and chromosomal mapping of the human nonfunctional gene for L-gulono-gamma-lactone oxidase, the enzyme for L-ascorbic acid biosynthesis missing in man. J. Biol. Chem. 1994, 269, 13685–13688. [Google Scholar] [CrossRef]
- Australian Government. Nutrient Reference Values for Australia and New Zealand. Vitamin C Canberra 2017. Available online: https://www.nhmrc.gov.au/sites/default/files/images/Nutrient-reference-aus-nz-executive-summary.pdf (accessed on 23 January 2017).
- Pullar, J.; Carr, A.; Vissers, M. The roles of vitamin C in skin health. Nutrients 2017, 9, 866. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, P.; Wiltshire, S.; Das, K.; Wilson, R. Vitamin C deficiency in an Australian cohort of metropolitan surgical patients. J. Pathol. 2018, 50, 654–658. [Google Scholar] [CrossRef] [PubMed]
- Gunton, J.E.; Girgis, C.M.; Lau, T.; Vicaretti, M.; Begg, L.; Flood, V. Vitamin C improves healing of foot ulcers: A randomised, double-blind, placebo-controlled trial. Br. J. Nutr. 2021, 126, 1451–1458. [Google Scholar] [CrossRef]
- Christie-David, D.; Gunton, J. Vitamin C deficiency and diabetes mellitus–easily missed? Diabetic Med. 2017, 34, 294–296. [Google Scholar] [CrossRef]
- Munday, M.-R.; Rodricks, R.; Fitzpatrick, M.; Flood, V.M.; Gunton, J.E. A pilot study examining vitamin C levels in periodontal patients. Nutrients 2020, 12, 2255. [Google Scholar] [CrossRef]
- Van Anholt, R.D.; Sobotka, L.; Meijer, E.P.; Heyman, H.; Groen, H.W.; Topinková, E.; van Leen, M.; Schols, J.M. Specific nutritional support accelerates pressure ulcer healing and reduces wound care intensity in non-malnourished patients. Nutrition 2010, 26, 867–872. [Google Scholar] [CrossRef]
- Cereda, E.; Gini, A.; Pedrolli, C.; Vanotti, A. Disease-specific, versus standard, nutritional support for the treatment of pressure ulcers in institutionalized older adults: A randomized controlled trial. J. Am. Geriatr. Soc. 2009, 57, 1395–1402. [Google Scholar] [CrossRef]
- Desneves, K.J.; Todorovic, B.E.; Cassar, A.; Crowe, T.C. Treatment with supplementary arginine, vitamin C and zinc in patients with pressure ulcers: A randomised controlled trial. Clin. Nutr. 2005, 24, 979–987. [Google Scholar] [CrossRef]
- Frias Soriano, L.; Lage Vazquez, M.A.; Maristany, C.P.; Xandri Graupera, J.M.; Wouters-Wesseling, W.; Wagenaar, L. The effectiveness of oral nutritional supplementation in the healing of pressure ulcers. J. Wound Care 2004, 13, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Taylor, T.V.; Rimmer, S.; Day, B.; Butcher, J.; Dymock, I.W. Ascorbic acid supplementation in the treatment of pressure-sores. Lancet 1974, 2, 544–546. [Google Scholar] [CrossRef]
- Ter Riet, G.; Kessels, A.G.; Knipschild, P.G. Randomized clinical trial of ascorbic acid in the treatment of pressure ulcers. J. Clin. Epidemiol. 1995, 48, 1453–1460. [Google Scholar] [CrossRef]
- Abrahmsohn, G.M.; Halberstein, R.A.; Fregeolle, S. Vitamin C and dental healing: Testing and placebo effect. Gen. Dent. 1993, 41, 523–527. [Google Scholar] [PubMed]
- Pisalsitsakul, N.; Pinnoi, C.; Sutanthavibul, N.; Kamolratanakul, P. Taking 200 mg vitamin C three times per day improved extraction socket wound healing parameters: A randomized clinical trial. Int. J. Dent. 2022, 2022, 6437200. [Google Scholar] [CrossRef]
- Yingcharoenthana, S.; Ampornaramveth, R.; Subbalekha, K.; Sinpitaksakul, P.; Kamolratanakul, P. A split-mouth randomized clinical trial to evaluate the effect of local and systemic administration of vitamin C on extraction wound healing. J. Oral Sci. 2021, 63, 198–200. [Google Scholar] [CrossRef]
- Yarahmadi, A.; Saeed Modaghegh, M.H.; Mostafavi-Pour, Z.; Azarpira, N.; Mousavian, A.; Bonakdaran, S.; Jarahi, L.; Samadi, A.; Peimani, M.; Hamidi Alamdari, D. The effect of platelet-rich plasma-fibrin glue dressing in combination with oral vitamin E and C for treatment of non-healing diabetic foot ulcers: A randomized, double-blind, parallel-group, clinical trial. Exp. Opin. Biol. Ther. 2021, 21, 687–696. [Google Scholar] [CrossRef]
- Li, X.; Tang, L.; Lin, Y.F.; Xie, G.F. Role of vitamin C in wound healing after dental implant surgery in patients treated with bone grafts and patients with chronic periodontitis. Clin. Implant Dent. Relat. Res. 2018, 20, 793–798. [Google Scholar] [CrossRef]
- Woolfe, S.N.; Kenney, E.B.; Hume, W.R.; Carranza, F.A., Jr. Relationship of ascorbic acid levels of blood and gingival tissue with response to periodontal therapy. J. Clin. Periodontol. 1984, 11, 159–165. [Google Scholar] [CrossRef]
- Ekrol, I.; Duckworth, A.D.; Ralston, S.H.; Court-Brown, C.M.; McQueen, M.M. The influence of vitamin C on the outcome of distal radial fractures: A double-blind, randomized controlled trial. J. Bone Joint Surg. Am. 2014, 96, 1451–1459. [Google Scholar] [CrossRef]
- Barbosa, E.; Faintuch, J.; Machado Moreira, E.A.; Goncalves da Silva, V.R.; Lopes Pereima, M.J.; Martins Fagundes, R.L.; Filho, D.W. Supplementation of vitamin E, vitamin C, and zinc attenuates oxidative stress in burned children: A randomized, double-blind, placebo-controlled pilot study. J. Burn Care Res. 2009, 30, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Blass, S.C.; Goost, H.; Tolba, R.H.; Stoffel-Wagner, B.; Kabir, K.; Burger, C.; Stehle, P.; Ellinger, S. Time to wound closure in trauma patients with disorders in wound healing is shortened by supplements containing antioxidant micronutrients and glutamine: A PRCT. Clin. Nutr. 2012, 31, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Kjaer, M.; Frederiksen, A.K.S.; Nissen, N.I.; Willumsen, N.; van Hall, G.; Jorgensen, L.N.; Andersen, J.R.; Ågren, M.S. Multinutrient supplementation increases collagen synthesis during early wound repair in a randomized controlled trial in patients with inguinal hernia. J. Nutr. 2020, 150, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Vaxman, F.; Olender, S.; Lambert, A.; Nisand, G.; Aprahamian, M.; Bruch, J.F.; Didier, E.; Volkmar, P.; Grenier, J.F. Effect of pantothenic acid and ascorbic acid supplementation on human skin wound healing process. A double-blind, prospective and randomized trial. Eur. Surg. Res. 1995, 27, 158–166. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age (Years) | EAR (mg/Day) | RDI (mg/Day) |
|---|---|---|
| 1–8 | 25 | 35 |
| 9–18 | 28 | 40 |
| >19 | 30 | 45 |
| Author, Year, Country | Study Type | No. Cases vs. Controls | Dosage, Duration | Baseline C Measured? | Wound Type | Study Outcomes |
|---|---|---|---|---|---|---|
| Abrahmsohn et al., 1993, USA | RCT | 81 vs. 80 | 3 weeks, 500 mg t.i.d. | No, diet score | Dental extraction | Vit. C group healed faster (p = 0.01). 1.2% in vit. C group had dry socket vs. 10% of placebo. 12.3% in vit. C group healed slowly vs. 37.5% in placebo. No differences with gender or age. |
| Ekrol et al., 2014, Scotland | RCT | 169 vs. 167 | 500 mg daily for 50 days | No, diet score | Fracture of the distal radius | No difference in time to fracture-healing. In non-displaced fracture subgroup, greater wrist flexion deficit (p = 0.008), pinch strength deficit (p = 0.02) and proportion with higher pain-score in vit. C group at 6 weeks but not at other times. At 52 weeks, higher rate of complications (p = 0.043) and greater pain (p = 0.045) in displaced fracture C group. No mention of correction for multiple comparisons. Measures would not retain significance if this needs to be added. |
| Gunton et al., 2021, Australia | RCT | 7 vs. 9 | 500 mg daily for 8 weeks | Yes, 50%deficient | Foot ulcers | Healing at 8 weeks (primary endpoint) sig. better in vit C group (p = 0.041). Time to 50% reduction in wound volume faster. Healing without amputation in all in vit. C group vs. 5 of 9 controls. |
| Li et al., 2018, China | RCT | 65 vs. 63 | 300 mg daily for 1 week postop | No | Dental implants | C group sig. higher healing rates than controls at day 7 (p < 0.05). No difference in pain between groups. |
| Pisalsitsakul et al., 2022, Thailand | RCT | 10 vs. 12 | 10 days, 600 mg or 1500 mg t.i.d. | No. Meal record 7 days after extraction | Dental extraction | Pain scores sig. lower in 600 mg group vs. placebo (p < 0.05). Greater reduction at extraction site deficit in 600 mg/d vs. placebo (p < 0.05). Trend to reduced wound depth in 1500 mg group versus placebo (p < 0.07). |
| Taylor et al., 1974, England | RCT | 10 vs. 10 | 500 mg twice daily for 4 weeks | Yes, leucocyte levels, mean in placebo 24 μg/108 cells and 22 in tx group. | Pressure ulcers | Increased vitamin C in treatment group (65.5 vs. 25.8). Mean reduction of ulcer of 42.7% in placebo vs. 84% in C group (p < 0.005). |
| Ter Riet et al., 1995, The Netherlands | RCT | 43 vs. 45 | 500 mg twice daily for 12 weeks | Yes, but deficiencies at baseline NR | Pressure ulcers | Mean increase 14.9 mg/litre in tx group, placebo group rose by 4.8 mg/litre, No significant difference in healing rates, 0.21 cm2 in C and 0.27 cm2/week in controls. |
| Woolfe et al., 1984, U.S.A | RCT | 5 vs. 5 | 250 mg 4× day for 6 weeks | Yes, not different at baseline or 6 weeks | Gingivitis | No sig. correlations between Gingival Index. Did not find an increase in serum vit. C levels between tx and controls. |
| Yingcharoenthana et al., 2021, Thailand | Single-blind RCT | 10 vs. 10 vs. 10 | 600 mg daily for 2 weeks | No | Dental extraction | Reduction in socket depth sig. higher in C group vs. controls (p = 0.028). No difference in radiographic density of new bone formation between groups. |
| Author, Year, Country | Study Type | No. Cases vs. Controls | Dosage, Duration | Additional Treatments | Baseline C Measured | Wound Type | Study Outcome |
|---|---|---|---|---|---|---|---|
| Barbosa et al., 2009, Brazil | RCT | 17 vs. 15 | 1 week, 1.5× UL, t.i.d. | Vit E and Zn | Yes, no sig. difference between groups | Burns | No differences in CRP. No. of days to complete tissue repair sig. lower in active group (p < 0.001). |
| Blass et al., 2012, Germany | RCT | 10 vs. 10 | 2 weeks, 2 sachets bd, 500 mg vit C | Vit E, A, Selenium, Zn, Glutamine | Yes, no sig. difference between groups | Trauma patients | CRP decreased in placebo group (p = 0.037). Wound closure faster in active group (29 vs. 58 days) (p = 0.01). No change in LoS. |
| Cereda et al., 2009, Italy | RCT | 13 vs. 15 | Oral 500 mg, tube fed 380 mg vit C daily | Protein, Arginine, Zn | No. Food diary, no differences at baseline. | Pressure ulcers | Greater reduction in wound surface area at 8-week follow-up in active group (57% vs. 33%) (p < 0.02). Sig. reduction in PUSH scores vs. controls (p < 0.05). |
| Desneves et al., 2005, Australia | RCT | 6 vs. 5 vs. 5 | 3 weeks, 2× day 72 mg OR 500 mg vit C | Zn, Arginine | Yes, no differences | Pressure ulcers | Increase in vitamin C in group 3. PUSH score at week 3 sig. lower in group treated with vit. C (p < 0.05) with sig. improvements in PU surface area (p < 0.01). |
| Frias Soriano et al., 2004, Spain | Prospective | 39 | 1–3× day for 3 weeks; 250 mg vit C | Protein, Vit E, Zn | No | Pressure ulcers | Reduced wound area (p < 0.001), exudate in infected ulcers (p = 0.012) and amount of necrotic tissue (p = 0.001). |
| Kjaer et al., 2020, Denmark | RCT | 11 vs. 10 | 4 weeks, 1250 mg vit C daily | Arginine, Glutamine, Zn | No | Hernia repair | Serum procollagen propeptide concentrations decreased post-op in control group vs. active group (p < 0.05). |
| Van Anholt et al., 2010, The Netherlands | RCT | 22 vs. 21 | 250 t.i.d. for 8 weeks; 250 mg vit C | Vit A, E, Zn, Cu protein, sel, arginine, folate | Yes, 23 mmol/L in tx group vs. 19.8 in control, 60.2 vs. 26.6 at end of study | Pressure ulcers | Decreased ulcer size vs. controls (p < 0.016). Fewer dressing changes required per week (p < 0.045). Serum vit C sig. increased (p = 0.015). |
| Vaxman et al., 1995, France | RCT | 18 vs. 22 | 1000 mg daily for 3 weeks | Pantothenic acid | Yes, no differences reported | Tattoo resection | Serum vit. C increased in active group vs. decreased in controls. No change in healing process. |
| Yarahmadi et al., 2021, Iran | RCT | 13 vs. 12 | 250 mg 2× day for 8 weeks | Vit E and PRP-FG dressing | No | Foot ulcers | Wound size reduced in both groups, and sig. greater in active group (p = 0.019). Decrease in CRP in active group (p < 0.05). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bechara, N.; Flood, V.M.; Gunton, J.E. A Systematic Review on the Role of Vitamin C in Tissue Healing. Antioxidants 2022, 11, 1605. https://doi.org/10.3390/antiox11081605
Bechara N, Flood VM, Gunton JE. A Systematic Review on the Role of Vitamin C in Tissue Healing. Antioxidants. 2022; 11(8):1605. https://doi.org/10.3390/antiox11081605
Chicago/Turabian StyleBechara, Nada, Victoria M. Flood, and Jenny E. Gunton. 2022. "A Systematic Review on the Role of Vitamin C in Tissue Healing" Antioxidants 11, no. 8: 1605. https://doi.org/10.3390/antiox11081605