
Metabolic Disorders in Patients with Chronic Hepatitis B Virus Infection: Coffee as a Panacea? (ANRS CO22 Hepather Cohort)

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
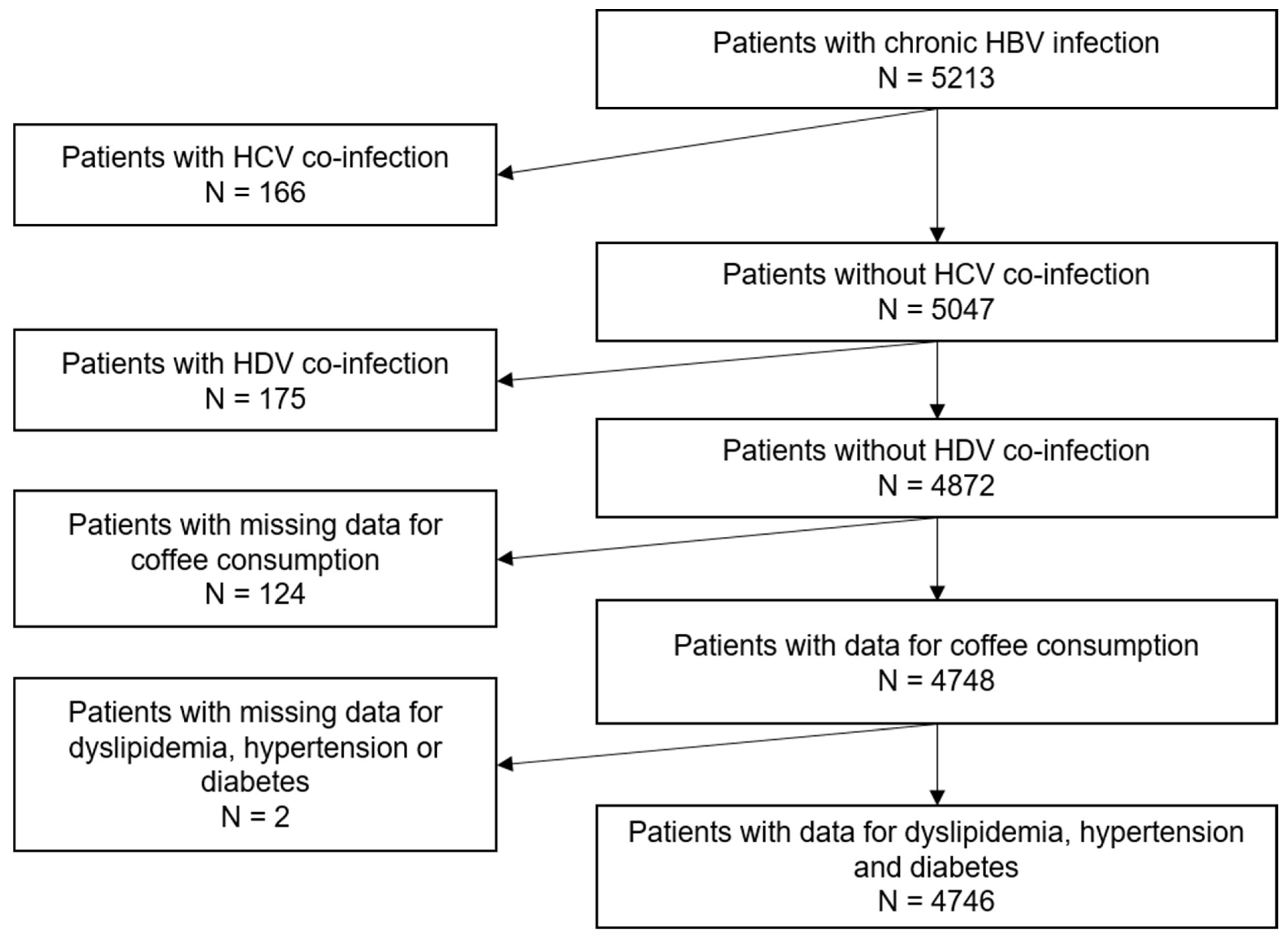
2.2. Study Population
2.3. Data Collection
2.4. Outcomes
2.5. Explanatory Variables
2.6. Statistical Analyses
3. Results
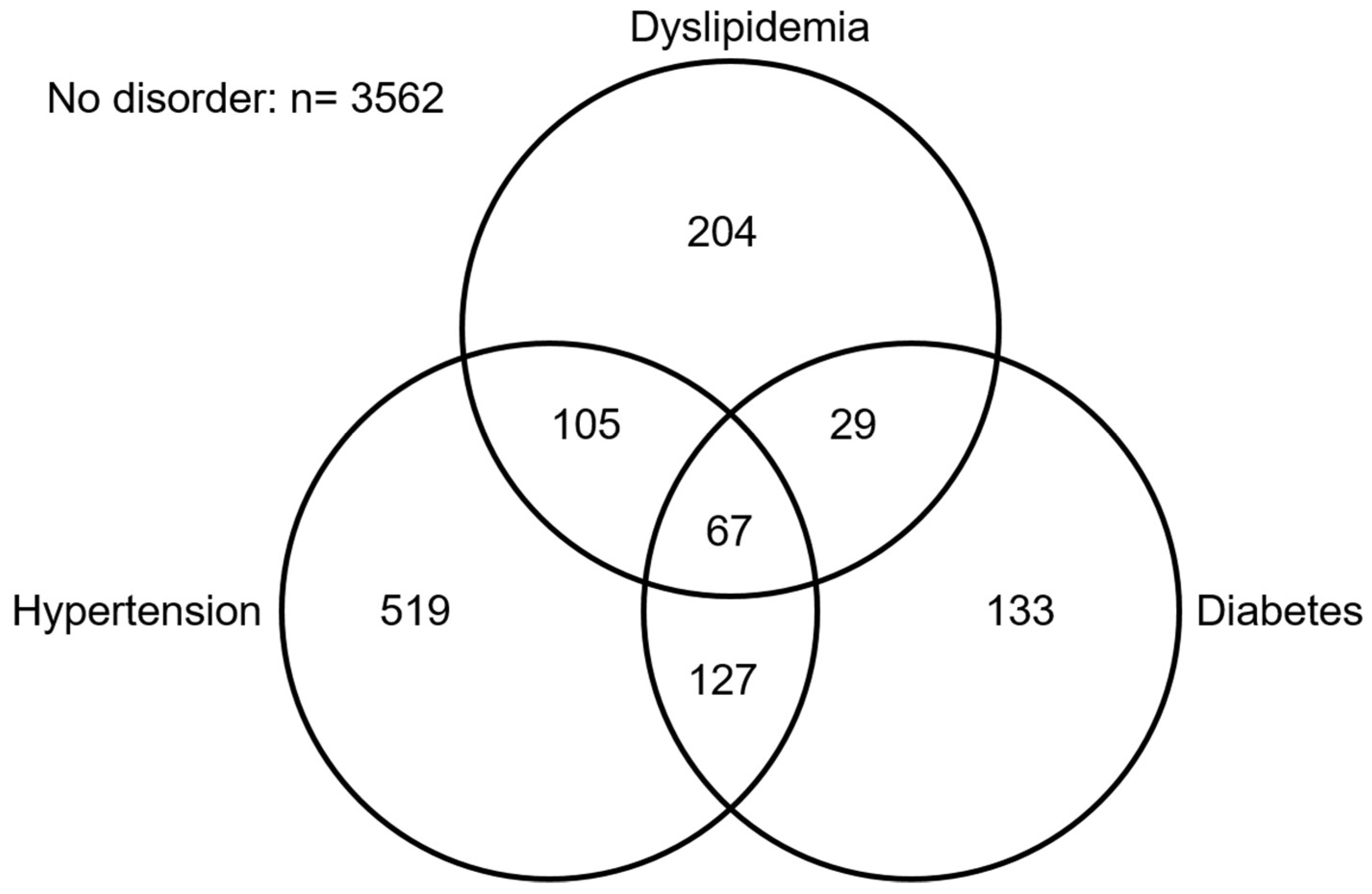
3.1. Study Population Characteristics
3.2. Factors Associated with Dyslipidemia
3.3. Factors Associated with Hypertension
3.4. Factors Associated with Diabetes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, J.; Ling, N.; Lei, Y.; Peng, M.; Hu, P.; Chen, M. Multifaceted Interaction between Hepatitis B Virus Infection and Lipid Metabolism in Hepatocytes: A Potential Target of Antiviral Therapy for Chronic Hepatitis B. Front. Microbiol. 2021, 12, 484. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.-B.; Liao, J.; Han, N.; Zhou, L.-Y.; Wang, X.-E.; Wang, Y.-J.; Tang, H. Association between Hepatitis B Virus Infection and Metabolic Syndrome in Southwest China: A Cross-sectional Study. Sci. Rep. 2020, 10, 6738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed] [Green Version]
- Li, Y.; Zhao, Y.; Wu, J. Serum HBV surface antigen positivity is associated with low prevalence of metabolic syndrome: A meta-analysis. PLoS ONE 2017, 12, e0177713. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.-W.; Lin, C.-L.; Liu, C.-J.; Yang, S.-H.; Tseng, Y.-L.; Wu, C.-F. Influence of Metabolic Risk Factors on Risk of Hepatocellular Carcinoma and Liver-Related Death in Men with Chronic Hepatitis B: A Large Cohort Study. Gastroenterology 2017, 153, 1006–1017.e5. [Google Scholar] [CrossRef] [PubMed]
- Bin Lee, Y.; Moon, H.; Lee, J.; Cho, E.J.; Yu, S.J.; Kim, Y.J.; Zoulim, F.; Lee, J.; Yoon, J. Association of Metabolic Risk Factors With Risks of Cancer and All-Cause Mortality in Patients with Chronic Hepatitis B. Hepatology 2021, 73, 2266–2277. [Google Scholar]
- Lam, L.; Fontaine, H.; Bourliere, M.; Lusivika-Nzinga, C.; Dorival, C.; Thabut, D.; Zoulim, F.; Habersetzer, F.; Asselah, T.; Duclos-Vallee, J.-C.; et al. Predictive factors for hepatocellular carcinoma in chronic hepatitis B using structural equation modeling: A prospective cohort study. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101713. [Google Scholar] [CrossRef]
- Si, J.; Yu, C.; Guo, Y.; Bian, Z.; Meng, R.; Yang, L.; Chen, Y.; Jin, J.; Liu, J.; Guo, Z.; et al. Chronic hepatitis B virus infection and total and cause-specific mortality: A prospective cohort study of 0.5 million people. BMJ Open 2019, 9, e027696. [Google Scholar] [CrossRef] [Green Version]
- Unger, L.W.; Forstner, B.; Schneglberger, S.; Muckenhuber, M.; Eigenbauer, E.; Scheiner, B.; Mandorfer, M.; Trauner, M.; Reiberger, T. Patterns and prevalence of dyslipidemia in patients with different etiologies of chronic liver disease. Wien. Klin. Wochenschr. 2019, 131, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.-A.; Shim, J.-J.; Lee, J.S.; Kim, B.-H.; Kim, J.W.; Oh, C.H.; Oh, C.-M.; Oh, I.-H.; Park, S.-Y. Effect of Statin Use on Liver Cancer Mortality Considering Hypercholesterolemia and Obesity in Patients with Non-Cirrhotic Chronic Hepatitis B. Yonsei Med. J. 2019, 60, 1203–1208. [Google Scholar] [CrossRef]
- Yang, X.; Ma, R.C.; So, W.Y.; Yu, L.W.; Kong, A.P.; Ko, G.T.; Xu, G.; Ozaki, R.; Tong, P.C.; Chan, J.C. Low triglyceride and nonuse of statins is associated with cancer in type 2 diabetes mellitus: The Hong Kong Diabetes Registry. Cancer 2011, 117, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wang, Y.; Luk, A.O.Y.; So, W.Y.; Ma, R.; Kong, A.P.S.; Xu, G.; Chan, J.C.N. Enhancers and attenuators of risk associations of chronic hepatitis B virus infection with hepatocellular carcinoma in type 2 diabetes. Endocr.-Relat. Cancer 2012, 20, 161–171. [Google Scholar] [CrossRef] [PubMed]
- de la Iglesia, R.; Loria-Kohen, V.; Zulet, M.A.; Martinez, J.A.; Reglero, G.; Ramirez de Molina, A. Dietary Strategies Implicated in the Prevention and Treatment of Metabolic Syndrome. Int. J. Mol. Sci. 2016, 17, 1877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippou, C.D.; Tsioufis, C.P.; Thomopoulos, C.G.; Mihas, C.C.; Dimitriadis, K.S.; Sotiropoulou, L.I.; Chrysochoou, C.A.; Nihoyannopoulos, P.I.; Tousoulis, D.M. Dietary Approaches to Stop Hypertension (DASH) Diet and Blood Pressure Reduction in Adults with and without Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.; Chrysoula, L.; Kotzakioulafi, E.; Theodoridis, X.; Chourdakis, M. Impact of the Level of Adherence to Mediterranean Diet on the Parameters of Metabolic Syndrome: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2021, 13, 1514. [Google Scholar] [CrossRef]
- Akhlaghi, M. Dietary Approaches to Stop Hypertension (DASH): Potential mechanisms of action against risk factors of the metabolic syndrome. Nutr. Res. Rev. 2020, 33, 1–18. [Google Scholar] [CrossRef]
- Visioli, F.; Galli, C. The role of antioxidants in the Mediterranean diet. Lipids 2001, 36, S49–S52. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Bjelakovic, M.; Nagorni, A.; Gluud, C. Antioxidant supplements for liver diseases. Cochrane Database Syst. Rev. 2011, 3, CD007749. [Google Scholar] [CrossRef]
- Ha, H.-L.; Shin, H.-J.; Feitelson, M.A.; Yu, D.-Y. Oxidative stress and antioxidants in hepatic pathogenesis. World J. Gastroenterol. 2010, 16, 6035–6043. [Google Scholar] [CrossRef]
- Alavian, S.M.; Showraki, A. Hepatitis B and its Relationship with Oxidative Stress. Hepat. Mon. 2016, 16, e37973. [Google Scholar] [CrossRef] [Green Version]
- Silva, R.F.M.; Pogačnik, L. Polyphenols from Food and Natural Products: Neuroprotection and Safety. Antioxidants 2020, 9, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Bo, C.; Bernardi, S.; Marino, M.; Porrini, M.; Tucci, M.; Guglielmetti, S.; Cherubini, A.; Carrieri, B.; Kirkup, B.; Kroon, P.; et al. Systematic Review on Polyphenol Intake and Health Outcomes: Is there Sufficient Evidence to Define a Health-Promoting Polyphenol-Rich Dietary Pattern? Nutrients 2019, 11, 1355. [Google Scholar]
- Fukushima, Y.; Tashiro, T.; Kumagai, A.; Ohyanagi, H.; Horiuchi, T.; Takizawa, K.; Sugihara, N.; Kishimoto, Y.; Taguchi, C.; Tani, M.; et al. Coffee and beverages are the major contributors to polyphenol consumption from food and beverages in Japanese middle-aged women. J. Nutr. Sci. 2014, 3, e48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nascimento-Souza, M.A.; de Paiva, P.G.; da Silva, A.; Duarte, M.S.L.; Ribeiro, A.Q. Coffee and Tea Group Contribute the Most to the Dietary Total Antioxidant Capacity of Older Adults: A Population Study in a Medium-Sized Brazilian City. J. Am. Coll. Nutr. 2020, 40, 713–723. [Google Scholar] [CrossRef]
- Cai, L.; Ma, D.; Zhang, Y.; Liu, Z.; Wang, P. The effect of coffee consumption on serum lipids: A meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 2012, 66, 872–877. [Google Scholar] [CrossRef]
- Cornelis, M.C.; van Dam, R.M. Habitual Coffee and Tea Consumption and Cardiometabolic Biomarkers in the UK Biobank: The Role of Beverage Types and Genetic Variation. J. Nutr. 2020, 150, 2772–2788. [Google Scholar] [CrossRef]
- Nerurkar, P.; Gandhi, K.; Chen, J. Correlations between Coffee Consumption and Metabolic Phenotypes, Plasma Folate, and Vitamin B12: NHANES 2003 to 2006. Nutrients 2021, 13, 1348. [Google Scholar] [CrossRef]
- Xu, R.; Yang, K.; Li, S.; Dai, M.; Chen, G. Effect of green tea consumption on blood lipids: A systematic review and meta-analysis of randomized controlled trials. Nutr. J. 2020, 19, 48. [Google Scholar] [CrossRef]
- Xie, C.; Cui, L.; Zhu, J.; Wang, K.; Sun, N.; Sun, C. Coffee consumption and risk of hypertension: A systematic review and dose–response meta-analysis of cohort studies. J. Hum. Hypertens. 2018, 32, 83–93. [Google Scholar] [CrossRef]
- Peng, X.; Zhou, R.; Wang, B.; Yu, X.; Yang, X.; Liu, K.; Mi, M. Effect of green tea consumption on blood pressure: A meta-analysis of 13 randomized controlled trials. Sci. Rep. 2014, 4, 6251. [Google Scholar] [CrossRef] [Green Version]
- Mahdavi-Roshan, M.; Salari, A.; Ghorbani, Z.; Ashouri, A. The effects of regular consumption of green or black tea beverage on blood pressure in those with elevated blood pressure or hypertension: A systematic review and meta-analysis. Complement. Ther. Med. 2020, 51, 102430. [Google Scholar] [CrossRef] [PubMed]
- Carlström, M.; Larsson, S.C. Coffee consumption and reduced risk of developing type 2 diabetes: A systematic review with meta-analysis. Nutr. Rev. 2018, 76, 395–417. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.K.; Inoue, M. Green tea and cancer and cardiometabolic diseases: A review of the current epidemiological evidence. Eur. J. Clin. Nutr. 2021, 75, 865–876. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y.; Han, G.; Hu, Y.; Bi, Y.; Li, L.; Zhu, D. Tea Consumption and Risk of Type 2 Diabetes: A Meta-Analysis of Cohort Studies. J. Gen. Intern. Med. 2009, 24, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.S.Y.; Covert, E.; Wilson, E.; Kottilil, S. Chronic Hepatitis B Infection: A Review. JAMA 2018, 319, 1802–1813. [Google Scholar] [CrossRef]
- Montuclard, C.; Hamza, S.; Rollot, F.; Evrard, P.; Faivre, J.; Hillon, P.; Di Martino, V.; Minello, A. Causes of death in people with chronic HBV infection: A population-based cohort study. J. Hepatol. 2015, 62, 1265–1271. [Google Scholar] [CrossRef]
- Pol, S.; Bourliere, M.; Lucier, S.; Hezode, C.; Dorival, C.; Larrey, D.; Bronowicki, J.-P.; Ledinghen, V.D.; Zoulim, F.; Tran, A.; et al. Safety and efficacy of daclatasvir-sofosbuvir in HCV genotype 1-mono-infected patients. J. Hepatol. 2017, 66, 39–47. [Google Scholar] [CrossRef]
- Carrieri, M.P.; Protopopescu, C.; Marcellin, F.; Wittkop, L.; Lacombe, K.; Esterle, L.; Sogni, P.; Salmon-Ceron, D. The impact of coffee consumption on fibrosis and steatosis in HIV-HCV co-infected patients. J. Hepatol. 2017, 68, 845–847. [Google Scholar] [CrossRef] [Green Version]
- Protopopescu, C.; Santos, M.; Sogni, P.; Marcellin, F.; Esterle, L.; Wittkop, L.; Rosenthal, E.; Morlat, P.; Roux, P.; de Araújo, W.; et al. Protective effect of cannabis and coffee consumption on HCV-related mortality in French HIV-HCV co-infected patients (ANRS CO13 HEPAVIH cohort). J. Hepatol. 2018, 68, S142–S143. [Google Scholar] [CrossRef]
- Ding, M.; Bhupathiraju, S.N.; Chen, M.; van Dam, R.M.; Hu, F.B. Caffeinated and Decaffeinated Coffee Consumption and Risk of Type 2 Diabetes: A Systematic Review and a Dose-Response Meta-analysis. Diabetes Care 2014, 37, 569–586. [Google Scholar] [CrossRef] [Green Version]
- Haute Autorité de Santé (French National Authority for Health). Screening Tool for Early Detection and Brief Intervention (Outil D’aide au Repérage Précoce et à L’intervention Brève). 2014. Available online: https://www.has-sante.fr/jcms/c_1795221/fr/outil-d-aide-au-reperage-precoce-et-intervention-breve-alcool-cannabis-tabac-chez-l-adulte (accessed on 24 October 2019).
- Institut National de la Statistique et des Etudes Economiques. Définition—Pauvreté Monétaire/Seuil de Pauvreté/Seuil de Pauvreté/Insee. Available online: https://www.insee.fr/fr/metadonnees/definition/c1653 (accessed on 10 December 2021).
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; SSulkowski, M.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef] [PubMed]
- García-Compeán, D.; González-González, J.A.; Lavalle-González, F.J.; González-Moreno, E.I.; Villarreal-Pérez, J.Z.; Maldonado-Garza, H.J. Current Concepts in Diabetes Mellitus and Chronic Liver Disease: Clinical Outcomes, Hepatitis C Virus Association, and Therapy. Dig. Dis. Sci. 2016, 61, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Shen, Y.; Cai, H.; Liu, Y.-M.; Qin, G. Hepatitis B virus infection status and risk of type 2 diabetes mellitus: A meta-analysis. Hepatol. Res. 2015, 45, 1100–1109. [Google Scholar] [CrossRef]
- World Health Organization. Body Mass Index—BMI. 2019. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 9 July 2019).
- Di Maso, M.; Boffetta, P.; Negri, E.; La Vecchia, C.; Bravi, F. Caffeinated Coffee Consumption and Health Outcomes in the US Population: A Dose-Response Meta-Analysis and Estimation of Disease Cases and Deaths Avoided. Adv. Nutr. 2021, 12, 1160–1176. [Google Scholar] [CrossRef]
- Hodge, A.; Lim, S.; Goh, E.; Wong, O.; Marsh, P.; Knight, V.; Sievert, W.; De Courten, B. Coffee Intake Is Associated with a Lower Liver Stiffness in Patients with Non-Alcoholic Fatty Liver Disease, Hepatitis C, and Hepatitis B. Nutrients 2017, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.L.; Chang, W.C.; Yi, C.H.; Hung, J.S.; Liu, T.T.; Lei, W.Y.; Hsu, C.S. Association of coffee consumption and liver fibrosis progression in patients with HBeAg-negative chronic hepatitis B: A 5-year population-based cohort study. J. Formos. Med. Assoc. 2019, 118, 628–635. [Google Scholar] [CrossRef]
- Du, Y.; Lv, Y.; Zha, W.; Hong, X.; Luo, Q. Effect of coffee consumption on dyslipidemia: A meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 2159–2170. [Google Scholar] [CrossRef]
- Saeed, M.; Naveed, M.; BiBi, J.; Kamboh, A.A.; Phil, L.; Chao, S. Potential nutraceutical and food additive properties and risks of coffee: A comprehensive overview. Crit. Rev. Food Sci. Nutr. 2019, 59, 3293–3319. [Google Scholar] [CrossRef]
- Farias-Pereira, R.; Park, C.-S.; Park, Y. Mechanisms of action of coffee bioactive components on lipid metabolism. Food Sci. Biotechnol. 2019, 28, 1287–1296. [Google Scholar] [CrossRef]
- Ren, Y.; Wang, C.; Xu, J.; Wang, S. Cafestol and Kahweol: A Review on Their Bioactivities and Pharmacological Properties. Int. J. Mol. Sci. 2019, 20, 4238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urgert, R.; Der Wouw, M.W.-V.; Hovenier, R.; Meyboom, S.; Beynen, A.C.; Katan, M.B. Diterpenes from coffee beans decrease serum levels of lipoprotein(a) in humans: Results from four randomised controlled trials. Eur. J. Clin. Nutr. 1997, 51, 431–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urgert, R.; Katan, M.B. THE cholesterol-raising factor from coffee beans. Annu. Rev. Nutr. 1997, 17, 305–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rendón, M.Y.; Scholz, M.B.D.S.; Bragagnolo, N. Physical characteristics of the paper filter and low cafestol content filter coffee brews. Food Res. Int. 2018, 108, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Strandhagen, E.; Thelle, D.S. Filtered coffee raises serum cholesterol: Results from a controlled study. Eur. J. Clin. Nutr. 2003, 57, 1164–1168. [Google Scholar] [CrossRef]
- Yan, L.-T.; Wang, L.-L.; Yao, J.; Yang, Y.-T.; Mao, X.-R.; Yue, W.; Mao, Y.-W.; Zhou, W.; Chen, Q.-F.; Chen, Y.; et al. Total bile acid-to-cholesterol ratio as a novel noninvasive marker for significant liver fibrosis and cirrhosis in patients with non-cholestatic chronic hepatitis B virus infection. Medicine 2020, 99, e19248. [Google Scholar] [CrossRef]
- Zhao, L.; Deng, C.; Lin, Z.; Giovannucci, E.; Zhang, X. Dietary Fats, Serum Cholesterol and Liver Cancer Risk: A Systematic Review and Meta-Analysis of Prospective Studies. Cancers 2021, 13, 1580. [Google Scholar] [CrossRef]
- Steffen, M.; Kuhle, C.; Hensrud, D.; Erwin, P.J.; Murad, M.H. The effect of coffee consumption on blood pressure and the development of hypertension: A systematic review and meta-analysis. J. Hypertens. 2012, 30, 2245–2254. [Google Scholar] [CrossRef]
- Turnbull, D.; Rodricks, J.V.; Mariano, G.F.; Chowdhury, F. Caffeine and cardiovascular health. Regul. Toxicol. Pharmacol. 2017, 89, 165–185. [Google Scholar] [CrossRef]
- Robertson, D.; Frölich, J.C.; Carr, R.K.; Watson, J.T.; Hollifield, J.W.; Shand, D.G.; Oates, J.A. Effects of Caffeine on Plasma Renin Activity, Catecholamines and Blood Pressure. N. Engl. J. Med. 1978, 298, 181–186. [Google Scholar] [CrossRef]
- Echeverri, D.; Montes, F.R.; Cabrera, M.; Galán, A.; Prieto, A. Caffeine’s Vascular Mechanisms of Action. Int. J. Vasc. Med. 2010, 2010, 834060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roshan, H.; Nikpayam, O.; Sedaghat, M.; Sohrab, G. Effects of green coffee extract supplementation on anthropometric indices, glycaemic control, blood pressure, lipid profile, insulin resistance and appetite in patients with the metabolic syndrome: A randomised clinical trial. Br. J. Nutr. 2018, 119, 250–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revuelta-Iniesta, R.; Al-Dujaili, E.A.S. Consumption of green coffee reduces blood pressure and body composition by influencing 11β-HSD1 enzyme activity in healthy individuals: A pilot crossover study using green and black coffee. BioMed Res. Int. 2014, 2014, 482704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janda, K.; Jakubczyk, K.; Baranowska-Bosiacka, I.; Kapczuk, P.; Kochman, J.; Rębacz-Maron, E.; Gutowska, I. Mineral Composition and Antioxidant Potential of Coffee Beverages Depending on the Brewing Method. Foods 2020, 9, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olechno, E.; Puścion-Jakubik, A.; Socha, K.; Zujko, M. Coffee Brews: Are They a Source of Macroelements in Human Nutrition? Foods 2021, 10, 1328. [Google Scholar] [CrossRef] [PubMed]
- Kremer, J.I.; Gömpel, K.; Bakuradze, T.; Eisenbrand, G.; Richling, E. Urinary Excretion of Niacin Metabolites in Humans after Coffee Consumption. Mol. Nutr. Food Res. 2018, 62, e1700735. [Google Scholar] [CrossRef] [Green Version]
- Baeza, G.; Sarriá, B.; Bravo, L.; Mateos, R. Polyphenol content, in vitro bioaccessibility and antioxidant capacity of widely consumed beverages. J. Sci. Food Agric. 2018, 98, 1397–1406. [Google Scholar] [CrossRef] [Green Version]
- Richelle, M.; Tavazzi, I.; Offord, E. Comparison of the Antioxidant Activity of Commonly Consumed Polyphenolic Beverages (Coffee, Cocoa, and Tea) Prepared per Cup Serving. J. Agric. Food Chem. 2001, 49, 3438–3442. [Google Scholar] [CrossRef]
- Kim, S.-A.; Joung, H.; Shin, S. Dietary pattern, dietary total antioxidant capacity, and dyslipidemia in Korean adults. Nutr. J. 2019, 18, 37. [Google Scholar] [CrossRef] [Green Version]
- Vichaibun, V.; Khananurak, K.; Sophonnithiprasert, T. Comparative analysis of plasma total antioxidant capacity in patients with hyperglycemia and hyperglycemia plus dyslipidemia. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 13, 90–94. [Google Scholar] [CrossRef]
- Villaverde, P.; Lajous, M.; Macdonald, C.-J.; Fagherazzi, G.; Bonnet, F.; Boutron-Ruault, M.-C. High dietary total antioxidant capacity is associated with a reduced risk of hypertension in French women. Nutr. J. 2019, 18, 31. [Google Scholar] [CrossRef] [PubMed]
- Rani, V.; Deep, G.; Singh, R.K.; Palle, K.; Yadav, U.C.S. Oxidative stress and metabolic disorders: Pathogenesis and therapeutic strategies. Life Sci. 2016, 148, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wan, C.; Huang, Y.; Li, M. Effects of tea consumption on metabolic syndrome: A systematic review and meta-analysis of randomized clinical trials. Phytother. Res. 2020, 34, 2857–2866. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Stepaniak, U.; Micek, A.; Topor-Mądry, R.; Pikhart, H.; Szafraniec, K.; Pająk, A. Association of daily coffee and tea consumption and metabolic syndrome: Results from the Polish arm of the HAPIEE study. Eur. J. Nutr. 2015, 54, 1129–1137. [Google Scholar] [CrossRef] [Green Version]
- Barré, T.; Nishimwe, M.L.; Protopopescu, C.; Marcellin, F.; Carrat, F.; Dorival, C.; Delarocque-Astagneau, E.; Larrey, D.; Bourlière, M.; Petrov-Sanchez, V.; et al. Cannabis use is associated with a lower risk of diabetes in chronic hepatitis C-infected patients (ANRS CO22 Hepather cohort). J. Viral Hepat. 2020, 27, 1473–1483. [Google Scholar] [CrossRef]
- Kolb, H.; Martin, S.; Kempf, K. Coffee and Lower Risk of Type 2 Diabetes: Arguments for a Causal Relationship. Nutrients 2021, 13, 1144. [Google Scholar] [CrossRef]
- Liu, D.; Zhou, L.; Zhang, X.; Zeng, Y.; Bai, L.; Wu, D.; Tang, H. Significantly Decreased Islet β Cell Function is Closely Associated with Hyperglycemia in Chronic Hepatitis B Patients. Int. J. Endocrinol. 2021, 2021, 1264707. [Google Scholar] [CrossRef]
- Kempf, K.; Herder, C.; Erlund, I.; Kolb, H.; Martin, S.; Carstensen, M.; Koenig, W.; Sundvall, J.; Bidel, S.; Kuha, S.; et al. Effects of coffee consumption on subclinical inflammation and other risk factors for type 2 diabetes: A clinical trial. Am. J. Clin. Nutr. 2010, 91, 950–957. [Google Scholar] [CrossRef] [Green Version]
- Alperet, D.J.; Rebello, S.A.; Khoo, E.Y.-H.; Tay, Z.; Seah, S.S.-Y.; Tai, B.-C.; Tai, E.S.; Emady-Azar, S.; Chou, C.J.; Darimont, C.; et al. The effect of coffee consumption on insulin sensitivity and other biological risk factors for type 2 diabetes: A randomized placebo-controlled trial. Am. J. Clin. Nutr. 2019, 111, 448–458. [Google Scholar] [CrossRef]
- Morvaridi, M.; Rayyani, E.; Jaafari, M.; Khiabani, A.; Rahimlou, M. The effect of green coffee extract supplementation on cardio metabolic risk factors: A systematic review and meta-analysis of randomized controlled trials. J. Diabetes Metab. Disord. 2020, 19, 645–660. [Google Scholar] [CrossRef]
- Craig, W.Y.; Palomaki, G.E.; Haddow, J.E. Cigarette smoking and serum lipid and lipoprotein concentrations: An analysis of published data. BMJ 1989, 298, 784–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.W.; Kim, H.J.; Min, K.; Lee, H.; Lee, S.-H.; Kim, S.; Kim, J.S.; Oh, B. The relationship between smoking cigarettes and metabolic syndrome: A cross-sectional study with non-single residents of Seoul under 40 years old. PLoS ONE 2021, 16, e0256257. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Noguchi, Y.; Fukui, T. The effects of cessation from cigarette smoking on the lipid and lipoprotein profiles: A meta-analysis. Prev. Med. 2003, 37, 283–290. [Google Scholar] [CrossRef]
- Moradinazar, M.; Pasdar, Y.; Najafi, F.; Shahsavari, S.; Shakiba, E.; Hamzeh, B.; Fakhri, N. Association between dyslipidemia and blood lipids concentration with smoking habits in the Kurdish population of Iran. BMC Public Health 2020, 20, 673. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, D.; Wang, Y. Cigarette Smoking and Adipose Tissue: The Emerging Role in Progression of Atherosclerosis. Mediat. Inflamm. 2017, 2017, 3102737. [Google Scholar] [CrossRef] [Green Version]
- Leone, A. Does Smoking Act as a Friend or Enemy of Blood Pressure? Let Release Pandora’s Box. Cardiol. Res. Pract. 2011, 2011, 264894. [Google Scholar] [CrossRef] [Green Version]
- Dikalov, S.; Itani, H.A.; Richmond, B.; Arslanbaeva, L.; Vergeade, A.; Rahman, S.M.J.; Boutaud, O.; Blackwell, T.; Massion, P.P.; Harrison, D.G.; et al. Tobacco smoking induces cardiovascular mitochondrial oxidative stress, promotes endothelial dysfunction, and enhances hypertension. Am. J. Physiol. Circ. Physiol. 2019, 316, H639–H646. [Google Scholar] [CrossRef]
- Audrain-McGovern, J.; Benowitz, N.L. Cigarette Smoking, Nicotine, and Body Weight. Clin. Pharmacol. Ther. 2011, 90, 164–168. [Google Scholar] [CrossRef] [Green Version]
- Aubin, H.-J.; Farley, A.; Lycett, D.; Lahmek, P.; Aveyard, P. Weight Gain in Smokers after Quitting Cigarettes: Meta-Analysis. BMJ 2012, 345, e4439. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3393785/ (accessed on 22 January 2020). [CrossRef] [Green Version]
- Jayedi, A.; Rashidy-Pour, A.; Khorshidi, M.; Shab-Bidar, S. Body mass index, abdominal adiposity, weight gain and risk of developing hypertension: A systematic review and dose-response meta-analysis of more than 2.3 million participants. Obes. Rev. 2018, 19, 654–667. [Google Scholar] [CrossRef]
- Braveman, P.; Gottlieb, L. The Social Determinants of Health: It’s Time to Consider the Causes of the Causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darmon, N.; Khlat, M. An overview of the health status of migrants in France, in relation to their dietary practices. Public Health Nutr. 2001, 4, 163–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, W.M.; Kelli, H.M.; Lisko, J.C.; Varghese, T.; Shen, J.; Sandesara, P.; Quyyumi, A.A.; Taylor, H.A.; Gulati, M.; Harold, J.G.; et al. Socioeconomic Status and Cardiovascular Outcomes: Challenges and Interventions. Circulation 2018, 137, 2166–2178. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.; Hosking, J.; Woodward, A.; Witten, K.; Macmillan, A.; Field, A.; Baas, P.; Mackie, H. Systematic literature review of built environment effects on physical activity and active transport—An update and new findings on health equity. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 158. [Google Scholar] [CrossRef] [PubMed]
- Rendón, M.Y.; Scholz, M.B.D.S.; Bragagnolo, N. Is cafestol retained on the paper filter in the preparation of filter coffee? Food Res. Int. 2017, 100, 798–803. [Google Scholar] [CrossRef]
- De Giuseppe, R.; Di Napoli, I.; Granata, F.; Mottolese, A.; Cena, H. Caffeine and blood pressure: A critical review perspective. Nutr. Res. Rev. 2019, 32, 169–175. [Google Scholar] [CrossRef]
- Bobková, A.; Hudáček, M.; Jakabová, S.; Belej, Ľ.; Capcarová, M.; Čurlej, J.; Bobko, M.; Árvay, J.; Jakab, I.; Čapla, J.; et al. The effect of roasting on the total polyphenols and antioxidant activity of coffee. J. Environ. Sci. Health Part B 2020, 55, 495–500. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study Population (N = 4746) N (%) | Coffee Consumption N (%) | ||||
|---|---|---|---|---|---|
| Characteristics (% of missing) | 0 cup/day | 1–2 cups/day | ≥3 cups/day | p-value | |
| Gender | |||||
| Male | 3004 (63.3) | 973 (56.6) | 1086 (62.0) | 945 (74.2) | <10−3 |
| Female | 1742 (36.7) | 746 (43.4) | 667 (38.0) | 329 (25.8) | |
| Age (years) | |||||
| <40 | 1945 (41.0) | 910 (52.9) | 643 (36.7) | 392 (30.8) | <10−3 |
| 40–49 | 1157 (24.4) | 384 (22.3) | 406 (23.2) | 367 (28.8) | |
| 50–59 | 847 (17.8) | 231 (13.4) | 317 (18.1) | 299 (23.5) | |
| ≥60 | 797 (16.8) | 194 (11.3) | 387 (22.1) | 216 (17.0) | |
| Place of birth | |||||
| France | 1377 (29.0) | 387 (22.5) | 472 (26.9) | 518 (40.7) | <10−3 |
| Europe 1 | 497 (10.5) | 103 (6.0) | 208 (11.9) | 186 (14.6) | |
| North Africa | 412 (8.7) | 83 (4.8) | 199 (11.4) | 130 (10.2) | |
| Sub-Saharan Africa 2 | 1753 (36.9) | 921 (53.6) | 557 (31.8) | 275 (21.6) | |
| Asia | 707 (14.9) | 225 (13.1) | 317 (18.1) | 165 (13.0) | |
| Body mass index (kg/m2) 3 (0.9) | |||||
| <25 (under or normal weight) | 2378 (50.6) | 889 (52.2) | 881 (50.8) | 608 (48.1) | 0.259 |
| ≥25 and <30 (overweight) | 1631 (34.7) | 566 (33.2) | 601 (34.7) | 464 (36.7) | |
| ≥30 (obese) | 693 (14.7) | 248 (14.6) | 252 (14.5) | 193 (15.3) | |
| Living in a couple (0.1) | |||||
| No | 1654 (34.9) | 703 (41.0) | 563 (32.2) | 388 (30.5) | <10−3 |
| Yes | 3086 (65.1) | 1013 (59.0) | 1188 (67.8) | 885 (69.5) | |
| Coffee consumption | |||||
| None | 1719 (36.2) | / | / | / | |
| 1–2 cups/day | 1753 (36.9) | / | / | / | |
| ≥3 cups/day | 1274 (26.8) | / | / | / | |
| Tea consumption (0.3) | |||||
| Non-daily | 2881 (60.9) | 1001 (58.3) | 1019 (58.4) | 861 (67.8) | <10−3 |
| Daily | 1851 (39.1) | 717 (41.7) | 726 (41.6) | 408 (32.2) | |
| Tea consumption (0.3) | |||||
| <3 cups/day | 4240 (89.6) | 1521 (88.5) | 1586 (90.9) | 1133 (89.3) | 0.069 |
| ≥3 cups/day | 492 (10.4) | 197 (11.5) | 159 (9.1) | 136 (10.7) | |
| Cannabis use (0.7) | |||||
| Never | 4417 (93.7) | 1637 (95.8) | 1652 (94.9) | 1128 (89.3) | <10−3 |
| Former | 176 (3.7) | 38 (2.2) | 57 (3.3) | 81 (6.4) | |
| Current | 120 (2.5) | 34 (2.0) | 32 (1.8) | 54 (4.3) | |
| Tobacco use | |||||
| Never | 3072 (64.7) | 1369 (79.6) | 1140 (65.1) | 563 (44.2) | <10−3 |
| Former | 830 (17.5) | 181 (10.5) | 338 (19.3) | 311 (24.4) | |
| Current | 843 (17.8) | 169 (9.8) | 274 (15.6) | 400 (31.4) | |
| Alcohol use (0.4) | |||||
| Abstinent without history of unhealthy use | 2711 (57.3) | 1149 (67.2) | 983 (56.3) | 579 (45.5) | <10−3 |
| Moderate use | 1750 (37.0) | 484 (28.3) | 664 (38.0) | 602 (47.3) | |
| Current or past unhealthy use | 268 (5.7) | 77 (4.5) | 100 (5.7) | 91 (7.2) | |
| Living in poverty (3.0) | |||||
| No | 2389 (51.9) | 707 (42.5) | 922 (54.1) | 760 (61.4) | <10−3 |
| Yes | 2214 (48.1) | 955 (57.5) | 781 (45.9) | 478 (38.6) | |
| Educational level (1.4) | |||||
| <upper secondary school certificate | 2283 (48.8) | 803 (47.4) | 855 (49.5) | 625 (49.8) | 0.335 |
| ≥upper secondary school certificate | 2395 (51.2) | 892 (52.6) | 872 (50.5) | 631 (50.2) | |
| Time since HBV diagnosis—in years (3.3) | |||||
| Median [IQR] | 9.2 [3.9–17.0] | 7.6 [3.2–13.7] | 9.5 [4.3–17.7] | 11.2 [4.6–19.6] | <10−3 |
| Advanced liver fibrosis 4 (11.5) | |||||
| No | 4020 (95.7) | 1450 (95.5) | 1494 (94.8) | 1076 (97.2) | 0.010 |
| Yes | 181 (4.3) | 68 (4.5) | 82 (5.2) | 31 (2.8) | |
| Dyslipidemia | |||||
| No | 4341 (91.5) | 1626 (94.6) | 1588 (90.6) | 1127 (88.5) | <10−3 |
| Yes | 405 (8.5) | 93 (5.4) | 165 (9.4) | 147 (11.5) | |
| Hypertension | |||||
| No | 3928 (82.8) | 1449 (84.3) | 1404 (80.1) | 1075 (84.4) | 0.001 |
| Yes | 818 (17.2) | 270 (15.7) | 349 (19.9) | 199 (15.6) | |
| Diabetes | |||||
| No | 4390 (92.5) | 1604 (93.3) | 1602 (91.4) | 1184 (92.9) | 0.078 |
| Yes | 356 (7.5) | 115 (6.7) | 151 (8.6) | 90 (7.1) | |
| Univariable Analysis | Multivariable Analysis (Model 1) 1 N = 4702 | Multivariable Analysis (Model 2) 1 N = 4702 | Multivariable Analysis (Model 3) 1 N = 4590 | |||||
|---|---|---|---|---|---|---|---|---|
| OR [95% CI] | p-Value | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value | |
| Gender | ||||||||
| Male | 1 | |||||||
| Female | 0.61 [0.49–0.77] | <10−3 | ||||||
| Age (years) | <10−3 | <10−3 | <10−3 | <10−3 | ||||
| <40 | 1 | 1 | 1 | 1 | ||||
| 40–49 | 2.93 [2.01–4.27] | <10−3 | 2.51 [1.72–3.69] | <10−3 | 2.51 [1.72–3.69] | <10−3 | 2.24 [1.50–3.34] | <10−3 |
| 50–59 | 8.01 [5.65–11.34] | <10−3 | 6.40 [4.47–9.15] | <10−3 | 6.40 [4.47–9.15] | <10−3 | 4.65 [3.13–6.90] | <10−3 |
| ≥60 | 9.79 [6.93–13.82] | <10−3 | 7.72 [5.38–11.09] | <10−3 | 7.72 [5.38–11.09] | <10−3 | 4.43 [2.91–6.75] | <10−3 |
| Place of birth | <10−3 | |||||||
| France | 1 | |||||||
| Europe 2 | 0.93 [0.67–1.28] | 0.641 | ||||||
| North Africa | 0.70 [0.48–1.02] | 0.063 | ||||||
| Sub-Saharan Africa 3 | 0.36 [0.27–0.47] | <10−3 | ||||||
| Asia | 0.74 [0.55–1.00] | 0.050 | ||||||
| Body mass index (kg/m2) 4 | <10−3 | <10−3 | <10−3 | |||||
| <25 (under or normal weight) | 1 | 1 | 1 | |||||
| ≥25 and <30 (overweight) | 1.76 [1.39–2.22] | <10−3 | 1.48 [1.16–1.89] | 0.001 | 1.48 [1.16–1.89] | 0.001 | ||
| ≥30 (obese) | 2.30 [1.74–3.04] | <10−3 | 1.86 [1.39–2.48] | <10−3 | 1.86 [1.39–2.48] | <10−3 | ||
| Living in a couple | ||||||||
| No | 1 | |||||||
| Yes | 1.40 [1.12–1.76] | 0.003 | ||||||
| Coffee consumption | <10−3 | 0.033 | 0.033 | 0.009 | ||||
| None | 1 | 1 | 1 | 1 | ||||
| 1–2 cups/day | 1.82 [1.40–2.36] | <10−3 | 1.28 [0.97–1.70] | 0.083 | 1.28 [0.97–1.70] | 0.083 | 1.32 [0.99–1.75] | 0.061 |
| ≥3 cups/day | 2.28 [1.74–2.99] | <10−3 | 1.49 [1.10–2.00] | 0.009 | 1.49 [1.10–2.00] | 0.009 | 1.62 [1.19–2.20] | 0.002 |
| Tea consumption | ||||||||
| Non-daily | 1 | |||||||
| Daily | 0.80 [0.64–0.99] | 0.039 | ||||||
| Tea consumption | ||||||||
| <3 cups/day | 1 | |||||||
| ≥3 cups/day | 0.94 [0.67–1.32] | 0.720 | ||||||
| Cannabis use | 0.222 | |||||||
| Never | 1 | |||||||
| Former | 1.29 [0.79–2.11] | 0.302 | ||||||
| Current | 0.56 [0.25–1.29] | 0.173 | ||||||
| Tobacco use | <10−3 | <10−3 | <10−3 | <10−3 | ||||
| Never | 1 | 1 | 1 | 1 | ||||
| Former | 2.76 [2.18–3.49] | <10−3 | 1.63 [1.26–2.11] | <10−3 | 1.63 [1.26–2.11] | <10−3 | 1.67 [1.28–2.18] | <10−3 |
| Current | 1.45 [1.10–1.91] | 0.009 | 1.47 [1.08–1.98] | 0.013 | 1.47 [1.08–1.98] | 0.013 | 1.49 [1.09–2.04] | 0.013 |
| Alcohol use | <10−3 | |||||||
| Abstinent without history of unhealthy use | 1 | |||||||
| Moderate use | 1.59 [1.29–1.97] | <10−3 | ||||||
| Current or past unhealthy use | 2.12 [1.45–3.10] | <10−3 | ||||||
| Living in poverty | ||||||||
| No | 1 | |||||||
| Yes | 0.73 [0.59–0.90] | 0.003 | ||||||
| Educational level | ||||||||
| <upper secondary school certificate | 1 | |||||||
| ≥upper secondary school certificate | 0.61 [0.49–0.75] | <10−3 | ||||||
| Time since HBV diagnosis (years) | 1.03 [1.03–1.05] | <10−3 | 1.01 [1.00–1.02] | 0.011 | ||||
| Advanced liver fibrosis 5 | ||||||||
| No | 1 | - | - | |||||
| Yes | 1.14 [0.69–1.88] | 0.598 | - | - | ||||
| Diabetes | ||||||||
| No | 1 | - | - | 1 | ||||
| Yes | 4.88 [3.76–6.33] | <10−3 | - | - | 2.61 [1.94–3.52] | <10−3 | ||
| Hypertension | ||||||||
| No | 1 | - | - | 1 | ||||
| Yes | 4.22 [3.41–5.23] | <10−3 | - | - | 2.00 [1.55–2.59] | <10−3 | ||
| Univariable Analysis | Multivariable Analysis (Model 1) 1 N = 4702 | Multivariable Analysis (Model 2) 1 N = 4702 | Multivariable Analysis (Model 3) 1 N = 4590 | |||||
|---|---|---|---|---|---|---|---|---|
| OR [95% CI] | p-Value | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value | |
| Gender | ||||||||
| Male | 1 | 1 | 1 | |||||
| Female | 0.75 [0.64–0.89] | 0.001 | 0.78 [0.63–0.95] | 0.014 | 0.79 [0.63–0.97] | 0.027 | ||
| Age (years) | <10−3 | <10−3 | <10−3 | <10−3 | ||||
| <40 | 1 | 1 | 1 | 1 | ||||
| 40–49 | 3.83 [2.84–5.17] | <10−3 | 4.02 [2.93–5.51] | <10−3 | 3.63 [2.60–5.06] | <10−3 | 3.69 [2.71–5.04] | <10−3 |
| 50–59 | 11.56 [8.71–15.35] | <10−3 | 13.02 [9.54–17.76] | <10−3 | 12.53 [9.02–17.39] | <10−3 | 10.58 [7.75–14.44] | <10−3 |
| ≥60 | 22.62 [17.11–29.91] | <10−3 | 26.58 [19.21–36.78] | <10−3 | 25.03 [17.75–35.30] | <10−3 | 21.62 [15.62–29.90] | <10−3 |
| Place of birth | <10−3 | <10−3 | <10−3 | <10−3 | ||||
| France | 1 | 1 | 1 | 1 | ||||
| Europe 2 | 0.71 [0.55–0.93] | 0.013 | 0.77 [0.57–1.05] | 0.103 | 0.74 [0.53–1.03] | 0.076 | 0.79 [0.58–1.07] | 0.126 |
| North Africa | 0.85 [0.64–1.11] | 0.231 | 0.93 [0.68–1.28] | 0.656 | 0.95 [0.68–1.31] | 0.740 | 0.85 [0.61–1.19] | 0.341 |
| Sub-Saharan Africa 3 | 0.57 [0.47–0.68] | <10−3 | 1.54 [1.20–1.98] | 0.001 | 1.55 [1.19–2.01] | 0.001 | 1.55 [1.20–1.99] | 0.001 |
| Asia | 0.54 [0.42–0.70] | <10−3 | 0.97 [0.73–1.30] | 0.861 | 1.02 [0.75–1.39] | 0.879 | 0.90 [0.68–1.21] | 0.491 |
| Body mass index (kg/m2) 4 | <10−3 | <10−3 | <10−3 | <10−3 | ||||
| <25 (under or normal weight) | 1 | 1 | 1 | 1 | ||||
| ≥25 and <30 (overweight) | 1.82 [1.52–2.17] | <10−3 | 1.56 [1.271.90] | <10−3 | 1.58 [1.27–1.95] | <10−3 | 1.44 [1.18–1.76] | <10−3 |
| ≥30 (obese) | 4.24 [3.47–5.19] | <10−3 | 3.97 [3.12–5.04] | <10−3 | 4.31 [3.36–5.55] | <10−3 | 3.25 [2.55–4.14] | <10−3 |
| Living in a couple | ||||||||
| No | 1 | |||||||
| Yes | 1.29 [1.10–1.52] | 0.002 | ||||||
| Coffee consumption | 0.001 | 0.001 | 0.004 | 0.003 | ||||
| None | 1 | 1 | 1 | 1 | ||||
| 1–2 cups/day | 1.33 [1.12–1.59] | 0.001 | 0.90 [0.73–1.11] | 0.338 | 0.91 [0.72–1.13] | 0.387 | 0.92 [0.74–1.14] | 0.425 |
| ≥3 cups/day | 0.99 [0.81–1.21] | 0.949 | 0.64 [0.50–0.82] | 0.001 | 0.65 [0.50–0.85] | 0.001 | 0.66 [0.51–0.85] | 0.001 |
| Tea consumption | ||||||||
| Non-daily | 1 | |||||||
| Daily | 0.77 [0.66–0.90] | 0.001 | ||||||
| Tea consumption | ||||||||
| <3 cups/day | 1 | |||||||
| ≥3 cups/day | 0.88 [0.68–1.14] | 0.329 | ||||||
| Cannabis use | 0.001 | |||||||
| Never | 1 | |||||||
| Former | 0.59 [0.37–0.95] | 0.028 | ||||||
| Current | 0.33 [0.16–0.68] | 0.002 | ||||||
| Tobacco use | <10−3 | 0.013 | 0.018 | 0.007 | ||||
| Never | 1 | 1 | 1 | 1 | ||||
| Former | 2.20 [1.84–2.63] | <10−3 | 1.19 [0.95–1.48] | 0.125 | 1.21 [0.96–1.52] | 0.111 | 1.26 [1.01–1.56] | 0.038 |
| Current | 0.63 [0.49–0.80] | <10−3 | 0.75 [0.57–1.00] | 0.047 | 0.76 [0.56–1.02] | 0.070 | 0.78 [0.59–1.03] | 0.083 |
| Alcohol use | <10−3 | |||||||
| Abstinent without history of unhealthy use | 1 | |||||||
| Moderate use | 1.26 [1.07–1.48] | 0.005 | ||||||
| Current or past unhealthy use | 2.42 [1.83–3.21] | <10−3 | ||||||
| Living in poverty | ||||||||
| No | 1 | |||||||
| Yes | 0.92 [0.78–1.07] | 0.258 | ||||||
| Educational level | ||||||||
| <upper secondary school certificate | 1 | 1 | 1 | |||||
| ≥upper secondary school certificate | 0.56 [0.48–0.65] | <10−3 | 0.81 [0.67–0.96] | 0.017 | 0.81 [0.67–0.98] | 0.031 | ||
| Time since HBV diagnosis—(years) | ||||||||
| Advanced liver fibrosis 5 | 1.03 [1.02–1.04] | <10−3 | ||||||
| No | 1 | 1 | ||||||
| Yes | 3.45 [2.54–4.70] | <10−3 | - | 1.50 [1.05–2.13] | 0.024 | - | ||
| Diabetes | - | - | ||||||
| No | 1 | - | - | 1 | ||||
| Yes | 7.23 [5.77–9.05] | <10−3 | - | - | 2.93 [2.23–3.84] | <10−3 | ||
| Hypertension | ||||||||
| No | 1 | - | - | 1 | ||||
| Yes | 4.22 [3.40–5.23] | <10−3 | - | - | 1.98 [1.52–2.57] | <10−3 | ||
| Univariable Analysis | Multivariable Analysis (Model 1) 1 N = 4702 | Multivariable Analysis (Model 2) 1 N = 4702 | Multivariable Analysis (Model 3) 1 N = 4590 | |||||
|---|---|---|---|---|---|---|---|---|
| OR [95% CI] | p- Value | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value | |
| Gender | ||||||||
| Male | 1 | 1 | ||||||
| Female | 0.75 [0.59–0.94] | 0.014 | 0.75 [0.58–0.98] | 0.032 | ||||
| Age (years) | <10−3 | <10−3 | <10−3 | <10−3 | ||||
| <40 | 1 | 1 | 1 | 1 | ||||
| 40–49 | 2.74 [1.82–4.15] | <10−3 | 2.60 [1.68–4.02] | <10−3 | 2.59 [1.62–4.14] | <10−3 | 2.15 [1.38–3.35] | 0.001 |
| 50–59 | 7.49 [5.13–10.94] | <10−3 | 7.86 [5.22–11.83] | <10−3 | 7.79 [5.07–11.99] | <10−3 | 4.81 [3.10–7.44] | <10−3 |
| ≥60 | 11.44 [7.93–16.53] | <10−3 | 12.73 [8.34–19.43] | <10−3 | 11.71 [7.57–18.12] | <10−3 | 6.41 [4.04–10.17] | <10−3 |
| Place of birth | <10−3 | 0.048 | 0.016 | |||||
| France | 1 | 1 | 1 | |||||
| Europe 2 | 1.14 [0.78–1.64] | 0.501 | 1.20 [0.80–1.80] | 0.387 | 1.25 [0.82–1.92] | 0.299 | ||
| North Africa | 1.85 [1.31–2.61] | 0.001 | 1.67 [1.11–2.50] | 0.014 | 1.91 [1.27–2.87] | 0.002 | ||
| Sub-Saharan Africa 3 | 0.74 [0.56–0.98] | 0.037 | 1.39 [0.99–1.95] | 0.056 | 1.42 [1.00–2.02] | 0.051 | ||
| Asia | 0.91 [0.64–1.29] | 0.607 | 1.64 [1.11–2.42] | 0.013 | 1.67 [1.11–2.50] | 0.013 | ||
| Body mass index (kg/m2) 4 | <10−3 | <10−3 | <10−3 | <10−3 | ||||
| <25 (under or normal weight) | 1 | 1 | 1 | 1 | ||||
| ≥25 and <30 (overweight) | 2.87 [2.17–3.79] | <10−3 | 2.41 [1.78–3.25] | <10−3 | 2.14 [1.57–2.92] | <10−3 | 2.23 [1.64–3.04] | <10−3 |
| ≥30 (obese) | 6.06 [4.51–8.14] | <10−3 | 5.13 [3.67–7.17] | <10−3 | 5.02 [3.61–6.99] | <10−3 | 3.73 [2.63–5.27] | <10−3 |
| Living in a couple | ||||||||
| No | 1 | |||||||
| Yes | 0.94 [0.75–1.18] | 0.581 | ||||||
| Coffee consumption | 0.079 | |||||||
| None | 1 | |||||||
| 1–2 cups/day | 1.31 [1.02–1.69] | 0.034 | ||||||
| ≥ 3 cups/day | 1.06 [0.80–1.41] | 0.689 | ||||||
| Tea consumption | ||||||||
| Non-daily | 1 | |||||||
| Daily | 0.83 [0.67–1.05] | 0.117 | ||||||
| Tea consumption | ||||||||
| <3 cups/day | 1 | |||||||
| ≥3 cups/day | 0.72 [0.49–1.07] | 0.109 | ||||||
| Cannabis use | 0.080 | |||||||
| Never | 1 | |||||||
| Former | 0.71 [0.37–1.37] | 0.311 | ||||||
| Current | 0.30 [0.10–0.96] | 0.043 | ||||||
| Tobacco use | <10−3 | |||||||
| Never | 1 | |||||||
| Former | 1.79 [1.39–2.31] | <10−3 | ||||||
| Current | 0.82 [0.59–1.13] | 0.225 | ||||||
| Alcohol use | <10−3 | 0.024 | 0.011 | |||||
| Abstinent without history of unhealthy use | 1 | 1 | 1 | |||||
| Moderate use | 0.80 [0.63–1.02] | 0.076 | 0.75 [0.57–0.99] | 0.041 | 0.73 [0.55–0.97] | 0.030 | ||
| Current or past unhealthy use | 2.21 [1.54–3.17] | <10−3 | 1.29 [0.84–1.96] | 0.240 | 1.37 [0.89–2.10] | 0.152 | ||
| Living in poverty | ||||||||
| No | 1 | 1 | 1 | 1 | ||||
| Yes | 1.32 [1.06–1.65] | 0.013 | 1.52 [1.17–1.98] | 0.002 | 1.73 [1.33–2.25] | <10−3 | 1.44 [1.10–1.88] | 0.008 |
| Educational level | ||||||||
| <upper secondary school certificate | 1 | |||||||
| ≥upper secondary school certificate | 0.53 [0.42–0.66] | <10−3 | ||||||
| Time since HBV diagnosis (years) | 1.00 [0.99–1.01] | 0.989 | ||||||
| Advanced liver fibrosis 5 | ||||||||
| No | 1 | - | 1 | - | ||||
| Yes | 3.60 [2.48–5.23] | <10−3 | - | 2.14 [1.40–3.28] | <10−3 | - | ||
| Diabetes | ||||||||
| No | 1 | - | - | 1 | ||||
| Yes | 7.23 [5.77–9.05] | <10−3 | - | - | 2.99 [2.28–3.92] | <10−3 | ||
| Hypertension | ||||||||
| No | 1 | - | - | 1 | ||||
| Yes | 4.88 [3.76–6.33] | <10−3 | - | - | 2.49 [1.84–3.38] | <10−3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barré, T.; Fontaine, H.; Pol, S.; Ramier, C.; Di Beo, V.; Protopopescu, C.; Marcellin, F.; Bureau, M.; Bourlière, M.; Dorival, C.; et al. Metabolic Disorders in Patients with Chronic Hepatitis B Virus Infection: Coffee as a Panacea? (ANRS CO22 Hepather Cohort). Antioxidants 2022, 11, 379. https://doi.org/10.3390/antiox11020379
Barré T, Fontaine H, Pol S, Ramier C, Di Beo V, Protopopescu C, Marcellin F, Bureau M, Bourlière M, Dorival C, et al. Metabolic Disorders in Patients with Chronic Hepatitis B Virus Infection: Coffee as a Panacea? (ANRS CO22 Hepather Cohort). Antioxidants. 2022; 11(2):379. https://doi.org/10.3390/antiox11020379
Chicago/Turabian StyleBarré, Tangui, Hélène Fontaine, Stanislas Pol, Clémence Ramier, Vincent Di Beo, Camelia Protopopescu, Fabienne Marcellin, Morgane Bureau, Marc Bourlière, Céline Dorival, and et al. 2022. "Metabolic Disorders in Patients with Chronic Hepatitis B Virus Infection: Coffee as a Panacea? (ANRS CO22 Hepather Cohort)" Antioxidants 11, no. 2: 379. https://doi.org/10.3390/antiox11020379