
AGEs and sRAGE Variations at Different Timepoints in Patients with Chronic Kidney Disease

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. sRAGE, esRAGE and cRAGE Quantification
2.3. AGE Quantification
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Metabolic and Renal Function Parameters at Baseline and Follow-Up (FU)
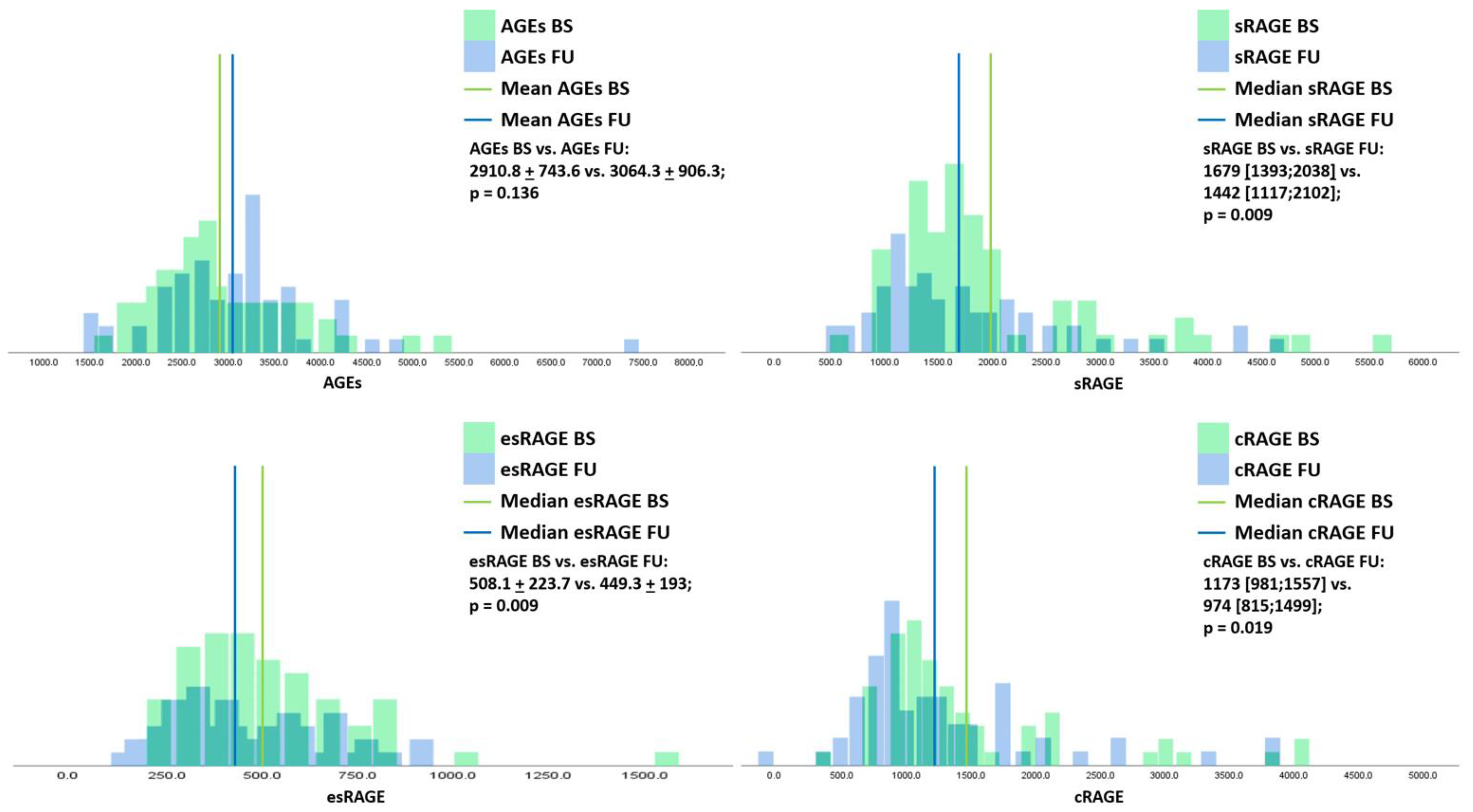
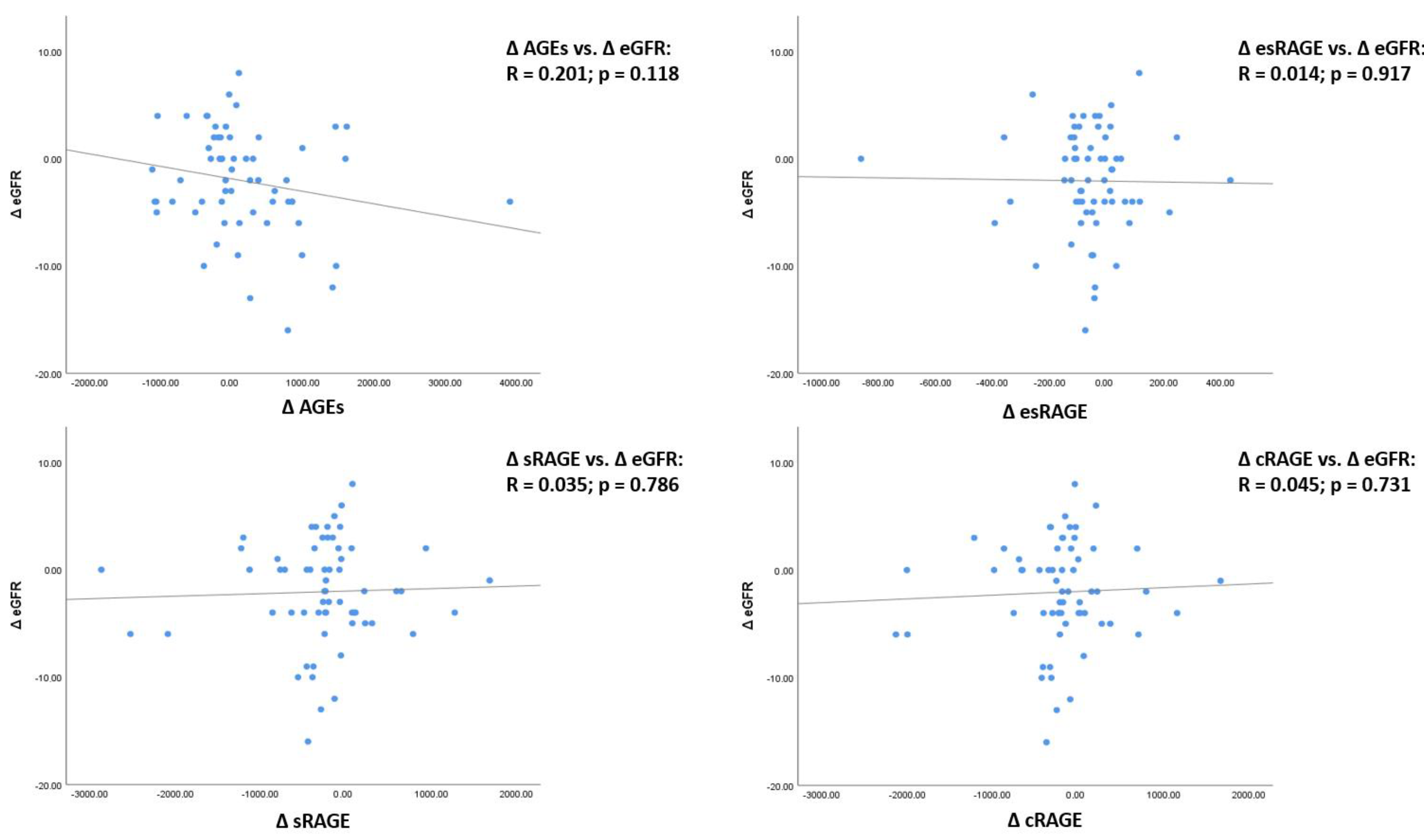
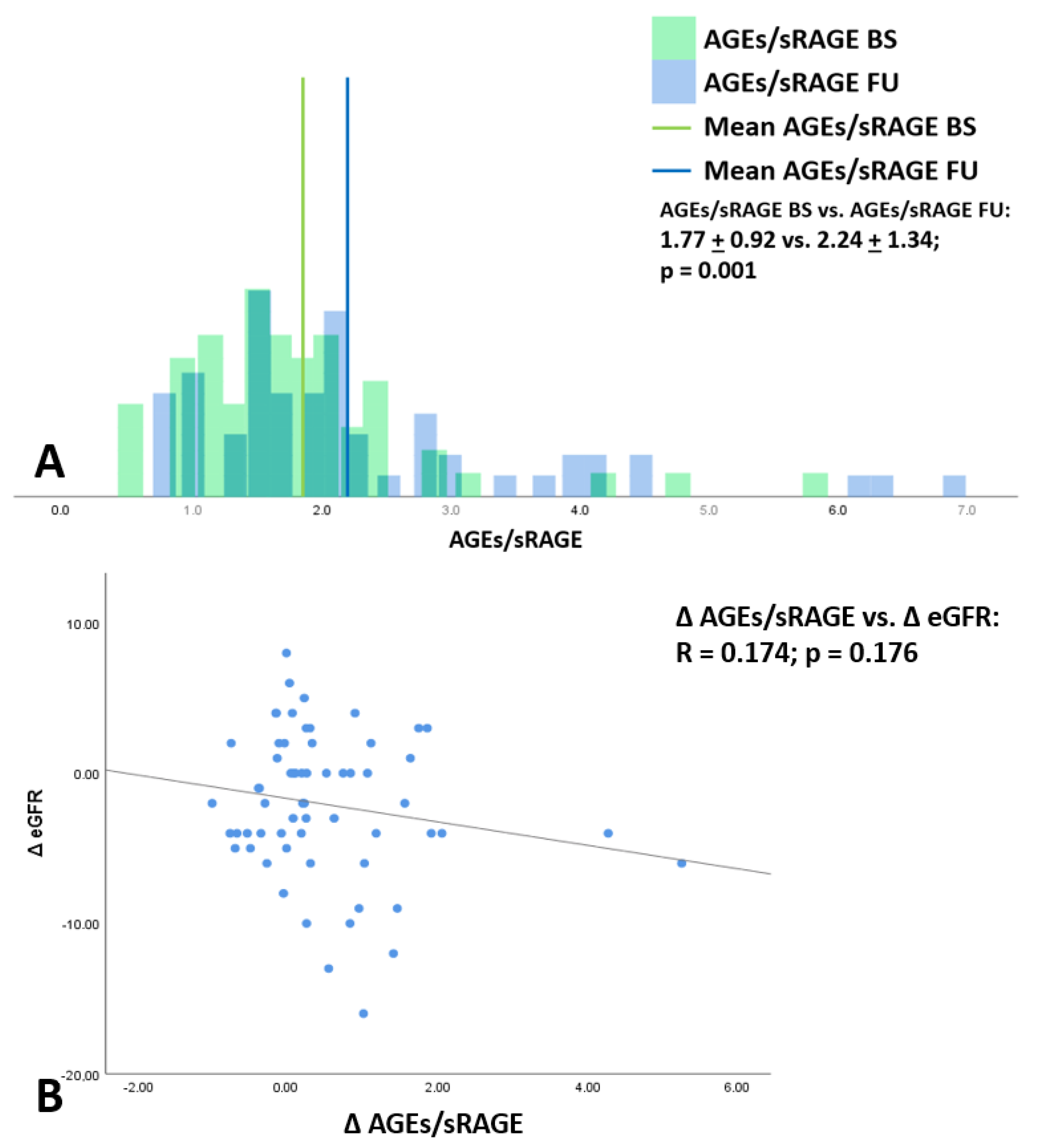
3.3. Changes of AGEs, sRAGE and Its Isoforms, and AGEs/sRAGE Ratio from Baseline to Follow-Up and Their Association with eGFR Variations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmed, N. Advanced glycation endproducts--role in pathology of diabetic complications. Diabetes Res. Clin. Pract. 2005, 67, 3–21. [Google Scholar] [CrossRef]
- Goldin, A.; Beckman, J.A.; Schmidt, A.M.; Creager, M.A. Advanced glycation end products: Sparking the development of diabetic vascular injury. Circulation 2006, 114, 597–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dozio, E.; Vettoretti, S.; Lungarella, G.; Messa, P.; Romanelli, M.M.C. Sarcopenia in Chronic Kidney Disease: Focus on Advanced Glycation End Products as Mediators and Markers of Oxidative Stress. Biomedicines 2021, 9, 405. [Google Scholar] [CrossRef] [PubMed]
- Bucala, R.; Vlassara, H. Advanced glycosylation end products in diabetic renal and vascular disease. Am. J. Kidney Dis. 1995, 26, 875–888. [Google Scholar] [CrossRef]
- Shimoike, T.; Inoguchi, T.; Umeda, F.; Nawata, H.; Kawano, K.; Ochi, H. The meaning of serum levels of advanced glycosylation end products in diabetic nephropathy. Metabolism 2000, 49, 1030–1035. [Google Scholar] [CrossRef]
- Tezuka, Y.; Nakaya, I.; Nakayama, K.; Nakayama, M.; Yahata, M.; Soma, J. Methylglyoxal as a prognostic factor in patients with chronic kidney disease. Nephrology 2019, 24, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Dozio, E.; Vettoretti, S.; Caldiroli, L.; Nerini-Molteni, S.; Tacchini, L.; Ambrogi, F.; Messa, P.; Romanelli, M.M.C. Advanced Glycation End Products (AGE) and Soluble Forms of AGE Receptor: Emerging Role as Mortality Risk Factors in CKD. Biomedicines 2020, 8, 638. [Google Scholar] [CrossRef]
- Calviño, J.; Cigarran, S.; Gonzalez-Tabares, L.; Menendez, N.; Latorre, J.; Cillero, S.; Millan, B.; Cobelo, C.; Sanjurjo-Amado, A.; Quispe, J.; et al. Advanced glycation end products (AGEs) estimated by skin autofluorescence are related with cardiovascular risk in renal transplant. PLoS ONE 2018, 13, e0201118. [Google Scholar] [CrossRef] [Green Version]
- Liebisch, M.; Bondeva, T.; Franke, S.; Daniel, C.; Amann, K.; Wolf, G. Activation of the receptor for advanced glycation end products induces nuclear inhibitor of protein phosphatase-1 suppression. Kidney Int. 2014, 86, 103–117. [Google Scholar] [CrossRef] [Green Version]
- Schlueter, C.; Hauke, S.; Flohr, A.M.; Rogalla, P.; Bullerdiek, J. Tissue-specific expression patterns of the RAGE receptor and its soluble forms--a result of regulated alternative splicing? Biochim. Biophys. Acta 2003, 1630, 1–6. [Google Scholar] [CrossRef]
- Lazo, M.; Halushka, M.K.; Shen, L.; Maruthur, N.; Rebholz, C.M.; Rawlings, A.; Hoogeveen, R.; Brinkley, T.E.; Ballantyne, C.M.; Astor, B.C.; et al. sRAGE and the risk for incident heart failure: The Atherosclerosis Risk in Communities Study. Am. Heart J. 2015, 170, 961–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dozio, E.; Ambrogi, F.; de Cal, M.; Vianello, E.; Ronco, C.; Romanelli, M.M.C. Role of the Soluble Receptor for Advanced Glycation End Products (sRAGE) as a Prognostic Factor for Mortality in Hemodialysis and Peritoneal Dialysis Patients. Mediat. Inflamm. 2018, 2018, 1347432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebholz, C.M.; Astor, B.C.; Grams, M.E.; Halushka, M.; Lazo, M.; Hoogetveen, R.; Ballantyne, C.M.; Coresh, J.; Selvin, E. Association of plasma levels of soluble receptor for advanced glycation end products and risk of kidney disease: The Atherosclerosis Risk in Communities study. Nephrol. Dial. Transplant. 2015, 30, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Yanagisawa, K.; Makita, Z.; Shiroshita, K.; Ueda, T.; Fusegawa, T.; Kuwajima, S.; Takeuchi, M.; Koike, T. Specific fluorescence assay for advanced glycation end products in blood and urine of diabetic patients. Metabolism 1998, 47, 1348–1353. [Google Scholar] [CrossRef]
- Guerin-Dubourg, A.; Cournot, M.; Planesse, C.; Debussche, X.; Meilhac, O.; Rondeau, P.; Bourdon, E. Association between Fluorescent Advanced Glycation End-Products and Vascular Complications in Type 2 Diabetic Patients. Biomed. Res. Int. 2017, 2017. [Google Scholar] [CrossRef]
- Boer, I.H.D.; Bakris, G.L. Diabetic Kidney Disease: A Determinant of Cardiovascular Risk in Type 1 Diabetes. Diabetes Care 2018, 41, 662–663. [Google Scholar] [CrossRef] [Green Version]
- Giacco, F.; Brownlee, M. Oxidative stress and diabetic complications. Circ. Res. 2010, 107, 1058–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda-Díaz, A.G.; Pazarín-Villaseñor, L.; Yanowsky-Escatell, F.G.; Andrade-Sierra, J. Oxidative Stress in Diabetic Nephropathy with Early Chronic Kidney Disease. J. Diabetes Res. 2016, 2016, 7047238. [Google Scholar] [CrossRef] [Green Version]
- Kamiński, T.W.; Pawlak, K.; Karbowska, M.; Myśliwiec, M.; Pawlak, D. Indoxyl sulfate—The uremic toxin linking hemostatic system disturbances with the prevalence of cardiovascular disease in patients with chronic kidney disease. BMC Nephrol. 2017, 18, 35. [Google Scholar] [CrossRef] [Green Version]
- Dozio, E.; Massaccesi, L.; Romanelli, M.M.C. Glycation and Glycosylation in Cardiovascular Remodeling: Focus on Advanced Glycation End Products and O-Linked Glycosylations as Glucose-Related Pathogenetic Factors and Disease Markers. J. Clin. Med. 2021, 10, 4792. [Google Scholar] [CrossRef]
- Alpert, M.A. Cardiac performance and morphology in end-stage renal disease. Am. J. Med. Sci. 2003, 325, 168–178. [Google Scholar] [CrossRef]
- Muntner, P.; He, J.; Astor, B.C.; Folsom, A.R.; Coresh, J. Traditional and nontraditional risk factors predict coronary heart disease in chronic kidney disease: Results from the atherosclerosis risk in communities study. J. Am. Soc. Nephrol. 2005, 16, 529–538. [Google Scholar] [CrossRef] [Green Version]
- Ratliff, B.B.; Abdulmahdi, W.; Pawar, R.; Wolin, M.S. Oxidant Mechanisms in Renal Injury and Disease. Antioxid. Redox Signal. 2016, 25, 119–146. [Google Scholar] [CrossRef] [Green Version]
- Mendoza, M.G.A.; Castillo-Henkel, C.; Medina-Santillan, R.; Luna, R.A.J.; Robles, H.V.; Romo, E.; Rios, A.; Escalante, B. Kidney damage after renal ablation is worsened in endothelial nitric oxide synthase -/- mice and improved by combined administration of L-arginine and antioxidants. Nephrology 2008, 13, 218–227. [Google Scholar] [CrossRef]
- Fujimoto, S.; Satoh, M.; Horike, H.; Hatta, H.; Haruna, Y.; Kobayashi, S.; Namikoshi, T.; Arakawa, S.; Tomita, N.; Kashihara, N. Olmesartan ameliorates progressive glomerular injury in subtotal nephrectomized rats through suppression of superoxide production. Hypertens. Res. 2008, 31, 305–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberg, B.P.; McMenamin, E.; Lucas, F.L.; McMonagle, E.; Morrow, J.; Ikizler, T.A.; Himmelfarb, J. Increased prevalence of oxidant stress and inflammation in patients with moderate to severe chronic kidney disease. Kidney Int. 2004, 65, 1009–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stinghen, A.E.; Massy, Z.A.; Vlassara, H.; Striker, G.E.; Boullier, A. Uremic Toxicity of Advanced Glycation End Products in CKD. J. Am. Soc. Nephrol. 2016, 27, 354–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yabuuchi, J.; Ueda, S.; Yamagishi, S.I.; Nohara, N.; Nagasawa, H.; Wakabayashi, K.; Matsui, T.; Yuichiro, H.; Kadoguchi, T.; Otsuka, T.; et al. Association of advanced glycation end products with sarcopenia and frailty in chronic kidney disease. Sci. Rep. 2020, 10, 17647. [Google Scholar] [CrossRef]
- Rabbani, N.; Thornalley, P.J. Advanced glycation end products in the pathogenesis of chronic kidney disease. Kidney Int. 2018, 93, 803–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, K.; Nakayama, M.; Kanno, M.; Kimura, H.; Watanabe, K.; Tani, Y.; Kusano, Y.; Suzuki, H.; Hayashi, Y.; Asahi, K.; et al. Skin autofluorescence is associated with the progression of chronic kidney disease: A prospective observational study. PLoS ONE 2013, 8, e83799. [Google Scholar] [CrossRef] [Green Version]
- Yan, L.; Mathew, L.; Chellan, B.; Gardner, B.; Earley, J.; Puri, T.S.; Hofmann Bowman, M.A. S100/Calgranulin-mediated inflammation accelerates left ventricular hypertrophy and aortic valve sclerosis in chronic kidney disease in a receptor for advanced glycation end products-dependent manner. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1399–1411. [Google Scholar] [CrossRef] [Green Version]
- Shardlow, A.; McIntyre, N.J.; Kolhe, N.V.; Nellums, L.B.; Fluck, R.J.; McIntyre, C.W.; Taal, M.W. The association of skin autofluorescence with cardiovascular events and all-cause mortality in persons with chronic kidney disease stage 3: A prospective cohort study. PLoS Med. 2020, 17, e1003163. [Google Scholar] [CrossRef]
- Vettoretti, S.; Caldiroli, L.; Armelloni, S.; Ferrari, C.; Cesari, M.; Messa, P. Sarcopenia is associated with malnutrition but not with systemic inflammation in older persons with advanced CKD. Nutrients 2019, 11, 1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aleshin, A.; Ananthakrishnan, R.; Li, Q.; Rosario, R.; Lu, Y.; Qu, W.; Song, F.; Bakr, S.; Szabolcs, M.; D’Agati, V.; et al. RAGE modulates myocardial injury consequent to LAD infarction via impact on JNK and STAT signaling in a murine model. Am. J. Physiol. Heart Circ. Physiol. 2008, 294, H1823–H1832. [Google Scholar] [CrossRef]
- Sakaguchi, T.; Yan, S.F.; Yan, S.D.; Belov, D.; Rong, L.L.; Sousa, M.; Andrassy, M.; Marso, S.P.; Duda, S.; Arnold, B.; et al. Central role of RAGE-dependent neointimal expansion in arterial restenosis. J. Clin. Investig. 2003, 111, 959–972. [Google Scholar] [CrossRef] [Green Version]
- Wendt, T.M.; Tanji, N.; Guo, J.; Kislinger, T.R.; Qu, W.; Lu, Y.; Bucciarelli, L.G.; Rong, L.L.; Moser, B.; Markowitz, G.S.; et al. RAGE drives the development of glomerulosclerosis and implicates podocyte activation in the pathogenesis of diabetic nephropathy. Am. J. Pathol. 2003, 162, 1123–1137. [Google Scholar] [CrossRef] [Green Version]
- Falcone, C.; Emanuele, E.; D’Angelo, A.; Buzzi, M.P.; Belvito, C.; Cuccia, M.; Geroldi, D. Plasma levels of soluble receptor for advanced glycation end products and coronary artery disease in nondiabetic men. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1032–1037. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.K.; Park, S.; Lee, M.J.; Song, Y.R.; Han, S.H.; Kim, S.G.; Kang, S.W.; Choi, K.H.; Kim, H.J.; Yoo, T.H. Plasma levels of soluble receptor for advanced glycation end products (sRAGE) and proinflammatory ligand for RAGE (EN-RAGE) are associated with carotid atherosclerosis in patients with peritoneal dialysis. Atherosclerosis 2012, 220, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.N.; Park, S.; Lee, M.J.; Song, Y.R.; Han, S.H.; Kim, S.G.; Kang, S.W.; Choi, K.H.; Kim, H.J.; Yoo, T.H. The association of low muscle mass with soluble receptor for advanced glycation end products (sRAGE): The Korean Sarcopenic Obesity Study (KSOS). Diabetes Metab. Res. Rev. 2018, 34, e2974. [Google Scholar] [CrossRef]
- Geroldi, D.; Falcone, C.; Emanuele, E.; D’Angelo, A.; Calcagnino, M.; Buzzi, M.P.; Scioli, G.A.; Fogari, R. Decreased plasma levels of soluble receptor for advanced glycation end-products in patients with essential hypertension. J. Hypertens. 2005, 23, 1725–1729. [Google Scholar] [CrossRef]
- Smith, D.J.; Yerkovich, S.T.; Towers, M.A.; Carroll, M.L.; Thomas, R.; Upham, J.W. Reduced soluble receptor for advanced glycation end-products in COPD. Eur. Respir. J. 2011, 37, 516–522. [Google Scholar] [CrossRef] [Green Version]
- Caspar-Bell, G.; Dhar, I.; Prasad, K. Advanced glycation end products (AGEs) and its receptors in the pathogenesis of hyperthyroidism. Mol. Cell. Biochem. 2016, 414, 171–178. [Google Scholar] [CrossRef]
- Nin, J.W.; Jorsal, A.; Ferreira, I.; Schalkwijk, C.G.; Prins, M.H.; Parving, H.H.; Tarnow, L.; Rossing, P.; Stehouwer, C.D. Higher plasma soluble Receptor for Advanced Glycation End Products (sRAGE) levels are associated with incident cardiovascular disease and all-cause mortality in type 1 diabetes: A 12-year follow-up study. Diabetes 2010, 59, 2027–2032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujisawa, K.; Katakami, N.; Kaneto, H.; Naka, T.; Takahara, M.; Sakamoto, F.; Irie, Y.; Miyashita, K.; Kubo, F.; Yasuda, T.; et al. Circulating soluble RAGE as a predictive biomarker of cardiovascular event risk in patients with type 2 diabetes. Atherosclerosis 2013, 227, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Kalousová, M.; Hodková, M.; Kazderová, M.; Fialová, J.; Tesar, V.; Dusilová-Sulková, S.; Zima, T. Soluble receptor for advanced glycation end products in patients with decreased renal function. Am. J. Kidney Dis. 2006, 47, 406–411. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Overall Cohort (n = 64) |
|---|---|
| General characteristics | |
| Age, (years) | 81 [75;85] |
| Males, n (%) | 45 (70) |
| Diabetes, n (%) | 40 (63) |
| Hypertension n (%) | 58 (91) |
| eGFR, (mL/min/1.73 m2) | 27 ± 10 |
| Prot-U 24 h (g/24 h) | 440 [201;1037] |
| BMI (kg/m2) | 28.4 ± 4.6 |
| Waist circumference, (cm) | 98 [93;103] |
| Arterial systolic pressure (mmHg) | 137 [127;145] |
| Arterial dyastolic pressure | 78 [67;85] |
| Metabolic characteristics | |
| Uric Acid (mg/dL) | 6.0 ± 1.4 |
| HbA1c (mmol/dL) | 49 ± 12 |
| Fasting blood Glucose (mg/dL) | 105 [91;144] |
| Total Cholesterol (mg/dL) | 162 ± 27 |
| HDL-Cholesterol (mg/dL) | 47 [40;58] |
| LDL-Cholesterol (mg/dL) | 81 [71;100] |
| Triglycerides (mg/dL) | 120 [100;162] |
| Albumin (g/dL) | 4 ± 0.4 |
| AGEs and RAGEs | |
| AGEs (arbitrary unit) | 3033 ± 789 |
| sRAGE (pg/mL) | 1341 [1453;2858] |
| esRAGE (pg/mL) | 508 ± 224 |
| cRAGE (pg/mL) | 1173 [982;1557] |
| AGEs/sRAGE (arbitrary unit) | 1.7 ± 0.9 |
| Lost at Follow-up (global cohort n = 132) | |
| Dialysis n (%) | 24 (17) |
| Death n (%) | 10 (7) |
| Variables | Overall Cohort Baseline (n = 64) | Overall Cohort Follow-Up (n = 64) | p |
|---|---|---|---|
| eGFR, (mL/min) | 27 ± 10 | 24 ± 9 | 0.004 |
| Prot-U 24 h (g/24 h) | 440 [201;1037] | 300 [166;882] | 0.288 |
| Arterial systolic pressure (mmHg) | 138 [127;145] | 140 [127;150] | 0.371 |
| Arterial dyastolic pressure (mmHg) | 78 [67;85] | 80 [70;85] | 0.942 |
| Fasting blood Glucose (mg/dL) | 105 [91;144] | 106 [91;142] | 0.02 |
| Albumin (g/dL) | 4.1 ± 0.28 | 4 ± 0.29 | 0.28 |
| Uric Acid (mg/dL) | 6 ± 1.4 | 6.7 ± 7.9 | 0.41 |
| Total Cholesterol (mg/dL) | 162 ± 27 | 159 ± 31 | 0.47 |
| HDL-Cholesterol (mg/dL) | 47 [40;58] | 45 [38;60] | 0.26 |
| LDL-Cholesterol (mg/dL) | 81 [71;100] | 81 [63;99] | 0.18 |
| Triglycerides (mg/dL) | 120 [100;162] | 133 [91;174] | 0.09 |
| HbA1c (mmol/dL) | 49 ± 12 | 49 ± 12 | 0.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molinari, P.; Caldiroli, L.; Dozio, E.; Rigolini, R.; Giubbilini, P.; Romanelli, M.M.C.; Messa, P.; Vettoretti, S. AGEs and sRAGE Variations at Different Timepoints in Patients with Chronic Kidney Disease. Antioxidants 2021, 10, 1994. https://doi.org/10.3390/antiox10121994
Molinari P, Caldiroli L, Dozio E, Rigolini R, Giubbilini P, Romanelli MMC, Messa P, Vettoretti S. AGEs and sRAGE Variations at Different Timepoints in Patients with Chronic Kidney Disease. Antioxidants. 2021; 10(12):1994. https://doi.org/10.3390/antiox10121994
Chicago/Turabian StyleMolinari, Paolo, Lara Caldiroli, Elena Dozio, Roberta Rigolini, Paola Giubbilini, Massimiliano M. Corsi Romanelli, Piergiorgio Messa, and Simone Vettoretti. 2021. "AGEs and sRAGE Variations at Different Timepoints in Patients with Chronic Kidney Disease" Antioxidants 10, no. 12: 1994. https://doi.org/10.3390/antiox10121994