Peer Victimization and Onset of Social Anxiety Disorder in Children and Adolescents


Abstract
:
1. Introduction
2. Materials and Methods
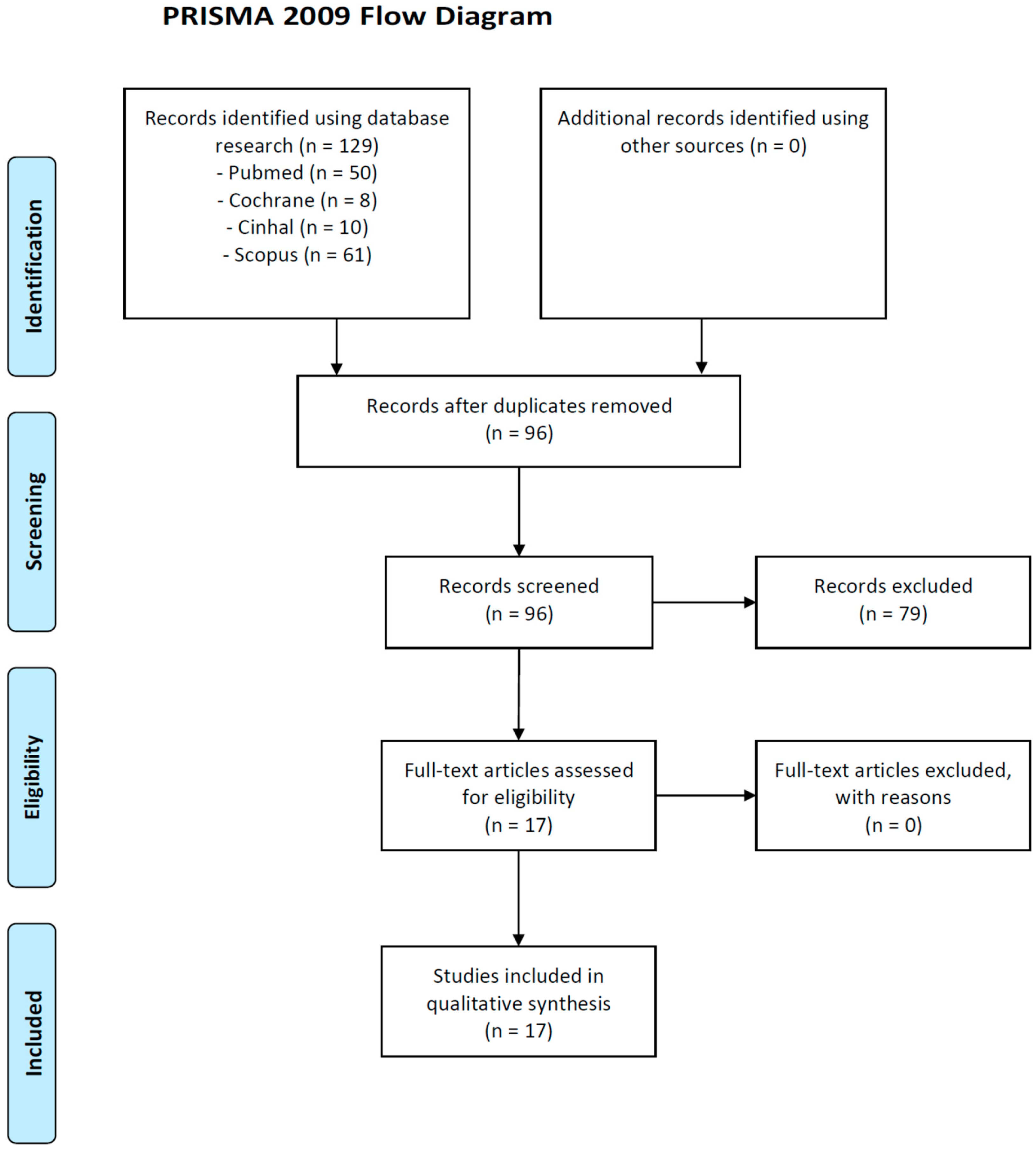
2.1. Study Design
2.2. Search Strategy
2.3. Selection Criteria
2.4. Selection Procedure, Data Extraction and Data Management
3. Data Synthesis
4. Results
4.1. Peer Victimization and Social Anxiety Disorder: Prevalence and Clinical Aspects
4.2. Clinical and Psychological Moderators of Relationship between Peer Victimization and Onset of Social Anxiety Disorder in Children and Adolescents
5. Discussion
6. Limitations
7. Implications for Practice and Research
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Haynie, D.; Nansel, T.; Eitel, P.; Crump, A.; Saylor, K.; Yu, K. Bullies, victims and bully/victims: Distinct groups of at-risk youth. J. Early Adolesc. 2001, 21, 29–49. [Google Scholar] [CrossRef]
- Nansel, T.R.; Overpeck, M.; Pilla, R.S.; Ruan, W.J.; Simons-Morton, B.; Scheidt, P. Bullying behaviors among US youth: Prevalence and association with psychosocial adjustment. JAMA 2001, 285, 2094–2100. [Google Scholar] [CrossRef] [PubMed]
- Olweus, D. The Nature of School Bullying. A Cross-National Perspective; Smith, P.K., Morita, Y., Junger-Tas, J., Olweus, D., Catalano, R., Slee, P., Eds.; Routledge: London, UK; New York, NY, USA, 1999. [Google Scholar]
- Skrzypiec, G.; Alinsug, E.; Nasiruddin, U.A.; Andreou, E.; Brighi, A.; Didaskalou, E.; Guarini, A.; Kang, S.W.; Kaur, K.; Kwon, S.; et al. Self-reported harm of adolescent peer aggression in three world regions. Child Abuse Negl. 2018, 85, 101–117. [Google Scholar] [CrossRef] [PubMed]
- Dooley, J.J.; Pyzalski, J.; Cross, D. Cyberbullying versus faceto-face bullying: A theoretical and conceptual review. Z. Psychol. 2009, 21, 182–188. [Google Scholar] [CrossRef]
- Olweus, D. Bullying at School. What We Know and What We can Do; Blackwell: Oxford, UK, 1993. [Google Scholar]
- Salmivalli, C.; Lagerspetz, K.; Björkqvist, K.; Österman, K.; Kaukiainen, A. Bullying as a group process: Participant roles and their relations to social status within the group. Aggress. Behav. 1996, 22, 1–15. [Google Scholar] [CrossRef]
- Salmivalli, C. Bullying and the peer group: A review. Aggress. Behav. 2010, 15, 112–120. [Google Scholar] [CrossRef]
- Inchley, J.; Currie, D.; Young, T.; Samdal, O.T.; Torsheim, T.; Li Augustson, L.; Mathison, F.; Aleman-Diaz, A.; Molcho, M.; Weber, M.; et al. Growing up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being. Available online: http://www.euro.who.int/en/publications/abstracts/growing-up-unequal.-hbsc-2016-study-20132014-survey (accessed on 6 June 2019).
- Eccles, J.; Midgley, C.; Wigfield, A.; Buchannan, C.; Reuman, D.; Flanagan, C.; Iver, D.M. Development during adolescence: The impact of stage-environment fit on young adolescents’ experiences in schools and in families. Am. Psychol. 1993, 48, 90–101. [Google Scholar] [CrossRef]
- Pellegrini, A.D.; Long, J.D. A longitudinal study of bullying, dominance, and victimization during the transition from primary school through secondary school. Br. J. Dev. Psychol. 2002, 20, 259–280. [Google Scholar] [CrossRef]
- Xie, H.; Swift, D.J.; Cairns, B.D.; Cairns, R.B. Aggressive behaviors in social interaction and developmental adaptation. A narrative analysis of interpersonal social conflicts during early adolescence. Soc. Dev. 2002, 11, 205–224. [Google Scholar] [CrossRef]
- Boxer, P.; Edwards-Leeper, L.; Goldstein, S.E.; Musher-Eizenman, D.; Dubow, E.F. Exposure to “low-level” aggression in school: Associations with aggressive behavior, future expectations, and perceived safety. Violence Vict. 2003, 18, 691–705. [Google Scholar]
- Juvonen, J.; Nishina, A.; Graham, S. Peer harassment, psychological adjustment, and school functioning in early adolescence. J. Educ. Psychol. 2000, 92, 349–359. [Google Scholar] [CrossRef]
- Boulton, M.J.; Trueman, M.; Murray, L. Associations between peer victimization, fear of future victimization and disrupted concentration on class work among junior school pupils. Br. J. Educ. Psychol. 2008, 78, 473–489. [Google Scholar] [CrossRef] [PubMed]
- Prinstein, M.J.; Cheah, C.S.; Guyer, A.E. Peer victimization, cue interpretation, and internalizing symptoms: preliminary concurrent and longitudinal findings for children and adolescents. J. Clin. Child Adolesc. Psychol. 2005, 34, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Carthy, T.; Horesh, N.; Apter, A.; Edge, M.D.; Gross, J.J. Emotional reactivity and cognitive regulation in anxious children. Behav. Res. Ther. 2010, 48, 384–393. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association (APA): Washington, DC, USA, 2000. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association (APA): Washington, DC, USA, 2013. [Google Scholar]
- Essau, C.A.; Conradt, J.; Petermann, F. Frequency and comorbidity of social anxiety and social phobia in adolescents. Results of a Bremen adolescent study. Fortschr. Neurol. Psychiatr. 1998, 66, 524–530. [Google Scholar] [CrossRef]
- Gren-Landell, M.; Tillfors, M.; Furmark, T.; Bohlin, G.; Andersson, G.; Svedin, C.G. Social phobia in Swedish adolescents: Prevalence and gender differences. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; McGonagle, K.A.; Zhao, S.; Nelson, C.B.; Hughes, M.; Eshleman, S.; Wittchen, H.U.; Kendler, K.S. Life-time and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Arch. Gen. Psychiatry 1994, 51, 8–19. [Google Scholar] [CrossRef]
- Wittchen, H.U.; Stein, M.B.; Kessler, R.C. Social fears and social phobia in a community sample of adolescents and young adults: Prevalence, risk factors and co-morbidity. Psychol. Med. 1999, 29, 309–323. [Google Scholar] [CrossRef]
- Bandelow, B.; Torrente, A.C.; Wedekind, D.; Broocks, A.; Hajak, G.; Ruther, E. Early traumatic life events, parental rearing styles, family history of mental disorders, and birth risk factors in patients with social anxiety disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2004, 254, 397–405. [Google Scholar] [CrossRef]
- Chartier, M.J.; Walker, J.R.; Stein, M.B. Social phobia and potential childhood risk factors in a community sample. Psychol. Med. 2001, 31, 307–315. [Google Scholar] [CrossRef]
- Magee, W.J. Effects of negative life experiences on phobia onset. Soc. Psychiatry Psychiatr. Epidemiol. 1999, 34, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Marteinsdottir, I.; Svensson, A.; Svedberg, M.; Anderberg, U.M.; von Knorring, L. The role of life events in social phobia. Nord J. Psychiatry 2007, 61, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Nelson, E.C.; Heath, A.C.; Madden, P.A.; Cooper, M.L.; Dinwiddie, S.H.; Bucholz, K.K.; Glowinski, A.; McLaughlin, T.; Dunne, M.P.; Statham, D.J.; et al. Association between self-reported childhood sexual abuse and adverse psychosocial outcomes: Results from a twin study. Arch. Gen. Psychiatry 2002, 59, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Ranta, K.; Kaltiala-Heino, R.; Pelkonen, M.; Marttunen, M. Associations between peer victimization, self-reported depression and social phobia among adolescents: The role of comorbidity. J. Adolesc. 2009, 32, 77–93. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.S.; La Greca, A.M.; Harrison, H.M. Peer victimization and social anxiety in adolescents: Prospective and reciprocal relationships. J. Youth Adolesc. 2009, 38, 1096–1109. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B.; Walker, J.R.; Anderson, G.; Hazen, A.L.; Ross, C.A.; Eldridge, G.; Forde, D.R. Childhood physical and sexual abuse in patients with anxiety disorders and in a community sample. Am. J. Psychiatry 1996, 153, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Storch, E.A.; Ledley, D.R. Peer victimization and psychosocial adjustment in children: Current knowledge and future directions. Clin. Pediatr. (Phila) 2005, 44, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Vernberg, E.M.; Abwender, D.A.; Ewell, K.K.; Beery, S.H. Social anxiety and peer relationships in early adolescence: A prospective analysis. J. Clin. Child Psychol. 1992, 21, 189–196. [Google Scholar] [CrossRef]
- Craig, W.M. The relationship among bullying, victimization, depression, anxiety, and aggression in elementary school children. Personal. Individ. Differ. 1998, 24, 123–130. [Google Scholar] [CrossRef]
- Dempsey, A.G.; Sulkowski, M.L.; Nichols, R.; Storch, E.A. Differences between peer victimization in cyber and physical settings and associated psychosocial adjustment in early adolescence. Psychol. Sch. 2009, 46, 962–972. [Google Scholar] [CrossRef]
- La Greca, A.M.; Harrison, H.M. Adolescent peer relations, friendships, and romantic relationships: Do they predict social anxiety and depression? J. Clin. Child Adolesc. Psychol. 2005, 34, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Richard, J.F.; Schneider, B.H.; Mallet, P. Revisiting the whole-school approach to bullying: Really looking at the whole school. Sch. Psychol. Int. 2011, 33, 263–284. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 8, e1000097. [Google Scholar] [CrossRef]
- Gren-Landell, M.; Aho, N.; Andersson, G.; Svedin, C.G. Social anxiety disorder and victimization in a community sample of adolescents. J. Adolesc. 2011, 34, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Pabian, S.; Vandebosch, H. An Investigation of Short-Term Longitudinal Associations Between Social Anxiety and Victimization and Perpetration of Traditional Bullying and Cyberbullying. J. Youth Adolesc. 2016, 45, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.S.; Kendall, P.C. Peer victimization among children and adolescents with anxiety disorders. Child Psychiatry Hum. Dev. 2015, 46, 393–405. [Google Scholar] [CrossRef]
- Davis, M.; Stadulis, R.; Neal-Barnett, A. Assessing the Effects of the Acting White Accusation Among Black Girls: Social Anxiety and Bullying Victimization. J. Natl. Med. Assoc. 2018, 110, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.L.; Potter, C.M.; Olino, T.M.; Abramson, L.Y.; Heimberg, R.G.; Alloy, L.B. The Temporal Sequence of Social Anxiety and Depressive Symptoms Following Interpersonal Stressors During Adolescence. J. Abnorm. Child Psychol. 2016, 44, 495–509. [Google Scholar] [CrossRef]
- Quinlan, E.B.; Barker, E.D.; Luo, Q.; Banaschewski, T.; Bokde, A.L.W.; Bromberg, U.; Büchel, C.; Desrivières, S.; Flor, H.; Frouin, V.; et al. Peer victimization and its impact on adolescent brain development and psychopathology. Mol. Psychiatry 2018, 12. [Google Scholar] [CrossRef]
- Ranta, K.; Kaltiala-Heino, R.; Frojd, S.; Marttunen, M. Peer victimization and social phobia: A follow-up study among adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 533–544. [Google Scholar] [CrossRef]
- Rudolph, K.D.; Miernicki, M.E.; Troop-Gordon, W.; Davis, M.M.; Telzer, E.H. Adding insult to injury: Neural sensitivity to social exclusion is associated with internalizing symptoms in chronically peer-victimized girls. Soc. Cogn. Affect. Neurosci. 2016, 11, 829–842. [Google Scholar] [CrossRef] [PubMed]
- Van Oort, F.V.; Greaves-Lord, K.; Ormel, J.; Verhulst, F.C.; Huizink, A.C. Risk indicators of anxiety throughout adolescence: The TRAILS study. Depress. Anxiety 2011, 28, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.C.; Luu, S.; Luh, D.L. Defending behaviors, bullying roles, and their associations with mental health in junior high school students: A population-based study. BMC Public Health 2016, 16, 1066. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.F.; Liu, T.L.; Ko, C.H.; Wu, Y.Y.; Cheng, C.P. Mediating effects of bullying involvement on the relationship of body mass index with social phobia, depression, suicidality, and self-esteem and sex differences in adolescents in Taiwan. Child Abuse Negl. 2014, 38, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.F.; Yang, P.; Wang, P.W.; Lin, H.C.; Liu, T.L.; Wu, Y.Y.; Tang, T. Association between school bullying levels/types and mental health problems among Taiwanese adolescents. Compr. Psychiatry 2014, 55, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Calvete, E.; Orue, I.; Gamez-Guadix, M. Do extraversion and neuroticism moderate the association between bullying victimization and internalizing symptoms? A three-wave longitudinal study. J. Sch. Psychol. 2016, 56, 1–11. [Google Scholar] [CrossRef]
- Ingram, R.E.; Luxton, D. Vulnerability-stress models. In Development of Psychopathology: A Vulnerability–Stress Perspective; Hankin, B.L., Abela, J.R.Z., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- Ladd, G.W.; Troop-Gordon, W. The role of chronic peer difficulties in the development of children’s psychological adjustment problems. Child Dev. 2003, 74, 1344–1367. [Google Scholar] [CrossRef]
- Shih, J.H.; Abela, J.R.; Starrs, C. Cognitive and interpersonal predictors of stress generation in children of affectively ill parents. J. Abnorm. Child Psychol. 2009, 37, 195–208. [Google Scholar] [CrossRef]
- Barbaranelli, C.; Carpara, G.; Rabasca, A.; Pastorelli, C. A questionnaire for measuring the Big Five in late childhood. Personal. Individ. Differ. 2003, 34, 645–664. [Google Scholar] [CrossRef]
- Early, M.C.; Biggs, B.K.; Makanui, K.P.; Legerski, J.P.; Van Allen, J.; Elledge, A.R.; Whiteside, S.P. Specificity of peer difficulties to social anxiety in early adolescence: Categorical and dimensional analyses with clinical and community samples. Anxiety Stress Coping 2017, 30, 647–660. [Google Scholar] [CrossRef]
- Ghoul, A.; Niwa, E.Y.; Boxer, P. The role of contingent self-worth in the relation between victimization and internalizing problems in adolescents. J. Adolesc. 2013, 36, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Silberg, J.L.; Copeland, W.; Linker, J.; Moore, A.A.; Roberson-Nay, R.; York, T.P. Psychiatric outcomes of bullying victimization: A study of discordant monozygotic twins. Psychol. Med. 2016, 46, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Spence, S.H.; Zubrick, S.R.; Lawrence, D. A profile of social, separation and generalized anxiety disorders in an Australian nationally representative sample of children and adolescents: Prevalence, comorbidity and correlates. Aust. J. Psychiatry 2018, 52, 446–460. [Google Scholar] [CrossRef] [PubMed]
- Chorpita, B.F.; Barlow, D.H. The development of anxiety: The role of control in the early environment. Psychol. Bull. 1998, 124, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Rose, A.J.; Rudolph, K.D. A review of sex differences in peer relationship processes: Potential trade-offs for the emotional and behavioral development of girls and boys. Psychol. Bull. 2006, 132, 98–131. [Google Scholar] [CrossRef] [PubMed]
- Crocker, J.; Knight, K. Contingencies of self-worth. Current Directions. Psychol. Sci. 2005, 14, 200–203. [Google Scholar] [CrossRef]
- Whitney, I.; Nabuzoka, D.; Smith, P.K. Bullying in schools: Mainstream and special needs. Support Learn. 1992, 7, 3–7. [Google Scholar] [CrossRef]
- Swearer, S.M.; Grills, A.E.; Haye, K.M.; Cary, P.T. Internalizing Problems in Students Involved in Bullying and Victimization: Implications for Intervention. In Bullying in American Schools: Asocial–Ecological Perspective on Prevention and Intervention; Espelage, D.L., Swearer, S.M., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2004. [Google Scholar]
- Williford, A.; Boulton, A.; Noland, B.; Little, T.D.; Karna, A.; Salmivalli, C. Effects of the KiVa anti-bullying program on adolescents’ depression, anxiety and perception of peers. J. Abnorm. Child Psychol. 2012, 40, 289–300. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Study | Sample | Study Design | Measure | Results | Limitations |
|---|---|---|---|---|---|
| Cohen and Kendall (2014) [41] | N: 90 Mean age: 11.06 (± 3.09) | Experimental study | Asher Loneliness Scale ADIS-C/P, CDI, CGAS, ERC, SPPC, MASC, SEQ-S, TQ-R | Overt victimization significantly predicted social anxiety (p = 0.003) and loneliness (p = 0.001); Relational victimization added significantly to the prediction of social anxiety (p = 0.002), depressive symptoms (p = 0.001), and loneliness (p < 0.001). | Study design: cross-sectional; Measures of victimization are not specific. |
| Davis (2017) [42] | N: 31 Mean age: 14 | Experimental study | AWEQ, MASC-2, GBS, MIBI | White accusation was significantly associated with social anxiety symptoms (p < 0.01), especially when it is interpreted as a negative evaluation; The accusation was significantly associated with bullying victimization (p < 0.05). | Only female participants; Small and specific sample. |
| Gren-Landell et al. (2011) [39] | N: 3211 Mean age: 17.3 | Cross-sectional study | SPSQ-C, JVQ | Significant association between SAD and high levels of peer victimization (p < 0.001); Females reported significantly more victimization of maltreatment, sexual victimization and victimization from peers and siblings (p < 0.001); Males reported a significant difference on the domain of peer/siblings victimization (p < 0.05). | Use of self-report instruments; Study design: cross-sectional. |
| Hamilton et al. (2016) [43] | N: 410 Mean age: 12.84 | Longitudinal study | CDI, MASC, ALEQ, SEQ-S, CTQ | Peer victimization, interpersonal stressors and emotional maltreatment predicted social anxiety and depressive symptoms. | The findings are not generalizable; Use of self-report instruments; No inclusion of a measures of overt victimization. |
| Pabian and Vandebosch (2015) [40] | N: 2128 Mean age: 13.02 | Longitudinal study | Self-Reported Cyberbullying Behavior, Self-Reported Traditional Bullying Involvement, SAS-A | At baseline social anxiety had a positive correlation with victimization of traditional bullying (p < 0.001), victimization of cyberbullying (p < 0.001), and perpetration of traditional bullying (p < 0.001); These aspects correlated positively with social anxiety 6 months later; Adolescents who scored higher on social anxiety had the same possibility to be victimized 6 months later that adolescents who scored lower | Use of self-report instruments; High drop-out rates; Measures of victimization are not specific. |
| Quinlan et al. (2018) [44] | N: 682 | Longitudinal study | OB/VQ, DAWBA, SDQ, CTQ, LEQ | Chronic adolescent peer victimization impact structural brain development and were related to psychopathology symptoms in late adolescence (depression: p = 0.001;generalized anxiety: p = 0.006); Chronic peer victimization was associated with steeper decreases in left putamen volume (p = 0.037) and these changes were also negatively associated with generalized anxiety (p = 0.020). | No information about peer victimization or early life stressors before age 14; No analysis of other brain regions linked to chronic peer victimization. |
| Ranta et al. (2013) [45] | N: 3278 Mean age: 15.5 | Longitudinal study | SPIN, BDI | Boys’ group there was a bidirectional association between direct peer victimization and social phobia (p < 0.05); Girls’ group, the relation victimization predicted the onset of social phobia (p < 0.001) | Use of self-report instruments; High drop-out rates. |
| Rudolph et al. (2016) [46] | N: 47 | Experimental study | SEQ-S, SMFQ, SAS-A, BIS, Social Achievement Goals Survey, NFA | Victimized girls reported higher levels of depressive symptoms (p < 0.001), social anxiety (p < 0.01), behavioral inhibition (p < 0.001) and avoidance-oriented need for approval (p < 0.05); Victimized girls had greater activation of the dorsal anterior cingulate cortex (dACC), the subgenual anterior cingulate cortex (sgACC) and anterior insula Activation to exclusion in the social pain network was associated with internalizing symptoms (p < 0.001). | No inclusion of a task measuring neural activation to other types of interpersonal stressors. |
| Van Oort et al. (2011) [47] | N: 2220 Age range: 10–12 | Longitudinal study | RCADS, PSI, EMBU-C, YSR, WISC-R, Family History Interview | Victimization experience was correlated to the presence of social phobia in late adolescence (p < 0.001); A moderate correlation with social phobia has been found in correlation with being a bully, experienced parents’ mental and physical health problems and the sociometric status (p < 0.05). | Not clinical sample; Not exhaustive analysis of risk indicator. |
| Wu et al. (2016) [48] | N: 2872 | Cross-sectional study | SASC-R, SPAI-C, CES-DC | Defending behaviours were positively associated with social anxiety and depressive symptoms (p = 0.005) in victims and bystanders; Victims and bully-victims also had greater social anxiety (p < 0.001) than bullies. | Study design: cross-sectional; No analysis about association of particular form of bullying, defending behaviors and mental health. |
| Yen et al. (2014a) [49] | N: 5252 | Cross-sectional study | BMI, C-SBEQ, SPIN, MC-CES-D, K-SADS-E, RSES | The severities of victimization of passive, active bullying and perpetration of passive bullying were positively associated with the severities of social phobia, depression and suicidality (p < 0.001); BMI was positively associated with the severities of victimization of passive (p < 0.001), active bullying (p < 0.01) and perpetration of passive bullying (p < 0.05). | Study design: cross-sectional; The data provided by the adolescents themselves; The findings are not generalizable. |
| Yen et al. (2014b) [50] | N: 1604 | Cross-sectional study | C-SBEQ, MC-CES-D, MASC-T, SPIN, ADHDS, K-SADS-E, CRAFFT | Victim of passive or active bullying and perpetrator of passive bullying were significantly associated with mental health problems, including social phobia (p < 0.001); Perpetrators of only active bullying reported less severe general anxiety and social phobia than perpetrators of only passive bullying (p < 0.001); Victims of both passive and active bullying had higher risks of social phobia (p < 0.001), depression (p < 0.001) and inattention (p < 0.001) than victims of only passive or active bullying. | Study design: cross-sectional; The data provided by the adolescents themselves; Different periods of measure about the experiences of bullying and mental health problems. |
| Study | Sample | Study Design | Measure | Results | Limitations |
|---|---|---|---|---|---|
| Calvete et al. (2016) [51] | N: 1440 Mean age: 13.54 | Longitudinal study | BFQ-C CES-D SAS-A | Extraversion girls had lower predictive association between victimization and social anxiety; Adolescents with high levels of extraversion presented a greater reduction in depressive symptoms; Neuroticism predicted both depression and social anxiety, but no significant interactions were evident between neuroticism and bullying victimization; The association between bullying victimization and social anxiety was stronger for boys than for girls (p < 0.001); The association between neuroticism and depression was stronger for girls (p < 0.001). | Use of self-report instruments; No differentiation between direct and indirect; Use few variables. |
| Early et al. (2017) [56] | N: 154 clinical sample N: 116 community sample Mean age: 13.07 | Cross-sectional, quantitative survey | MINI-KID SCAS-C SCAS-P Peer acceptance 3 items PEQ -VS | Significant group differences in participant self-rated social acceptance (p < 0.001), parent-rated social acceptance (p < 0.001), and relational victimization (p < 0.05); Social anxiety group presented lowest social acceptance compared to other anxiety group and the community sample; Girls in the community sample showed more overt victimization than girls with SAD and other anxiety diagnoses; The results showed significant interaction between group status and self-reported social anxiety (p < 0.05) and nonsocial anxiety (p < 0.05) in predicting relational victimization in the community sample. | Use of rating scale without behavior observation. |
| Ghoul et al. (2013) [57] | N: 716 Mean age: 15.95 | Experimental study | RCDAS SWCQ Exposure to School Aggression Scale | Results showed that victimization and contingent self-worth were positively correlated with social phobia (p < 0.001); Higher levels of contingent self-worth amplify the effect of victimization on internalizing problems; For social phobia, this effect appeared to be salient only for boys. | Use of self-report instruments; No longitudinal data. |
| Silberg et al. (2016) [58] | N: 145 pairs Age range: 8–17 | Longitudinal study | CAPA SCID | Bullied MZ twins compared to their non-bullied co-twin have the higher rate of social anxiety (27%), separation anxiety (15%), Attention Deficit and Hyperactivity Disorder (5%), and young adult suicidality (12%); Significant individual-specific environmental correlations between bullying victimization and social anxiety, separation anxiety and young adult suicidality; Highly significant association between early bullying victimization and later social anxiety (p < 0.001) and bullying victimization and later young adult suicidality (p < 0.05); Genetic factors were also influential in bullying victimization and social anxiety. | Need to replicate the data. |
| Spence et al. (2017) [59] | N: 6310 Age range: 4–17 | DISC-IV Social envirometal dataImpact of functioning | Social anxiety disorder, separation anxiety disorder and generalized anxiety disorder were all associated with having a parent with a mental health problem and repeated bullying over the previous 12 months (p < 0.001). | Not analysis of lifetime presence of disorders; Use parental report. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pontillo, M.; Tata, M.C.; Averna, R.; Demaria, F.; Gargiullo, P.; Guerrera, S.; Pucciarini, M.L.; Santonastaso, O.; Vicari, S. Peer Victimization and Onset of Social Anxiety Disorder in Children and Adolescents. Brain Sci. 2019, 9, 132. https://doi.org/10.3390/brainsci9060132
Pontillo M, Tata MC, Averna R, Demaria F, Gargiullo P, Guerrera S, Pucciarini ML, Santonastaso O, Vicari S. Peer Victimization and Onset of Social Anxiety Disorder in Children and Adolescents. Brain Sciences. 2019; 9(6):132. https://doi.org/10.3390/brainsci9060132
Chicago/Turabian StylePontillo, Maria, Maria Cristina Tata, Roberto Averna, Francesco Demaria, Prisca Gargiullo, Silvia Guerrera, Maria Laura Pucciarini, Ornella Santonastaso, and Stefano Vicari. 2019. "Peer Victimization and Onset of Social Anxiety Disorder in Children and Adolescents" Brain Sciences 9, no. 6: 132. https://doi.org/10.3390/brainsci9060132