

Phytochemicals and Glioma: Results from Dietary Mixed Exposure
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Intake Assessment
2.3. Assessment of Phytochemical Intake
2.4. Other Variables
2.5. Statistical Analysis
3. Results
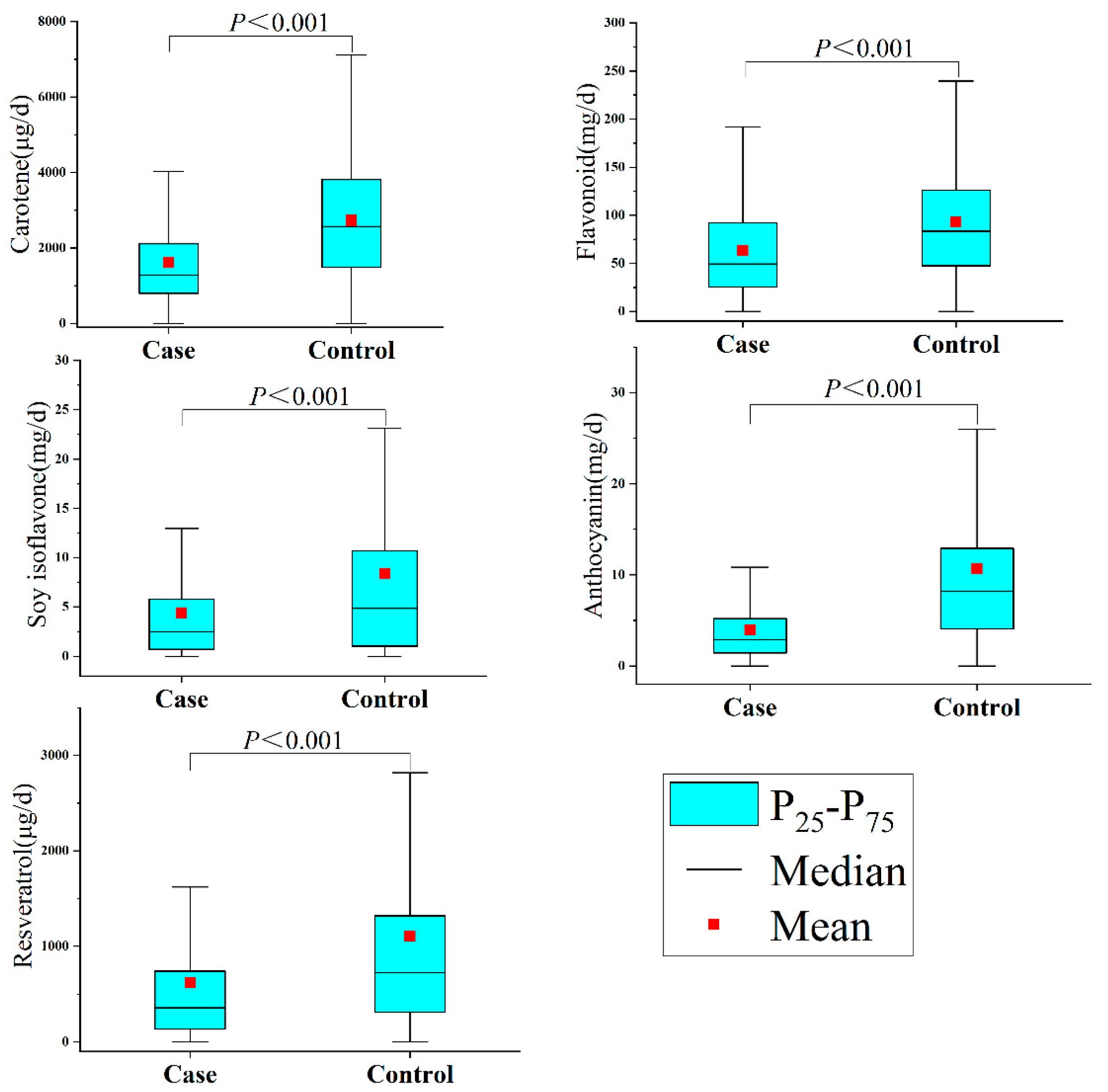
3.1. Characteristics of the Study Population and Phytochemicals
3.2. Association between Phytochemicals and Glioma
3.3. Phytochemicals and Pathological Classification and Grading of Glioma
3.4. Subgroup Analysis and Sensitivity Analysis
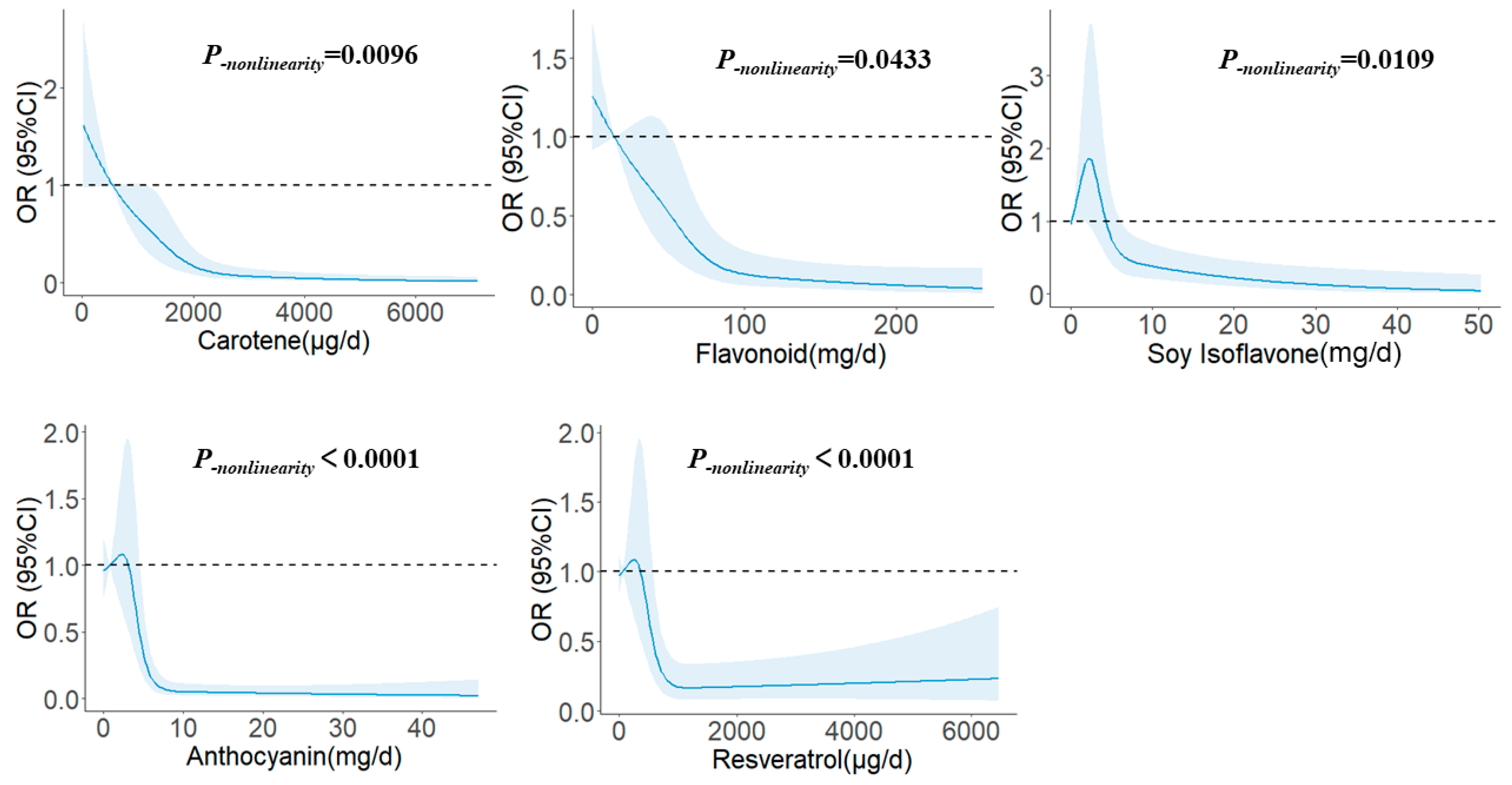
3.5. Dose–Response Relationship
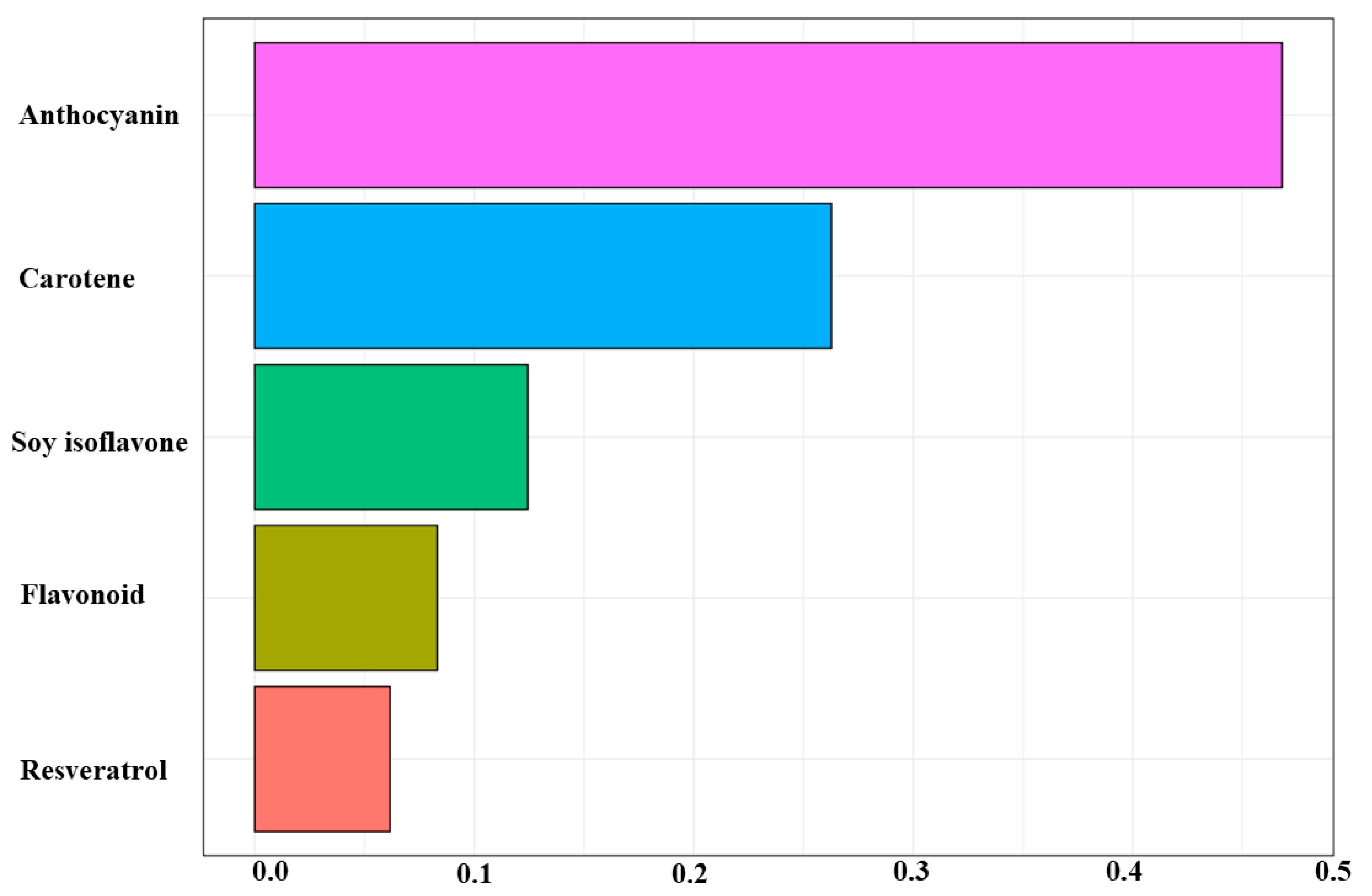
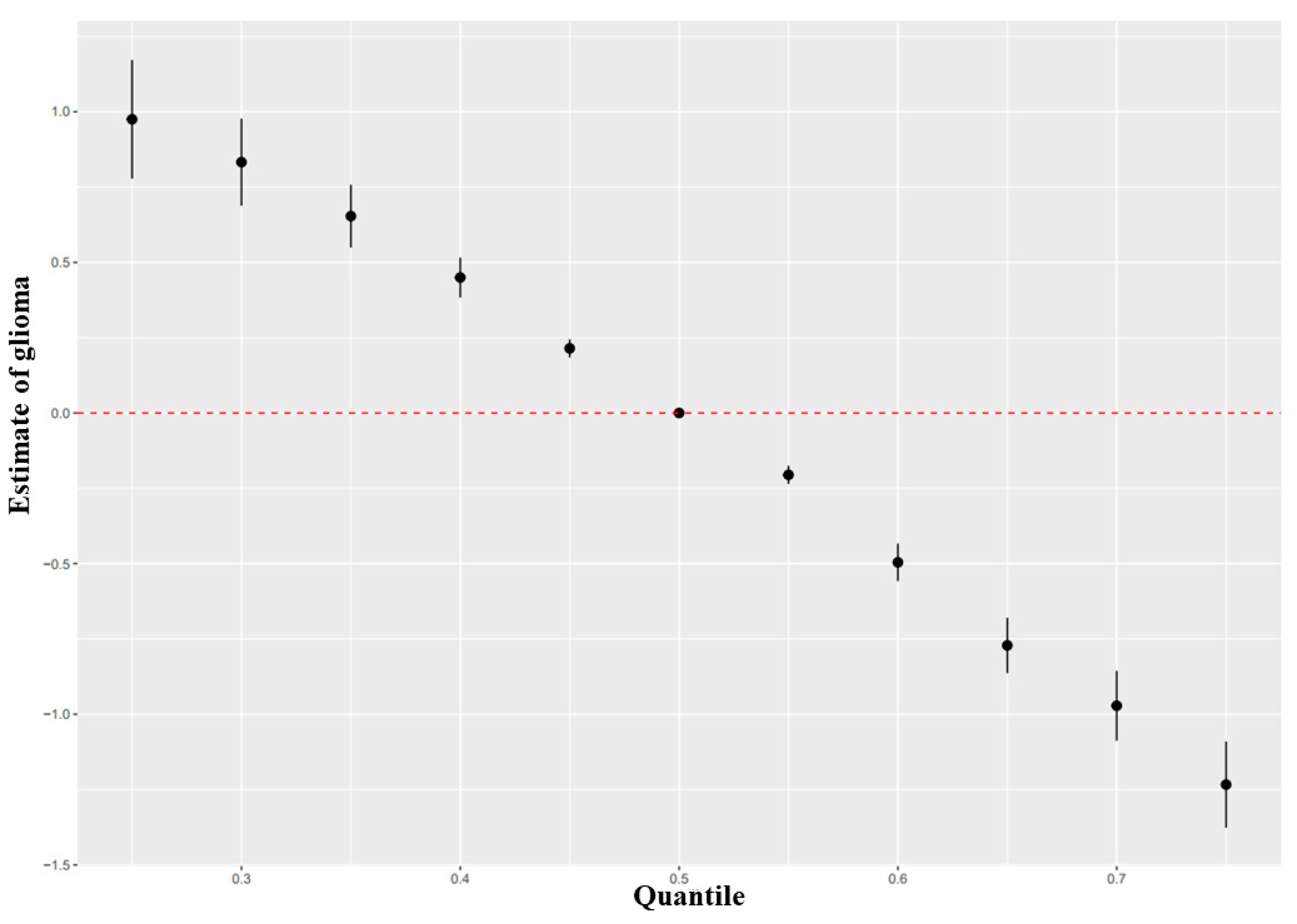
3.6. Effects of Mixed Exposure of Phytochemicals on Glioma Based on WQS and BKMR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Howes, M.J.; Simmonds, M.S. The role of phytochemicals as micronutrients in health and disease. Curr. Opin. Clin. Nutr. 2014, 17, 558–566. [Google Scholar] [CrossRef]
- Kotecha, R.; Takami, A.; Espinoza, J.L. Dietary phytochemicals and cancer chemoprevention: A review of the clinical evidence. Oncotarget 2016, 7, 52517–52529. [Google Scholar] [CrossRef] [Green Version]
- Manach, C.; Scalbert, A.; Morand, C.; Remesy, C.; Jimenez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.J.; Gan, R.Y.; Li, S.; Zhou, Y.; Li, A.N.; Xu, D.P.; Li, H.B. Antioxidant Phytochemicals for the Prevention and Treatment of Chronic Diseases. Molecules 2015, 20, 21138–21156. [Google Scholar] [CrossRef] [Green Version]
- Milani, A.; Basirnejad, M.; Shahbazi, S.; Bolhassani, A. Carotenoids: Biochemistry, pharmacology and treatment. Brit. J. Pharmacol. 2017, 174, 1290–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakai, S.; Fujita, M.; Kamei, Y. Health Promotion Effects of Soy Isoflavones. J. Nutr. Sci. Vitaminol. 2020, 66, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Priyadarsini, R.V.; Nagini, S. Cancer chemoprevention by dietary phytochemicals: Promises and pitfalls. Curr. Pharm. Biotechno. 2012, 13, 125–136. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Lee, J.; Choi, I.J.; Kim, Y.I.; Kwon, O.; Kim, H.; Kim, J. Dietary Carotenoids Intake and the Risk of Gastric Cancer: A Case-Control Study in Korea. Nutrients 2018, 10, 1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowles, J.R.; Ranard, K.M.; Smith, J.W.; An, R.; Erdman, J.J. Increased dietary and circulating lycopene are associated with reduced prostate cancer risk: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2017, 20, 361–377. [Google Scholar] [CrossRef]
- Feng, X.L.; Ho, S.C.; Mo, X.F.; Lin, F.Y.; Zhang, N.Q.; Luo, H.; Zhang, X.; Zhang, C.X. Association between flavonoids, flavonoid subclasses intake and breast cancer risk: A case-control study in China. Eur. J. Cancer Prev. 2020, 29, 493–500. [Google Scholar] [CrossRef]
- Woo, H.D.; Kim, J. Dietary flavonoid intake and risk of stomach and colorectal cancer. World J. Gastroentero. 2013, 19, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.; Liu, X.; Tian, Y.; Xie, C.; Li, Q.; Cui, H.; Sun, C. Flavonoids, Flavonoid Subclasses, and Esophageal Cancer Risk: A Meta-Analysis of Epidemiologic Studies. Nutrients 2016, 8, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, Y.; Lv, J.; Guo, Y.; Bian, Z.; Gao, M.; Du, H.; Yang, L.; Chen, Y.; Zhang, X.; Wang, T.; et al. Soy intake and breast cancer risk: A prospective study of 300,000 Chinese women and a dose-response meta-analysis. Eur. J. Epidemiol. 2020, 35, 567–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levi, F.; Pasche, C.; Lucchini, F.; Ghidoni, R.; Ferraroni, M.; La Vecchia, C. Resveratrol and breast cancer risk. Eur. J. Cancer Prev. 2005, 14, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Crespo, I.; Vital, A.L.; Gonzalez-Tablas, M.; Patino, M.C.; Otero, A.; Lopes, M.C.; de Oliveira, C.; Domingues, P.; Orfao, A.; Tabernero, M.D. Molecular and Genomic Alterations in Glioblastoma Multiforme. Am. J. Pathol. 2015, 185, 1820–1833. [Google Scholar] [CrossRef] [Green Version]
- Hanif, F.; Muzaffar, K.; Perveen, K.; Malhi, S.M.; Simjee, S. Glioblastoma Multiforme: A Review of its Epidemiology and Pathogenesis through Clinical Presentation and Treatment. Asian Pac. J. Cancer Prev. 2017, 18, 3–9. [Google Scholar] [CrossRef]
- Anjum, K.; Shagufta, B.I.; Abbas, S.Q.; Patel, S.; Khan, I.; Shah, S.; Akhter, N.; Hassan, S. Current status and future therapeutic perspectives of glioblastoma multiforme (GBM) therapy: A review. Biomed. Pharmacother. 2017, 92, 681–689. [Google Scholar] [CrossRef]
- Pan, H.C.; Jiang, Q.; Yu, Y.; Mei, J.P.; Cui, Y.K.; Zhao, W.J. Quercetin promotes cell apoptosis and inhibits the expression of MMP-9 and fibronectin via the AKT and ERK signalling pathways in human glioma cells. Neurochem. Int. 2015, 80, 60–71. [Google Scholar] [CrossRef]
- Kim, H.; Moon, J.Y.; Ahn, K.S.; Cho, S.K. Quercetin induces mitochondrial mediated apoptosis and protective autophagy in human glioblastoma U373MG cells. Oxid. Med. Cell. Longev. 2013, 2013, 596496. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Feng, H.; Zhang, Y. Resveratrol inhibits hypoxia-induced glioma cell migration and invasion by the p-STAT3/miR-34a axis. Neoplasma 2016, 63, 532–539. [Google Scholar] [CrossRef] [Green Version]
- Rigi, S.; Shayanfar, M.; Mousavi, S.M.; Mohammad-Shirazi, M.; Sharifi, G.; Esmaillzadeh, A. Dietary phytochemical index in relation to risk of glioma: A case-control study in Iranian adults. Nutr. J. 2021, 20, 31. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; He, Y.; Kang, X.; Wang, C.; Chen, F.; Kang, Z.; Yang, S.; Zhang, R.; Peng, Y.; Li, W. Association between dietary minerals and glioma: A case-control study based on Chinese population. Front. Nutr. 2023, 10, 1118997. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Wen-Hua, Z.; Zhi-Ping, H.; Xin, Z.; Li, H.E.; Water, W.; Jun-Ling, W.; Kyoko, H.; Jun-Shi, C. Reproducibility and Validity of a Chinese Food Frequency Questionnaire. Biomed. Environ. Sci. 2010, 23, 1–38. [Google Scholar]
- Yang, Y.X. China Food Composition Tables: Standard Edition; Peking University Medical Press: Beijing, China, 2018. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Morgan, L.L.; Miller, A.B.; Sasco, A.; Davis, D.L. Mobile phone radiation causes brain tumors and should be classified as a probable human carcinogen (2A) (review). Int. J. Oncol. 2015, 46, 1865–1871. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Du, J.; Li, H.; Yang, Y.; Cai, C.; Gao, Q.; Xing, Y.; Shao, B.; Li, G. Multiple-element exposure and metabolic syndrome in Chinese adults: A case-control study based on the Beijing population health cohort. Environ. Int. 2020, 143, 105959. [Google Scholar] [CrossRef]
- Carrico, C.; Gennings, C.; Wheeler, D.C.; Factor-Litvak, P. Characterization of Weighted Quantile Sum Regression for Highly Correlated Data in a Risk Analysis Setting. J. Agric. Biol. Environ. Stat. 2015, 20, 100–120. [Google Scholar] [CrossRef]
- Czarnota, J.; Gennings, C.; Wheeler, D.C. Assessment of weighted quantile sum regression for modeling chemical mixtures and cancer risk. Cancer Inform. 2015, 14, 159–171. [Google Scholar] [CrossRef] [Green Version]
- Bobb, J.F.; Valeri, L.; Claus, H.B.; Christiani, D.C.; Wright, R.O.; Mazumdar, M.; Godleski, J.J.; Coull, B.A. Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics 2015, 16, 493–508. [Google Scholar] [CrossRef] [Green Version]
- Bobb, J.F.; Claus, H.B.; Valeri, L.; Coull, B.A. Statistical software for analyzing the health effects of multiple concurrent exposures via Bayesian kernel machine regression. Environ. Health-Glob. 2018, 17, 67. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Amaya, D.B. Structures and Analysis of Carotenoid Molecules. Subcell. Biochem. 2016, 79, 71–108. [Google Scholar] [CrossRef] [PubMed]
- Eggersdorfer, M.; Wyss, A. Carotenoids in human nutrition and health. Arch. Biochem. Biophys. 2018, 652, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, T. A large scale cohort study on cancer risks by diet--with special reference to the risk reducing effects of green-yellow vegetable consumption. Princess Takamatsu Symp. 1985, 16, 41–53. [Google Scholar]
- Knekt, P.; Jarvinen, R.; Seppanen, R.; Rissanen, A.; Aromaa, A.; Heinonen, O.P.; Albanes, D.; Heinonen, M.; Pukkala, E.; Teppo, L. Dietary antioxidants and the risk of lung cancer. Am. J. Epidemiol. 1991, 134, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cui, R.; Xiao, Y.; Fang, J.; Xu, Q. Effect of Carotene and Lycopene on the Risk of Prostate Cancer: A Systematic Review and Dose-Response Meta-Analysis of Observational Studies. PLoS ONE 2015, 10, e137427. [Google Scholar] [CrossRef]
- Yu, N.; Su, X.; Wang, Z.; Dai, B.; Kang, J. Association of Dietary Vitamin A and beta-Carotene Intake with the Risk of Lung Cancer: A Meta-Analysis of 19 Publications. Nutrients 2015, 7, 9309–9324. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Zhang, B. The association of dietary beta-carotene and vitamin A intake on the risk of esophageal cancer: A meta-analysis. Rev. Esp. Enferm. Dig. 2020, 112, 620–626. [Google Scholar] [CrossRef]
- Tedeschi-Blok, N.; Lee, M.; Sison, J.D.; Miike, R.; Wrensch, M. Inverse association of antioxidant and phytoestrogen nutrient intake with adult glioma in the San Francisco Bay Area: A case-control study. Bmc Cancer 2006, 6, 148. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Ward, M.H.; Tucker, K.L.; Graubard, B.I.; McComb, R.D.; Potischman, N.A.; Weisenburger, D.D.; Heineman, E.F. Diet and risk of adult glioma in eastern Nebraska, United States. Cancer Cause Control. 2002, 13, 647–655. [Google Scholar] [CrossRef]
- Terry, M.B.; Howe, G.; Pogoda, J.M.; Zhang, F.F.; Ahlbom, A.; Choi, W.; Giles, G.G.; Little, J.; Lubin, F.; Menegoz, F.; et al. An international case-control study of adult diet and brain tumor risk: A histology-specific analysis by food group. Ann. Epidemiol. 2009, 19, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Holick, C.N.; Giovannucci, E.L.; Rosner, B.; Stampfer, M.J.; Michaud, D.S. Prospective study of intake of fruit, vegetables, and carotenoids and the risk of adult glioma. Am. J. Clin. Nutr. 2007, 85, 877–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurmu, F.; Hussein, S.; Laing, M. The potential of orange-fleshed sweet potato to prevent vitamin A deficiency in Africa. Int. J. Vitam. Nutr. Res. 2014, 84, 65–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, W.; Zhong, X.; Xu, L.; Han, W. Association between Dietary Vitamin A Intake and the Risk of Glioma: Evidence from a Meta-analysis. Nutrients 2015, 7, 8897–8904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.Z.; Li, S.; Garcia, E.; Glubrecht, D.D.; Poon, H.Y.; Easaw, J.C.; Godbout, R. Association between cytoplasmic CRABP2, altered retinoic acid signaling, and poor prognosis in glioblastoma. Glia 2016, 64, 963–976. [Google Scholar] [CrossRef] [Green Version]
- Aherne, S.A.; O’Brien, N.M. Dietary flavonols: Chemistry, food content, and metabolism. Nutrition 2002, 18, 75–81. [Google Scholar] [CrossRef]
- Kocic, B.; Kitic, D.; Brankovic, S. Dietary flavonoid intake and colorectal cancer risk: Evidence from human population studies. J. Buon 2013, 18, 34–43. [Google Scholar]
- Middleton, E.J. Effect of plant flavonoids on immune and inflammatory cell function. Adv. Exp. Med. Biol. 1998, 439, 175–182. [Google Scholar] [CrossRef]
- Lambert, J.D.; Hong, J.; Yang, G.Y.; Liao, J.; Yang, C.S. Inhibition of carcinogenesis by polyphenols: Evidence from laboratory investigations. Am. J. Clin. Nutr. 2005, 81, 284S–291S. [Google Scholar] [CrossRef] [Green Version]
- Bever, A.M.; Cassidy, A.; Rimm, E.B.; Stampfer, M.J.; Cote, D.J. A prospective study of dietary flavonoid intake and risk of glioma in US men and women. Am. J. Clin. Nutr. 2021, 114, 1314–1327. [Google Scholar] [CrossRef]
- Rizzo, G.; Baroni, L. Soy, Soy Foods and Their Role in Vegetarian Diets. Nutrients 2018, 10, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, H.B.; Zhang, Y.F.; Yang, J.D.; Lu, K.L. Study on soy isoflavone consumption and risk of breast cancer and survival. Asian Pac. J. Cancer Prev. 2012, 13, 995–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeLorenze, G.N.; McCoy, L.; Tsai, A.L.; Quesenberry, C.J.; Rice, T.; Il’Yasova, D.; Wrensch, M. Daily intake of antioxidants in relation to survival among adult patients diagnosed with malignant glioma. Bmc Cancer 2010, 10, 215. [Google Scholar] [CrossRef] [Green Version]
- Alappat, B.; Alappat, J. Anthocyanin Pigments: Beyond Aesthetics. Molecules 2020, 25, 5500. [Google Scholar] [CrossRef]
- Khoo, H.E.; Azlan, A.; Tang, S.T.; Lim, S.M. Anthocyanidins and anthocyanins: Colored pigments as food, pharmaceutical ingredients, and the potential health benefits. Food Nutr. Res. 2017, 61, 1361779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynn, A.; Mathew, S.; Moore, C.T.; Russell, J.; Robinson, E.; Soumpasi, V.; Barker, M.E. Effect of a tart cherry juice supplement on arterial stiffness and inflammation in healthy adults: A randomised controlled trial. Plant. Food Hum. Nutr. 2014, 69, 122–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, S.H.; Ahn, I.S.; Kim, S.O.; Kong, C.S.; Chung, H.Y.; Do, M.S.; Park, K.Y. Anti-obesity and hypolipidemic effects of black soybean anthocyanins. J. Med. Food 2007, 10, 552–556. [Google Scholar] [CrossRef]
- Wang, X.; Yang, D.Y.; Yang, L.Q.; Zhao, W.Z.; Cai, L.Y.; Shi, H.P. Anthocyanin Consumption and Risk of Colorectal Cancer: A Meta-Analysis of Observational Studies. J. Am. Coll. Nutr. 2019, 38, 470–477. [Google Scholar] [CrossRef]
- Chen, J.; Xu, B.; Sun, J.; Jiang, X.; Bai, W. Anthocyanin supplement as a dietary strategy in cancer prevention and management: A comprehensive review. Crit. Rev. Food Sci. 2022, 62, 7242–7254. [Google Scholar] [CrossRef]
- Gusman, J.; Malonne, H.; Atassi, G. A reappraisal of the potential chemopreventive and chemotherapeutic properties of resveratrol. Carcinogenesis 2001, 22, 1111–1117. [Google Scholar] [CrossRef] [Green Version]
- Pervaiz, S.; Holme, A.L. Resveratrol: Its biologic targets and functional activity. Antioxid. Redox Sign 2009, 11, 2851–2897. [Google Scholar] [CrossRef] [PubMed]
- Rotelli, M.T.; Bocale, D.; De Fazio, M.; Ancona, P.; Scalera, I.; Memeo, R.; Travaglio, E.; Zbar, A.P.; Altomare, D.F. IN-VITRO evidence for the protective properties of the main components of the Mediterranean diet against colorectal cancer: A systematic review. Surg. Oncol. 2015, 24, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Fulda, S. Resveratrol and derivatives for the prevention and treatment of cancer. Drug. Discov. Today 2010, 15, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Dybkowska, E.; Sadowska, A.; Swiderski, F.; Rakowska, R.; Wysocka, K. The occurrence of resveratrol in foodstuffs and its potential for supporting cancer prevention and treatment. A review. Rocz. Panstw. Zakl. Hig. 2018, 69, 5–14. [Google Scholar]
- Cai, H.; Scott, E.; Kholghi, A.; Andreadi, C.; Rufini, A.; Karmokar, A.; Britton, R.G.; Horner-Glister, E.; Greaves, P.; Jawad, D.; et al. Cancer chemoprevention: Evidence of a nonlinear dose response for the protective effects of resveratrol in humans and mice. Sci. Transl. Med. 2015, 7, 117r–298r. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langcake., P.; Pryce, R.J. The production of resveratrol by Vitis vinifera and other members of the Vitaceae as a response to infection or injury. Physiol. Plant Pathol. 1976, 9, 77–86. [Google Scholar] [CrossRef]
- Mousavi, S.M.; Shayanfar, M.; Rigi, S.; Mohammad-Shirazi, M.; Sharifi, G.; Esmaillzadeh, A. Adherence to the Mediterranean dietary pattern in relation to glioma: A case-control study. Clin. Nutr. 2021, 40, 313–319. [Google Scholar] [CrossRef]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [Green Version]
- Coelho, P.L.; Oliveira, M.N.; Da, S.A.; Pitanga, B.P.; Silva, V.D.; Faria, G.P.; Sampaio, G.P.; Costa, M.F.; Braga-de-Souza, S.; Costa, S.L. The flavonoid apigenin from Croton betulaster Mull inhibits proliferation, induces differentiation and regulates the inflammatory profile of glioma cells. Anti-Cancer Drug. 2016, 27, 960–969. [Google Scholar] [CrossRef]
- Wang, L.S.; Stoner, G.D. Anthocyanins and their role in cancer prevention. Cancer Lett. 2008, 269, 281–290. [Google Scholar] [CrossRef] [Green Version]
- Dadgostar, E.; Fallah, M.; Izadfar, F.; Heidari-Soureshjani, R.; Aschner, M.; Tamtaji, O.R.; Mirzaei, H. Therapeutic Potential of Resveratrol in the Treatment of Glioma: Insights into its Regulatory Mechanisms. Mini-Rev. Med. Chem. 2021, 21, 2835–2847. [Google Scholar] [CrossRef]
- Chen, Q.H.; Wu, B.K.; Pan, D.; Sang, L.X.; Chang, B. Beta-carotene and its protective effect on gastric cancer. World J. Clin. Cases 2021, 9, 6591–6607. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Jo, Y.U.; Shin, H.; Lee, J.; Chae, S.U.; Bae, S.K.; Na, K. Anthocyanin-fucoidan nanocomplex for preventing carcinogen induced cancer: Enhanced absorption and stability. Int. J. Pharmaceut 2020, 586, 119597. [Google Scholar] [CrossRef] [PubMed]
- Sabarinathan, D.; Mahalakshmi, P.; Vanisree, A.J. Naringenin, a flavanone inhibits the proliferation of cerebrally implanted C6 glioma cells in rats. Chem-Biol. Interact. 2011, 189, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Chen, J.; Wang, J.; Gong, S.; Jin, H.; Sheng, P.; Qi, X.; Lv, L.; Dong, Y.; Hou, L. Body mass index and risk of brain tumors: A systematic review and dose-response meta-analysis. Eur. J. Clin. Nutr. 2016, 70, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.C.; Krewski, D.; Armstrong, B.K.; Chetrit, A.; Giles, G.G.; Hours, M.; McBride, M.L.; Parent, M.E.; Sadetzki, S.; Siemiatycki, J.; et al. Allergy and brain tumors in the INTERPHONE study: Pooled results from Australia, Canada, France, Israel, and New Zealand. Cancer Cause Control 2013, 24, 949–960. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Francis, S.S.; Barnholtz-Sloan, J.S. Epidemiology of Brain and Other CNS Tumors. Curr. Neurol. Neurosci. 2021, 21, 68. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | p-Value a,b | |||||
|---|---|---|---|---|---|---|---|
| Case | Control | p Value a | Case | Control | p Value a | ||
| Age (years) | 42.29 ± 12.93 | 41.01 ± 12.83 | 0.235 | 43.04 ± 13.31 | 41.33 ± 12.90 | 0.171 | 0.072 |
| BMI | 24.60 ± 3.08 | 24.16 ± 3.21 | 0.095 | 23.30 ± 3.32 | 21.63 ± 2.76 | <0.001 | <0.001 |
| High-risk residential area (%) | 0.688 | 0.138 | 0.534 | ||||
| Yes | 21.8 | 23.2 | 20.7 | 15.3 | |||
| No | 78.2 | 76.8 | 79.3 | 84.7 | |||
| Occupation (%) | 0.354 | 0.002 | 0.024 | ||||
| Manual workers | 29.6 | 25.0 | 22.5 | 14.4 | |||
| Mental workers | 59.5 | 61.3 | 43.3 | 59.5 | |||
| Others | 10.9 | 13.7 | 34.2 | 26.1 | |||
| Education level (%) | 0.003 | <0.001 | <0.001 | ||||
| Primary school and below | 3.5 | 2.8 | 11.3 | 2.3 | |||
| Middle school | 39.8 | 26.8 | 43.7 | 23.0 | |||
| University and above | 56.7 | 70.4 | 45.0 | 74.7 | |||
| Household income (%) | <0.001 | <0.001 | <0.001 | ||||
| <3000 CNY/month | 8.1 | 20.1 | 11.7 | 15.8 | |||
| 3000–10,000 CNY/month | 75.4 | 49.6 | 76.6 | 48.6 | |||
| >10,000 CNY/month | 16.5 | 30.3 | 11.7 | 35.6 | |||
| Smoking status (%) | 0.036 | 0.308 | 0.039 | ||||
| Never smoking | 47.9 | 56.3 | 98.2 | 99.5 | |||
| Former smoking | 22.2 | 14.4 | 0.9 | 0 | |||
| Current smoking | 29.9 | 29.2 | 0.9 | 0.5 | |||
| History of allergies (%) | 0.471 | <0.001 | <0.001 | ||||
| Yes | 8.5 | 10.2 | 6.8 | 20.3 | |||
| No | 91.5 | 89.8 | 93.2 | 79.7 | |||
| History of head trauma (%) | 0.374 | 1.000 | 0.474 | ||||
| Yes | 13.7 | 11.3 | 8.1 | 8.1 | |||
| No | 86.3 | 88.7 | 91.9 | 91.9 | |||
| Family history of cancer (%) | 0.005 | 0.078 | 0.001 | ||||
| Yes | 27.1 | 17.3 | 33.8 | 26.1 | |||
| No | 72.9 | 82.7 | 66.2 | 73.9 | |||
| Physical Activity (%) | <0.001 | <0.001 | <0.001 | ||||
| Low | 16.2 | 45.1 | 10.4 | 46.8 | |||
| Moderate | 44.7 | 34.8 | 36.9 | 38.3 | |||
| High | 39.1 | 20.1 | 52.7 | 14.9 | |||
| Phytochemicals | T1 | T2 | T3 | Continuous c | p-Value |
|---|---|---|---|---|---|
| Carotene | ≤1255.00 | 1255.00–2569.31 | >2569.31 | ||
| Case/Control | 247/91 | 174/171 | 85/244 | ||
| Model 1 a | 1 | 0.33 (0.22–0.48) | 0.13 (0.08–0.19) | 0.76 (0.72–0.81) | <0.001 |
| Model 2 b | 1 | 0.29 (0.15–0.54) | 0.07 (0.03–0.14) | 0.67 (0.60–0.75) | <0.001 |
| Flavonoid | ≤42.82 | 42.82–93.63 | >93.63 | ||
| Case/Control | 223/115 | 158/179 | 125/212 | ||
| Model 1 a | 1 | 0.45 (0.33–0.62) | 0.29 (0.20–0.40) | 0.91 (0.88–0.93) | <0.001 |
| Model 2 b | 1 | 0.40 (0.23–0.72) | 0.11 (0.05–0.23) | 0.85 (0.80–0.90) | <0.001 |
| Soy isoflavone | ≤1.66 | 1.66–6.33 | >6.33 | ||
| Case/Control | 189/149 | 208/129 | 109/228 | ||
| Model 1 a | 1 | 1.18 (0.85–1.64) | 0.35 (0.24–0.49) | 0.94 (0.92–0.96) | <0.001 |
| Model 2 b | 1 | 1.10 (0.64–1.91) | 0.29 (0.16–0.52) | 0.92 (0.89–0.95) | <0.001 |
| Anthocyanin | 247/91 | 200/137 | 59/278 | ||
| Case/Control | ≤2.76 | 2.76–7.57 | >7.57 | ||
| Model 1 a | 1 | 0.54 (0.38–0.78) | 0.07 (0.05–0.12) | 0.84 (0.81–0.87) | <0.001 |
| Model 2 b | 1 | 0.40 (0.21–0.74) | 0.05 (0.02–0.10) | 0.83 (0.78–0.87) | <0.001 |
| Resveratrol | ≤289.85 | 289.85–848.88 | >848.88 | ||
| Case/Control | 216/122 | 179/158 | 111/226 | ||
| Model 1 a | 1 | 0.60 (0.43–0.83) | 0.27 (0.19–0.38) | 0.79 (0.73–0.86) | <0.001 |
| Model 2 b | 1 | 0.52 (0.29–0.90) | 0.18 (0.10–0.35) | 0.84 (0.75–0.95) | <0.001 |
| Pathological Classification c | Model 1 a | p Value | Model 2 b | p-Value |
|---|---|---|---|---|
| Astrocytoma | ||||
| Carotene | 0.70 (0.60–0.81) | <0.001 | 0.33 (0.16–0.67) | 0.003 |
| Flavonoid | 0.91 (0.86–0.96) | 0.001 | 0.77 (0.65–0.92) | 0.003 |
| Soy isoflavone | 0.90 (0.85–0.96) | 0.001 | 0.77 (0.66–0.91) | 0.002 |
| Anthocyanin | 0.74 (0.65–0.84) | <0.001 | 0.71 (0.57–0.88) | 0.001 |
| Resveratrol | 0.67 (0.53–0.86) | 0.001 | 0.50 (0.30–0.85) | 0.011 |
| Glioblastoma | ||||
| Carotene | 0.79 (0.74–0.86) | <0.001 | 0.72 (0.61–0.85) | <0.001 |
| Flavonoid | 0.91 (0.88–0.95) | <0.001 | 0.85 (0.77–0.94) | 0.001 |
| Soy isoflavone | 0.94 (0.91–0.97) | <0.001 | 0.88 (0.81–0.95) | 0.001 |
| Anthocyanin | 0.86 (0.82–0.90) | <0.001 | 0.82 (0.74–0.91) | <0.001 |
| Resveratrol | 0.84 (0.75–0.93) | 0.001 | 0.84 (0.69–1.04) | 0.103 |
| Glioma Grading c | Model 1 a | p Value | Model 2 b | p-Value |
|---|---|---|---|---|
| Low grade | ||||
| Carotene | 0.71 (0.61–0.83) | <0.001 | 0.23 (0.08–0.62) | 0.004 |
| Flavonoid | 0.91 (0.86–0.97) | 0.002 | 0.82 (0.70–0.95) | 0.009 |
| Soy isoflavone | 0.94 (0.90–0.99) | 0.009 | 0.95 (0.89–1.02) | 0.171 |
| Anthocyanin | 0.81 (0.74–0.89) | <0.001 | 0.69 (0.55–0.86) | 0.001 |
| Resveratrol | 0.81 (0.69–0.95) | 0.011 | 0.83 (0.62–1.11) | 0.205 |
| High grade | ||||
| Carotene | 0.78 (0.73–0.83) | <0.001 | 0.69 (0.60–0.80) | <0.001 |
| Flavonoid | 0.91 (0.88–0.94) | <0.001 | 0.80 (0.74–0.88) | <0.001 |
| Soy isoflavone | 0.94 (0.91–0.97) | <0.001 | 0.91 (0.86–0.96) | 0.001 |
| Anthocyanin | 0.84 (0.80–0.88) | <0.001 | 0.79 (0.72–0.86) | <0.001 |
| Resveratrol | 0.78 (0.70–0.87) | <0.001 | 0.75 (0.63–0.90) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, W.; Wang, C.; Chen, F.; He, Y.; Yin, S.; Peng, Y.; Li, W. Phytochemicals and Glioma: Results from Dietary Mixed Exposure. Brain Sci. 2023, 13, 902. https://doi.org/10.3390/brainsci13060902
Zhang W, Wang C, Chen F, He Y, Yin S, Peng Y, Li W. Phytochemicals and Glioma: Results from Dietary Mixed Exposure. Brain Sciences. 2023; 13(6):902. https://doi.org/10.3390/brainsci13060902
Chicago/Turabian StyleZhang, Weichunbai, Ce Wang, Feng Chen, Yongqi He, Shuo Yin, Yue Peng, and Wenbin Li. 2023. "Phytochemicals and Glioma: Results from Dietary Mixed Exposure" Brain Sciences 13, no. 6: 902. https://doi.org/10.3390/brainsci13060902