

Down-Regulation of Tinnitus Negative Valence via Concurrent HD-tDCS and PEI Technique: A Pilot Study

 , , , , and
, , , , and
Abstract
:1. Introduction
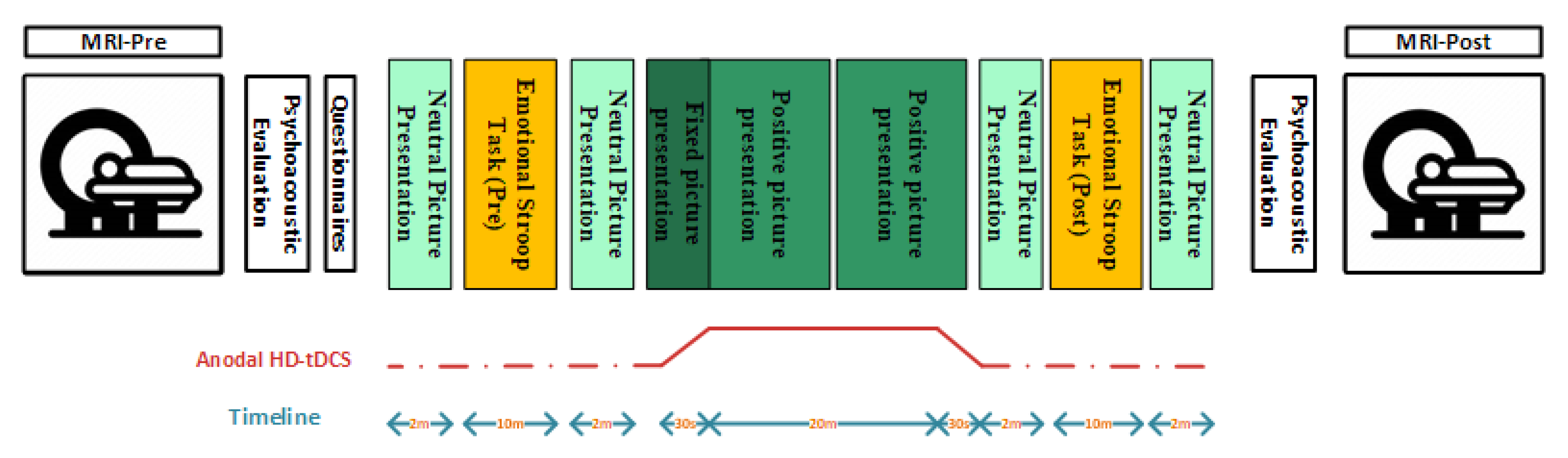
2. Methods
2.1. Subjects
2.2. Audiological Profile
2.3. Behavioral Profile
2.4. High-Definition Transcranial Direct Current Stimulation
2.5. Positive Emotion Induction
2.6. MR Acquisition
2.7. MR Data Preprocessing
2.8. Processing/Functional Data Analysis
3. Results
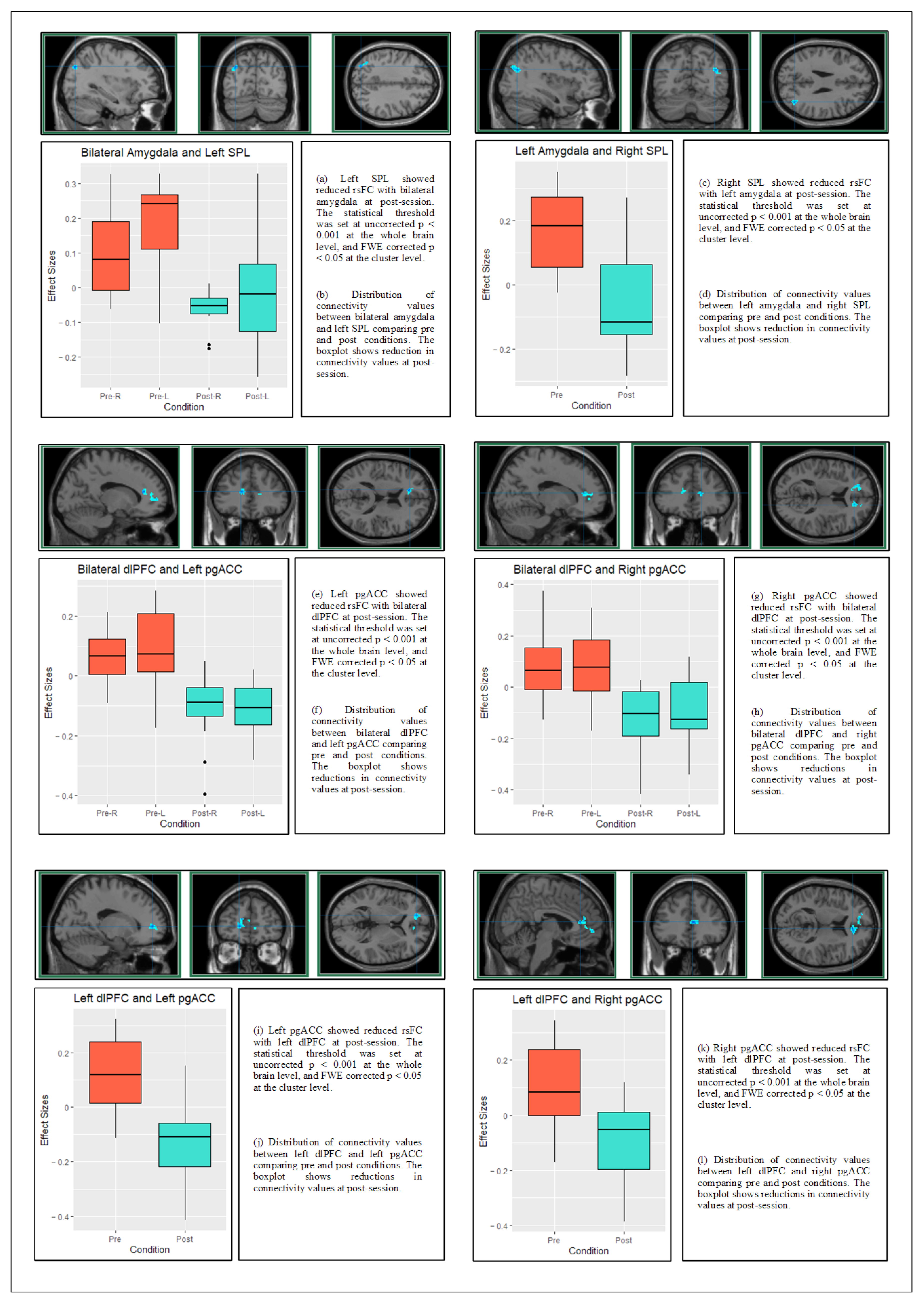
3.1. Effects on Neural Correlates: Resting-State Functional Connectivity
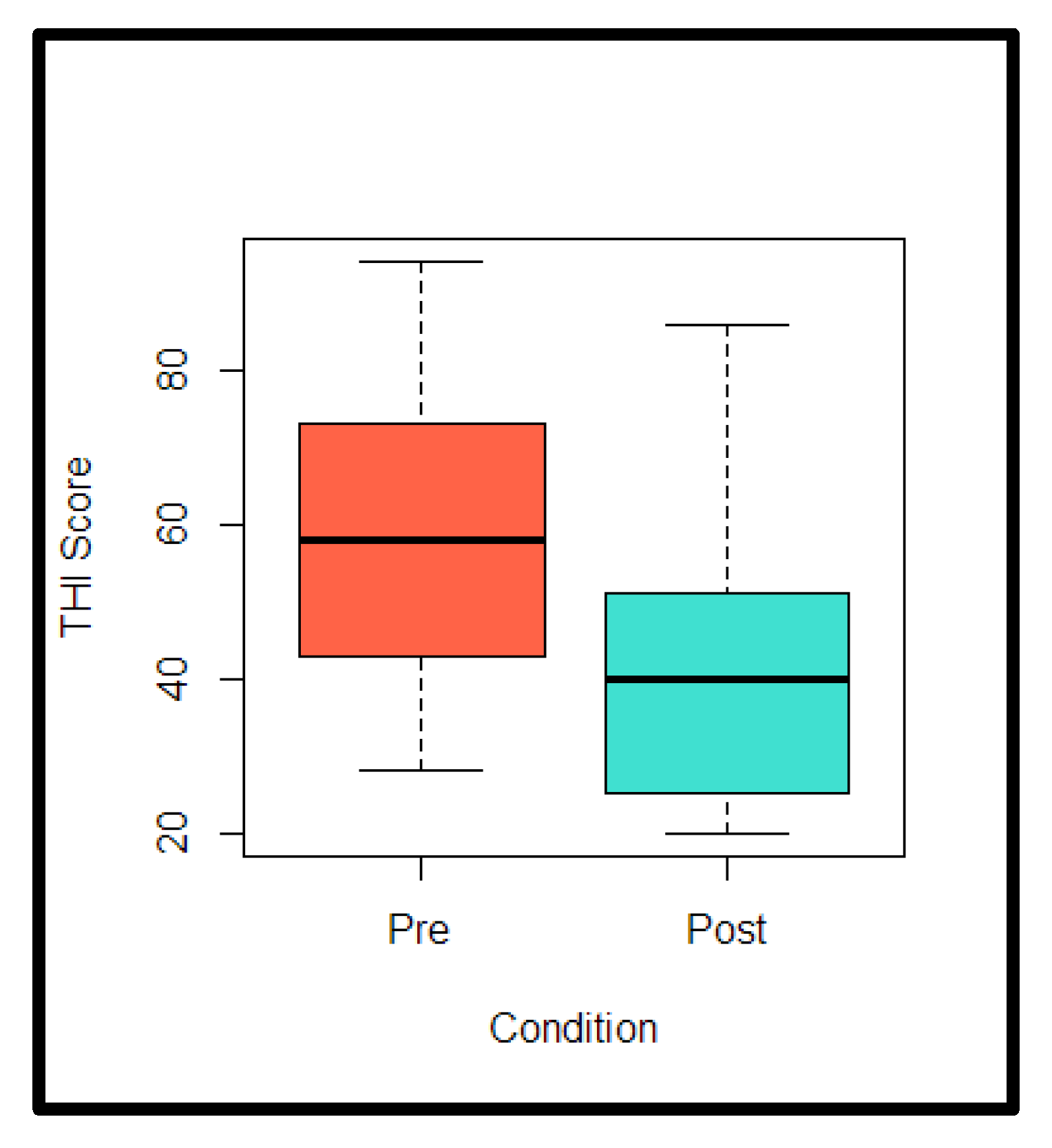
3.2. Effects on Behavioral Correlates: Tinnitus Handicap Inventory
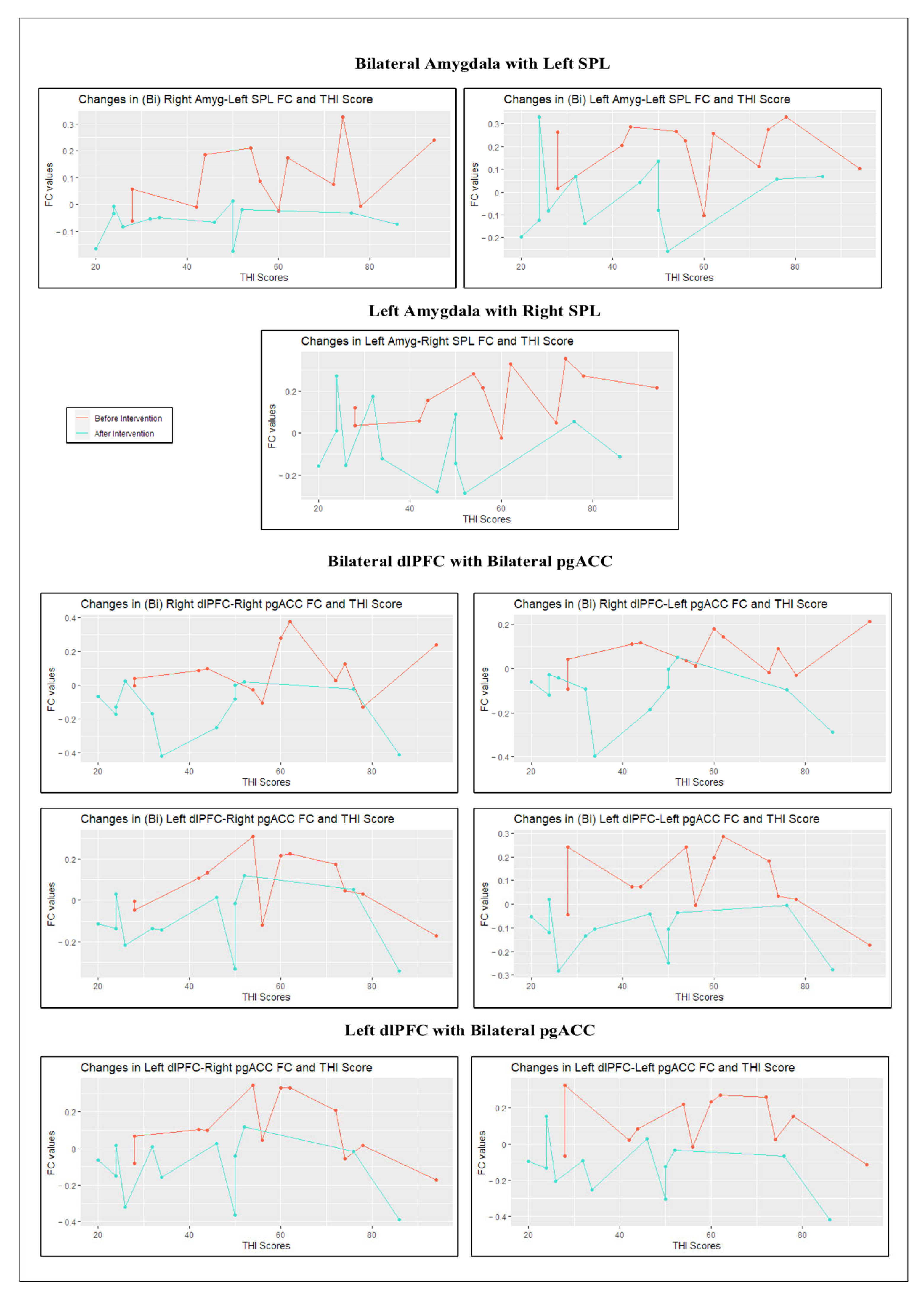
3.3. Effects on FC-THI Relationship
4. Discussion
4.1. Neural Correlate
4.2. Amygdala–SPL
4.3. dlPFC-pgACC
4.4. Behavioral Correlate
4.5. Neurofunctional Tinnitus Model
5. Conclusions
6. Limitations and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ghodratitoostani, I.; Zana, Y.; Delbem, A.C.B.; Sani, S.S.; Ekhtiari, H.; Sanchez, T.G. Theoretical Tinnitus Framework: A Neurofunctional Model. Front. Neurosci. 2016, 10, 370. [Google Scholar] [CrossRef] [PubMed]
- Hébert, S.; Canlon, B.; Hasson, D.; Hanson, L.L.M.; Westerlund, H.; Theorell, T. Tinnitus severity is reduced with reduction of depressive mood—A prospective population study in Sweden. PLoS ONE 2012, 7, e37733. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, L. The epidemiology of tinnitus. Audiol. Med. 2004, 2, 8–17. [Google Scholar] [CrossRef]
- Jastreboff, P.J. Phantom auditory perception (tinnitus): Mechanisms of generation and perception. Neurosci. Res. 1990, 8, 221–254. [Google Scholar] [CrossRef]
- Zenner, H.P.; Pfister, M.; Birbaumer, N. Tinnitus sensitization: Sensory and psychophysiological aspects of a new pathway of acquired centralization of chronic tinnitus. Otol. Neurotol. 2006, 27, 1054–1063. [Google Scholar] [CrossRef]
- McKenna, L.; Handscomb, L.; Hoare, D.; Hall, D. A scientific cognitive-behavioral model of tinnitus: Novel conceptualizations of tinnitus distress. Front. Neurol. 2014, 5, 196. [Google Scholar] [CrossRef]
- Hallam, R.; McKenna, L.; Shurlock, L. Tinnitus impairs cognitive efficiency. Int. J. Audiol. 2004, 43, 218–226. [Google Scholar] [CrossRef]
- Zenner, H.-P.; Zalaman, I.M. Cognitive tinnitus sensitization: Behavioral and neurophysiological aspects of tinnitus centralization. Acta Oto-Laryngol. 2004, 124, 436–439. [Google Scholar] [CrossRef]
- Davidson, R.J.; Putnam, K.M.; Larson, C.L. Dysfunction in the neural circuitry of emotion regulation—A possible prelude to violence. Science 2000, 289, 591–594. [Google Scholar] [CrossRef]
- Alves, N.T.; Fukusima, S.S.; Aznar-Casanova, J.A. Models of brain asymmetry in emotional processing. Psychol. Neurosci. 2008, 1, 63–66. [Google Scholar]
- Herrington, J.D.; Mohanty, A.; Koven, N.S.; Fisher, J.E.; Stewart, J.L.; Banich, M.T.; Webb, A.G.; Miller, G.A.; Heller, W. Emotion-modulated performance and activity in left dorsolateral prefrontal cortex. Emotion 2005, 5, 200. [Google Scholar] [CrossRef] [PubMed]
- Jackson, D.C.; Mueller, C.J.; Dolski, I.; Dalton, K.M.; Nitschke, J.B.; Urry, H.L.; Davidson, R.J. Now you feel it, now you don’t: Frontal brain electrical asymmetry and individual differences in emotion regulation. Psychol. Sci. 2003, 14, 612–617. [Google Scholar] [CrossRef]
- Jackson, D.C.; Burghy, C.A.; Hanna, A.J.; Larson, C.L.; Davidson, R.J. Resting frontal and anterior temporal EEG asymmetry predicts ability to regulate negative emotion. In Psychophysiology; Cambridge Univ Press: New York, NY, USA, 2000. [Google Scholar]
- Weissman, J.L.; Hirsch, B.E. Imaging of tinnitus: A review. Radiology 2000, 216, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Ochsner, K.N.; Bunge, S.A.; Gross, J.J.; Gabrieli, J.D.E. Rethinking feelings: An FMRI study of the cognitive regulation of emotion. J. Cogn. Neurosci. 2002, 14, 1215–1229. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.; Siebner, H.R.; Ward, N.S.; Lee, L.; Nitsche, M.A.; Paulus, W.; Frackowiak, R.S. How does transcranial DC stimulation of the primary motor cortex alter regional neuronal activity in the human brain? Eur. J. Neurosci. 2005, 22, 495–504. [Google Scholar] [CrossRef]
- Fregni, F.; Boggio, P.S.; Nitsche, M.; Bermpohl, F.; Antal, A.; Feredoes, E.; Marcolin, M.A.; Rigonatti, S.P.; Silva, M.T.; Paulus, W.; et al. Anodal transcranial direct current stimulation of prefrontal cortex enhances working memory. Exp. Brain Res. 2005, 166, 23–30. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633. [Google Scholar] [CrossRef]
- Vanneste, S.; Plazier, M.; Van Der Loo, E.; Van de Heyning, P.; Congedo, M.; De Ridder, D. The neural correlates of tinnitus-related distress. Neuroimage 2010, 52, 470–480. [Google Scholar] [CrossRef]
- Vanneste, S.; De Ridder, D. Bifrontal transcranial direct current stimulation modulates tinnitus intensity and tinnitus-distress-related brain activity. Eur. J. Neurosci. 2011, 34, 605–614. [Google Scholar] [CrossRef]
- Teismann, H.; Wollbrink, A.; Okamoto, H.; Schlaug, G.; Rudack, C.; Pantev, C. Combining transcranial direct current stimulation and tailor-made notched music training to decrease tinnitus-related distress—A pilot study. PLoS ONE 2014, 9, e89904. [Google Scholar] [CrossRef]
- Yadollahpour, A.; Mayo, M.; Saki, N.; Rashidi, S.; Bayat, A. A chronic protocol of bilateral transcranial direct current stimulation over auditory cortex for tinnitus treatment: Dataset from a double-blinded randomized controlled trial. F1000Research 2018, 7, 733. [Google Scholar] [CrossRef] [PubMed]
- Martins, M.L.; Souza, D.D.S.; Cavalcante, M.E.d.O.B.; Barboza, H.N.; de Medeiros, J.F.; Andrade, S.M.M.D.S.; Machado, D.G.D.S.; da Rosa, M.R.D. Effect of transcranial direct current stimulation for tinnitus treatment: A systematic review and meta-analysis. Neurophysiol. Clin. 2022, 52, 1–16. [Google Scholar] [CrossRef]
- Lefebvre-Demers, M.; Doyon, N.; Fecteau, S. Non-invasive neuromodulation for tinnitus: A meta-analysis and modeling studies. Brain Stimul. 2021, 14, 113–128. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.P.; Teixeira, V.N.; Dall’igna, C.; Dallagnol, D.; Smith, M.M. Brazilian Portuguese Language version of the” Tinnitus Handicap Inventory”: Validity and reproducibility. Braz. J. Otorhinolaryngol. 2006, 72, 808–810. [Google Scholar] [CrossRef] [PubMed]
- Carpenter-Thompson, J.R.; Schmidt, S.; McAuley, E.; Husain, F.T. Increased frontal response may underlie decreased tinnitus severity. PLoS ONE 2015, 10, e0144419. [Google Scholar] [CrossRef]
- Ghodratitoostani, I.; Gonzatto, O.A.J.; Vaziri, Z.; Delbem, A.C.B.; Makkiabadi, B.; Datta, A.; Thomas, C.; Hyppolito, M.A.; Santos, A.C.D.; Louzada, F.; et al. Dose-Response Transcranial Electrical Stimulation Study Design: A Well-Controlled Adaptive Seamless Bayesian Method to Illuminate Negative Valence Role in Tinnitus Perception. Front. Hum. Neurosci. 2022, 16, 811550. [Google Scholar] [CrossRef]
- Fioravanti-Bastos, A.C.M.; Cheniaux, E.; Landeira-Fernandez, J. Development and validation of a short-form version of the Brazilian state-trait anxiety inventory. Psicol. Reflexão Crítica 2011, 24, 485–494. [Google Scholar] [CrossRef]
- Rondinoni, C.; Amaro, E., Jr.; Cendes, F.; Santos, A.; Salmon, C.; Amaro, E. Effect of scanner acoustic background noise on strict resting-state fMRI. Braz. J. Med. Biol. Res. 2013, 46, 359–367. [Google Scholar] [CrossRef]
- Whitfield-Gabrieli, S.; Nieto-Castanon, A. Conn: A functional connectivity toolbox for correlated and anticorrelated brain networks. Brain Connect. 2012, 2, 125–141. [Google Scholar] [CrossRef]
- Nieto-Castanon, A. Handbook of Functional Connectivity Magnetic Resonance Imaging Methods in CONN; Hilbert Press: Boston, MA, USA, 2020. [Google Scholar]
- Fassbender, C.; Simoes-Franklin, C.; Murphy, K.; Hester, R.; Meaney, J.F.; Robertson, I.; Garavan, H. The role of a right fronto-parietal network in cognitive control. J. Psychophysiol. 2006, 20, 286–296. [Google Scholar] [CrossRef]
- Golm, D.; Schmidt-Samoa, C.; Dechent, P.; Kröner-Herwig, B. Neural correlates of tinnitus related distress: An fMRI-study. Hear. Res. 2013, 295, 87–99. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Vanneste, S.; Congedo, M. The distressed brain: A group blind source separation analysis on tinnitus. PLoS ONE 2011, 6, e24273. [Google Scholar] [CrossRef] [PubMed]
- Shahsavarani, S.; Schmidt, S.A.; Khan, R.A.; Tai, Y.; Husain, F.T. Salience, emotion, and attention: The neural networks underlying tinnitus distress revealed using music and rest. Brain Res. 2021, 1755, 147277. [Google Scholar] [CrossRef]
- Schmidt, S.A.; Akrofi, K.; Carpenter-Thompson, J.R.; Husain, F.T. Default mode, dorsal attention and auditory resting state networks exhibit differential functional connectivity in tinnitus and hearing loss. PLoS ONE 2013, 8, e76488. [Google Scholar] [CrossRef] [PubMed]
- Brett, M.; Anton, J.L.; Valabregue, R.; Poline, J.B. Region of interest analysis using an SPM toolbox. In Proceedings of the 8th International Conference on Functional Mapping of The human Brain, Sendai, Japan, 2 June 2002. [Google Scholar]
- Team, R. RStudio: Integrated Development Environment for R, 1.4. 1106. R Studio; PBC: Boston, MA, USA, 2021. [Google Scholar]
- Ghodratitoostani, I.; Delbem, A.C.B.; Torabi-Nami, M.; Makkiabadi, B.; Jalilvand, H.; Sanchez, T.G. Theoretical tinnitus multimodality framework: A neurofunctional model. J. Adv. Med. Sci. Appl. Technol. 2016, 2, 181–189. [Google Scholar] [CrossRef]
- Dumais, K.M.; Chernyak, S.; Nickerson, L.D.; Janes, A.C. Sex differences in default mode and dorsal attention network engagement. PLoS ONE 2018, 13, e0199049. [Google Scholar] [CrossRef] [PubMed]
- Dixon, M.L.; Andrews-Hanna, J.R.; Spreng, R.N.; Irving, Z.C.; Mills, C.; Girn, M.; Christoff, K. Interactions between the default network and dorsal attention network vary across default subsystems, time, and cognitive states. Neuroimage 2017, 147, 632–649. [Google Scholar] [CrossRef]
- Brissenden, J.A.; Levin, E.J.; Osher, D.E.; Halko, M.A.; Somers, D.C. Functional evidence for a cerebellar node of the dorsal attention network. J. Neurosci. 2016, 36, 6083–6096. [Google Scholar] [CrossRef]
- Behrmann, M.; Geng, J.J.; Shomstein, S. Parietal cortex and attention. Curr. Opin. Neurobiol. 2004, 14, 212–217. [Google Scholar] [CrossRef]
- Mantini, D.; Perrucci, M.G.; Del Gratta, C.; Romani, G.L.; Corbetta, M. Electrophysiological signatures of resting state networks in the human brain. Proc. Natl. Acad. Sci. USA 2007, 104, 13170–13175. [Google Scholar] [CrossRef]
- Hu, H.; Lyu, Y.; Li, S.; Yuan, Z.; Ye, C.; Han, Z.; Lin, G. Aberrant Resting-State Functional Connectivity of the Dorsal Attention Network in Tinnitus. Neural Plast. 2021, 2021, 2804533. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Zanao, T.A.; Vanderhasselt, M.-A.; Valiengo, L.; de Oliveira, J.F.; Boggio, P.S.; Lotufo, P.A.; Benseñor, I.M.; Fregni, F. Enhancement of affective processing induced by bifrontal transcranial direct current stimulation in patients with major depression. Neuromodulation Technol. Neural Interface 2014, 17, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.T.; Basanovic, J.; Notebaert, L.; MacLeod, C.; Clarke, P.J. Attentional bias mediates the effect of neurostimulation on emotional vulnerability. J. Psychiatr. Res. 2017, 93, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Ironside, M.; Browning, M.; Ansari, T.L.; Harvey, C.J.; Sekyi-Djan, M.N.; Bishop, S.J.; Harmer, C.J.; O’Shea, J. Effect of prefrontal cortex stimulation on regulation of amygdala response to threat in individuals with trait anxiety: A randomized clinical trial. JAMA Psychiatry 2019, 76, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Bush, G.; Luu, P.; Posner, M.I. Cognitive and emotional influences in anterior cingulate cortex. Trends Cogn. Sci. 2000, 4, 215–222. [Google Scholar] [CrossRef]
- Vogt, B.A.; Nimchinsky, E.A.; Vogt, L.J.; Hof, P.R. Human cingulate cortex: Surface features, flat maps, and cytoarchitecture. J. Comp. Neurol. 1995, 359, 490–506. [Google Scholar] [CrossRef]
- Amemori, K.I.; Graybiel, A.M. Localized microstimulation of primate pregenual cingulate cortex induces negative decision-making. Nat. Neurosci. 2012, 15, 776–785. [Google Scholar] [CrossRef]
- Bartra, O.; McGuire, J.T.; Kable, J.W. The valuation system: A coordinate-based meta-analysis of BOLD fMRI experiments examining neural correlates of subjective value. Neuroimage 2013, 76, 412–427. [Google Scholar] [CrossRef]
- Clithero, J.A.; Rangel, A. Informatic parcellation of the network involved in the computation of subjective value. Soc. Cogn. Affect. Neurosci. 2014, 9, 1289–1302. [Google Scholar] [CrossRef]
- Mesulam, M.-M. Spatial attention and neglect: Parietal, frontal and cingulate contributions to the mental representation and attentional targeting of salient extrapersonal events. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 1999, 354, 1325–1346. [Google Scholar] [CrossRef]
- Maddock, R.J. The retrosplenial cortex and emotion: New insights from functional neuroimaging of the human brain. Trends Neurosci. 1999, 22, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Posner, M.I.; Petersen, S.E. The attention system of the human brain. Annu. Rev. Neurosci. 1990, 13, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Armony, J.L.; Dolan, R.J. Modulation of spatial attention by fear-conditioned stimuli: An event-related fMRI study. Neuropsychologia 2002, 40, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Rolls, E.T. The orbitofrontal cortex. Philos. Trans. R. Soc. London Ser. B Biol. Sci. 1996, 351, 1433–1444. [Google Scholar]
- Vuilleumier, P.; Armony, J.; Dolan, R. Reciprocal links between emotion and attention. Hum. Brain Funct. 2003, 2, 419–444. [Google Scholar]
- Yukie, M.; Shibata, H. Interactions in the monkey. Cingulate Neurobiol. Dis. 2009, 145–162. [Google Scholar]
- Vogt, B.A.; Pandya, D.N. Cingulate cortex of the rhesus monkey: II. Cortical afferents. J. Comp. Neurol. 1987, 262, 271–289. [Google Scholar] [CrossRef]
- Pandya, D.N.; Van Hoesen, G.W.; Mesulam, M.-M. Efferent connections of the cingulate gyrus in the rhesus monkey. Exp. Brain Res. 1981, 42, 319–330. [Google Scholar] [CrossRef]
- Schlee, W.; Hartmann, T.; Langguth, B.; Weisz, N. Abnormal resting-state cortical coupling in chronic tinnitus. BMC Neurosci. 2009, 10, 11. [Google Scholar] [CrossRef]
- Song, J.J.; Vanneste, S.; De Ridder, D. Dysfunctional noise cancelling of the rostral anterior cingulate cortex in tinnitus patients. PLoS ONE 2015, 10, e0123538. [Google Scholar] [CrossRef]
- Song, J.-J.; Vanneste, S.; Schlee, W.; Van de Heyning, P.; De Ridder, D. Onset-related differences in neural substrates of tinnitus-related distress: The anterior cingulate cortex in late-onset tinnitus, and the frontal cortex in early-onset tinnitus. Brain Struct. Funct. 2015, 220, 571–584. [Google Scholar] [CrossRef] [PubMed]
- Peña-Gómez, C.; Vidal-Piñeiro, D.; Clemente, I.C.; Leone, P.; Bartrés-Faz, D. Down-regulation of negative emotional processing by transcranial direct current stimulation: Effects of personality characteristics. PLoS ONE 2011, 6, e22812. [Google Scholar] [CrossRef] [PubMed]
- Boggio, P.S.; Zaghi, S.; Fregni, F. Modulation of emotions associated with images of human pain using anodal transcranial direct current stimulation (tDCS). Neuropsychologia 2009, 47, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Clarke, P.J.F.; Van Bockstaele, B.; Marinovic, W.; Howell, J.A.; Boyes, M.E.; Notebaert, L. The effects of left DLPFC tDCS on emotion regulation, biased attention, and emotional reactivity to negative content. Cogn. Affect. Behav. Neurosci. 2020, 20, 1323–1335. [Google Scholar] [CrossRef]
- Rêgo, G.G.; Lapenta, O.M.; Marques, L.M.; Costa, T.L.; Leite, J.; Carvalho, S.; Gonçalves, F.; Brunoni, A.R.; Fregni, F.; Boggio, P.S. Hemispheric dorsolateral prefrontal cortex lateralization in the regulation of empathy for pain. Neurosci. Lett. 2015, 594, 12–16. [Google Scholar] [CrossRef]
- Dedoncker, J.; Brunoni, A.R.; Baeken, C.; Vanderhasselt, M.-A. A systematic review and meta-analysis of the effects of transcranial direct current stimulation (tDCS) over the dorsolateral prefrontal cortex in healthy and neuropsychiatric samples: Influence of stimulation parameters. Brain Stimul. 2016, 9, 501–517. [Google Scholar] [CrossRef]
- Frank, E.; Schecklmann, M.; Landgrebe, M.; Burger, J.; Kreuzer, P.; Poeppl, T.B.; Kleinjung, T.; Hajak, G.; Langguth, B. Treatment of chronic tinnitus with repeated sessions of prefrontal transcranial direct current stimulation: Outcomes from an open-label pilot study. J. Neurol. 2012, 259, 327–333. [Google Scholar] [CrossRef]
- Vanneste, S.; Plazier, M.; Ost, J.; van der Loo, E.; Van de Heyning, P.; De Ridder, D. Bilateral dorsolateral prefrontal cortex modulation for tinnitus by transcranial direct current stimulation: A preliminary clinical study. Exp. Brain Res. 2010, 202, 779–785. [Google Scholar] [CrossRef]
- Faber, M.; Vanneste, S.; Fregni, F.; De Ridder, D. Top down prefrontal affective modulation of tinnitus with multiple sessions of tDCS of dorsolateral prefrontal cortex. Brain Stimul. 2012, 5, 492–498. [Google Scholar] [CrossRef]
- Uhrig, M.K.; Etrautmann, N.; Ebaumgärtner, U.; Etreede, R.-D.; Ehenrich, F.; Ehiller, W.; Emarschall, S. Emotion elicitation: A comparison of pictures and films. Front. Psychol. 2016, 7, 180. [Google Scholar] [CrossRef]
- Menon, V.; Uddin, L.Q. Saliency, switching, attention and control: A network model of insula function. Brain Struct. Funct. 2010, 214, 655–667. [Google Scholar] [CrossRef] [PubMed]
- Elton, A.; Gao, W. Divergent task-dependent functional connectivity of executive control and salience networks. Cortex 2014, 51, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Viinikainen, M.; Kätsyri, J.; Sams, M. Representation of perceived sound valence in the human brain. Hum. Brain Mapp. 2012, 33, 2295–2305. [Google Scholar] [CrossRef] [PubMed]
- Anders, S.; Lotze, M.; Erb, M.; Grodd, W.; Birbaumer, N. Brain activity underlying emotional valence and arousal: A response-related fMRI study. Hum. Brain Mapp. 2004, 23, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Husain, F.T. Neural networks of tinnitus in humans: Elucidating severity and habituation. Hear. Res. 2016, 334, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Pessoa, L. Understanding brain networks and brain organization. Phys. Life Rev. 2014, 11, 400–435. [Google Scholar] [CrossRef] [PubMed]
- Carpenter-Thompson, J.R.; Akrofi, K.; Schmidt, S.A.; Dolcos, F.; Husain, F.T. Alterations of the emotional processing system may underlie preserved rapid reaction time in tinnitus. Brain Res. 2014, 1567, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Friston, K.; Frith, C.; Liddle, P.F.; Frackowiak, R. Functional connectivity: The principal-component analysis of large (PET) data sets. J. Cereb. Blood Flow Metab. 1993, 13, 5–14. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Tinnitus Duration (Years) | THI | State Anxiety Scores—STAI | LMT dB HL | PTA (dB HL) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Loudness Pre | Loudness Post | ||||||||
| 1st Session | Last Session | 1st Session | Last Session | 1st Session | Last Session | ||||
| mean | 51.2 | 9 | 57.7 | 43.3 | 46.9 | 39.5 | 54 | 47.7 | 34.5 |
| SD | 12.9 | 5 | 20.1 | 21.0 | 15.3 | 9.8 | 9.5 | 12.8 | 12.7 |
| p-value | 0.018 | 0.056 | 0.049 | ||||||
| Network | Seeds | MNI Coordinates | ||
|---|---|---|---|---|
| x | y | z | ||
| EmotionProcessing | Right amygdala Left amygdala | 18 −17 | −7 −2 | −17 −24 |
| Fronto-Parietal Network (FPN) | Right dorsolateral prefrontal cortex Left dorsolateral prefrontal cortex | 41 −43 | 38 33 | 30 28 |
| Cingulo-opercular network (CON) | Right anterior insula Left anterior insula | 47 −44 | 14 13 | 0 1 |
| Auditory Network (AN) | Right primary auditory cortex Left primary auditory cortex | 41 −55 | −27 −22 | 6 9 |
| Dorsal Attention Network 1 (DAN−1) | Right posterior intraparietal sulcus Left posterior intraparietal sulcus | 26 −23 | −62 −70 | 53 46 |
| Dorsal Attention Network 2 (DAN-2) | Right frontal eye field Left frontal eye field | 27 −25 | −11 −11 | 54 54 |
| Default Mode Network (DMN) | Medial prefrontal cortex Posterior cingulate cortex | 8 −2 | 59 −50 | 19 25 |
| Network | Seeds | Region | BA | Cluster Size | Peak MNI Coordinates | Peak Intensity | Cluster-Level p FWE-Corrected | CoG * Regions | ||
|---|---|---|---|---|---|---|---|---|---|---|
| x | y | z | ||||||||
| Emotion Processing | Bilateral Amygdala | L SPL | 113 | −32 | −76 | 36 | −6.80 | 0.004 * | L Parietal Lobe | |
| Left Amygdala | R SPL | 79 | 38 | −68 | 28 | −6.58 | 0.038 | R Posterior MTG | ||
| Fronto-Parietal Network | Bilateral dlPFC | L pgACC | 10/32 | 206 | −14 | 36 | 16 | −7.03 | 0.00008 ** | L MFG-BA 10 |
| R pgACC | 32 | 107 | 16 | 38 | 12 | −5.80 | 0.0086 * | R MFG-ACC | ||
| Left dlPFC | R Sup. pgACC | 32 | 145 | 6 | 36 | 12 | −7.41 | 0.00084 ** | R PreACC-BA32 | |
| L pgACC | 10 | 113 | −16 | 50 | 4 | −6.87 | 0.0045 * | L Superior MFG | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaziri, Z.; Salmon, C.E.G.; Ghodratitoostani, I.; Santos, A.C.d.; Hyppolito, M.A.; Delbem, A.C.B.; Leite, J.P. Down-Regulation of Tinnitus Negative Valence via Concurrent HD-tDCS and PEI Technique: A Pilot Study. Brain Sci. 2023, 13, 826. https://doi.org/10.3390/brainsci13050826
Vaziri Z, Salmon CEG, Ghodratitoostani I, Santos ACd, Hyppolito MA, Delbem ACB, Leite JP. Down-Regulation of Tinnitus Negative Valence via Concurrent HD-tDCS and PEI Technique: A Pilot Study. Brain Sciences. 2023; 13(5):826. https://doi.org/10.3390/brainsci13050826
Chicago/Turabian StyleVaziri, Zahra, Carlos E. G. Salmon, Iman Ghodratitoostani, Antonio Carlos dos Santos, Miguel A. Hyppolito, Alexandre C. B. Delbem, and João P. Leite. 2023. "Down-Regulation of Tinnitus Negative Valence via Concurrent HD-tDCS and PEI Technique: A Pilot Study" Brain Sciences 13, no. 5: 826. https://doi.org/10.3390/brainsci13050826