
Combined Use of Frameless Neuronavigation and In Situ Optical Guidance in Brain Tumor Needle Biopsies

Abstract
:1. Introduction
2. Materials and Methods
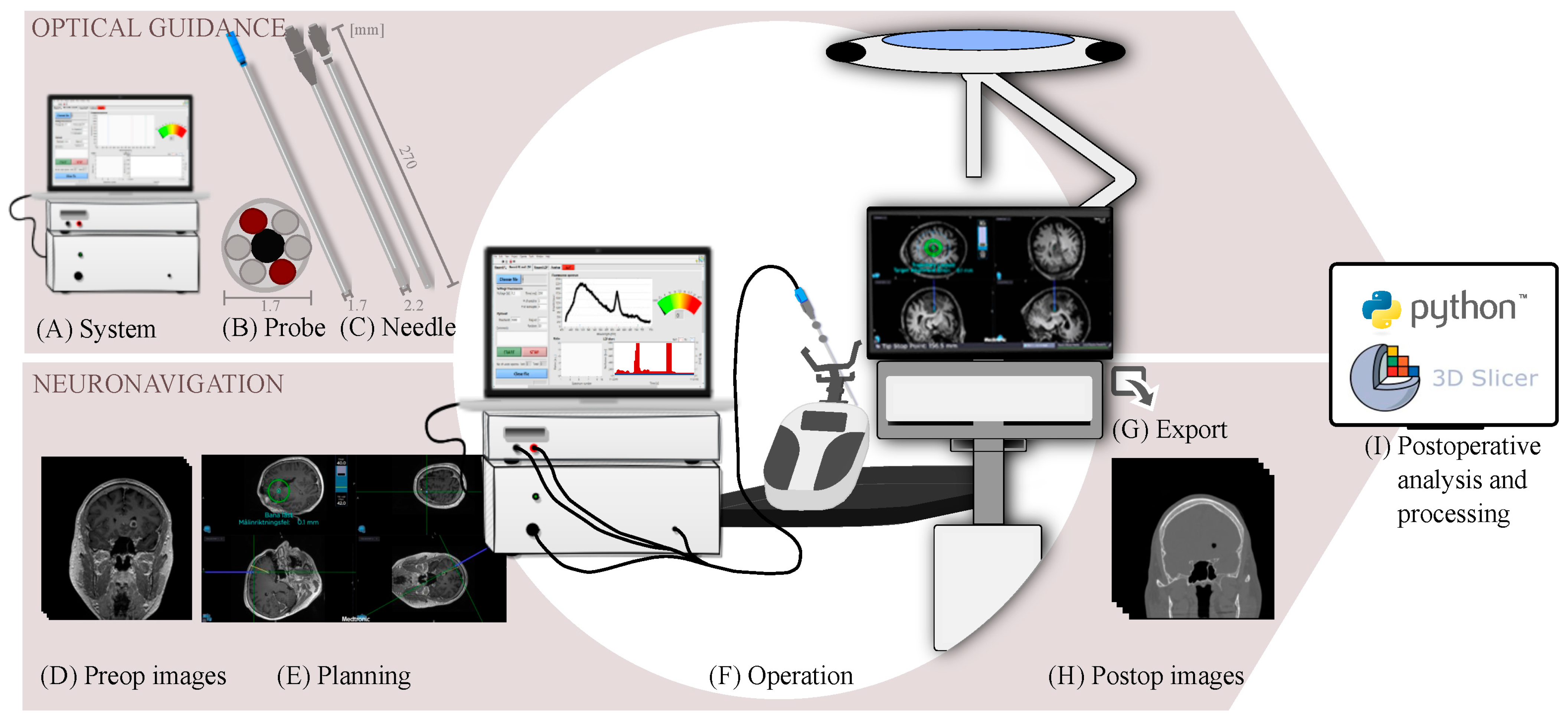
2.1. Optical Guidance
2.1.1. System Development
2.1.2. Probe Redesign
2.1.3. Evaluation of System Dynamics
2.2. Neuronavigation
2.2.1. Image Acquisition
2.2.2. Frameless Navigation
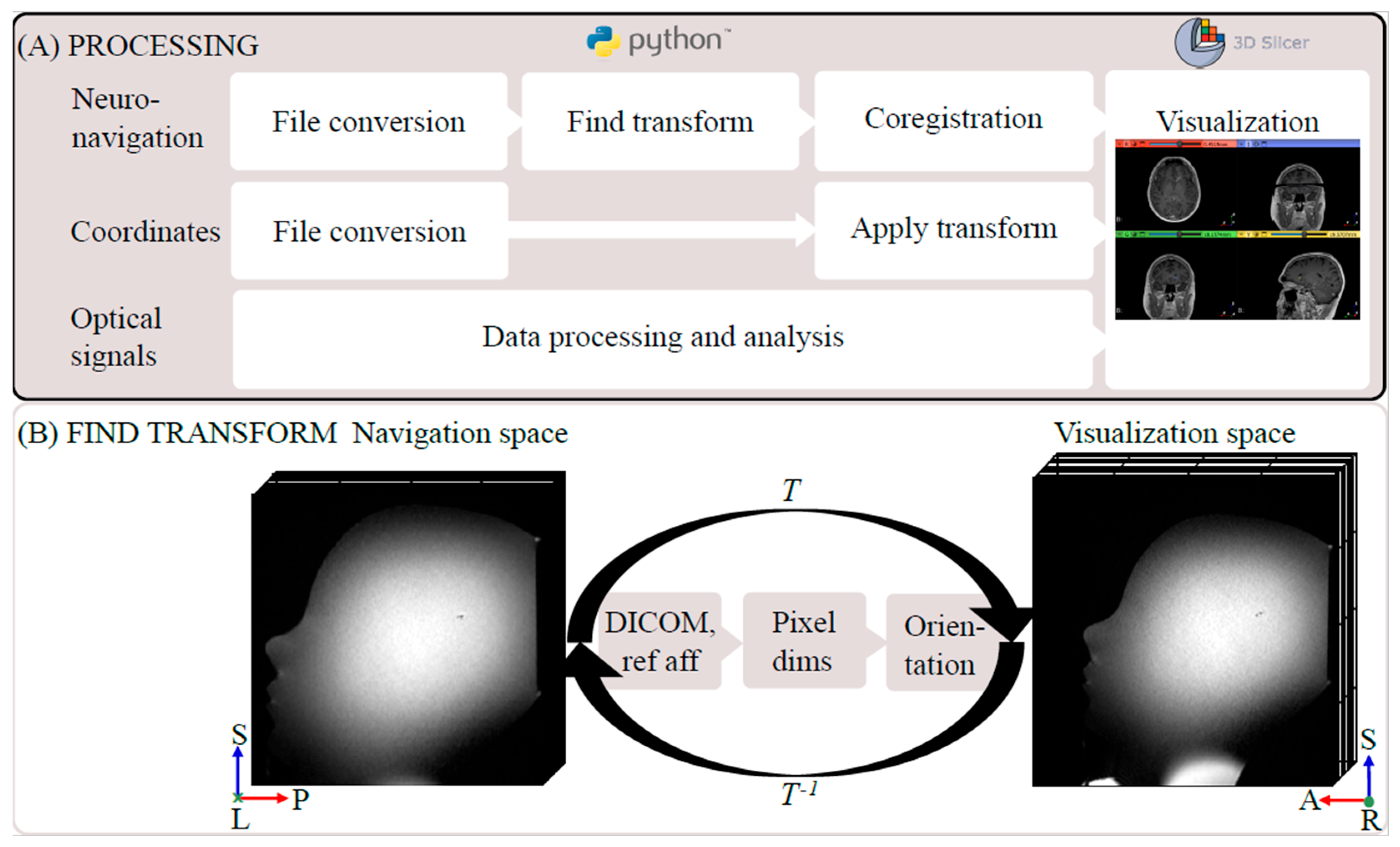
2.2.3. Coordinate Transform and Image Coregistration
2.2.4. Phantom Evaluation
2.3. Combined Evaluation
2.3.1. Patients
2.3.2. Frameless Neuronavigation with Optical Measurements
2.3.3. Postoperative Analysis and Visualization
3. Results
3.1. Optical System Dynamics
3.2. Phantom Neuronavigation and Transform
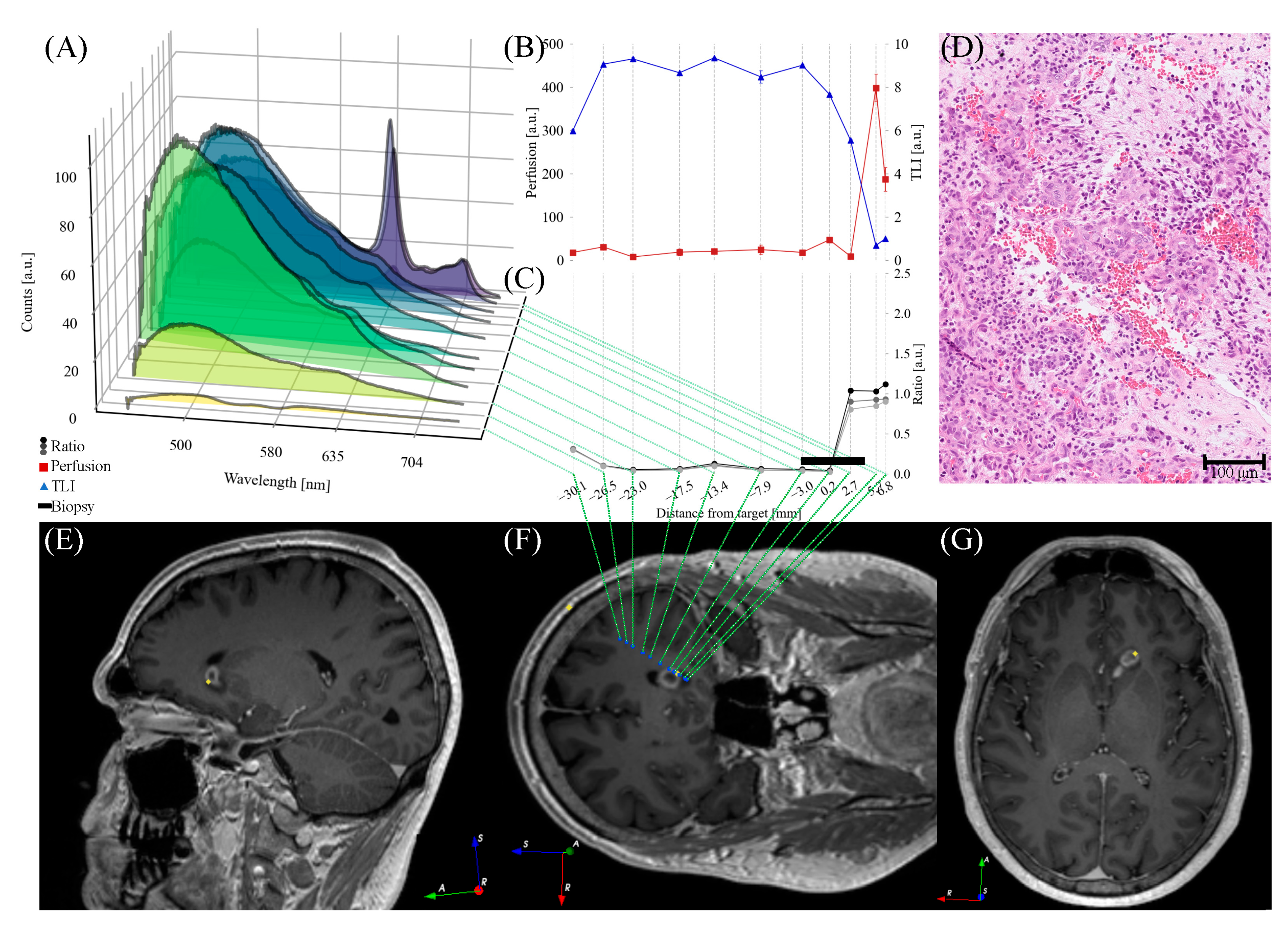
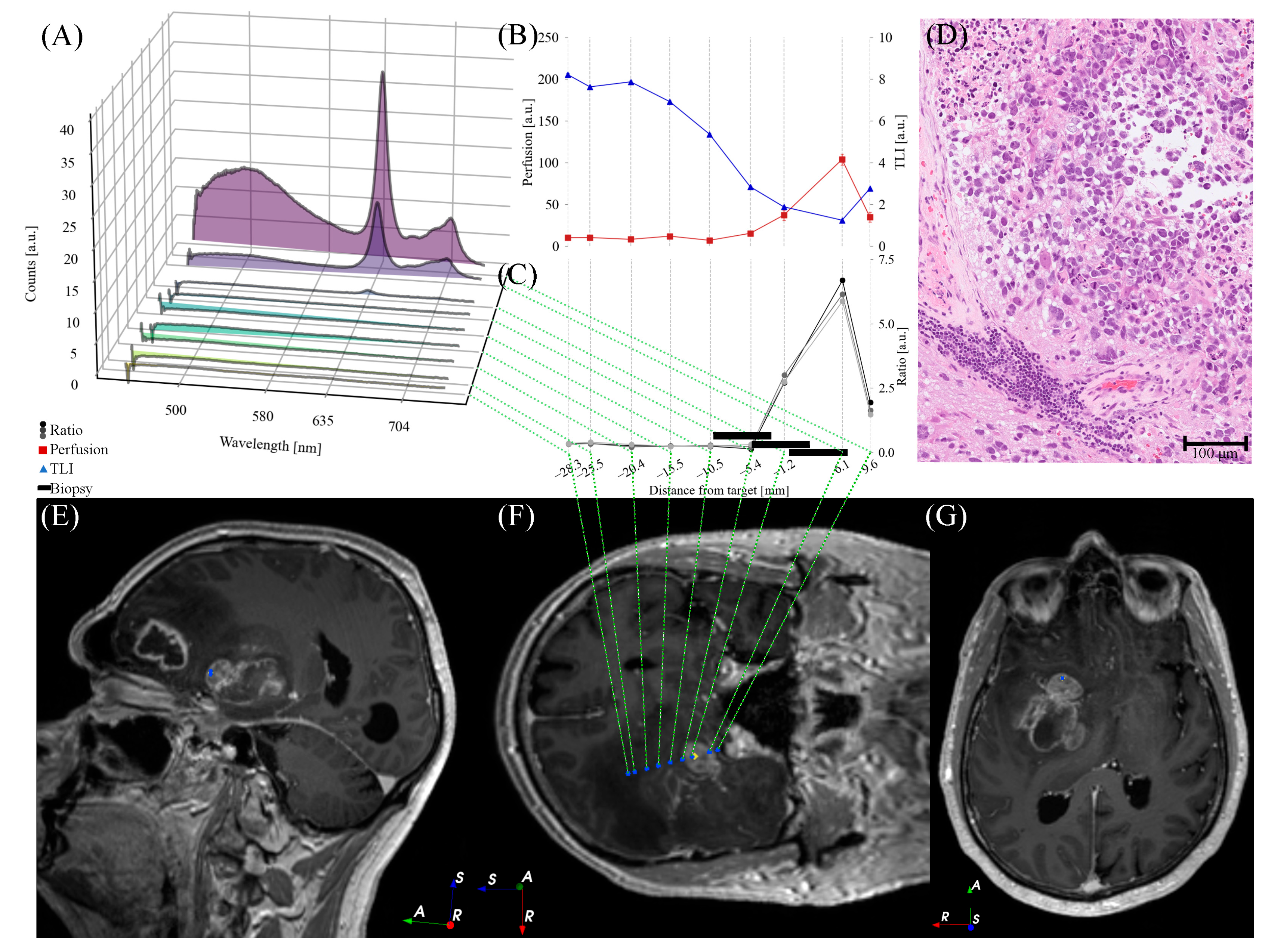
3.3. Patient Cases
4. Discussion
4.1. In Situ Optical Feedback on Tissue Characteristics
4.1.1. Indication of Tumor Tissue
4.1.2. Addressing the Risk of Hemorrhage
4.2. Navigation in Neurosurgery
4.3. Limitations and Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


Appendix B

References
- Azagury, D.E.; Dua, M.M.; Barrese, J.C.; Henderson, J.M.; Buchs, N.C.; Ris, F.; Cloyd, J.M.; Martinie, J.B.; Razzaque, S.; Nicolau, S.; et al. Image-Guided Surgery. Curr. Probl. Surg. 2015, 52, 476–520. [Google Scholar] [CrossRef] [PubMed]
- Miner, R.C. Image-Guided Neurosurgery. J. Med. Imaging Radiat. Sci. 2017, 48, 328–335. [Google Scholar] [CrossRef]
- Wang, M.N.; Song, Z.J. Classification and Analysis of the Errors in Neuronavigation. Neurosurgery 2011, 68, 1131–1143. [Google Scholar] [CrossRef] [PubMed]
- Kongkham, P.N.; Knifed, E.; Tamber, M.S.; Bernstein, M. Complications in 622 Cases of Frame-Based Stereotactic Biopsy, a Decreasing Procedure. Can. J. Neurol. Sci. 2008, 35, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Riche, M.; Amelot, A.; Peyre, M.; Capelle, L.; Carpentier, A.; Mathon, B. Complications after Frame-Based Stereotactic Brain Biopsy: A Systematic Review. Neurosurg. Rev. 2021, 44, 301–307. [Google Scholar] [CrossRef]
- Khatab, S.; Spliet, W.; Woerdeman, P.A. Frameless Image-Guided Stereotactic Brain Biopsies: Emphasis on Diagnostic Yield. Acta Neurochir. (Wien) 2014, 156, 1441–1450. [Google Scholar] [CrossRef]
- Livermore, L.J.; Ma, R.; Bojanic, S.; Pereira, E.A. Yield and Complications of Frame-Based and Frameless Stereotactic Brain Biopsy—The Value of Intra-Operative Histological Analysis. Br. J. NeuroSurg. 2014, 28, 637–644. [Google Scholar] [CrossRef]
- Acerbi, F.; Broggi, M.; Eoli, M.; Anghileri, E.; Cuppini, L.; Pollo, B.; Schiariti, M.; Visintini, S.; Orsi, C.; Franzini, A.; et al. Fluorescein-Guided Surgery for Grade Iv Gliomas with a Dedicated Filter on the Surgical Microscope: Preliminary Results in 12 Cases. Acta Neurochir. (Wien) 2013, 155, 1277–1286. [Google Scholar] [CrossRef]
- Hadjipanayis; Constantinos, G.; Stummer, W. 5-Ala and Fda Approval for Glioma Surgery. J. Neuro-Oncol. 2019, 141, 479–486. [Google Scholar] [CrossRef]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.-J. Fluorescence-Guided Surgery with 5-Aminolevulinic Acid for Resection of Malignant Glioma: A Randomised Controlled Multicentre Phase Iii Trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- von Campe, G.; Moschopulos, M.; Hefti, M. 5-Aminolevulinic Acid-Induced Protoporphyrin Ix Fluorescence as Immediate Intraoperative Indicator to Improve the Safety of Malignant or High-Grade Brain Tumor Diagnosis in Frameless Stereotactic Biopsies. Acta Neurochir. (Wien) 2012, 154, 585–588. [Google Scholar] [CrossRef]
- Millesi, M.; Kiesel, B.; Wöhrer, A.; Mercea, P.A.; Bissolo, M.; Roetzer, T.; Wolfsberger, S.; Furtner, J.; Knosp, E.; Widhalm, G. Is Intraoperative Pathology Needed If 5-Aminolevulinic-Acid-Induced Tissue Fluorescence Is Found in Stereotactic Brain Tumor Biopsy? Neurosurgery 2020, 86, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Del Maestro, M.; Fanti, A.; Airoldi, C.; Fleetwood, T.; Crobeddu, E.; Cossandi, C. Use of Fluorescein Sodium–Assisted Intraoperative Sample Validation to Maximize the Diagnostic Yield of Stereotactic Brain Biopsy: Progress toward a New Standard of Care? J. Neurosurg. 2023, 138, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Thien, A.; Han, J.X.; Kumar, K.; Ng, Y.P.; Rao, J.P.; Ng, W.H.; King, N.K.K. Investigation of the Usefulness of Fluorescein Sodium Fluorescence in Stereotactic Brain Biopsy. Acta Neurochir. (Wien) 2018, 160, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Haj-Hosseini, N.; Richter, J.C.O.; Milos, P.; Hallbeck, M.; Wårdell, K. 5-Ala Fluorescence and Laser Doppler Flowmetry for Guidance in a Stereotactic Brain Tumor Biopsy. BioMed. Opt. Express 2018, 9, 2284–2296. [Google Scholar] [CrossRef]
- Wårdell, K.; Zsigmond, P.; Richter, J.; Hemm, S. Relationship between Laser Doppler Signals and Anatomy During Deep Brain Stimulation Electrode Implantation toward the Ventral Intermediate Nucleus and Subthalamic Nucleus. Neurosurgery 2013, 72, ons127-40. [Google Scholar] [CrossRef]
- Zsigmond, P.; Hemm-Ode, S.; Wårdell, K. Optical Measurements During Deep Brain Stimulation Lead Implantation: Safety Aspects. Ster. Funct. NeuroSurg. 2017, 95, 392–399. [Google Scholar] [CrossRef]
- Richter, J.; Haj-Hosseini, N.; Milos, P.; Hallbeck, M.; Wårdell, K. Optical Brain Biopsy with a Fluorescence and Vessel Tracing Probe. Oper. NeuroSurg. (Hagerstown) 2021, 21, 217–224. [Google Scholar] [CrossRef]
- Wårdell, K.; Klint, E.; Milos, P.; Richter, J. One-Insertion Stereotactic Brain Biopsy Using in-Vivo Optical Guidance—A Case Study. Oper. NeuroSurg. (Hagerstown) 2023. [Google Scholar] [CrossRef]
- Georgiopoulos, M.; Ellul, J.; Chroni, E.; Constantoyannis, C. Efficacy, Safety, and Duration of a Frameless Fiducial-Less Brain Biopsy Versus Frame-Based Stereotactic Biopsy: A Prospective Randomized Study. J. Neurol. Surg. A Cent. Eur. NeuroSurg. 2018, 79, 31–38. [Google Scholar]
- Kesserwan, M.A.; Shakil, H.; Lannon, M.; McGinn, R.; Banfield, L.; Nath, S.; Alotaibi, M.; Kasper, E.; Sharma, S. Frame-Based Versus Frameless Stereotactic Brain Biopsies: A Systematic Review and Meta-Analysis. Surg. Neurol. Int. 2021, 12, 52. [Google Scholar] [CrossRef] [PubMed]
- Ungar, L.; Nachum, O.; Zibly, Z.; Wohl, A.; Harel, R.; Attia, M.; Spiegelmann, R.; Zaubermann, J.; Feldman, Z.; Knoller, N.; et al. Comparison of Frame-Based Versus Frameless Image-Guided Intracranial Stereotactic Brain Biopsy: A Retrospective Analysis of Safety and Efficacy. World NeuroSurg. 2022, 164, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, S.; He, Y.; Bartek, J.; Alattar, A.A.; Chen, C.C. Comparison of Frame-Based Versus Frameless Intracranial Stereotactic Biopsy: Systematic Review and Meta-Analysis. World Neurosurg. 2019, 127, 607–616.e4. [Google Scholar] [CrossRef]
- Vychopen, M.; Wach, J.; Borger, V.; Schneider, M.; Eichhorn, L.; Maciaczyk, J.; Bara, G.; Vatter, H.; Banat, M.; Hamed, M. Patient Safety Comparison of Frameless and Frame-Based Stereotactic Navigation for Brain Biopsy—A Single Center Cohort Study. Brain Sci. 2022, 12, 1178. [Google Scholar] [CrossRef]
- Dorward, N.L.; Paleologos, T.S.; Alberti, O.; Thomas, D.G.T. The Advantages of Frameless Stereotactic Biopsy over Frame-Based Biopsy. Br. J. Neurosurg. 2002, 16, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Sciortino, T.; Fernandes, B.; Nibali, M.C.; Gay, L.G.; Rossi, M.; Lopci, E.; Colombo, A.E.; Elefante, M.G.; Pessina, F.; Bello, L.; et al. Frameless Stereotactic Biopsy for Precision Neurosurgery: Diagnostic Value, Safety, and Accuracy. Acta Neurochir. 2019, 161, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Klint, E.; Mauritzon, S.; Ragnemalm, B.; Richter, J.; Wårdell, K. Fluora—A System for Combined Fluorescence and Microcirculation Measurements in Brain Tumor Surgery. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 1512–1515. [Google Scholar]
- Bendsoe, N.; Persson, L.; Johansson, A.; Axelsson, J.; Svensson, J.; Gräfe, S.; Trebst, T.; Andersson-Engels, S.; Svanberg, S.; Svanberg, K. Fluorescence Monitoring of a Topically Applied Liposomal Temoporfin Formulation and Photodynamic Therapy of Nonpigmented Skin Malignancies. J. Environ. Pathol. Toxicol. Oncol. 2007, 26, 117–126. [Google Scholar] [CrossRef]
- Manifold, R.; Anderson, C. Increased Cutaneous Oxygen Availability by Topical Application of Hydrogen Peroxide Cream Enhances the Photodynamic Reaction to Topical 5-Aminolevulinic Acid-Methyl Ester. Arch. Dermatol. Res. 2011, 303, 285–292. [Google Scholar] [CrossRef]
- Li, X.; Morgan, P.S.; Ashburner, J.; Smith, J.; Rorden, C. The First Step for Neuroimaging Data Analysis: Dicom to Nifti Conversion. J. Neurosci. Methods 2016, 264, 47–56. [Google Scholar] [CrossRef]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4itk: Improved N3 Bias Correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef] [PubMed]
- Gorgolewski, K.; Burns, C.; Madison, C.; Clark, D.; Halchenko, Y.; Waskom, M.; Ghosh, S. Nipype: A Flexible, Lightweight and Extensible Neuroimaging Data Processing Framework in Python. Front. Neuroinformatics 2011, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3d Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- WHO. Classification of Tumours Editorial Board. In Central Nervous System Tumours, 5th ed.; Who Classification of Tumours Series; International Agency for Research on Cancer: Lyon, France, 2021; Volume 6. [Google Scholar]
- Collaud, S.; Juzeniene, A.; Moan, J.; Lange, N. On the Selectivity of 5-Aminolevulinic Acid-Induced Protoporphyrin Ix Formation. Curr. Med. Chem Anticancer Agents 2004, 4, 301–316. [Google Scholar] [CrossRef]
- Hefti, M.; von Campe, G.; Moschopulos, M.; Siegner, A.; Looser, H.; Landolt, H. 5-Aminolevulinic Acid Induced Protoporphyrin Ix Fluorescence in High-Grade Glioma Surgery: A One-Year Experience at a Single Institutuion. Swiss Med. Wkly. 2008, 138, 180–185. [Google Scholar] [PubMed]
- Evers, G.; Kamp, M.; Warneke, N.; Berdel, W.; Sabel, M.; Stummer, W.; Ewelt, C. 5-Aminolaevulinic Acid-Induced Fluorescence in Primary Central Nervous System Lymphoma. World NeuroSurg. 2017, 98, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Kiesel, B.; Millesi, M.; Woehrer, A.; Furtner, J.; Bavand, A.; Roetzer, T.; Mischkulnig, M.; Wolfsberger, S.; Preusser, M.; Knosp, E.; et al. 5-Ala-Induced Fluorescence as a Marker for Diagnostic Tissue in Stereotactic Biopsies of Intracranial Lymphomas: Experience in 41 Patients. NeuroSurg. Focus 2018, 44, E7. [Google Scholar] [CrossRef]
- Cornelius, J.F.; Kamp, M.A.; Tortora, A.; Knipps, J.; Krause-Molle, Z.; Beez, T.; Petridis, A.K.; Sabel, M.; Schipper, J.; Steiger, H.J. Surgery of Small Anterior Skull Base Meningiomas by Endoscopic 5-Aminolevulinic Acid Fluorescence Guidance: First Clinical Experience. World NeuroSurg. 2019, 122, e890–e895. [Google Scholar] [CrossRef]
- Millesi, M.; Kiesel, B.; Mischkulnig, M.; Martínez-Moreno, M.; Wöhrer, A.; Wolfsberger, S.; Knosp, E.; Widhalm, G. Analysis of the Surgical Benefits of 5-Ala-Induced Fluorescence in Intracranial Meningiomas: Experience in 204 Meningiomas. J. NeuroSurg. 2016, 125, 1408–1419. [Google Scholar] [CrossRef]
- Valdes, P.A.; Millesi, M.; Widhalm, G.; Roberts, D.W. 5-Aminolevulinic Acid Induced Protoporphyrin Ix (Ala-Ppix) Fluorescence Guidance in Meningioma Surgery. J. Neuro-Oncol. 2019, 141, 555–565. [Google Scholar] [CrossRef]
- Eljamel, M.S. Fluorescence Image-Guided Surgery of Brain Tumors: Explained Step-by-Step. Photodiagnosis Photodyn 2008, 5, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Knipps, J.; Fischer, I.; Neumann, L.M.; Rapp, M.; Dibué-Adjei, M.; von Saß, C.F.; Placke, J.-M.; Mijderwijk, H.-J.; Steiger, H.-J.; Sabel, M.; et al. Quantification of Ppix-Fluorescence of Cerebral Metastases: A Pilot Study. Clin. Exp. Metastasis 2019, 36, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Giordano, M.; Gallieni, M.; Zaed, I.; Samii, A. Use of Frameless Stereotactic Navigation System Combined with Intraoperative Magnetic Resonance Imaging and 5-Aminolevulinic Acid. World Neurosurg. 2019, 131, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Shofty, B.; Richetta, C.; Haim, O.; Kashanian, A.; Gurevich, A.; Grossman, R. 5-Ala-Assisted Stereotactic Brain Tumor Biopsy Improve Diagnostic Yield. Eur J. Surg. Oncol 2019, 45, 2375–2378. [Google Scholar] [CrossRef] [PubMed]
- Desroches, J.; Lemoine, É.; Pinto, M.; Marple, E.; Urmey, K.; Diaz, R.; Guiot, M.C.; Wilson, B.C.; Petrecca, K.; Leblond, F. Development and First in-Human Use of a Raman Spectroscopy Guidance System Integrated with a Brain Biopsy Needle. J. Biophotonics 2019, 12, e201800396. [Google Scholar] [CrossRef]
- Anna, I.; Bartosz, P.; Lech, P.; Halina, A. Novel Strategies of Raman Imaging for Brain Tumor Research. Oncotarget 2017, 8, 85290–85310. [Google Scholar] [CrossRef]
- Livermore, L.J.; Isabelle, M.; Bell, I.M.; Scott, C.; Walsby-Tickle, J.; Gannon, J.; Plaha, P.; Vallance, C.; Ansorge, O. Rapid Intraoperative Molecular Genetic Classification of Gliomas Using Raman Spectroscopy. Neurooncol. Adv. 2019, 1, vdz008. [Google Scholar] [CrossRef]
- Wahl, J.; Klint, E.; Hallbeck, M.; Hillman, J.; Wårdell, K.; Ramser, K. Impact of Preprocessing Methods on the Raman Spectra of Brain Tissue. BioMed. Opt. Express 2022, 13, 6763–6777. [Google Scholar] [CrossRef]
- Richter, J.C.O.; Haj-Hosseini, N.; Hallbeck, M.; Wårdell, K. Combination of Hand-Held Probe and Microscopy for Fluorescence Guided Surgery in the Brain Tumor Marginal Zone. Photodiagnosis Photodyn 2017, 18, 185–192. [Google Scholar] [CrossRef]
- Wilson, B.; Kim, A.; Valdes, P.; Paulsen, K.; Roberts, D. Biopsy Device with Integrated Optical Spectroscopy Guidance. Patent EP2793706A4, 14 October 2015. [Google Scholar]
- Ramakonar, H.; Quirk, B.C.; Kirk, R.W.; Li, J.; Jacques, A.; Lind, C.R.P.; McLaughlin, R.A. Intraoperative Detection of Blood Vessels with an Imaging Needle During Neurosurgery in Humans. Sci. Adv. 2018, 4, eaav4992. [Google Scholar] [CrossRef]
- Skyrman, S.; Lai, M.; Edström, E.; Burström, G.; Förander, P.; Homan, R.; Kor, F.; Holthuizen, R.; Hendriks, B.H.W.; Persson, O.; et al. Augmented Reality Navigation for Cranial Biopsy and External Ventricular Drain Insertion. NeuroSurg. Focus 2021, 51, E7. [Google Scholar] [CrossRef] [PubMed]
- Widmann, G.; Schullian, P.; Ortler, M.; Bale, R. Frameless Stereotactic Targeting Devices: Technical Features, Targeting Errors and Clinical Results. Int. J. Med. Robot 2012, 8, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.W.; Valdés, P.A.; Harris, B.T.; Fontaine, K.M.; Hartov, A.; Fan, X.; Ji, S.; Lollis, S.S.; Pogue, B.W.; Leblond, F.; et al. Coregistered Fluorescence-Enhanced Tumor Resection of Malignant Glioma: Relationships between Δ-Aminolevulinic Acid-Induced Protoporphyrin Ix Fluorescence, Magnetic Resonance Imaging Enhancement, and Neuropathological Parameters. Clinical Article. J. NeuroSurg. 2011, 114, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Qian, Z.; Victor, S.; Gu, Y.; Giller, C.; Liu, H. Look-Ahead Distance of a Fiber Probe Used to Assist Neurosurgery: Phantom and Monte Carlo Study. Opt. Express 2003, 11, 1844–1855. [Google Scholar] [CrossRef]
- Johansson, J.; Fredriksson, I.; Wårdell, K.; Eriksson, O. Simulation of Reflected Light Intensity Changes During Navigation and Radio-Frequency Lesioning in the Brain. J. Biomed. Opt. 2009, 14, 044040. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | |||
|---|---|---|---|
| Parameter | 1 | 2 | 3 |
| Image Acquisition | |||
| Reference space | MR DICOM | CT | MR DICOM |
| Pixel spacing [mm] | 1 × 1 × 1 | 1 × 0.977 × 0.977 | 1 × 1 × 1 |
| Field of view [mm] | 192 × 256 × 256 | 176 × 256 × 256 | 176 × 256 × 256 |
| Acquisition time [min] | 21 | 21 | 21 |
| Postoperative image type | CT | CT | MR |
| Neuronavigation Errors | |||
| Registration [mm] | 1.9 | 1.5 | 1.6 |
| Targeting [mm] | 0.1 | 0.2 | 0.5 |
| Time | |||
| Optical measurement [min] | 7 | 7 | 9 |
| Intraop diagnosis [min] | 50 | 60 | 60 |
| Final Diagnosis | |||
| CNS WHO 2021 | High-grade astrocytoma, IDH-wildtype | Glioblastoma, IDH-wildtype, grade 4 | Primary diffuse large B-cell lymphoma of the CNS |
| Analysis (pre- vs. postop) | |||
| Euclidian distance [mm] | 3.1 ± 0.48 | 3.3 ± 1.2 | 1.3 ± 0.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klint, E.; Richter, J.; Wårdell, K. Combined Use of Frameless Neuronavigation and In Situ Optical Guidance in Brain Tumor Needle Biopsies. Brain Sci. 2023, 13, 809. https://doi.org/10.3390/brainsci13050809
Klint E, Richter J, Wårdell K. Combined Use of Frameless Neuronavigation and In Situ Optical Guidance in Brain Tumor Needle Biopsies. Brain Sciences. 2023; 13(5):809. https://doi.org/10.3390/brainsci13050809
Chicago/Turabian StyleKlint, Elisabeth, Johan Richter, and Karin Wårdell. 2023. "Combined Use of Frameless Neuronavigation and In Situ Optical Guidance in Brain Tumor Needle Biopsies" Brain Sciences 13, no. 5: 809. https://doi.org/10.3390/brainsci13050809