
β Oscillations of Dorsal STN as a Potential Biomarker in Parkinson’s Disease Motor Subtypes: An Exploratory Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
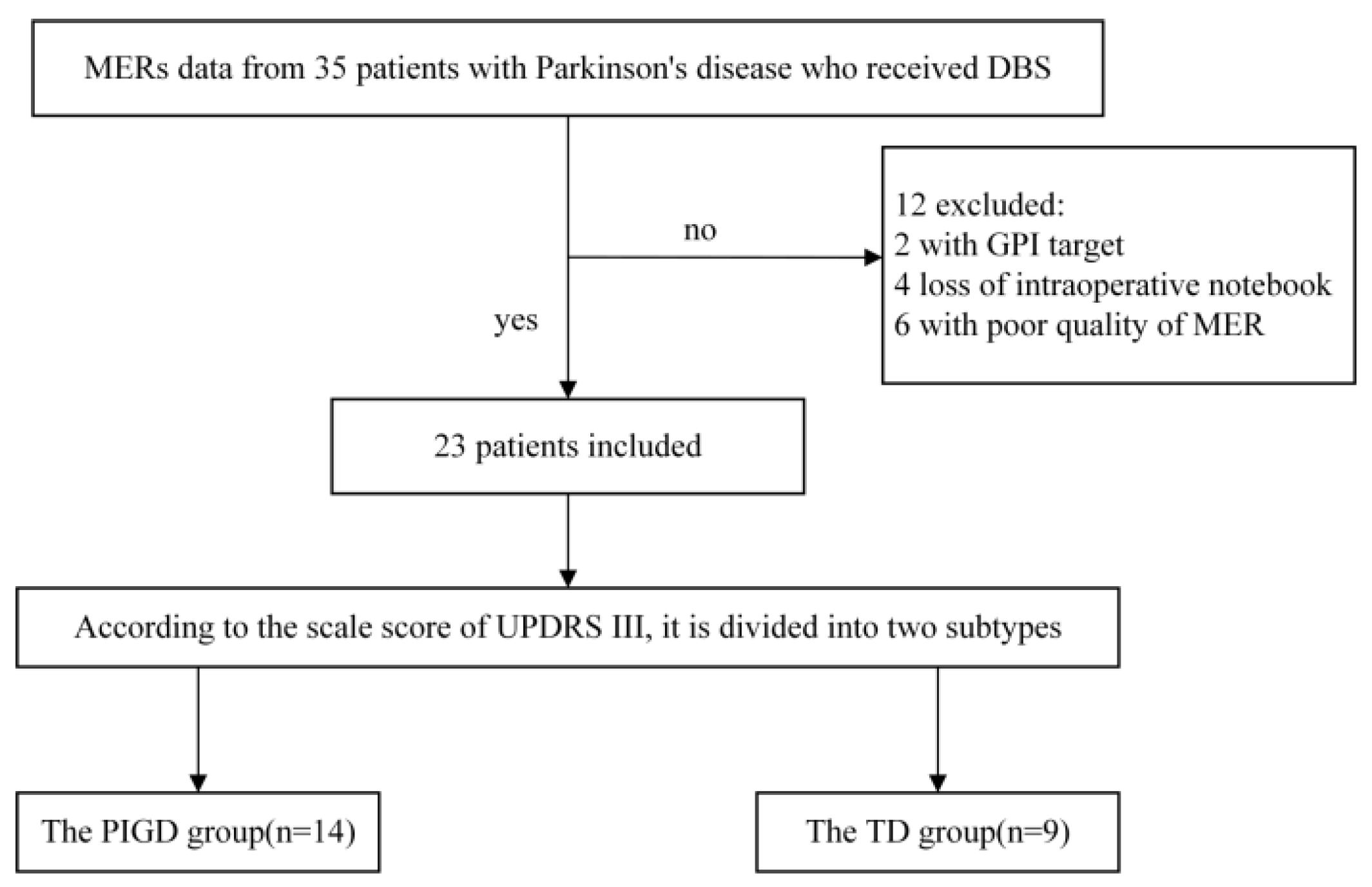
2.1. Patient Data
2.2. Clinical Information
2.3. Microelectrode Recording
2.4. Spike Extraction
2.5. Spike Power Spectrum Density Estimation
2.6. Background Activity
2.7. Coherence between Spike and Background Activity
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Comparisons of MBIs, FRs, and AIs
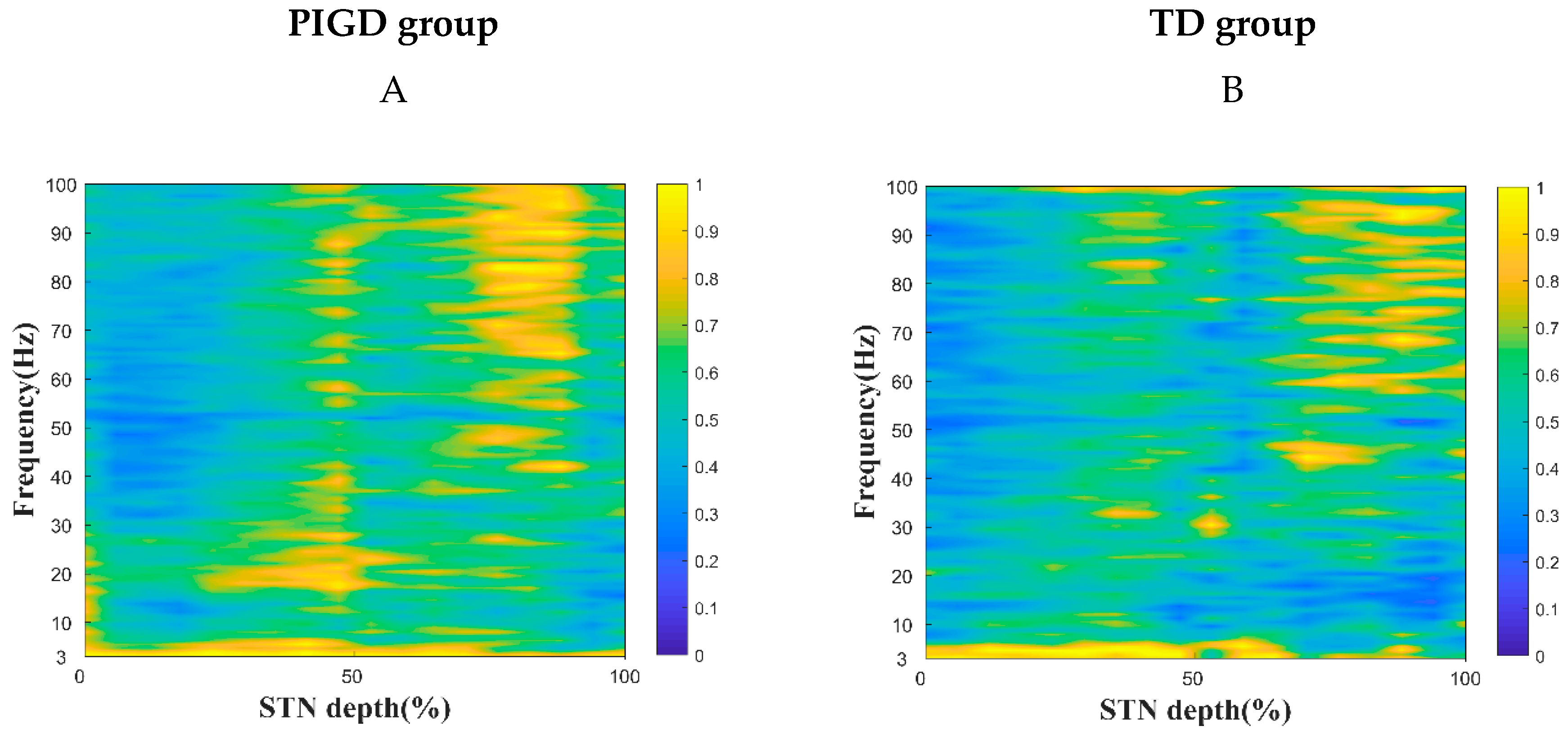
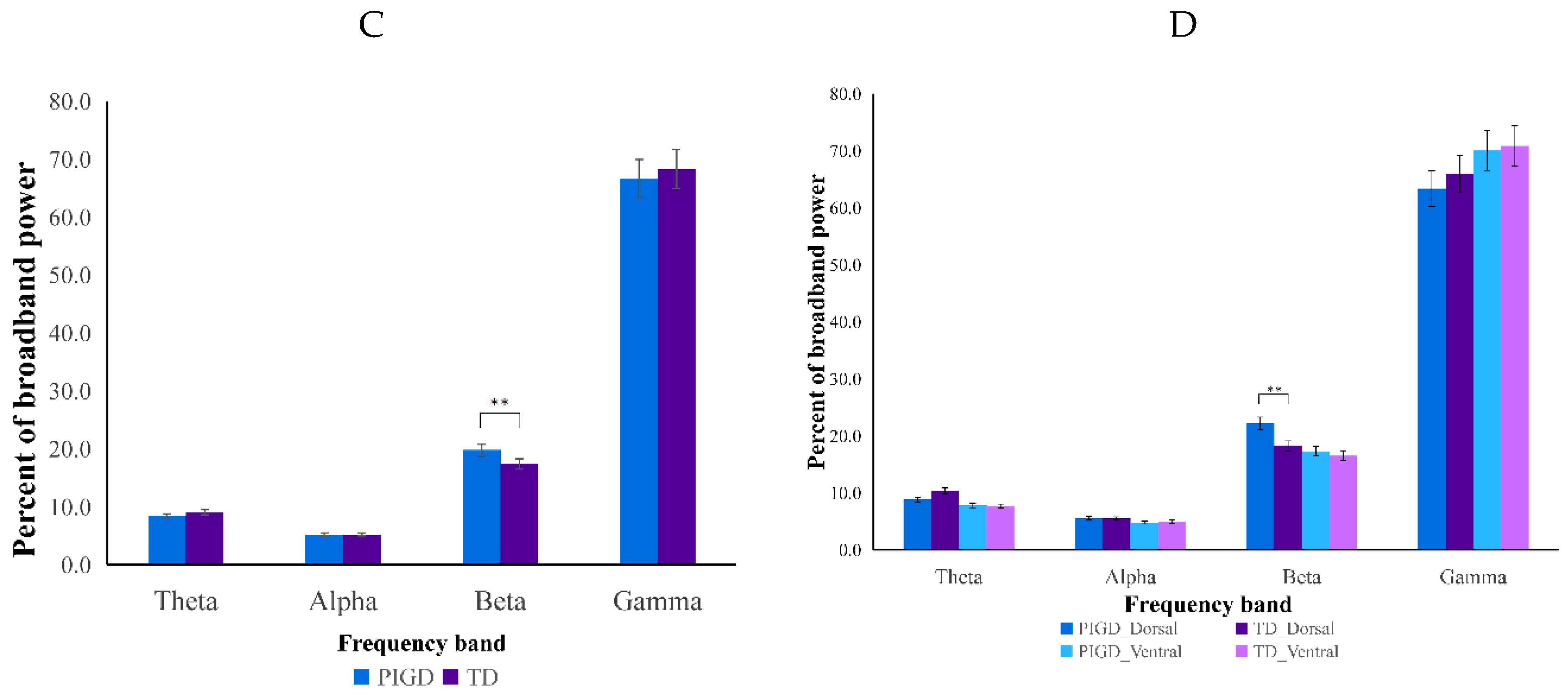
3.3. Spike PSD and Coherence
3.4. Distinction between PIGD and TD Subtypes Correlates with β Oscillations on the Dorsal Side of the STN
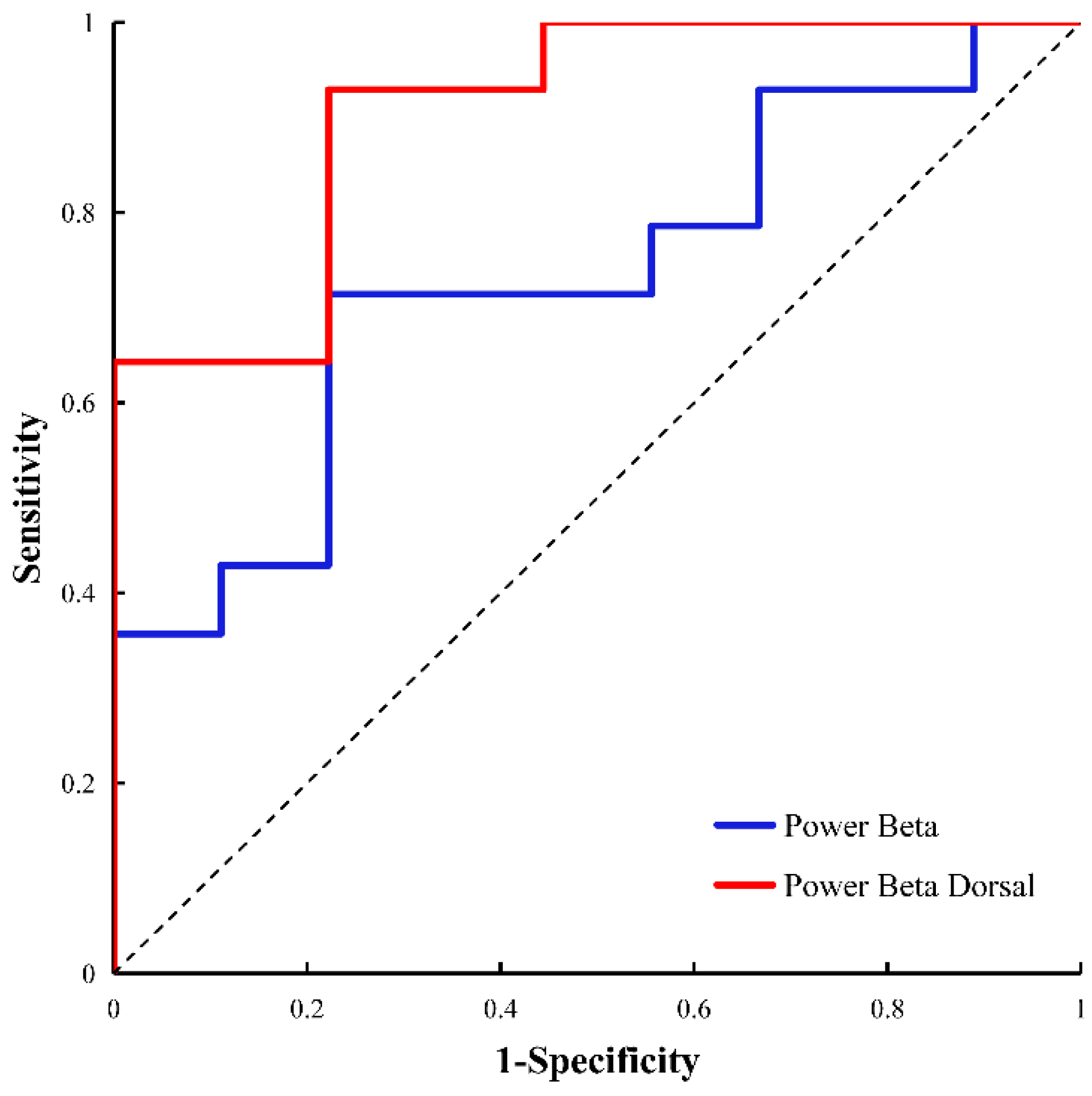
3.5. Identifying and Predicting PIGD and TD
4. Discussion
4.1. Dorsal β Oscillations in Relation to Two Subtypes of PIGD and TD
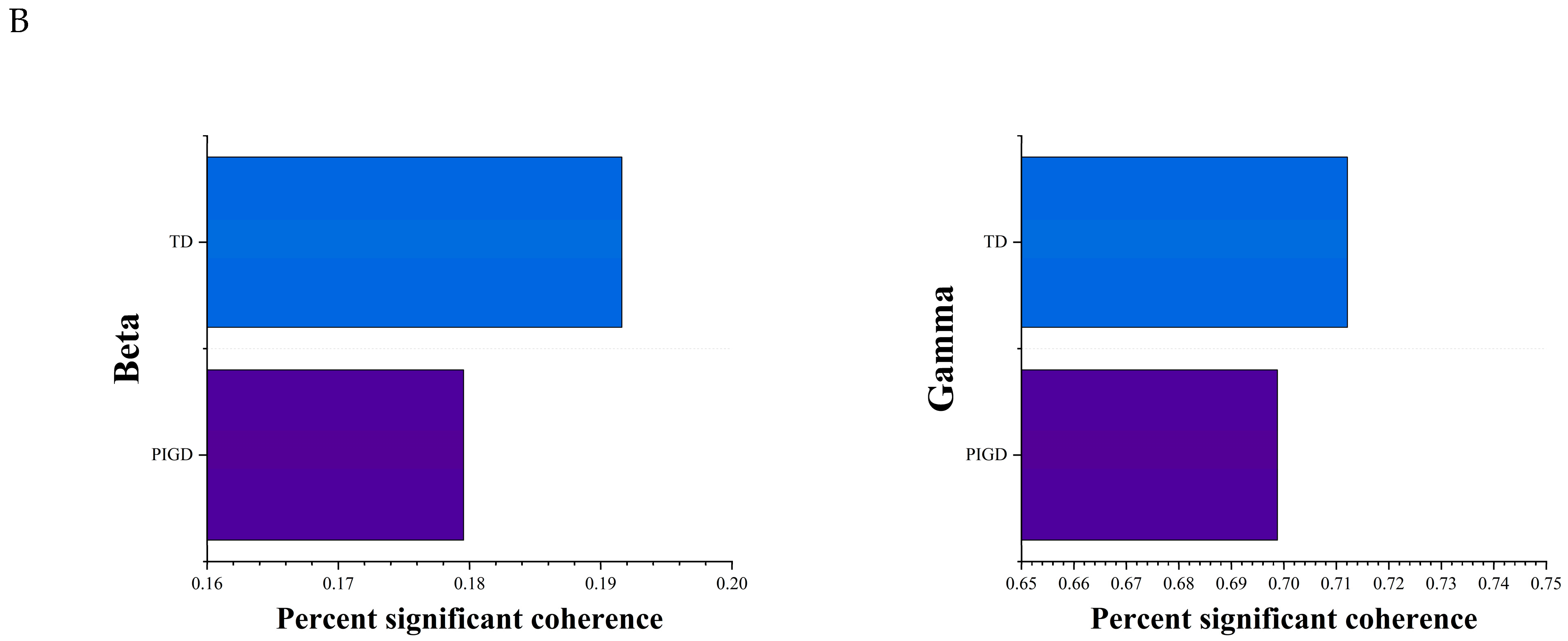
4.2. Coherence Analysis of the Two PIGD and TD Subtypes
4.3. Correlation of PSD and UPDRS Scores
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Breger, L.S.; Fuzzati Armentero, M.T. Genetically engineered animal models of Parkinson’s disease: From worm to rodent. Eur. J. Neurosci. 2019, 49, 533–560. [Google Scholar] [CrossRef]
- Jankovic, J.; Friedman, D.I.; Pirozzolo, F.J.; Mccrary, J.A. Progressive supranuclear palsy: Motor, neurobehavioral, and neuro-ophthalmic findings. Adv. Neurol. 1990, 53, 293. [Google Scholar]
- Stebbins, G.T.; Goetz, C.G.; Burn, D.J.; Jankovic, J.; Khoo, T.K.; Tilley, B.C. How to identify tremor dominant and postural instability/gait difficulty groups with the movement disorder society unified Parkinson’s disease rating scale: Comparison with the unified Parkinson’s disease Rating scale. Mov. Disord. 2013, 28, 668–670. [Google Scholar] [CrossRef] [PubMed]
- Alves, G.; Larsen, J.P.; Emre, M.; Wentzel-Larsen, T.; Aarsland, D. Changes in motor subtype and risk for incident dementia in Parkinson’s disease. Mov. Disord. 2010, 21, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; Kapadia, A.S. Functional Decline in Parkinson Disease. Arch. Neurol. 2001, 58, 1611. [Google Scholar] [CrossRef] [PubMed]
- Auyeung, M.; Tsoi, T.H.; Mok, V.; Cheung, C.M.; Lee, C.N.; Li, R.; Yeung, E. Ten year survival and outcomes in a prospective cohort of new onset Chinese Parkinson’s disease patients. J. Neurol. Neurosurg. Psychiatry 2012, 83, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Michmizos, K.P.; Nikita, K.S. Addition of deep brain stimulation signal to a local field potential driven Izhikevich model masks the pathological firing pattern of an STN neuron. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; Volume 2011, pp. 7290–7293. [Google Scholar]
- Kostoglou, K.; Michmizos, K.P.; Stathis, P.; Sakas, D.; Nikita, K.S.; Mitsis, G.D. Classification and Prediction of Clinical Improvement in Deep Brain Stimulation From Intraoperative Microelectrode Recordings. IEEE Trans. Bio-Med. Eng. 2017, 64, 1123–1130. [Google Scholar] [CrossRef]
- Baaske, M.K.; Kormann, E.; Holt, A.B.; Gulberti, A.; McNamara, C.G.; Pötter-Nerger, M.; Westphal, M.; Engel, A.K.; Hamel, W.; Brown, P.; et al. Parkinson’s disease uncovers an underlying sensitivity of subthalamic nucleus neurons to beta-frequency cortical input in vivo. Neurobiol. Dis. 2020, 146, 105119. [Google Scholar] [CrossRef]
- Woerd, E.S.; Oostenveld, R.; de Lange, F.P.; Praamstra, P. A shift from prospective to reactive modulation of beta-band oscillations in Parkinson’s disease-ScienceDirect. NeuroImage 2014, 100, 507–519. [Google Scholar] [CrossRef]
- Hammond, C.; Bergman, H.; Brown, P. Pathological synchronization in Parkinson’s disease: Networks, models and treatments. Trends Neurosci. 2007, 30, 357–364. [Google Scholar] [CrossRef]
- Bouthour, W.; Mégevand, P.; Donoghue, J.; Lüscher, C.; Birbaumer, N.; Krack, P. Biomarkers for closed-loop deep brain stimulation in Parkinson disease and beyond. Nat. Rev. Neurol. 2019, 15, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Neumann, W.J.; Staub-Bartelt, F.; Horn, A.; Schanda, J.; Schneider, G.H.; Brown, P.; Kühn, A.A. Long term correlation of subthalamic beta band activity with motor impairment in patients with Parkinson’s disease. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2017, 128, 2286–2291. [Google Scholar] [CrossRef]
- Neumann, W.J.; Degen, K.; Schneider, G.H.; Brücke, C.; Huebl, J.; Brown, P.; Kühn, A. Subthalamic synchronized oscillatory activity correlates with motor impairment in patients with Parkinson’s disease. Mov. Disord. 2016, 31, 1748–1751. [Google Scholar] [CrossRef]
- Oswal, A.; Beudel, M.; Zrinzo, L.; Limousin, P.; Brown, P. Deep brain stimulation modulates synchrony within spatially and spectrally distinct resting state networks in Parkinson’s disease. Brain 2016, 139, aww048. [Google Scholar] [CrossRef]
- Guo, S.; Zhuang, P.; Hallett, M.; Zheng, Z.; Zhang, Y.; Li, J.; Li, Y. Subthalamic deep brain stimulation for Parkinson’s disease: Correlation between locations of oscillatory activity and optimal site of stimulation. Park. Relat. Disord 2013, 19, 109–114. [Google Scholar] [CrossRef]
- Zaidel, A.; Spivak, A.; Grieb, B.; Bergman, H.; Israel, Z. Subthalamic span of beta oscillations predicts deep brain stimulation efficacy for patients with Parkinson’s disease. Brain 2010, 133, 2007–2021. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, Z.; Hu, K.; Mo, Y.; Cao, P.; Hou, X.; He, X.; Zhang, S.; Xue, S. α and θ oscillations in the subthalamic nucleus are potential biomarkers for Parkinson’s disease with depressive symptoms. Park. Relat. Disord. 2021, 90, 98–104. [Google Scholar] [CrossRef]
- Dolan, K.; Martens, H.C.; Schuurman, P.R.; Bour, L.J. Automatic noise-level detection for extra-cellular micro-electrode recordings. Med. Biol. Eng. Comput. 2009, 47, 791–800. [Google Scholar] [CrossRef]
- Lin, S.H.; Lai, H.Y.; Lo, Y.C.; Chou, C.; Chou, Y.T.; Yang, S.H.; Sun, I.; Chen, B.W.; Wang, C.F.; Liu, G.T.; et al. Decreased Power but Preserved Bursting Features of Subthalamic Neuronal Signals in Advanced Parkinson’s Patients under Controlled Desflurane Inhalation Anesthesia. Front. Neurosci. 2017, 11, 701. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Ling, Y.T.; Yang, C.; Liu, Y.; Xian, W.B.; Zhang, L.N.; Guo, Q.Q.; Jin, X.Y.; Wu, B.; Zhang, C.M.; et al. Optimized Propofol Anesthesia Increases Power of Subthalamic Neuronal Activity in Patients with Parkinson’s Disease Undergoing Deep Brain Stimulation. Neurol. Ther. 2021, 10, 785–802. [Google Scholar] [CrossRef]
- Tsai, S.T.; Chuang, W.Y.; Kuo, C.C.; Chao, P.C.; Chen, T.Y.; Hung, H.Y.; Chen, S.Y. Dorsolateral subthalamic neuronal activity enhanced by median nerve stimulation characterizes Parkinson’s disease during deep brain stimulation with general anesthesia. J. Neurosurg. 2015, 123, 1394–1400. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.M.; Zhuang, P.; Li, Y.J.; Zhang, Y.Q.; Li, J.Y.; Wang, Y.P.; Li, J.P. Asymmetry of Subthalamic Neuronal Firing Rate and Oscillatory Characteristics in Parkinson’s Disease. Neuropsychiatr. Dis. Treat. 2020, 16, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Chen, S.Y.; Chen, T.Y.; Pan, J.I.; Tsai, S.T. Desflurane and sevoflurane differentially affect activity of the subthalamic nucleus in Parkinson’s disease. Br. J. Anaesth. 2021, 126, 477–485. [Google Scholar] [CrossRef]
- Moran, A.; Bergman, H.; Israel, Z.; Bar-Gad, I. Subthalamic nucleus functional organization revealed by parkinsonian neuronal oscillations and synchrony. Brain 2008, 131, 3395–3409. [Google Scholar] [CrossRef] [PubMed]
- Bejjani, B.P.; Gervais, D.; Arnulf, I.; Papadopoulos, S.; Demeret, S.; Bonnet, A.M.; Cornu, P.; Damier, P.; Agid, Y. Axial parkinsonian symptoms can be improved: The role of levodopa and bilateral subthalamic stimulation. J. Neurol. Neurosurg. Psychiatry 2000, 68, 595–600. [Google Scholar] [CrossRef]
- Kempf, F.; Kühn, A.A.; Kupsch, A.; Brücke, C.; Weise, L.; Schneider, G.H.; Brown, P. Premovement activities in the subthalamic area of patients with Parkinson’s disease and their dependence on task. Eur. J. Neurosci. 2007, 25, 3137–3145. [Google Scholar] [CrossRef]
- Kühn, A.; David, W.; Andreas, K.; Patricia, L.; Marwan, H.; Gerd-Helge, S.; Kielan, Y.; Peter, B. Event-related beta desynchronization in human subthalamic nucleus correlates with motor performance. Brain 2004, 127, 735–746. [Google Scholar] [CrossRef]
- Trottenberg, T.; Kupsch, A.; Schneider, G.H.; Brown, P.; Kühn, A.A. Frequency-dependent distribution of local field potential activity within the subthalamic nucleus in Parkinson’s disease. Exp. Neurol. 2007, 205, 287–291. [Google Scholar] [CrossRef]
- Amtage, F.; Henschel, K.; Schelter, B.; Vesper, J.; Timmer, J.; Lücking, C.H.; Hellwig, B. High functional connectivity of tremor related subthalamic neurons in Parkinson’s disease. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2009, 120, 1755–1761. [Google Scholar] [CrossRef]
- Williams, D.; Tijssen, M.; Van Bruggen, G.; Bosch, A.; Insola, A.; Di Lazzaro, V.; Mazzone, P.; Oliviero, A.; Quartarone, A.; Speelman, H.; et al. Dopamine-dependent changes in the functional connectivity between basal ganglia and cerebral cortex in humans. Brain 2002, 125, 1558–1569. [Google Scholar] [CrossRef]
- Wang, D.D.; de Hemptinne, C.; Miocinovic, S.; Ostrem, J.L.; Galifianakis, N.B.; San Luciano, M.; Starr, P.A. Pallidal Deep-Brain Stimulation Disrupts Pallidal Beta Oscillations and Coherence with Primary Motor Cortex in Parkinson’s Disease. J. Neurosci. Off. J. Soc. Neurosci. 2018, 38, 4556–4568. [Google Scholar] [CrossRef] [PubMed]
- Telkes, I.; Viswanathan, A.; Jimenez-Shahed, J.; Abosch, A.; Ozturk, M.; Gupte, A.; Jankovic, J.; Ince, N.F. Local field potentials of subthalamic nucleus contain electrophysiological footprints of motor subtypes of Parkinson’s disease. Proc. Natl. Acad. Sci. USA 2018, 115, E8567–E8576. [Google Scholar] [CrossRef] [PubMed]
- López-Azcárate, J.; Tainta, M.; Rodríguez-Oroz, M.C.; Valencia, M.; González, R.; Guridi, J.; Iriarte, J.; Obeso, J.A.; Artieda, J.; Alegre, M. Coupling between beta and high-frequency activity in the human subthalamic nucleus may be a pathophysiological mechanism in Parkinson’s disease. J. Neurosci. Off. J. Soc. Neurosci. 2010, 30, 6667–6677. [Google Scholar] [CrossRef] [PubMed]
- Bologna, M.; Paparella, G.; Fasano, A.; Hallett, M.; Berardelli, A. Evolving concepts on bradykinesia. Brain 2020, 143, 727–750. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PIGD Group (n = 14) | TD Group (n = 9) | p Value | |
|---|---|---|---|
| Age (years), | 61.29 ± 4.93 | 61.56 ± 8.73 | 0.92 a |
| Age at onset of PD (years), | 52.36 ± 5.08 | 53.65 ± 10.49 | 0.73 a |
| Height (cm), | 160.14 ± 9.02 | 163.89 ± 10.92 | 0.56 a |
| Sex (male/female) | 5/9 | 5/4 | 0.34 b |
| Body mass index (kg/m−2) | 23.014 ± 4.76 | 23.978 ± 3.06 | 0.59 a |
| Duration of PD (years), | 8.91 ± 6.03 | 7.89 ± 3.89 | 0.65 a |
| Weight (kg), | 59.29 ± 13.47 | 64.00 ± 6.46 | 0.34 a |
| LEDD (mg), | 1003.43 ± 359.16 | 1002.78 ± 263.93 | 0.99 a |
| UPDRS III off, | 53.93 ± 10.916 | 49.00 ± 13.295 | 0.90 a |
| H&Y stage, | 3.32 ± 0.66 | 2.88 ± 0.54 | 0.12 a |
| Part III | Tremor | Rigidity | Bradykinesia | Axial | ||
|---|---|---|---|---|---|---|
| Med off | PIGD | 53.93 ± 10.91 | 3.36 ± 3.22 | 12.64 ± 4.60 | 20.50 ± 3.61 | 13.36 ± 3.71 |
| TD | 49.00 ± 13.29 | 7.56 ± 4.66 | 10.89 ± 4.51 | 18.33 ± 3.50 | 9.00 ± 3.70 | |
| Med on | PIGD | 24.57 ± 7.40 | 1.14 ± 1.91 | 4.71 ± 3.60 | 10.36 ± 3.97 | 5.86 ± 1.79 |
| TD | 24.11 ± 9.88 | 0.56 ± 0.72 | 6.89 ± 3.95 | 9.89 ± 6.15 | 4.56 ± 2.18 | |
| DBS on | PIGD | 21.07 ± 10.79 | 0.00 ± 0.00 | 3.86 ± 2.17 | 9.14 ± 4.40 | 5.07 ± 3.09 |
| TD | 18.56 ± 7.24 | 1.00 ± 1.58 | 2.67 ± 3.46 | 8.11 ± 2.36 | 3.22 ± 1.92 | |
| p value | Med off | 0.34 | 0.01 * | 0.37 | 0.17 | 0.01 * |
| Med on | 0.90 | 0.39 | 0.18 | 0.82 | 0.13 | |
| DBS on | 0.54 | 0.09 | 0.32 | 0.52 | 0.14 |
| MER Features | UPDRS III (Med-on) | |||||
|---|---|---|---|---|---|---|
| UPDRS III | Tremor | Rigidity | Bradykinesia | Axial Symptoms | Gait | |
| Power_Theta | −0.02/0.946 | −0.264/0.362 | −0.383/0.176 | 0.401/0.155 | 0.568/0.034 * | 0.203/0.487 |
| Power_Alpha | −0.123/0.674 | −0.081/0.782 | −0.229/0.43 | −0.029/0.922 | −0.272/0.348 | −0.051/0.864 |
| Power_Beta | 0.002/0.994 | −0.025/0.933 | 0.025/0.934 | −0.158/0.589 | −0.353/0.216 | −0.203/0.487 |
| Power_Gamma | 0.194/0.507 | −0.133/0.65 | 0.069/0.815 | 0.301/0.296 | 0.466/0.093 | 0.051/0.864 |
| Power_Dorsal_Theta | −0.172/0.557 | −0.225/0.44 | −0.225/0.439 | 0.118/0.688 | 0.552/0.041 * | 0.456/0.101 |
| Power_Dorsal_Alpha | −0.577/0.031 * | −0.447/0.109 | −0.523/0.055 | −0.301/0.296 | 0.025/0.933 | 0.152/0.604 |
| Power_Dorsal_Beta | −0.081/0.782 | 0.153/0.602 | −0.022/0.94 | −0.247/0.394 | −0.582/0.029 * | −0.506/0.065 |
| Power_Dorsal_Gamma | 0.194/0.507 | −0.133/0.65 | 0.105/0.722 | 0.234/0.421 | 0.502/0.067 | 0.051/0.864 |
| Power_Ventral_Theta | 0.115/0.697 | 0.02/0.947 | −0.352/0.217 | 0.486/0.078 | 0.254/0.382 | −0.101/0.73 |
| Power_Ventral_Alpha | 0.152/0.604 | 0.192/0.51 | −0.111/0.705 | 0.216/0.458 | −0.201/0.49 | −0.203/0.487 |
| Power_Ventral_Beta | 0.059/0.84 | −0.22/0.451 | 0.147/0.616 | −0.145/0.621 | −0.256/0.377 | −0.051/0.864 |
| Power_Ventral_Gamma | 0.119/0.685 | −0.027/0.927 | −0.116/0.693 | 0.303/0.292 | 0.192/0.51 | −0.017/0.837 |
| Firing rate | −0.163/0.578 | 0.076/0.795 | −0.082/0.779 | −0.12/0.682 | 0.238/0.413 | 0.238/0.358 |
| Asymmetry_Index | −0.256/0.378 | −0.168/0.566 | −0.087/0.768 | −0.301/0.296 | 0.274/0.343 | −0.341/0.263 |
| MBI | −0.269/0.353 | 0.36/0.206 | −0.232/0.426 | −0.105/0.722 | 0.1/0.735 | −0.051/0.864 |
| MER Features | UPDRS III (Med-on) | |||||
|---|---|---|---|---|---|---|
| UPDRS III | Tremor | Rigidity | Bradykinesia | Axial Symptoms | Gait | |
| Power_Theta | −0.083/0.831 | 0.484/0.186 | −0.05/0.898 | −0.276/0.472 | 0.604/0.085 | −0.26/0.5 |
| Power_Alpha | −0.133/0.732 | 0.335/0.378 | −0.05/0.898 | −0.351/0.354 | 0.604/0.085 | −0.173/0.656 |
| Power_Beta | −0.617/0.077 | −0.149/0.702 | −0.603/0.086 | −0.762/0.017 * | 0.477/0.194 | −0.007/0.974 |
| Power_Gamma | −0.567/0.112 | −0.261/0.498 | −0.527/0.145 | −0.644/0.061 | 0.621/0.074 | 0.346/0.361 |
| Power_Dorsal_Theta | −0.133/0.732 | 0.335/0.378 | −0.05/0.898 | −0.351/0.354 | 0.604/0.085 | −0.173/0.656 |
| Power_Dorsal_Alpha | −0.1/0.798 | 0.41/0.273 | −0.033/0.932 | −0.301/0.431 | 0.57/0.109 | −0.26/0.5 |
| Power_Dorsal_Beta | −0.717/0.03 * | −0.261/0.498 | −0.603/0.086 | −0.828/0.006 ** | 0.451/0.223 | 0.26/0.5 |
| Power_Dorsal_Gamma | −0.467/0.205 | −0.186/0.631 | −0.628/0.07 | −0.502/0.168 | 0.383/0.309 | 0.173/0.656 |
| Power_Ventral_Theta | 0.033/0.932 | 0.596/0.09 | −0.142/0.715 | −0.008/0.983 | 0.57/0.109 | −0.346/0.361 |
| Power_Ventral_Alpha | 0.2/0.606 | 0.634/0.067 | 0.176/0.651 | 0.033/0.932 | 0.613/0.079 | −0.173/0.656 |
| Power_Ventral_Beta | −0.183/0.637 | 0.298/0.436 | −0.109/0.781 | −0.544/0.13 | 0.145/0.71 | −0.346/0.361 |
| Power_Ventral_Gamma | −0.533/0.139 | −0.261/0.498 | −0.377/0.318 | −0.753/0.019 * | 0.417/0.264 | 0.173/0.656 |
| Firing rate | −0.517/0.154 | 0.41/0.273 | −0.444/0.232 | −0.536/0.137 | −0.383/0.309 | −0.433/0.244 |
| Asymmetry_Index | −0.217/0.576 | 0.037/0.924 | −0.251/0.515 | −0.368/0.33 | −0.358/0.345 | −0.693/0.039 * |
| MBI | 0.55/0.125 | 0.484/0.186 | 0.285/0.458 | 0.728/0.026 * | 0.06/0.879 | −0.26/0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Zeng, Y.; Lin, M.; Wang, Y.; Ye, Q.; Meng, F.; Cai, G.; Cai, G. β Oscillations of Dorsal STN as a Potential Biomarker in Parkinson’s Disease Motor Subtypes: An Exploratory Study. Brain Sci. 2023, 13, 737. https://doi.org/10.3390/brainsci13050737
Li Y, Zeng Y, Lin M, Wang Y, Ye Q, Meng F, Cai G, Cai G. β Oscillations of Dorsal STN as a Potential Biomarker in Parkinson’s Disease Motor Subtypes: An Exploratory Study. Brain Sciences. 2023; 13(5):737. https://doi.org/10.3390/brainsci13050737
Chicago/Turabian StyleLi, Yongjie, Yuqi Zeng, Mangui Lin, Yingqing Wang, Qinyong Ye, Fangang Meng, Guofa Cai, and Guoen Cai. 2023. "β Oscillations of Dorsal STN as a Potential Biomarker in Parkinson’s Disease Motor Subtypes: An Exploratory Study" Brain Sciences 13, no. 5: 737. https://doi.org/10.3390/brainsci13050737