
Can Post-Operative Posterior Reversible Encephalopathy Syndrome (PRES) Be Considered an Insidious Rare Surgical Complication?

 , , ,
, , ,
Abstract
:1. Introduction
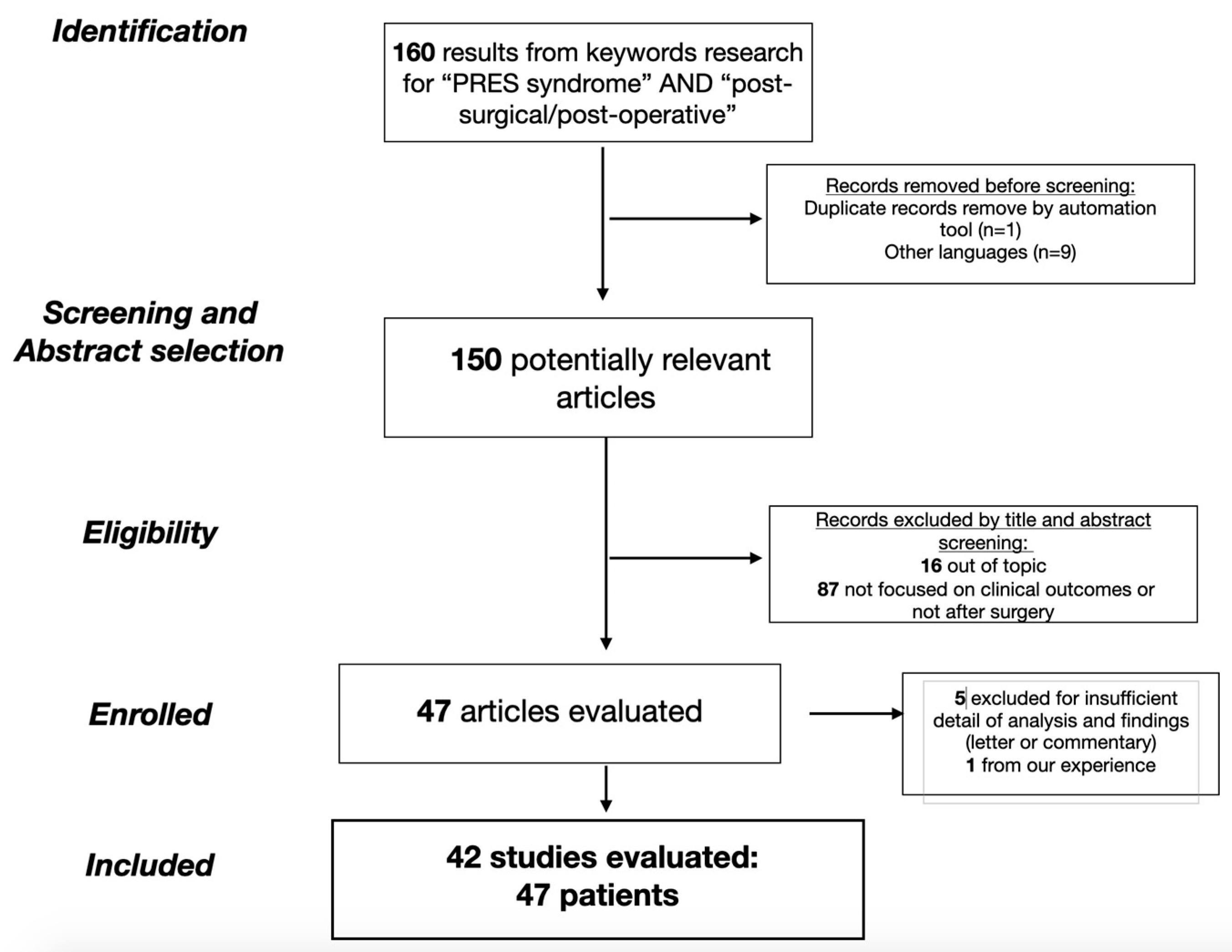
2. Materials and Methods
Eligibility Criteria
- Meta-analysis, case series, clinical study or clinical image reporting cases of patients who suffered from PRES syndrome after a surgical procedure.
- Cases reported without detailed clinical features of patients;
- Cases reported without description of radiological images;
- Papers that report other pathologies (off topic);
- Papers written in languages other than English.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hinchey, J.; Chaves, C.; Appignani, B.; Breen, J.; Pao, L.; Wang, A.; Pessin, M.S.; Lamy, C.; Mas, J.L.; Caplan, L.R. A reversible posterior leukoencephalopathy syndrome. N. Engl. J. Med. 1996, 334, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.F.; Chaudhari, R.; Wintermark, M. Imaging of Atypical and Complicated Posterior Reversible Encephalopathy Syndrome. Front. Neurol. 2019, 10, 964. [Google Scholar] [CrossRef] [PubMed]
- Bing, F.; M’biene, S.; Gay, S. Brainstem Posterior Reversible Encephalopathy Syndrome with Spinal Cord Involvement (PRES-SCI). Rev. Neurol. 2020, 176, 874–877. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.H.; Wijdicks, E.F.; Manno, E.M.; Rabinstein, A.A. Clinical Spectrum of Reversible Posterior Leukoencephalopathy Syndrome. Arch. Neurol. 2008, 65, 205–210. [Google Scholar] [CrossRef]
- Fugate, J.E.; Rabinstein, A.A. Posterior reversible encephalopathy syndrome: Clinical and radiological manifestations, pathophysiology, and outstanding questions. Lancet Neurol. 2015, 14, 914–925. [Google Scholar] [CrossRef]
- Brubaker, L.M.; Smith, J.K.; Lee, Y.Z.; Lin, W.; Castillo, M. Hemodynamic and Permeability Changes in Posterior Reversible Encephalopathy Syndrome Measured by Dynamic Susceptibility Perfusion-Weighted MR Imaging. Am. J. Neuroradiol. 2005, 26, 825–830. [Google Scholar]
- Liman, T.G.; Bohner, G.; Heuschmann, P.U.; Endres, M.; Siebert, E. The clinical and radiological spectrum of posterior reversible encephalopathy syndrome: The retrospective Berlin PRES study. J. Neurol. 2011, 259, 155–164. [Google Scholar] [CrossRef]
- Hinduja, A. Posterior Reversible Encephalopathy Syndrome: Clinical Features and Outcome. Front. Neurol. 2019, 11, 71. [Google Scholar] [CrossRef]
- Bartynski, W.S.; Boardman, J.F. Distinct Imaging Patterns and Lesion Distribution in Posterior Reversible Encephalopathy Syndrome. AJNR Am. J. Neuroradiol. 2007, 28, 1320–1327. [Google Scholar] [CrossRef]
- Kummer, S.; Schaper, J.; Mayatepek, E.; Tibussek, D. Posterior Reversible Encephalopathy Syndrome in Early Infancy. Klin. Padiatr. 2010, 222, 269–270. [Google Scholar] [CrossRef]
- Rykken, J.B.; McKinney, A.M. Posterior reversible encephalopathy syndrome. Semin. Ultrasound. CT MR 2014, 35, 118–135. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.K.; Yoon, J.U.; Park, S.-C.; Lee, H.J.; Kim, W.S.; Yoon, J.Y. Postoperative blindness associated with posterior reversible encephalopathy syndrome: A case report. J. Anesth. 2010, 24, 783–785. [Google Scholar] [CrossRef] [PubMed]
- Triquenot-Bagan, A.; Gerardin, E.; Guegan-Massardier, E.; Onnient, Y.; Leroy, F.; Mihout, B. Postoperative Reversible Posterior Leukoencephalopathy Syndrome. Cerebrovasc. Dis. 2003, 16, 430–432. [Google Scholar] [CrossRef]
- Zimering, J.H.; Mesfin, A. Posterior reversible encephalopathy syndrome following elevated mean arterial pressures for cervical spinal cord injury. J. Spinal. Cord. Med. 2016, 41, 111–114. [Google Scholar] [CrossRef]
- Moriarity, J.L., Jr.; Lim, M.; Storm, P.B.; Beauchamp, N.J., Jr.; Olivi, A. Reversible Posterior Leukoencephalopathy Occurring during Resection of a Posterior Fossa Tumor: Case Report and Review of the Literature. Neurosurgery 2001, 49, 1237–1240, discussion 1239–1240. [Google Scholar] [CrossRef]
- Horbinski, C.; Bartynski, W.S.; Carson-Walter, E.; Hamilton, R.L.; Tan, H.P.; Cheng, S. Reversible encephalopathy after cardiac transplantation: Histologic evidence of endothelial activation, T-cell specific trafficking, and vascular endothelial growth factor expression. Am. J. Neuroradiol. 2008, 30, 588–590. [Google Scholar] [CrossRef] [PubMed]
- Won, S.C.; Kwon, S.Y.; Han, J.W.; Choi, S.Y.; Lyu, C.J. Posterior Reversible Encephalopathy Syndrome in Childhood With Hematologic/Oncologic Diseases. Pediatr. Hematol. Oncol. 2009, 31, 505–508. [Google Scholar] [CrossRef]
- Patel, A.J.; Fox, B.D.; Fulkerson, D.H.; Yallampalli, S.; Illner, A.; Whitehead, W.E.; Curry, D.J.; Luerssen, T.G.; Jea, A. Posterior reversible encephalopathy syndrome during posterior fossa tumor resection in a child. J. Neurosurg. Pediatr. 2010, 6, 377–380. [Google Scholar] [CrossRef]
- Gopalakrishnan, C.V.; Vikas, V.; Nair, S. Posterior Reversible Encephalopathy Syndrome in a Case of Postoperative Spinal Extradural Haematoma: Case Report and Review of Literature. Asian Spine J. 2011, 5, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Cuadrado, I.; Lassaletta, L.; Royo, A.; Cerdeño, V.; Roda, J.M.; Gavilán, J. Reversible Posterior Leukoencephalopathy Syndrome after Lateral Skull Base Surgery. Otol. Neurotol. 2011, 32, 838–840. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.M.; Tannuri, A.C.; Gibelli, N.E.; Ayoub, A.A.; Maksoud-Filho, J.G.; Andrade, W.C.; Velhote, M.C.; Silva, M.M.; Pinho, M.L.; Miyatani, H.T.; et al. Posterior reversible encephalopathy syndrome after liver transplantation in children: A rare complication related to calcineurin inhibitor effects. Pediatr. Transplant. 2010, 15, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Sadek, A.R.; Waters, R.J.; Sparrow, O.C. Posterior reversible encephalopathy syndrome: A case following reversible cerebral vasoconstriction syndrome masquerading as subarachnoid haemorrhage. Acta Neurochir. 2012, 154, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Avecillas-Chasín, J.M.; Gómez, G.; Jorquera, M.; Alvarado, L.R.; Barcia, J.A. Delayed posterior reversible encephalopathy syndrome (PRES) after posterior fossa surgery. Acta Neurochir. 2013, 155, 1045–1047. [Google Scholar] [CrossRef] [PubMed]
- Hansberry, D.R.; Agarwal, N.; Tomei, K.L.; Goldstein, I.M. Posterior reversible encephalopathy syndrome in a patient with a Chiari I malformation. Surg. Neurol. Int. 2013, 4, 130. [Google Scholar] [CrossRef]
- Kuhnt, D.; Becker, A.; Benes, L.; Nimsky, C. Reversible Cortical Blindness and Internuclear Ophthalmoplegia after Neurosurgical Operation: Case Report and Review of the Literature. J. Neurol. Surg. Part A Central Eur. Neurosurg. 2013, 74, e128–e132. [Google Scholar] [CrossRef]
- Riaz, N.; Behnia, M.M.; Catalano, P.W.; Davis, J. A Patient with Moderate Post-Operative Hypertension Presenting with Posterior Reversible Encephalopathy Syndrome: A Case Report. Tanaffos 2013, 12, 58–61. [Google Scholar]
- Shah, R.; Kubisz-Pudelko, A.; Reid, J. Posterior reversible encephalopathy syndrome following an inadvertent dural puncture during an emergency laparotomy for ischemic colitis—A case report. Local Reg. Anesth. 2014, 7, 1–4. [Google Scholar] [CrossRef]
- González Quarante, L.H.; Mena-Bernal, J.H.; Martín, B.P.; Ramírez Carrasco, M.; Muñoz Casado, M.J.; Martínez de Aragón, A.; de las Heras, R.S. Posterior reversible encephalopathy syndrome (PRES): A rare condition after resection of posterior fossa tumors: Two new cases and review of the literature. Childs Nerv. Syst. 2016, 32, 857–863. [Google Scholar] [CrossRef]
- Sorour, M.; Sayama, C.; Couldwell, W.T. Posterior Reversible Encephalopathy Syndrome after Surgical Resection of a Giant Vestibular Schwannoma: Case Report and Literature Review. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2015, 77, 274–279. [Google Scholar] [CrossRef]
- Stanford, F.C.; Pratt, J.S.; Meireles, O.R.; Bredella, M.A. Posterior reversible encephalopathy syndrome (PRES) after bariatric surgery—A potential consequence associated with rapid withdrawal of antihypertensive medications. BMJ Case Rep. 2015, 2015, bcr2015212290. [Google Scholar] [CrossRef]
- Elkoundi, A.; Bensghir, M.; Meziane, M.; Haimeur, C. Perioperative visual loss following transurethral resection surgery: Not always a transurethral resection syndrome. Can. J. Anaesth. 2016, 63, 1295–1296. [Google Scholar] [CrossRef] [PubMed]
- Fok, A.; Chandra, R.; Gutman, M.; Ligtermoet, M.; Seneviratne, U.; Kempster, P. Posterior Reversible Encephalopathy Syndrome and Subarachnoid Hemorrhage after Lumboperitoneal Shunt for Fulminant Idiopathic Intracranial Hypertension. J. Neuroophthalmol. 2016, 36, 164–166. [Google Scholar] [CrossRef] [PubMed]
- Giussani, A.; Ardissino, G.; Belingheri, M.; Dilena, R.; Raiteri, M.; Pasciucco, A.; Colico, C.; Beretta, C. Posterior reversible encephalopathy syndrome after kidney transplantation in pediatric recipients: Two cases. Pediatr. Transplant. 2015, 20, 68–71. [Google Scholar] [CrossRef]
- Sato, N.; Machida, H.; Kodaka, M.; Nishiyama, K.; Komori, M. Perioperative posterior reversible encephalopathy syndrome in a patient with no history of hypertension: A case report. JA Clin. Rep. 2016, 2, 494. [Google Scholar] [CrossRef] [PubMed]
- Scarpino, M.; Olivo, G.; Quilghini, P.; Lanzo, G.; Moretti, M.; Carrai, R.; Fontanari, P.; Amantini, A.; Grippo, A. Cortical Blindness After Cardiac Surgery: Just an Ischemic Mechanism? J. Cardiothorac. Vasc. Anesth. 2016, 30, 1053–1056. [Google Scholar] [CrossRef]
- Wakasaki, T.; Gotoh, S.; Tomonobe, E.; Mihara, T.; Fukushima, J. Posterior Reversible Encephalopathy Syndrome during Combined Modality Therapy for Head and Neck Squamous Cell Carcinoma. Ann. Otol. Rhinol. Laryngol. 2016, 125, 844–849. [Google Scholar] [CrossRef]
- Vakharia, K.; Siasios, I.; Dimopoulos, V.G.; Pollina, J. Posterior Reversible Encephalopathy Syndrome Resolving Within 48 Hours in a Normotensive Patient Who Underwent Thoracic Spine Surgery. J. Clin. Med. Res. 2016, 8, 263–266. [Google Scholar] [CrossRef]
- Abusabha, Y.; Petridis, A.K.; Kraus, B.; Kamp, M.A.; Steiger, H.-J.; Beseoglu, K. Life-threatening posterior reversible encephalopathy syndrome in the cerebellum treated by posterior fossa decompression. Acta Neurochir. 2017, 159, 1325–1328. [Google Scholar] [CrossRef]
- Ban, S.P.; Hwang, G.; Kim, C.H.; Kwon, O.K. Reversible cerebral vasoconstriction syndrome combined with posterior reversible encephalopathy syndrome after heart transplantation. J. Clin. Neurosci. 2017, 42, 118–121. [Google Scholar] [CrossRef]
- Davi, C.B.; Moraes, B.P.; Lichtenfels, B.F.; Castro Filho, J.B.S.; Portal, M.M.; Montenegro, R.M.; Manfro, R.C. Posterior reversible leukoencephalopathy syndrome (PRES) after kidney transplantation: A case report. Braz. J. Nephrol. 2018, 40, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Durán, S.; Barrantes-Freer, A.; Rohde, V.; Von Der Brelie, C. Posterior reversible encephalopathy syndrome presenting in the anterior circulation with malignant intracranial hypertension requiring surgical decompression: A case report and literature review. Acta Neurochir. 2017, 159, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, T.F.; Sweis, R.T.; Nockels, R.P. Reversible postoperative blindness caused by bilateral status epilepticus amauroticus following thoracolumbar deformity correction: Case report. J. Neurosurg. Spine 2017, 27, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Magsi, S.; Zafar, A. Malignant Posterior Reversible Encephalopathy Syndrome—An Exacting Challenge for Neurocritical Care Physicians. Neurohospitalist 2017, 7, 196–199. [Google Scholar] [CrossRef]
- Villelli, N.W.; Prevedello, D.M.; Ikeda, D.S.; Montaser, A.S.; Otto, B.A.; Carrau, R.L. Posterior Reversible Encephalopathy Syndrome Causing Vision Loss Following Endoscopic Endonasal Resection of Pituitary Adenoma: A Case Report. World Neurosurg. 2017, 100, e1–e10. [Google Scholar] [CrossRef] [PubMed]
- Delgado-López, P.D.; Garcés-Pérez, G.; García-Carrasco, J.; Alonso-García, E.; Gómez-Menéndez, A.I.; Martín-Alonso, J. Posterior Reversible Encephalopathy Syndrome with Status Epilepticus Following Surgery for Lumbar Stenosis and Spondylolisthesis: Case report. World Neurosurg. 2018, 116, 309–315. [Google Scholar] [CrossRef]
- Khatri, D.; Bhaisora, K.S.; Parab, A.; Srivastava, A.K.; Das, K.K. Unusual Delayed Presentation of Posterior Reversible Encephalopathy Syndrome Following Vestibular Schwannoma Surgery: A Rare Neurologic Emergency. World Neurosurg. 2018, 120, 532–536. [Google Scholar] [CrossRef]
- Kerkeni, Y.; Louati, H.; Hamzaoui, M. Intestinal duplication revealed by posterior reversible encephalopathy syndrome. Korean J. Pediatr. 2018, 61, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Magray, M.A.; Mufti, G.N.; Bhat, N.A.; Baba, A.A.; Buch, M.H.; Hasan, F.U.; Banday, S.B. Posterior Reversible Encephalopathy Syndrome after Augmentation Cystoplasty in a Child with Neurogenic Bladder. J. Indian Assoc. Pediatr. Surg. 2018, 23, 158–160. [Google Scholar] [CrossRef]
- Oxford, B.G.; Khattar, N.K.; Adams, S.W.; Schaber, A.S.; Williams, B.J. Posterior reversible encephalopathy syndrome with lumbar drainage and surgery: Coincidence or correlation? A case report. BMC Neurol. 2019, 19, 214. [Google Scholar] [CrossRef]
- Liu, J.F.; Shen, T.; Zhang, Y.T. Posterior reversible encephalopathy syndrome and heart failure tacrolimus-induced after liver transplantation: A case report. World J. Clin. Cases 2020, 8, 2870–2875. [Google Scholar] [CrossRef]
- Rastogi, A.; Kaur, J.; Hyder, R.; Bhaskar, B.; Upadhyaya, V.; Rai, A.S. A case of post-operative posterior reversible encephalopathy syndrome in children: A preventable neurological catastrophe. Indian J. Anaesth. 2020, 64, 62–65. [Google Scholar] [CrossRef]
- Wong, M.; Rajendran, S.; Bindiganavile, S.H.; Bhat, N.; Lee, A.G.; Baskin, D.S. Posterior Reversible Encephalopathy Syndrome After Transsphenoidal Resection of Pituitary Macroadenoma. World Neurosurg. 2020, 142, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Fugate, J.E.; Claassen, D.O.; Cloft, H.J.; Kallmes, D.F.; Kozak, O.S.; Rabinstein, A.A. Posterior Reversible Encephalopathy Syndrome: Associated Clinical and Radiologic Findings. Mayo Clin. Proc. 2010, 85, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Granata, G.; Greco, A.; Iannella, G.; Granata, M.; Manno, A.; Savastano, E.; Magliulo, G. Posterior reversible encephalopathy syndrome—Insight into pathogenesis, clinical variants and treatment approaches. Autoimmun. Rev. 2015, 14, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Natsume, J.; Kidokoro, H.; Ishihara, N. Clinical and neuroimaging find- ings in children with posterior reversible encephalopathy syn-drome. Eur. J. Paediatr. Neurol. 2015, 19, 672–678. [Google Scholar] [CrossRef]
- Sharma, A.; Whitesell, R.T.; Moran, K.J. Imaging pattern of intracranial hemorrhage in the setting of posterior reversible encephalopathy syndrome. Neuroradiology 2009, 52, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Tetsuka, S.; Ogawa, T. Posterior reversible encephalopathy syndrome: A review with emphasis on neuroimaging characteristics. J. Neurol. Sci. 2019, 15, 72–79. [Google Scholar] [CrossRef]
- Strandgaard, S.; Olesen, J.; Skinhoj, E.; Lassen, N.A. Autoregulation of brain circulation in severe arterial hypertension. Br. Med. J. 1973, 1, 507–510. [Google Scholar] [CrossRef]
- Chen, Z.; Shen, G.Q.; Lerner, A.; Gao, B. Immune system activation in the pathogenesis of posterior reversible encephalopathy syndrome. Brain Res. Bull. 2017, 131, 93–99. [Google Scholar] [CrossRef]
- Lassen, N. A Regulation of cerebral circulation. Acta Anaesthesiol. Scand. Suppl. 1971, 45, 78–80. [Google Scholar] [CrossRef]
- Feske, S.K. Posterior reversible encephalopathy syndrome: A review. Semin. Neurol. 2011, 31, 202–215. [Google Scholar] [CrossRef]
- Bartynski, W.S. Posterior reversible encephalopathy syndrome, part 2: Controversies surrounding pathophysiology of vasogenic edema. AJNR Am. J. Neuroradiol. 2008, 29, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Gauiran, D.V.T.; Lladoc-Natividad, T.E.B.; Rocha, I.I.; Manapat-Reyes, B.H. Seizure and acute vision loss in a Fillipino lupus patient: A case of posterior reversible encephalopathy syndrome with intraparenchymal hemorrhage. Case Rep. Med. 2018, 2018, 4238676. [Google Scholar] [PubMed]
- Mayama, M.; Uno, K.; Tano, S.; Yoshihara, M.; Ukai, M.; Kishigami, Y.; Ito, Y.; Oguchi, H. Incidence of posterior reversible encephalopathy syndrome in eclamptic and patients with preeclampsia with neurologic symptoms. Am. J. Obstet. Gynecol. 2016, 215, 239.e1–239.e5. [Google Scholar] [CrossRef] [PubMed]
- Marra, A.; Vargas, M.; Striano, P.; Del Guercio, L.; Buonanno, P.; Servillo, G. Posterior reversible encephalopathy syndrome: The endothelial hypotheses. Med. Hypotheses 2014, 82, 619–622. [Google Scholar] [PubMed]
- Goldman, L.; Caldera, D.L.; Nussbaum, S.R.; Southwick, F.S.; Krogstad, D.; Murray, B.; Burke, D.S.; O’Malley, T.A.; Goroll, A.H.; Caplan, C.H.; et al. Multifactorial Index of Cardiac Risk in Noncardiac Surgical Procedures. N. Engl. J. Med. 1977, 297, 845–850. [Google Scholar]
- Yi, J.H.; Ha, S.H.; Kim, Y.K.; Choi, E.M. Posterior reversible encephalopathy syndrome in an untreated hypertensive patient after spinal surgery under general anesthesia—A case report. Korean J. Anesthesiol. 2011, 60, 369–372. [Google Scholar] [CrossRef]
- Zhang, Y.X.; Zheng, Y.; Zhang, B.J.; Zhang, Y.; Ding, M.P.; Zhang, B.R. Variant type of posterior reversible encephalopathy syndrome with diffuse cerebral white matter and brainstem involvement associated with intracranial hemorrhage. J. Stroke Cerebrovasc. Dis. 2016, 25, 233–235. [Google Scholar] [CrossRef]
- Yamagami, K.; Maeda, Y.; Iihara, K. Variant Type of Posterior Reversible Encephalopathy Syndrome Associated with Deep Brain Hemorrhage: Case Report and Review of the Literature. World Neurosurg. 2019, 134, 176–181. [Google Scholar]
- McKinney, A.M.; Short, J.; Truwit, C.L.; McKinney, Z.J.; Lozak, O.S.; SantaCruz, K.S.; Teksam, M. Posterior Reversible Encephalopathy Syndrome: Incidence of Atypical Regions of Involvement and Imaging Findings. Am. J. Roentgenol. 2007, 189, 904–912. [Google Scholar] [CrossRef]
- MacKenzie, E.T.; Strandgaard, S.; Graham, D.I.; Jones, J.V.; Harper, A.M.; Farrar, J.K. Effects of acutely induced hypertension in cats on pial arteriolar caliber, local cerebral blood flow, and the blood-brain barrier. Circ. Res. 1976, 39, 33–41. [Google Scholar] [CrossRef]
- Lamy, C.; Oppenheim, C.; Mas, J.L. Posterior reversible encephalopathy syndrome. Handb. Clin. Neurol. 2014, 121, 1687–1701. [Google Scholar] [PubMed]
- Karia, S.J.; Rykken, J.B.; McKinney, Z.J.; Zhang, L.; McKinney, A.M. Utility and significance of gadolinium-based contrast enhancement in posterior reversible encephalopathy syndrome. AJNR Am. J. Neuroradiol. 2016, 37, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Armocida, D.; Marzetti, F.; Pesce, A.; Caporlingua, A.; D’Angelo, L.; Santoro, A. Purely Meningeal Intracranial Relapse of Melanoma Brain Metastases After Surgical Resection and Immunotherapy as a Unique Disease Progression Pattern: Our Experience and Review of the Literature. World Neurosurg. 2019, 134, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Ou, S.; Xia, L.; Wang, L.; Xia, L.; Zhou, Q.; Pan, S. Posterior Reversible Encephalopathy Syndrome With Isolated Involving Infratentorial Structures. Front. Neurol. 2018, 9, 843. [Google Scholar] [CrossRef]
- Kastrup, O.; Gerwig, M.; Frings, M.; Diener, H.C. Posterior reversible encephalopathy syndrome (PRES): Electroencephalo- graphic findings and seizure patterns. J. Neurol. 2012, 259, 1383–1389. [Google Scholar] [CrossRef]
- Armocida, D.; Pesce, A.; Frati, A.; Miscusi, M.; Paglia, F.; Raco, A. Pneumoventricle of Unknown Origin: A Personal Experience and Literature Review of a Clinical Enigma. World Neurosurg. 2019, 122, 661–664. [Google Scholar] [CrossRef]
- Armocida, D.; Arcidiacono, U.A.; Palmieri, M.; Pesce, A.; Cofano, F.; Picotti, V.; Salvati, M.; D’andrea, G.; Garbossa, D.; Santoro, A.; et al. Intracranial Meningioma in Elderly Patients. Retrospective Multicentric Risk and Surgical Factors Study of Morbidity and Mortality. Diagnostics 2022, 12, 351. [Google Scholar] [CrossRef]
- Chardain, A.; Mesnage, V.; Alamowitch, S.; Bourdain, F. Posterior reversible encephalopathy syndrome (PRES) and hypomagnesemia: A frequent association? Rev. Neurol. 2016, 172, 384–388. [Google Scholar] [CrossRef]
- Gao, B.; Yu, B.X.; Li, R.S.; Zhang, G.; Xie, H.Z.; Liu, F.L.; Lv, C. Cytotoxic edema in posterior reversible encephalopathy syn- drome: Correlation of MRI features with serum albumin levels. AJNR Am. J. Neuroradiol. 2015, 36, 1884–1889. [Google Scholar] [CrossRef]
- Pirker, A.; Kramer, L.; Voller, B.; Loader, B.; Auff, E.; Prayer, D. Type of edema in posterior reversible encephalopathy syndrome depends on serum albumin levels: An MR imaging study in 28 patients. AJNR Am. J. Neuroradiol. 2011, 32, 527–531. [Google Scholar] [CrossRef] [PubMed]
- D’angelo, L.; Armocida, D.; Sampirisi, L.; Paglia, F.; Berra, L.V.; Santoro, A. Role of endoscopic surgical biopsy in diagnoses of intraventricular/periventricular tumors: Review of literature including a monocentric case series. Acta Neurol. Belg. 2020, 120, 517–530. [Google Scholar] [CrossRef]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C. 2014 evidence-based 005 guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [PubMed]
- Aranas, R.M.; Prabhakaran, S.; Lee, V.H. Posterior Reversible Encephalopathy Syndrome Associated with Hemorrhage. Neurocritical. Care 2009, 10, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Hiramatsu, H.; Sakai, N.; Namba, H. Cerebral Hemorrhage Due to Posterior Reversible Encephalopathy Syndrome Associated With Autonomic Dysreflexia in a Spinal Cord Injury Patient. Neurol. Medico-Chir. 2012, 52, 640–643. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. | Authors | Year | No. Pts. | Age | Sex | Comorbidity/Risk Factors | Pathology | Complications of Procedure | Time of Onset (Days) | Neurological Symptoms | Time of Symptoms Relapse (Days) | Outcome | Complications or Notes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Moriarity JL et al. [15] | 2001 | 1 | 19 | M | None | Posterior Fossa Tumor | Hypo-hypertension | 1 | Seizure | 56 | Good | / |
| 2 | Triquenot-Bagan et al. [13] | 2003 | 1 | 55 | M | Ischemic cardiopathy | Abdominal aortic aneurysm | No | 4 | Visual loss, headache | 13 | Good | Hypertension residual |
| 3 | Horbinski C. et al. [16] | 2009 | 1 | 57 | M | Hypertension | Cardiac transplant | No | 5 | Seizure | / | / | |
| 4 | Won SC et al. [17] | 2009 | 2 | 6 | F | None | Neuroblastoma | No | 1 | Seizure | 5 months | Good | |
| 5 | 11 | F | None | Osteosarcoma | No | 1 | Visual loss, seizure | 3 | Good | ||||
| 6 | Kim TK et al. [12] | 2010 | 1 | 44 | F | None | Uterin Mioma | Hypertension | 1 | Visual loss, headache | 1 | Good | |
| 7 | Patel AJ et al. [18] | 2010 | 1 | 6 | M | None | Pylocitic astrocytoma | Hypertension | 1 | Low cranial nerves injury | 14 | Good | / |
| 8 | Gopalakrishan et al. [19] | 2011 | 1 | 14 | F | None | Hemangioma dorsal | Hemorrhage | 1 | Seizure | 4 | Good | / |
| 9 | Sanchez-Cuadrado et al. [20] | 2011 | 1 | 58 | M | None | Head-neck tumor (ear) | No | 2 | Confusion, visual loss | 5 | Good | |
| 10 | Santos MM et al. [21] | 2011 | 2 | 9 | M | Biliar athresy | Liver transplant | No | 8 | Seizure, hemiparesis | 28 | Good | / |
| 11 | 13 | F | Alagylle’s syndrome | Liver transplant | No | 3 | Seizure, hypertension | 3 months | Good | / | |||
| 12 | Yi JH. et al. | 2011 | 1 | 71 | F | Cardiomegaly | Spinal lumbar stenosis L4-L5 | No | 1 | Seizure | 8 | Good | |
| 13 | Sadek A-R et al. [22] | 2012 | 1 | 51 | F | Hypertension | SAH aneurysm | No | 19 | Visual loss, hemiparesis | / | Worse | Coma |
| 14 | Avecillas-Chasin JM et al. [23] | 2013 | 1 | 19 | M | None | Posterior Fossa Tumor | No | 7 | Visual loss, seizure | 7 | Good | |
| 15 | Hansberry DR et al. [24] | 2013 | 1 | 25 | F | None | Chiari malformation | No | 6 | Hemiparesis, swallowing deficit | 2 | Stable | Hemiparesis |
| 16 | Kuhnt D. et al. [25] | 2013 | 1 | 63 | M | Hypertension | Intracranial Hemangiopericytoma | Hypotension-hypertension | 1 | Visual loss, ophthalmoplegia | 8 | Stable | Reduced visual acuity |
| 17 | Riaz N. et al. [26] | 2013 | 1 | 56 | M | Smoking | Lung cancer | Bronco-pleural fistula | 3 | Visual loss, confusion | 10 | Good | |
| 18 | Shah R. et al. [27] | 2014 | 1 | 62 | F | Hypertension, Celiac disease | Peritonitis, colitis | No | 3 | Visual loss, headache | 21 | Stable | Reduced visual acuity |
| 19 | González Quarante LH et al. [28] | 2015 | 2 | 4 | M | None | Medulloblastoma | No | 9 | Seizure | 1 month | Good | |
| 20 | 14 | M | None | Medulloblastoma | No | 2 | Seizure | 14 | Good | ||||
| 21 | Sorour M. et al. [29] | 2015 | 1 | 57 | F | Hypothyroidism | Vestibular schwannoma | No | 2 | Seizure | 13 | Good | |
| 22 | Stanford FC et al. [30] | 2015 | 1 | 61 | F | Carotid stenosis, hyperlipidemia, obesity | Bariatic surgery | No | 21 | Visual loss, hemiparesis | 1 month | Good | IRC |
| 23 | Elkoundi A. et al. [31] | 2016 | 1 | 67 | M | Hypertension, IPB | TURP | No | 1 | Blindness | 2 | Stable | Blind |
| 24 | Fok A. et al. [32] | 2016 | 1 | 33 | F | Hypertension | Idiopathic intracranial hypertension | No | Seizure, hemiparesis | 14 | Stable | Reduced visual acuity | |
| 25 | Giussani A. et al. [33] | 2016 | 2 | 7 | M | None | End-stage renal disease | No | 5 | Seizure | 1 month | Good | Tacrolimus therapy |
| 26 | 6 | M | None | End-stage renal disease | No | 10 | Seizure, confusion | 21 | Good | ||||
| 27 | Sato N et al. [34] | 2016 | 1 | 46 | F | None | Leiomioma uterin | No | 1 | Seizure | 49 | Good | / |
| 28 | Scarpino M et al. [35] | 2016 | 1 | 69 | / | Aortic stenosis | Aortic plasty | No | 1 | Confusion, visual loss | 1 month | Good | / |
| 29 | Wakasaki T et al. [36] | 2016 | 1 | 56 | F | Gastritis, stroke | Head-neck tumor | No | 4 | Visual loss, headache | 28 | Good | Epilepsy |
| 30 | Vakharia K. et al. [37] | 2016 | 1 | 60 | M | Renal cancer | Spinal renal metastases | No | 1 | Visual loss | 2 months | Good | |
| 31 | Abusabha Y. et al. [38] | 2017 | 1 | 52 | M | Hypertension | Posterior Fossa Tumor | No | 1 | Coma | 21 | Stable | |
| 32 | Ban SP et al. [39] | 2017 | 1 | 52 | M | Dilatative cardiomyopathy | Heart transplant | No | 8 | Seizure | 3 months | Good | / |
| 33 | Davi CB et. al. [40] | 2017 | 1 | 48 | F | Polycystic kidney | Kidney transplant | IRA | 10 | Lethargy, emianopsy | 2 | Good | / |
| 34 | Hernandez-Duran S. et al. [41] | 2017 | 1 | 44 | F | Hypertension, obesity, DM II | Idiopathic intracranial hypertension | No | 1 | Coma | 42 | Good | |
| 35 | Ibrahim TF et al. [42] | 2017 | 1 | 67 | M | Hypertension, kidney failure | Degenerative scoliosis | IRA | 6 | Visual loss | 2 | Good | / |
| 36 | Magsi et al. [43] | 2017 | 1 | 62 | F | Hyperlipidemia, colitis | Intraparenchymal spontaneous hemorrhage | No | 4 | Visual loss | 3 months | Good | / |
| 37 | Villelli NW et al. [44] | 2017 | 1 | 59 | F | None | Pituitary adenoma | No | 1 | Visual loss, Headache | 18 months | Stable | Residual visual deficit |
| 38 | Delgado-Lopez et al. [45] | 2018 | 1 | 82 | F | Hypertension | Spinal lumbar stenosis L4-L5 | No | 1 | Seizure | 12 | Stable | Residual hemiparesis |
| 39 | Khatri D. et al. [46] | 2018 | 1 | 23 | F | None | Vestibular schwannoma | No | 6 months | Seizure | 14 | Stable | Residual epilepsy |
| 40 | Kerkeni Y. et al. [47] | 2018 | 1 | 13 | F | Duplication uterine cyst | Surgical asportation | No | 7 | Seizure | 9 months | Good | |
| 41 | Magray MA et al. [48] | 2018 | 1 | 8 | M | Meningocele | Neurogenic bladder | No | 12 | Visual loss | 29 | Good | |
| 42 | Zimering J. et al. [14] | 2018 | 1 | 68 | F | DM II, AR | C5-C6 subluxation | No | Seizure | 14 | Good | ||
| 43 | Oxford BG et al. [49] | 2019 | 1 | 69 | M | Hypertension, hyperlipidemia | Rathke Cistis | No | 2 | Visual loss | 6 months | Good | Hypertension residual |
| 44 | Liu J-F et al. [50] | 2020 | 1 | 40 | F | Hepatitis | Hepatic transplant | No | 10 months | Seizure | 7 | Good | |
| 45 | Rastogi A et al. [51] | 2020 | 1 | 12 | M | Thalassemia | Splenectomy | No | 2 | Visual loss, Headache | 7 | Good | / |
| 46 | Wong M. et al. [52] | 2020 | 1 | 51 | F | None | Intracranial suprasellar mass | No | 4 | Visual loss | 7 | Good | |
| 47 | Our cases | 2020 | 1 | 55 | F | Hypertension | Intraparenchymal spontaneous hemorrhage | No | 21 | Seizure | 42 | Stable | Hydrocephalus 4 weeks after surgery |
| No. Patients | 47 | |
| Age | Mean: 40.9 | Min: 4 Max: 82 |
| Sex | F: 25 M: 21 | |
| Comorbidity and risk factors | Cardiopathy: 14 pts—29.78% | |
| No risk factors or comorbidity: 16 pts—34% | ||
| Surgical Procedure | Cranial surgery: 21 pts | 44.68% |
| Organ transplant: 8 pts | 17% | |
| Orthopedic-spine surgery: 6 pts | 12.77% | |
| Abdominal/general surgery: 4 pts | 8.51% | |
| Gynecology: 3 pts | 6.4% | |
| Vascular: 2 pts | 4.26% | |
| Urology: 2 pts | 4.26% | |
| Thoracic surgery: 1 pt | 2.13% | |
| Eventual complications of procedure | None: 39 pts | |
| Blood pressure instability: 4 pts | ||
| IRA: 2 pts | ||
| Bronco-pleural fistula: 1 pt | ||
| Hemorrhage: 1 pt | ||
| Time of onset of PRES | Mean: 4.1 days | Min: 1 day Max: 10 months |
| Neurological Symptoms | Visual loss/reduced acuity: 19 pts | |
| Seizure: 21 pts | ||
| Hemiparesis: 5 pts | ||
| Dizziness/confusion: 5 pts | ||
| Cranial nerves injury: 2 pts | ||
| Coma: 2 pts | ||
| Eventual time of symptoms relapse | Mean: 45.2 days | Min: 1 day Max: 18 months |
| Prognosis | Good: 35 pts (74.5%) | |
| Stable: 10 pts (21.3%) | ||
| Worst: 1 pt (0.02%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frati, A.; Armocida, D.; Tartara, F.; Cofano, F.; Corvino, S.; Paolini, S.; Santoro, A.; Garbossa, D. Can Post-Operative Posterior Reversible Encephalopathy Syndrome (PRES) Be Considered an Insidious Rare Surgical Complication? Brain Sci. 2023, 13, 706. https://doi.org/10.3390/brainsci13050706
Frati A, Armocida D, Tartara F, Cofano F, Corvino S, Paolini S, Santoro A, Garbossa D. Can Post-Operative Posterior Reversible Encephalopathy Syndrome (PRES) Be Considered an Insidious Rare Surgical Complication? Brain Sciences. 2023; 13(5):706. https://doi.org/10.3390/brainsci13050706
Chicago/Turabian StyleFrati, Alessandro, Daniele Armocida, Fulvio Tartara, Fabio Cofano, Sergio Corvino, Sergio Paolini, Antonio Santoro, and Diego Garbossa. 2023. "Can Post-Operative Posterior Reversible Encephalopathy Syndrome (PRES) Be Considered an Insidious Rare Surgical Complication?" Brain Sciences 13, no. 5: 706. https://doi.org/10.3390/brainsci13050706