
Is Specific Learning Disorder Predicted by Developmental Language Disorder? Evidence from a Follow-Up Study on Italian Children

Abstract
:1. Introduction
1.1. Epidemiology, Biological, and Environmental Risk Factors
1.2. Proximal and Distal Predictors of SLD and DLD
2. Materials and Methods
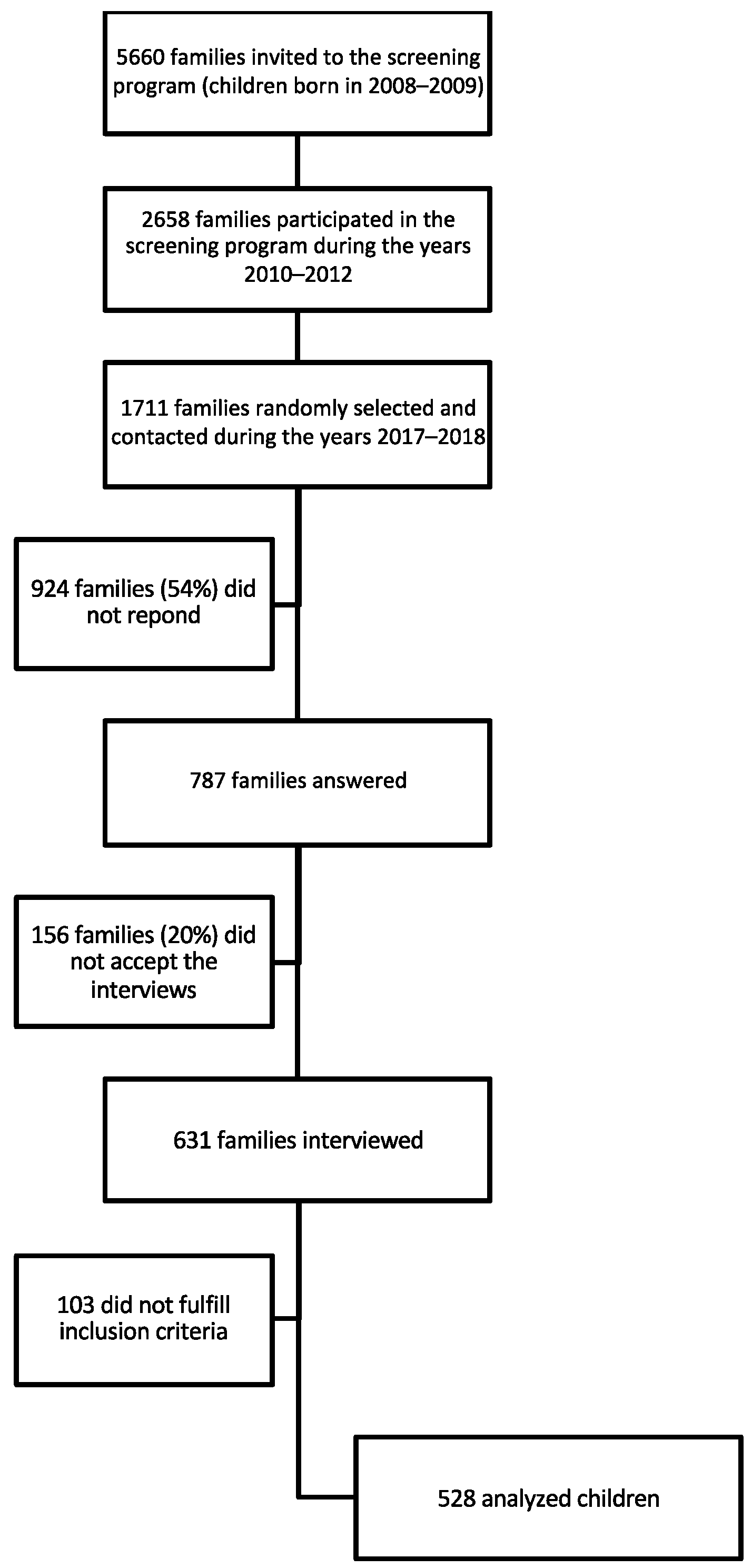
2.1. Participants and Procedure
2.2. Instruments
2.2.1. MB-CDI Italian Words and Sentences Short Form
2.2.2. Parental Interview on Language and Academic Outcome
2.3. Coding and Measures
Statistical Analysis
3. Results
4. Discussion
5. Limitations of the Current Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question Number | Question | Answer |
|---|---|---|
| Section 1 | ||
| Introduction | As you may recall, when your child was about three years old you participated in a screening program by the Mantua Local Health Authority to check whether your child’s communication and language development was adequate for his or her age. On that occasion, you were asked to fill in a questionnaire where you had to indicate how many words he said and whether he produced sentences. Do you remember? With this interview, we want to find out how your child’s language has developed since that point. The information you give us, as it is sensitive information, will not be disseminated outside the research and will be kept anonymous. The interview will take about 5 min. | |
| 1 | After completing the questionnaire, were you contacted by a pediatrician and/or local health services about a language delay in your child? |
|
| 2 | Did your child have a follow-up within a few months after that contact at the local health services (LHS) or at a specialized clinical center? |
|
| 3 | Did the follow-up visit confirm the outcome of the screening, i.e., the result of the questionnaire? |
|
| 4 | Did the follow-up visit reveal any developmental difficulties other than language difficulty? |
|
| 5 | What kind of difficulties? | text |
| 6 | Has the child, as a consequence of the difficulties that were noted, undergone therapy? |
|
| 7 | Who has been following the child’s development? |
|
| 8 | For how long? | text |
| Section 2 | ||
| 9 | Around the age of 4–5, did you notice any language difficulties in the child? |
|
| 10 | What kind of difficulties? | text |
| 11 | Have other developmental and/or behavioral difficulties arisen? |
|
| 12 | What kind of difficulties? | text |
| 13 | Was a clinical evaluation carried out after the difficulties emerged? |
|
| 14 | Who performed this evaluation? |
|
| 15 | What diagnosis was given in the clinician’s report? | text |
| 16 | Has the child, as a result of the difficulties that arose, followed or continued to follow therapy? |
|
| 17 | Who oversaw that therapy? |
|
| 18 | For how long? | text |
| Section 3 | ||
| 19 | Did any difficulties in reading and/or in writing emerge in the first two years of primary school that caused concern to teachers? |
|
| 20 | What difficulties caused concern? | text |
| 21 | Have other difficulties (e.g., in other subjects, behavior, attention) been reported? |
|
| 22 | What kind of difficulties? | text |
| 23 | Was a clinical evaluation carried out after the difficulties emerged? |
|
| 24 | Who performed the evaluation? |
|
| 25 | What diagnosis was given in the clinician’s report? | text |
| 26 | Has the child, as a result of the difficulties that arose, followed or continued to follow therapy? |
|
| 27 | Who followed and assessed the child’s progress? |
|
| 28 | For how long? | text |
| Ending | If you want to tell us any comments or considerations you have regarding the child’s developmental supervision and success or lack of it, you are welcome. Thank you. | text |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2022. [Google Scholar] [CrossRef]
- National Joint Committee on Learning Disabilities—Definition of Learning Disabilities. Available online: https://njcld.files.wordpress.com/2018/10/ld-definition.pdf (accessed on 2 April 2021).
- Sistema Nazionale Linee Guida dell’Istituto Superiore di Sanità (SNLG-ISS), Linea Guida sulla Gestione dei Disturbi Specifici dell’Apprendimento. Available online: https://snlg.iss.it/wp-content/uploads/2022/03/LG-389-AIP_DSA.pdf (accessed on 20 January 2022).
- Wagner, R.K.; Zirps, F.A.; Edwards, A.A.; Wood, S.G.; Joyner, R.E.; Becker, B.J.; Liu, G.; Beal, B. The prevalence of dyslexia: A new approach to its estimation. J. Learn. Disabil. 2020, 53, 354–365. [Google Scholar] [CrossRef]
- Yang, L.; Li, C.; Li, X.; Zhai, M.; An, Q.; Zhang, Y.; Zhao, J.; Weng, X. Prevalence of Developmental Dyslexia in Primary School Children: A Systematic Review and Meta-Analysis. Brain Sci. 2022, 12, 240. [Google Scholar] [CrossRef]
- Katusic, S.K.; Colligan, R.C.; Barbaresi, W.J.; Schaid, D.J.; Jacobsen, S.J. Incidence of reading disability in a population-based birth cohort, 1976–1982, Rochester, Minn. Mayo Clin. Proc. 2001, 76, 1081–1092. [Google Scholar] [CrossRef]
- Lin, Y.; Zhang, X.; Huang, Q.; Lv, L.; Huang, A.; Li, A.; Wu, K.; Huang, Y. The prevalence of dyslexia in primary school children and their Chinese literacy assessment in Shantou, China. Int. J. Environ. Res. Public Health 2020, 17, 7140. [Google Scholar] [CrossRef]
- Peters, L.; Ansari, D. Are specific learning disorders truly specific, and are they disorders? Trends Neurosci. Educ. 2019, 17, 100115. [Google Scholar] [CrossRef] [PubMed]
- Barbiero, C.; Montico, M.; Lonciari, I.; Monasta, L.; Penge, R.; Vio, C.; Tressoldi, P.E.; Carrozzi, M.; De Petris, A.; De Cagno, A.G.; et al. The lost children: The underdiagnosis of dyslexia in Italy. A cross-sectional national study. PLoS ONE 2019, 14, e0210448. [Google Scholar] [CrossRef] [PubMed]
- Plomin, R.; Kovas, Y. Generalist genes and learning disabilities. Psychol. Bull. 2005, 131, 592–617. [Google Scholar] [CrossRef] [PubMed]
- DeFries, J.C.; Fulker, D.W.; LaBuda, M.C. Evidence for a genetic etiology in reading disability of twins. Nature 1987, 329, 537–539. [Google Scholar] [CrossRef]
- Georgitsi, M.; Dermitzakis, I.; Soumelidou, E.; Bonti, E. The polygenic nature and complex genetic architecture of specific learning disorder. Brain Sci. 2021, 11, 631. [Google Scholar] [CrossRef] [PubMed]
- Arnett, A.B.; Pennington, B.F.; Peterson, R.L.; Willcutt, E.G.; DeFries, J.C.; Olson, R.K. Explaining the sex difference in dyslexia. J. Child Psychol. Psychiatry 2017, 58, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Chilosi, A.M.; Brovedani, P.; Cipriani, P.; Casalini, C. Sex differences in early language delay and in developmental language disorder. J. Neurosci. Res. 2023, 101, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, P.; Pasqualetti, P.; Volterra, V.; Caselli, M.C. Gender differences in early stages of language development. Some evidence and possible explanations. J. Neurosci. Res. 2023, 101, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, J.; Hoffmann, P.; Schmäl, C.; Schulte-Körne, G.; Nöthen, M.M. Genetics of dyslexia: The evolving landscape. J. Med. Genet. 2007, 44, 289–297. [Google Scholar] [CrossRef]
- Snowling, M.J.; Muter, V.; Carroll, J. Children at family risk of dyslexia: A follow-up in early adolescence. J. Child Psychol. Psychiatry 2007, 48, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Mascheretti, S.; Andreola, C.; Scaini, S.; Sulpizio, S. Beyond genes: A systematic review of environmental risk factors in specific reading disorder. Res. Dev. Disabil. 2018, 82, 147–152. [Google Scholar] [CrossRef]
- Rescorla, L. Age 17 Language and Reading Outcomes in Late-Talking Toddlers: Support for a Dimensional Perspective on Language Delay. J. Speech Lang. Hear. Res. 2009, 52, 16–30. [Google Scholar] [CrossRef]
- Snowling, M.J.; Nash, H.M.; Gooch, D.C.; Hayiou-Thomas, M.E.; Hulme, C. Wellcome Language & Reading Project Team. Developmental outcomes for children at high risk of dyslexia and children with developmental language disorder. Child Dev. 2019, 90, e548–e564. [Google Scholar] [CrossRef] [PubMed]
- Rescorla, L. Language and reading outcomes to age 9 in late-talking toddlers. J. Speech Lang. Hear. Res. 2002, 45, 360–371. [Google Scholar] [CrossRef]
- Brizzolara, D.; Casalini, C.; Gasperini, F.; Roncoli, S.; Mazzotti, S.; Cipriani, P.; Chilosi, A.M. A follow-up study of reading and writing in Italian children with Specific Language Impairment. In Language: Normal and Pathological Development; Riva, D., Rapin, I., Zardini, G., Eds.; John Libbey Eurotext: Montrouge, France, 2006; pp. 239–252. [Google Scholar]
- Chilosi, A.M.; Brizzolara, D.; Lami, L.; Pizzoli, C.; Gasperini, F.; Pecini, C.; Cipriani, P.; Zoccolotti, P. Reading and spelling disabilities in children with and without a history of early language delay: A neuropsychological and linguistic study. Child Neuropsychol. 2009, 15, 582–604. [Google Scholar] [CrossRef]
- McArthur, G.M.; Hogben, J.H.; Edwards, V.T.; Heath, S.M.; Mengler, E.D. On the “specifics” of specific reading disability and specific language impairment. J. Child Psychol. Psychiatry 2000, 41, 869–874. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; Snowling, M.J.; Thompson, P.A.; Greenhalgh, T.; CATALISE-2 Consortium. Phase 2 of CATALISE: A multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology. J. Child Psychol. Psychiatry 2017, 58, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Snowling, M.J.; Moll, K.; Hulme, C. Language difficulties are a shared risk factor for both reading disorder and mathematics disorder. J. Exp. Child Psychol. 2021, 202, 105009. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; Snowling, M.J. Developmental dyslexia and specific language impairment: Same or different? Psychol. Bull. 2004, 130, 858–886. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; McDonald, D.; Bird, S.; Hayiou-Thomas, M. Children who read words accurately despite language impairment: Who are they and how do they do it? Child Dev. 2009, 80, 593–605. [Google Scholar] [CrossRef]
- Fraser, J.; Goswami, U.; Conti-Ramsden, G. Dyslexia and Specific Language Impairment: The Role of Phonology and Auditory Processing. Sci. Stud. Read. 2010, 14, 8–29. [Google Scholar] [CrossRef]
- Catts, H.W.; Adlof, S.M.; Hogan, T.P.; Weismer, S.E. Are specific language impairment and dyslexia distinct disorders? J. Speech Lang. Hear. Res. 2005, 48, 1378–1396. [Google Scholar] [CrossRef] [PubMed]
- Adlof, S.M.; Scoggins, J.; Brazendale, A.; Babb, S.; Petscher, Y. Identifying children at risk for language impairment or dyslexia with group-administered measures. J. Speech Lang. Hear. Res. 2017, 60, 3507–3522. [Google Scholar] [CrossRef] [PubMed]
- Ramus, F.; Marshall, C.R.; Rosen, S.; van der Lely, H.K. Phonological deficits in specific language impairment and developmental dyslexia: Towards a multidimensional model. Brain 2013, 136, 630–645. [Google Scholar] [CrossRef]
- Snowling, M.J.; Duff, F.J.; Nash, H.M.; Hulme, C. Language profiles and literacy outcomes of children with resolving, emerging, or persisting language impairments. J. Child Psychol. Psychiatry 2016, 57, 1360–1369. [Google Scholar] [CrossRef] [PubMed]
- Snowling, M.J.; Hulme, C. Annual Research Review: Reading disorders revisited—The critical importance of oral language. J. Child Psychol. Psychiatry 2021, 62, 635–653. [Google Scholar] [CrossRef]
- van Viersen, S.; de Bree, E.H.; Verdam, M.; Krikhaar, E.; Maassen, B.; van der Leij, A.; de Jong, P.F. Delayed early vocabulary development in children at family risk of dyslexia. J. Speech Lang. Hear. Res. 2017, 60, 937–949. [Google Scholar] [CrossRef] [PubMed]
- Maassen, B.A.M.; Krikhaar, E.; van der Leij, A.; Fikkert, P. Early productive vocabulary composition as precursor of dyslexia. J. Speech Lang. Hear. Res. 2022, 65, 760–774. [Google Scholar] [CrossRef]
- Torppa, M.; Lyytinen, P.; Erskine, J.; Eklund, K.; Lyytinen, H. Language development, literacy skills, and predictive connections to reading in Finnish children with and without familial risk for dyslexia. J. Learn. Disabil. 2010, 43, 308–321. [Google Scholar] [CrossRef]
- Lyytinen, P.; Eklund, K.; Lyytinen, H. Language development and literacy skills in late talking toddlers with and without FR for dyslexia. Ann. Dyslexia 2005, 55, 166–192. [Google Scholar] [CrossRef] [PubMed]
- Psyridou, M.; Eklund, K.; Poikkeus, A.M.; Torppa, M. Reading outcomes of children with delayed early vocabulary: A follow-up from age 2–16. Res. Dev. Disabil. 2018, 78, 114–124. [Google Scholar] [CrossRef]
- Desmarais, C.; Sylvestre, A.; Meyer, F.; Bairati, I.; Rouleau, N. Three profiles of language abilities in toddlers with an expressive vocabulary delay: Variations on a theme. J. Speech Lang. Hear. Res. 2010, 53, 699–709. [Google Scholar] [CrossRef]
- Hsu, H.C.; Iyer, S.N. Early gesture, early vocabulary, and risk of language impairment in preschoolers. Res. Dev. Disabil. 2016, 57, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.L. A systematic review and meta-analysis of predictors of expressive-language outcomes among late talkers. J. Speech Lang. Hear. Res. 2017, 60, 853–864. [Google Scholar] [CrossRef]
- Chilosi, A.M.; Pfanner, L.; Pecini, C.; Salvadorini, R.; Casalini, C.; Brizzolara, D.; Cipriani, P. Which linguistic measures distinguish transient from persistent language problems in Late Talkers from 2 to 4 years? A study on Italian speaking children. Res. Dev. Disabil. 2019, 89, 59–68. [Google Scholar] [CrossRef]
- Bello, A.; Onofrio, D.; Caselli, M.C. Prediction and persistence of late talking: A study of Italian toddlers at 29 and 34 months. Res. Dev. Disabil. 2018, 75, 40–48. [Google Scholar] [CrossRef]
- Ellis, E.M.; Thal, D.J. Early language delay and risk for language impairment. Perspect. Lang. Learn. Educ. 2008, 15, 93–100. [Google Scholar] [CrossRef]
- Thal, D.J.; Marchman, V.A.; Tomblin, J.B. Late-Talking toddlers: Characterization and prediction of continued delay. In Late Talkers. Language, Development, Interventions and Outcomes; Rescorla, L.A., Dale, P.S., Eds.; Paul Brookes Publishing: Baltimore, MA, USA, 2013; pp. 91–112. [Google Scholar]
- Zambrana, I.C.; Ystrom, E.; Schlberg, S.; Pons, F. Action imitation at 11/2 years is better than pointing gesture in predicting late development of language production at 3 years of age. Child Dev. 2013, 84, 560–573. [Google Scholar] [CrossRef] [PubMed]
- Sansavini, A.; Favilla, M.E.; Guasti, M.T.; Marini, A.; Millepiedi, S.; Di Martino, M.V.; Vecchi, S.; Battajon, N.; Bertolo, L.; Capirci, O.; et al. Developmental Language Disorder: Early Predictors, Age for the Diagnosis, and Diagnostic Tools. A Scoping Review. Brain Sci. 2021, 11, 654. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, P.; Bello, A.; Lasorsa, F.R.; Caselli, M.C. Do Spoken Vocabulary and Gestural Production Distinguish Children with Transient Language Delay from Children Who Will Show Developmental Language Disorder? A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 3822. [Google Scholar] [CrossRef] [PubMed]
- Bigozzi, L.; Tarchi, C.; Pezzica, S.; Pinto, G. Evaluating the Predictive Impact of an Emergent Literacy Model on Dyslexia in Italian Children: A Four-Year Prospective Cohort Study. J. Learn. Disabil. 2016, 49, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Moll, K.; Thompson, P.A.; Mikulajova, M.; Jagercikova, Z.; Kucharska, A.; Franke, H.; Hulme, C.; Snowling, M.J. Precursors of reading difficulties in Czech and Slovak children at-risk of dyslexia. Dyslexia 2016, 22, 120–136. [Google Scholar] [CrossRef]
- Caselli, M.C.; Bello, A.; Rinaldi, P.; Stefanini, S.; Pasqualetti, P. Il Primo vocabolario del bambino. In Gesti, Parole e Frasi. Forme Lunghe e Forme Brevi del Questionario e Valori di Riferimento per la Fascia 8–36 Mesi; Franco Angeli: Milano, Italy, 2015. [Google Scholar]
- Rinaldi, P.; Pasqualetti, P.; Stefanini, S.; Bello, A.; Caselli, M.C. The Italian Words and Sentences MB-CDI: Normative data and concordance between complete and short forms. J. Child Lang. 2019, 46, 546–566. [Google Scholar] [CrossRef]
- Lasorsa, F.R.; Caselli, M.C.; Simonelli, I.; Stefanini, S.; Pasqualetti, P.; Rinaldi, P. Exploring Agreement between MB-CDI Short Forms for Evaluating the Language Skills of Italian Children Aged 18–24 Months. Folia Phoniatr. Logop. 2021, 73, 552–564. [Google Scholar] [CrossRef]
- Bello, A.; Giannantoni, P.; Pettenati, P.; Stefanini, S.; Caselli, M.C. Assessing lexicon: Validation and developmental data of the Picture Naming Game (PiNG), a new picture naming task for toddlers. Int. J. Lang. Comm. Dis. 2012, 47, 589–602. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Zoccolotti, P.; Friedmann, N. From dyslexia to dyslexias, from dysgraphia to dysgraphias, from a cause to causes: A look at current research on developmental dyslexia and dysgraphia. Cortex 2010, 46, 1211–1215. [Google Scholar] [CrossRef] [PubMed]
- Montecchi, C.; Rinaldi, S. The Primary Language Disorder and the School Learning. A Systematic Review. Logop. Comun. 2022, 18, 231–262. [Google Scholar] [CrossRef]




| Domain | Variable | Coding |
|---|---|---|
| Biological factor (data taken from the anamnestic section of the MB-CDI) | child’s sex/gender | 0 = girl; |
| 1 = boy | ||
| family history of language and/or learning disorders as a proxy of familial risk of SLD | 0 = absence; | |
| 1 = presence | ||
| Environmental factor (data taken from the anamnestic section of the MB-CDI) | mother’s level of education | 0 = primary/secondary school; |
| 1 = high school; | ||
| 2 = university | ||
| Communicative and linguistic abilities (data taken from the MB-CDI) | use communicative gestures | 0 = not yet; |
| to name or to request | 1 = sometimes/often; | |
| requesting pointing | 0 = not yet; | |
| 1 = sometimes/often | ||
| declarative pointing | 0 = not yet; | |
| 1 = sometimes/often | ||
| verbal imitation frequency | 0 = not yet; | |
| 1 = sometimes/often | ||
| pretending play | 0 = not yet; | |
| 1 = sometimes/often | ||
| decontextualized | 0 = not yet; | |
| comprehension | 1 = sometimes/often | |
| phonological accuracy | 0 = only caregivers understand him/her; | |
| 1 = simplifies words; | ||
| 2 = speaks like an adult | ||
| vocabulary size | 0 = <10th percentile; | |
| 1 = >10th percentile | ||
| word–word combination use | 0 = not yet; | |
| 1 = sometimes/often |
| No Previous LD or DLD | Previous LD (without DLD) | DLD (without LD) | DLD (with Previous LD) | |
|---|---|---|---|---|
| Children with SLD n = 37 | 24 (64.86%) | 2 (5.41%) | 2 (5.41%) | 9 (24.32%) |
| Children without SLD n = 491 | 391 (79.63%) | 50 (10.18%) | 27 (5.5%) | 23 (4.68%) |
| Dependent Variable: Presence of SLD | |||||||
|---|---|---|---|---|---|---|---|
| Univariable Analysis | Multivariable Analysis | ||||||
| Independent Variable | Category | OR | 95% CI | p Value | OR | 95% CI | Adj p Value |
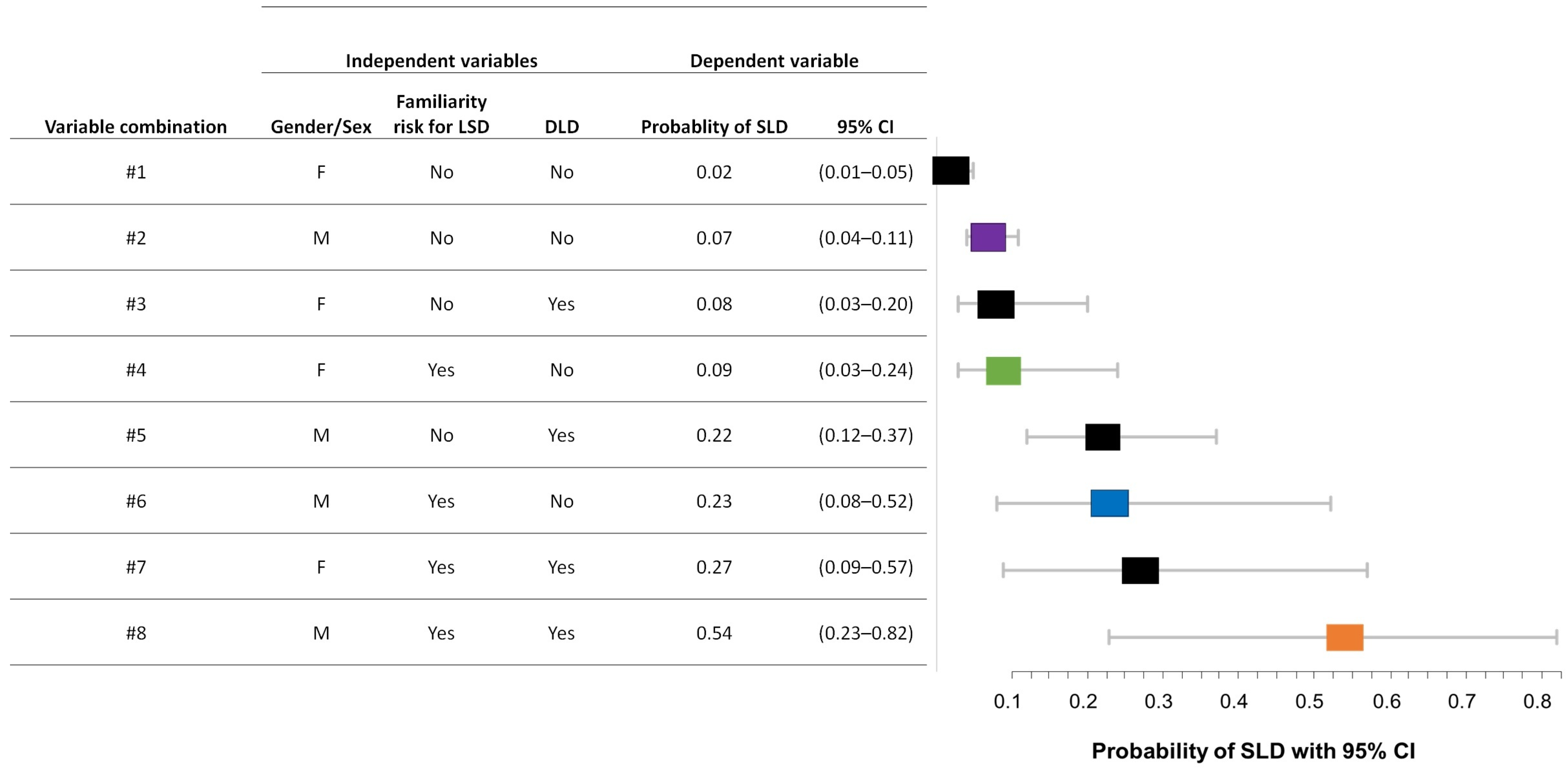
| Child’s sex/gender | M vs. F | 2.74 | 1.25–6.67 | 0.016 | 3.33 | 1.28–7.69 | 0.017 |
| Familial risk of LSD | Yes vs. No | 3.04 | 0.84–8.72 | 0.056 | 4.12 | 1.19–14.29 | 0.028 |
| Mother’s level of education | Primary/secondary vs. High school | 2.0 | 0.87–4.54 | 0.103 | |||
| Primary/secondary vs. University | 2.50 | 0.88–7.14 | 0.086 | Not selected by stepwise | |||
| Use of communicative gestures | Not yet vs. Sometimes/Often | 1.89 | 0.41–9.09 | 0.411 | |||
| Requesting pointing | Not yet vs. Sometimes/Often | 1.85 | 0.22–16.67 | 0.568 | |||
| Declarative pointing | Not yet vs. Sometimes/Often | 0.84 | 0.32–2.22 | 0.722 | |||
| Verbal imitation | Not yet vs. Sometimes/Often | 4.27 | 1.48–12.33 | 0.007 | Not selected by stepwise | ||
| Phonological accuracy | Only caregivers understand him/her vs. simplifies words/speaks like an adult | 1.12 | 0.54–2.32 | 0.771 | |||
| Vocabulary size | <10th percentile vs. >10th percentile | 2.57 | 1.12–5.55 | 0.019 | Not selected by stepwise | ||
| Word–word combination | Not yet vs. Sometimes/Often | 2.33 | 1.04–5.17 | 0.038 | Not selected by stepwise | ||
| Presence of DLD | Yes vs. No | 3.77 | 1.62–8.26 | 0.001 | 3.88 | 1.69–8.91 | 0.002 |
| Dependent Variable: Presence of DLD | |||||||
|---|---|---|---|---|---|---|---|
| Univariable Analysis | Multivariable Analysis | ||||||
| Independent Variable | Category | OR | 95% CI | p Value | OR | 95% CI | Adj p Value |
| Child’s sex/gender | M vs. F | 1.22 | 0.70–2.17 | 0.482 | |||
| Familial risk of LSD | Yes vs. No | 2.08 | 0.67–5.44 | 0.163 | |||
| Mother’s level of education | Primary/secondary vs. High school | 1.25 | 0.58–2.63 | 0.57 | |||
| Primary/secondary vs. University | 1.22 | 0.52–2.86 | 0.653 | ||||
| Declarative pointing | Not yet vs. Sometimes/Often | 0.56 | 0.23–1.35 | 0.195 | |||
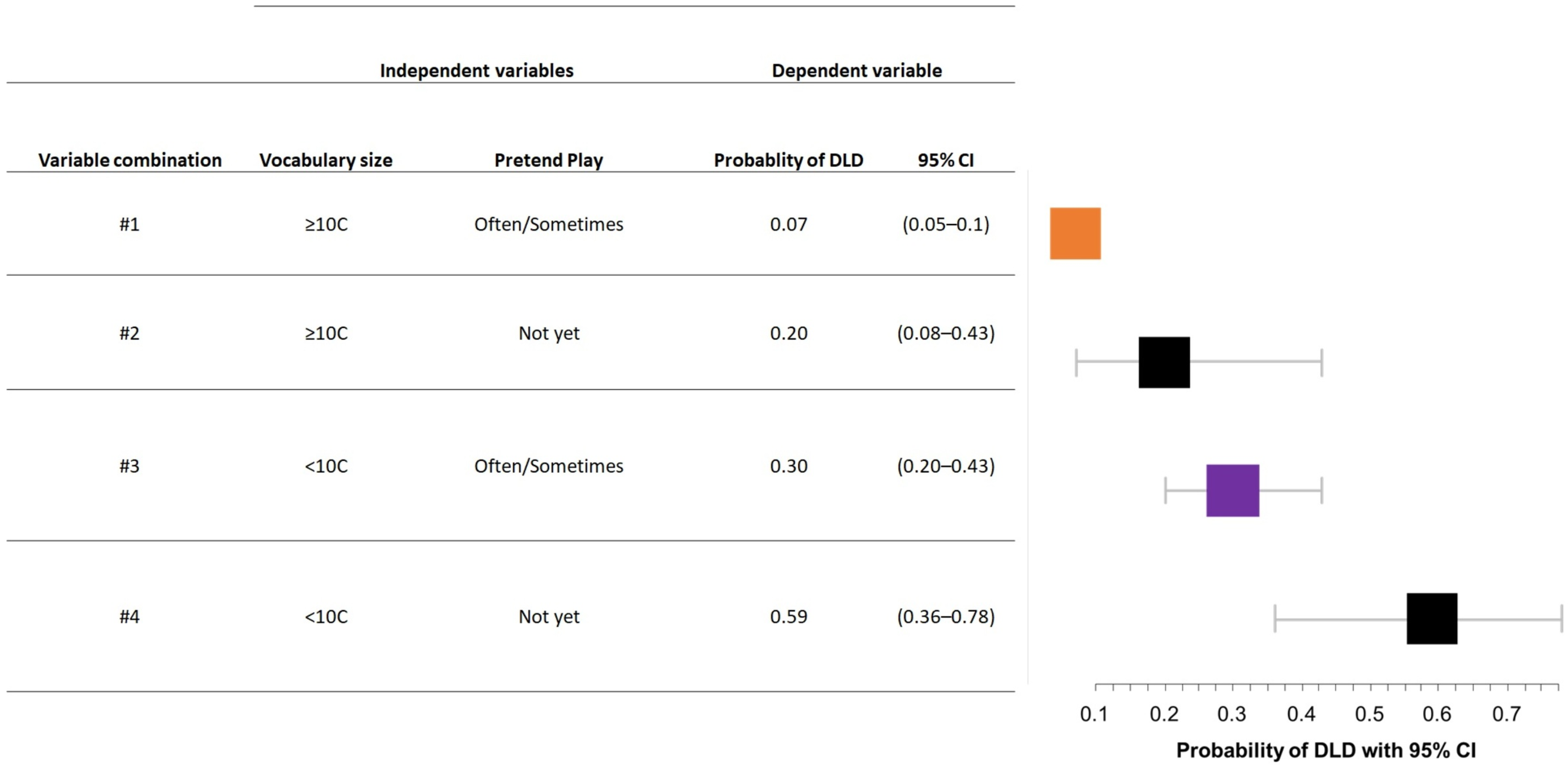
| Pretend play | Not yet vs. Sometimes/Often | 2.63 | 1.13–6.15 | 0.025 | Not selected by stepwise | ||
| Decontextualized comprehension | Not yet vs. Sometimes/Often | 1.55 | 0.18–13.52 | 0.69 | |||
| Verbal imitation | Not yet vs. Sometimes/Often | 11.2 | 4.61–27.35 | <0.001 | 3.22 | 1.14–9.09 | 0.028 |
| Phonological accuracy | Only caregivers understand him/her vs. simplifies words/speaks like an adult | 1.45 | 0.83–2.55 | 0.197 | |||
| Vocabulary size | <10th percentile vs. >10th percentile | 7.53 | 4.09–13.9 | <0.001 | 5.73 | 2.95–11.14 | <0.001 |
| Word–word combination | Not yet vs. Sometimes/Often | 6.77 | 3.71–12.32 | <0.001 | Not selected by stepwise | ||
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Independent Variable | Category | OR | 95% CI | p Value | OR | 95% CI | Adj p Value |
| Child’s sex/gender | M vs. F | 1.67 | 1.03–2.70 | 0.037 | Not selected by stepwise | ||
| Familial risk of SLD | Yes vs. No | 1.72 | 0.67–4.44 | 0.262 | |||
| Mother’s level of education | Primary/secondary vs. High school | 1.56 | 0.83–2.86 | 0.163 | Not selected by stepwise | ||
| Primary/secondary vs. University | 2.33 | 1.09–5.00 | 0.03 | ||||
| Use of communicative gestures | Not yet vs. Sometimes/Often | 0.99 | 0.52–1.89 | 0.982 | |||
| Pretend play | Not yet vs. Sometimes/Often | 2.15 | 0.96–4.81 | 0.063 | Not selected by stepwise | ||
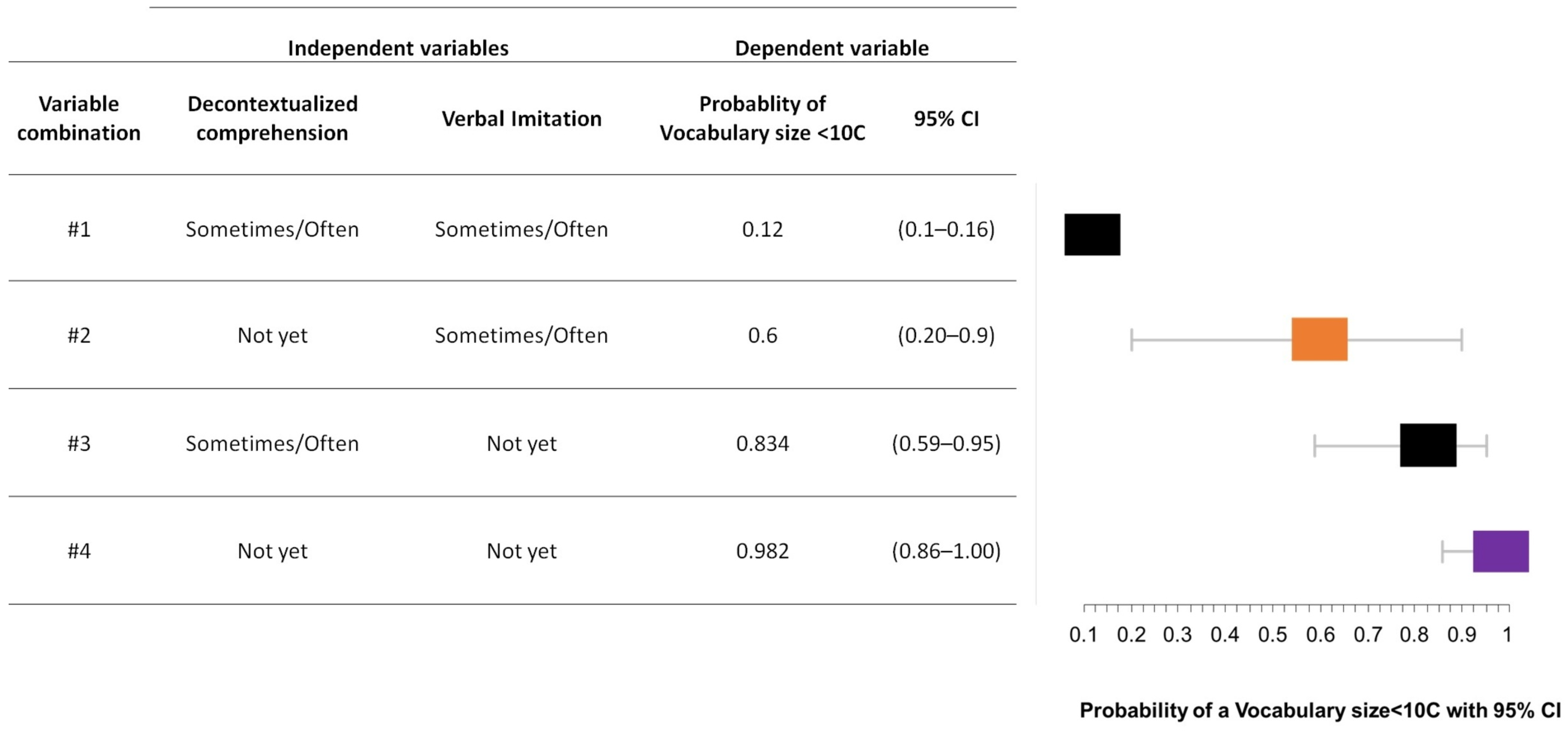
| Decontextualized comprehension | Not yet vs. Sometimes/Often | 11.25 | 2.03–62.5 | 0.006 | 11.11 | 1.78–50 | 0.017 |
| Verbal imitation | Not yet vs. Sometimes/Often | 44.43 | 12.8–154.53 | <0.001 | 33.33 | 10–100 | <0.001 |
| Phonological accuracy | Only caregivers understand him/her vs. simplifies words/speaks like an adult | 1.23 | 0.49–1.34 | 0.416 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rinaldi, P.; Bello, A.; Simonelli, I.; Caselli, M.C. Is Specific Learning Disorder Predicted by Developmental Language Disorder? Evidence from a Follow-Up Study on Italian Children. Brain Sci. 2023, 13, 701. https://doi.org/10.3390/brainsci13040701
Rinaldi P, Bello A, Simonelli I, Caselli MC. Is Specific Learning Disorder Predicted by Developmental Language Disorder? Evidence from a Follow-Up Study on Italian Children. Brain Sciences. 2023; 13(4):701. https://doi.org/10.3390/brainsci13040701
Chicago/Turabian StyleRinaldi, Pasquale, Arianna Bello, Ilaria Simonelli, and Maria Cristina Caselli. 2023. "Is Specific Learning Disorder Predicted by Developmental Language Disorder? Evidence from a Follow-Up Study on Italian Children" Brain Sciences 13, no. 4: 701. https://doi.org/10.3390/brainsci13040701