
Neurophysiological and Clinical Effects of Upper Limb Robot-Assisted Rehabilitation on Motor Recovery in Patients with Subacute Stroke: A Multicenter Randomized Controlled Trial Study Protocol
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
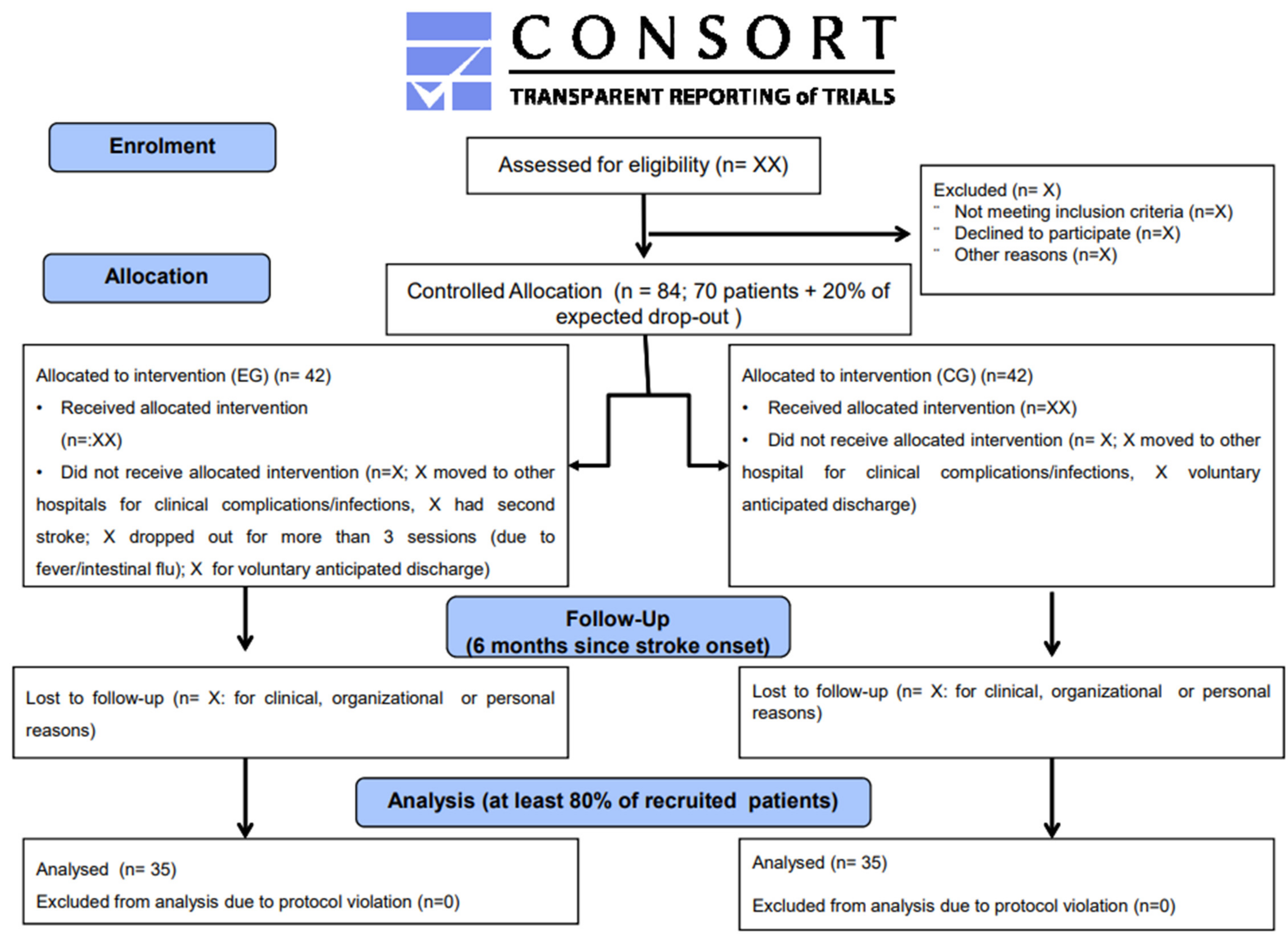
2.1. Study Design
2.2. Participants (Recruitment)
2.3. Sample Population and Randomization
2.4. Outcome Assessment
2.5. Clinical Outcome Measure
2.5.1. Primary Outcome
2.5.2. Secondary Outcomes
- Body function: MAS (shoulder, elbow, and wrist);
- Activity (capacity/performance): Box and Block Test; Nine Hole Peg Test; Frenchay Arm Test; Modified Barthel Index;
- Participation: Modified Rankin Scale.
- A_FORCE: measures of the force exerted by the patient for each movement;
- A_MOVE: measures the patient’s 3D work area (paint the walls of the room);
- A-GOAL: movement functionality.
2.6. Neurophysiological Signals
3. Procedure
3.1. Control Group
3.2. Experimental Group
3.3. Safety and Adverse Event Reporting
3.4. Data Management
3.5. Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwakkel, G.; Kollen, B.J.; van der Grond, J.; Prevo, A.J. Probability of regaining dexterity in the flaccid upper limb: Impact of severity of paresis and time since onset in acute stroke. Stroke 2003, 34, 2181–2186. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2018, 9, CD006876. [Google Scholar] [CrossRef] [PubMed]
- Tomassini, V.; Jbabdi, S.; Kincses, Z.T.; Bosnell, R.; Douaud, G.; Pozzilli, C.; Matthews, P.M.; Johansen-Berg, H. Structural and functional bases for individual differences in motor learning. Hum. Brain Mapp. 2011, 32, 494–508. [Google Scholar] [CrossRef] [PubMed]
- Waddell, K.J.; Birkenmeier, R.L.; Moore, J.L.; Hornby, T.G.; Lang, C.E. Feasibility of high-repetition, task-specific training for individuals with upper-extremity paresis. Am. J. Occup. Ther. 2014, 68, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, H.; Bosomworth, H.; Krebs, H.I.; van Wijck, F.; Howel, D.; Wilson, N.; Aird, L.; Alvarado, N.; Andole, S.; Cohen, D.L.; et al. Robot assisted training for the upper limb after stroke (RATULS): A multicentre randomised controlled trial. Lancet 2019, 394, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, R.S.; Morone, G.; Naro, A.; Gandolfi, M.; Liotti, V.; D’aurizio, C.; Straudi, S.; Focacci, A.; Pournajaf, S.; Aprile, I.; et al. Robot-Assisted Training for Upper Limb in Stroke (ROBOTAS): An Observational, Multicenter Study to Identify Determinants of Efficacy. J. Clin. Med. 2021, 10, 5245. [Google Scholar] [CrossRef] [PubMed]
- Duret, C.; Hutin, E.; Lehenaff, L.; Gracies, J.M. Do all sub acute stroke patients benefit from robot-assisted therapy? A retrospective study. Restor. Neurol. Neurosci. 2015, 33, 57–65. [Google Scholar] [CrossRef]
- Morone, G.; Cocchi, I.; Paolucci, S.; Iosa, M. Robot-assisted therapy for arm recovery for stroke patients: State of the art and clinical implication. Expert Rev. Med. Devices 2020, 17, 223–233. [Google Scholar] [CrossRef]
- Klamroth-Marganska, V.; Blanco, J.; Campen, K.; Curt, A.; Dietz, V.; Ettlin, T.; Felder, M.; Fellinghauer, B.; Guidali, M.; Kollmar, A.; et al. Three-dimensional, task-specific robot therapy of the arm after stroke: A multicentre, parallel-group randomised trial. Lancet Neurol. 2014, 13, 159–166. [Google Scholar] [CrossRef]
- Morone, G.; Capone, F.; Iosa, M.; Cruciani, A.; Paolucci, M.; Martino Cinnera, A.; Musumeci, G.; Brunelli, N.; Costa, C.; Paolucci, S.; et al. May Dual Transcranial Direct Current Stimulation Enhance the Efficacy of Robot-Assisted Therapy for Promoting Upper Limb Recovery in Chronic Stroke? Neurorehabilit. Neural Repair 2022, 36, 800–809. [Google Scholar] [CrossRef]
- Maier, M.; Ballester, B.R.; Verschure, P.F.M.J. Principles of Neurorehabilitation after Stroke Based on Motor Learning and Brain Plasticity Mechanisms. Front. Syst. Neurosci. 2019, 13, 74. [Google Scholar] [CrossRef] [PubMed]
- Ballanti, S.; Campagnini, S.; Liuzzi, P.; Hakiki, B.; Scarpino, M.; Macchi, C.; Oddo, C.M.; Carrozza, M.C.; Grippo, A.; Mannini, A. EEG-based methods for recovery prognosis of patients with disorders of consciousness: A systematic review. Clin. Neurophysiol. 2022, 144, 98–114. [Google Scholar] [CrossRef] [PubMed]
- Asadi, B.; Cuenca-Zaldivar, J.N.; Nakhostin Ansari, N.; Ibáñez, J.; Herrero, P.; Calvo, S. Brain Analysis with a Complex Network Approach in Stroke Patients Based on Electroencephalography: A Systematic Review and Meta-Analysis. Healthcare 2023, 11, 666. [Google Scholar] [CrossRef]
- Nuwer, M.R.; Husain, A.M.; Soto, F. Overview of intraoperative neuromonitoring. Handb. Clin. Neurol. 2022, 186, 3–9. [Google Scholar] [PubMed]
- Milani, G.; Antonioni, A.; Baroni, A.; Malerba, P.; Straudi, S. Relation between EEG Measures and Upper Limb Motor Recovery in Stroke Patients: A Scoping Review. Brain Topogr. 2022, 35, 651–666. [Google Scholar] [CrossRef]
- Khan, A.; Chen, C.; Yuan, K.; Wang, X.; Mehra, P.; Liu, Y.; Tong, K.Y. Changes in electroencephalography complexity and functional magnetic resonance imaging connectivity following robotic hand training in chronic stroke. Top. Stroke Rehabil. 2021, 28, 276–288. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European recommendations for surface electromyography. Roessingh Res. Dev. 1999, 8, 13–54. [Google Scholar]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Russo, M.; Milardi, D.; Leo, A.; Filoni, S.; Trinchera, A.; Bramanti, P. Is two better than one? Muscle vibration plus robotic rehabilitation to improve upper limb spasticity and function: A pilot randomized controlled trial. PLoS ONE 2017, 12, e0185936. [Google Scholar] [CrossRef]
- Kwakkel, G.; Kollen, B.; Twisk, J. Impact of Time on Improvement of Outcome after Stroke. Stroke 2006, 37, 2348–2353. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.; Mazzoleni, S.; Morone, G.; Iosa, M.; Galletti, F.; Smania, N. The role of feedback in the robotic-assisted upper limb rehabilitation in people with multiple sclerosis: A systematic review. Expert Rev. Med. Devices 2023, 20, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.G.; Maresca, G.; De Luca, R.; Stagnitti, M.C.; Porcari, B.; Ferrera, M.C.; Galletti, F.; Casella, C.; Manuli, A.; Calabrò, R.S. The Growing Use of Virtual Reality in Cognitive Rehabilitation: Fact, Fake or Vision? A Scoping Review. J. Natl. Med. Assoc. 2019, 111, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Norman, S.L.; Wolpaw, J.R.; Reinkensmeyer, D.J. Targeting neuroplasticity to improve motor recovery after stroke: An artificial neural network model. Brain Commun. 2022, 4, fcac264. [Google Scholar] [CrossRef]
- Hwang, F.J.; Roth, R.H.; Wu, Y.W.; Sun, Y.; Kwon, D.K.; Liu, Y.; Ding, J.B. Motor learning selectively strengthens cortical and striatal synapses of motor engram neurons. Neuron 2022, 110, 2790–2801.e5. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, R.S.; Naro, A.; Russo, M.; Leo, A.; De Luca, R.; Balletta, T.; Buda, A.; La Rosa, G.; Bramanti, A.; Bramanti, P. The role of virtual reality in improving motor performance as revealed by EEG: A randomized clinical trial. J. Neuroeng. Rehabil. 2017, 14, 53. [Google Scholar] [CrossRef]


{kind=link}
| TIDieR Item | Experimental Group | Control Group | Experimental and Control Groups | |||
|---|---|---|---|---|---|---|
| 1. Name | Upper limb rehabilitation through Armeo Power exoskeleton | Upper limb rehabilitation through conventional therapy | Passive, active-assisted, and active exercises addressed for shoulder, arm, and hand motor rehabilitation | Exercises for muscle strength | Stretching exercises | Functional activity training |
| 2. Why | To improve upper limb motor functioning | To improve upper limb motor functioning | To improve mobility and muscle activation, to preserve the passive range-of-motion (ROM), and to prevent contractures and spasticity | To improve muscle strength | To prevent muscle retraction/contractures and spasticity | To improve autonomy in activities of daily living |
| 3. What (materials) | Exoskeleton with auditory and visual bio-feedback | Proprioceptive and therapy objects | With or without continuous shoulder and/or elbow passive motion | Soft weights, elastic resistance bands, and therapy objects assisted by physiotherapist | Manually assisted by physiotherapist | Objects typically present in the home for activities of daily living |
| 4.What (procedures) | The exoskeleton will be donned and customized on the patient and they will be asked to interact with it in an assist-as-needed modality, receiving a real-time visual biofeedback and interacting with serious video-games.During the first session, the device will be adjusted to the patient’s arm size and the angle of suspension. The working space and the exercises will be selected once the upper limb has been fitted with the system. The selection of personalized exercises is based on the motor skills of each patient and the difficulty can be gradually increased during training. | The exercises will consist of passive, active-assisted, and active exercises for the shoulder, elbow, and wrist in a seated position | Gradual increasing the degree of flexion and extension or a physical therapist will passively mobilize the joints into flexion and extension | The exercises will consist of isometric, isotonic contraction of the upper limb muscles | The exercises will consist of stretching the upper limb muscles | The patients will follow training on activities of daily living. The patient will perform training with assistance, with aids, or autonomously. |
| 5. Who provided | Senior physical therapists who are experts in neurorehabilitation | Occupational Therapists | ||||
| 6. How | An individual face-to-face treatment session | |||||
| 7. Where | Rehabilitation gym in an intensive subacute rehabilitation hospital | |||||
| 8. When and how much | 45 + 60 (occupational therapy; functional therapy (trunk control, standing, and walking training), speech therapy, and/or neuro-cognitive therapy) | |||||
| 9. Tailoring | The exercise will be tailored to participants’ goals, current abilities, and preferences, also considering the patient’s point of view | |||||
| 10. Modifications | The exercises difficulty will be increased gradually session by session, depending on current progress, level of pain, and ability. | |||||
| 11. How well (planned) | Organizing periodical updating meetings with the team of physical therapists and other clinicians involved in the study to conduct the treatments in the most homogeneous way possible and to address any problems and/or critical points that may be encountered during the trial execution. | |||||
| 12. How well (actual) | Physical therapist delivering the treatments will register how many sessions a patient attended and completed. | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pournajaf, S.; Morone, G.; Straudi, S.; Goffredo, M.; Leo, M.R.; Calabrò, R.S.; Felzani, G.; Paolucci, S.; Filoni, S.; Santamato, A.; et al. Neurophysiological and Clinical Effects of Upper Limb Robot-Assisted Rehabilitation on Motor Recovery in Patients with Subacute Stroke: A Multicenter Randomized Controlled Trial Study Protocol. Brain Sci. 2023, 13, 700. https://doi.org/10.3390/brainsci13040700
Pournajaf S, Morone G, Straudi S, Goffredo M, Leo MR, Calabrò RS, Felzani G, Paolucci S, Filoni S, Santamato A, et al. Neurophysiological and Clinical Effects of Upper Limb Robot-Assisted Rehabilitation on Motor Recovery in Patients with Subacute Stroke: A Multicenter Randomized Controlled Trial Study Protocol. Brain Sciences. 2023; 13(4):700. https://doi.org/10.3390/brainsci13040700
Chicago/Turabian StylePournajaf, Sanaz, Giovanni Morone, Sofia Straudi, Michela Goffredo, Maria Rosaria Leo, Rocco Salvatore Calabrò, Giorgio Felzani, Stefano Paolucci, Serena Filoni, Andrea Santamato, and et al. 2023. "Neurophysiological and Clinical Effects of Upper Limb Robot-Assisted Rehabilitation on Motor Recovery in Patients with Subacute Stroke: A Multicenter Randomized Controlled Trial Study Protocol" Brain Sciences 13, no. 4: 700. https://doi.org/10.3390/brainsci13040700