
Betting on Non-Invasive Brain Stimulation to Treat Gambling Disorder: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Records Screening and Data Extraction
2.3. Studies Quality Assessment
2.4. Quantitative Analysis
3. Systematic Review Results
3.1. Studies Selection
3.2. Quality Assessment
3.3. Participants’ Characteristics
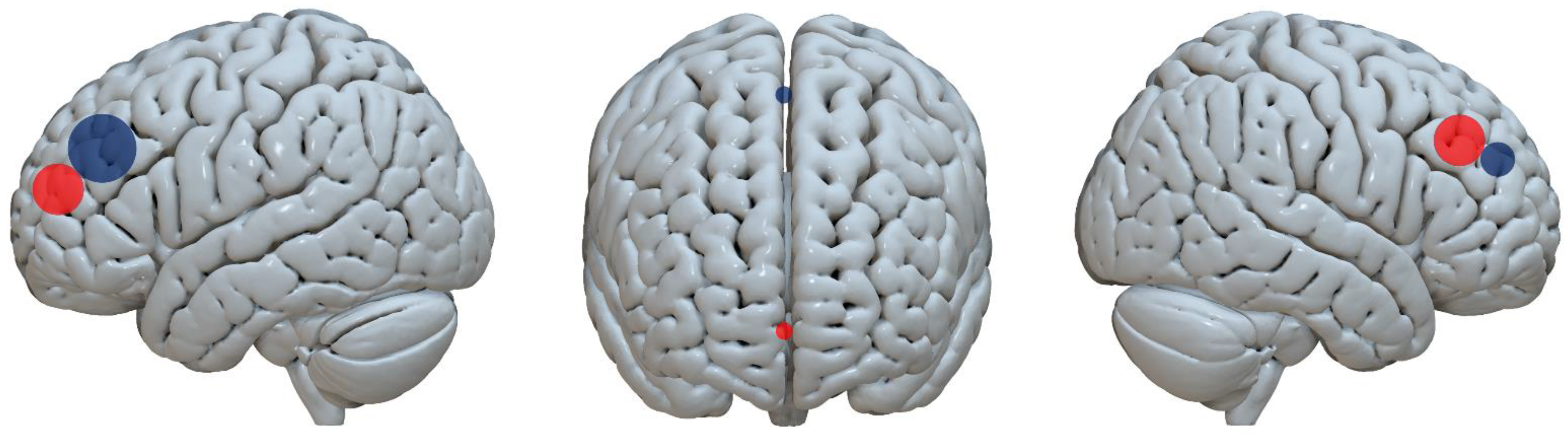
3.4. Stimulation Protocols
3.5. TDCS Studies

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References | Stimulation Site | Stimulation Protocol | Craving Measures Included | Other Measures (Clinical/Behavioral) | Follow-Up | Study Design | Blinding | Results |
|---|---|---|---|---|---|---|---|---|
| Del Mauro et al. [98] | Left and right DLPFC | Anode right DLPFC and cathode left DLPFC. Intensity 2 mA, 20 min, electrodes 5 × 5, three sessions per week for two weeks. | MATE | VAS; SCQ; BDI; SCL-90 (GSI index); WHOQOL-B; and BIS-11 | At 3 and 6 months after treatment | Open label | NR | Improvements in craving scores, desire to use substances, mood, impulsivity, and quality of life |
| Martinotti et al. * [100] | Left and right DLPFC | Anode right DLPFC, cathode left DLPFC; 1.5 mA, 20 min, electrodes 5 × 5, 5 consecutive days (1 tDCS session per day) | VAS | BIS-11; gambling behaviors/substance consumption Timeline Follow-Back; HAM-D; HAM-A; and Y-MRS | None | Randomized sham-controlled | Double-blind | Overall reductions in anxiety, mood, impulsivity, and craving scores. In the latter, larger effects in the real condition |
| Soyata et al. * [99] | Left and right DLPFC | Anode right DLPFC, cathode left DLPFC; 2 mA, 20 min, electrodes 5 × 7, 3 every-other-day sessions (active or sham) | NR | SOGS, PGSI and BIS-11 (at baseline); IGT; and WCST | None | Randomized sham-controlled | Triple-blind | Improvements in cognitive flexibility and decision-making processes in the real tDCS group |
3.6. TMS Studies
| References | Stimulation Site | Stimulation Protocol | Craving Measures Included | Other Measures (Clinical/Behavioral) | Follow-Up | Study Design | Blinding | Results |
|---|---|---|---|---|---|---|---|---|
| Cardullo et al. [103] | Left DLPFC | Twice daily for 5 consecutive days and twice daily once a week over 8 weeks; 15 Hz, 100% of the RMT; 60 impulses per train, 15 s ITI, 40 trains, 13 min duration | G-SAS | CCQ; PSQI; BDI-II; SAS; and SCL-90-R (GSI index) | After 5, 30, and 60 days of treatment | Case series | NR | Gambling severity, craving for cocaine, and negative-affect symptoms improved after treatment and at the follow-ups |
| Gay et al. [102] | Left DLPFC | Two sessions of active and sham rTMS (1-week washout); 10 Hz, 110% of the RMT, 94 trains, 10 s ITI, 3008 pulses in total | VAS cue-induced | NCs control; NCs desire; and PG-YBOCS | None | Randomized sham-controlled crossover | Double-blind | Improvements in cue-induced craving after the real rTMS. No changes in gambling behavior 7 days after |
| Pettorruso et al. [104] | Left DLPFC | Twice daily, 5 days a week for 2 weeks (20 sessions) and twice daily once a week for three months (24 sessions); 15 Hz, 100% RMT, 60 pulses per train, 15 s ITI, 40 trains, 2400 pulses, 13 min duration | PG-YBOCS | G-SAS; Gambling behaviors Timeline Follow Back; BDI; and SAS² | 2, 4, 8, and 12 weeks | Open label | NR | Improvements in gambling severity and the days spent gambling after the intensive and maintenance phases |
| Rosenberg et al. [105] | Left DLPFC | 15 sessions (1 session/day), 1 Hz, 110% RMT, 10 min duration | VAS | DAGS; Y-BOCS; HDRS; HARS; SOGS; CGI-I; and SAS³ | Families’ interviews | Open label | NR | The authors reported no significant effect. Scores seemed to reduce, but no statistical analysis was provided |
| Salerno et al. [106] | Pre-SMA, bilaterally | 10 sessions of cTBS. CTBS consists of bursts of 3 pulses separated by 20 ms (i.e., 50 Hz), with each triplet repeated every 200 ms (i.e., 5 Hz); 80% of RMT, 2 trains of 600 pulses, separated by 1 min, a total of 1200 pulses | PG-YBOCS | GUQ; BIS-11; HAM-A; HAM-D; SDS; CGI; and FTND | After the 10 sessions and after 30 days | Open label | NR | Significant improvement in GD severity and CGI after treatment and at follow-up |
| Sauvaget et al. * [101] | Right DLPFC | Two sessions of active and sham rTMS (1-week washout); 1 Hz, 120% of RMT, one train, 360 pulses, 6 min duration | VAS | GACS; heart rate; and blood pressure | None | Randomized sham-controlled crossover | Double-blind | Improvement in the urge to gamble after treatment. No differences between real vs. sham stimulations |
| Zack et al. [81] | mPFC, right DLPFC | Three sessions: rTMS, cTBS, and sham (1-week washout). RTMS: mPFC, 80% of AMT, 3 epochs of 15 10-pulse trains, 10 Hz, 10 s ITI, 450 pulses. CTBS: right DLPFC, 80% of AMT, 3 cTBS epochs, 50 Hz, 900 pulses in total | VAS pre and post-TMS | DDT; Stroop task; blood pressure; ARCI; POMS-vigor scale; and VAS pre and post-slot machine game | None | Sham-controlled crossover | Double-blind | Reduction in the desire to gamble after rTMS, but not cTBS. |
3.7. Outcome Measures
4. Meta-Analysis Results
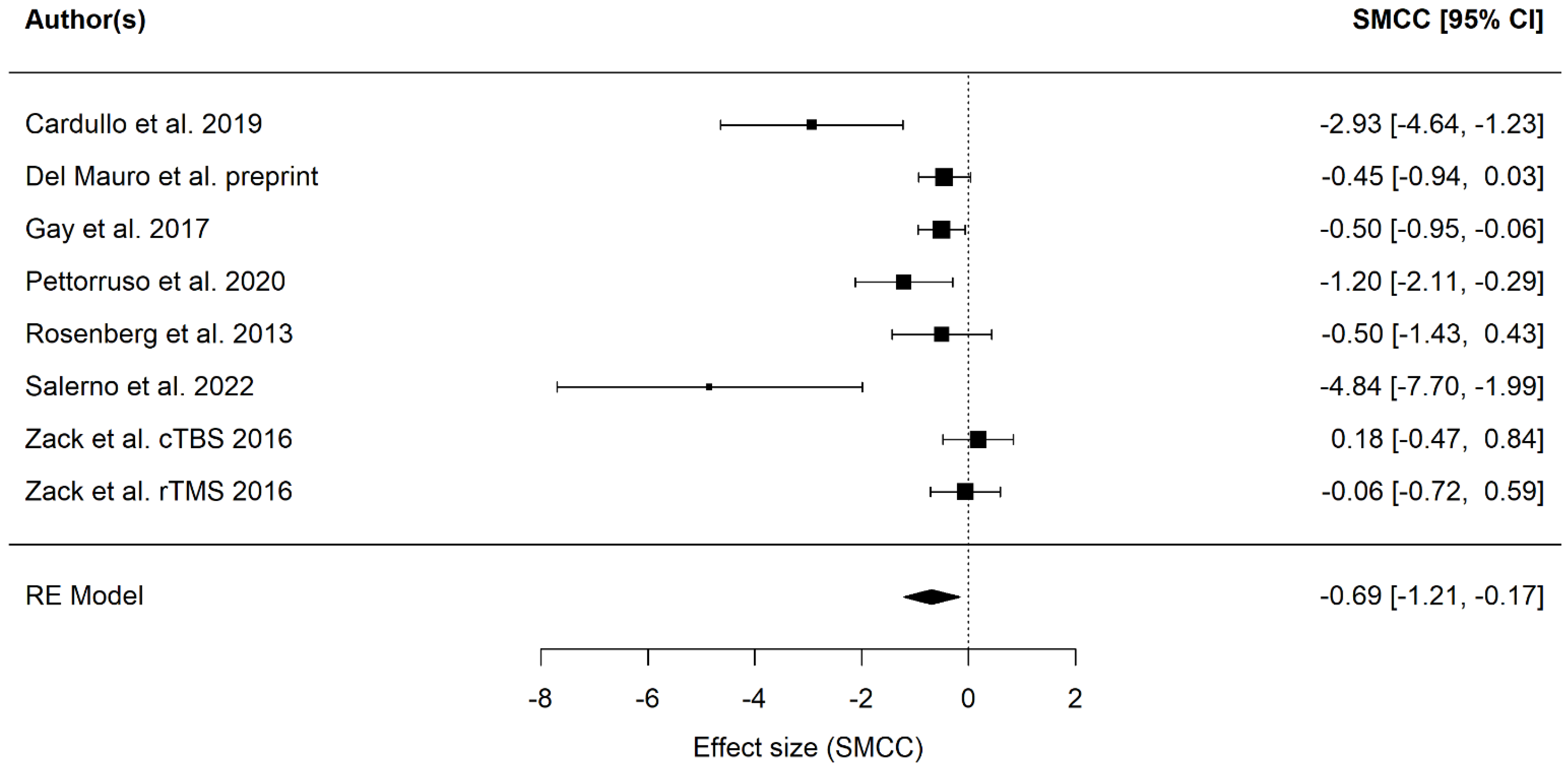
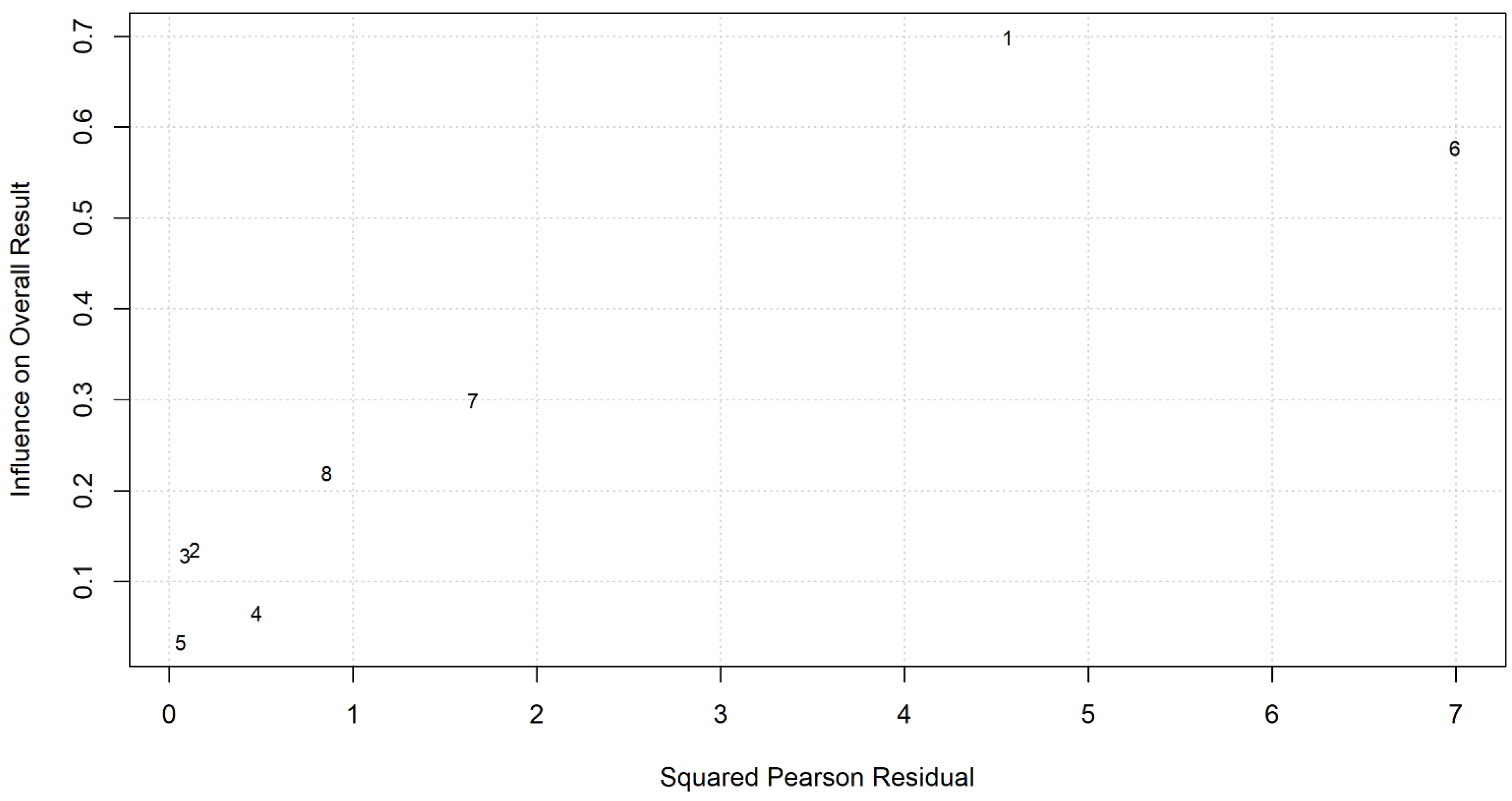
4.1. Primary Endpoint: Craving Scores
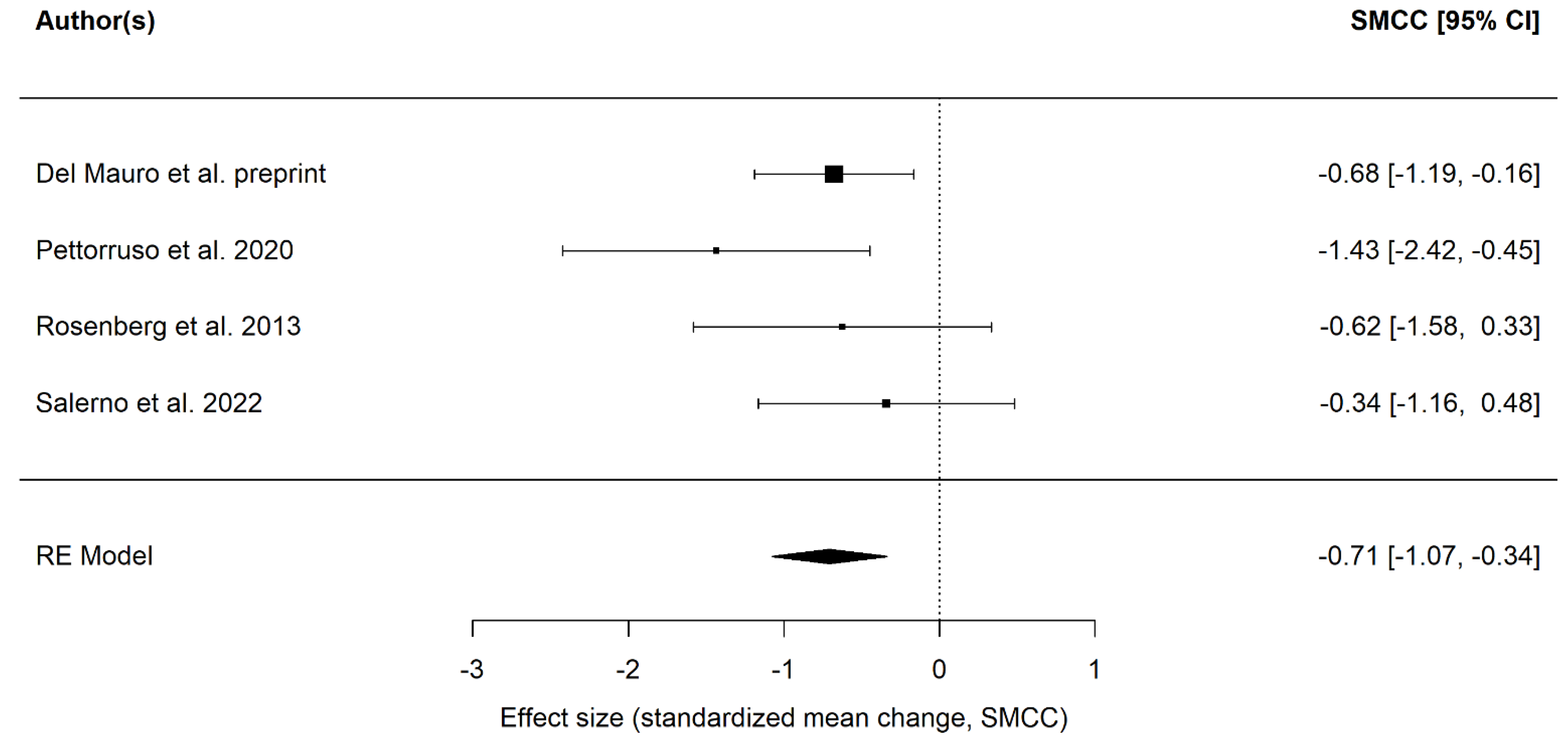
4.2. Secondary Endpoint: Depressive Symptoms
5. Discussion
Limitations and Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Potenza, M.N.; Kosten, T.R.; Rounsaville, B.J. Pathological gambling. Jama 2001, 286, 141–144. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American psychiatric association: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th ed.; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Romanczuk-Seiferth, N.; Brink, W.V.D.; Goudriaan, A.E. From Symptoms to Neurobiology: Pathological Gambling in the Light of the New Classification in DSM-5. Neuropsychobiology 2014, 70, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Abbott, M.; Romild, U.; Volberg, R. The prevalence, incidence, and gender and age-specific incidence of problem gambling: Results of the Swedish longitudinal gambling study (Swelogs). Addiction 2018, 113, 699–707. [Google Scholar] [CrossRef]
- Karlsson, A.; Håkansson, A. Gambling disorder, increased mortality, suicidality, and associated comorbidity: A longitudinal nationwide register study. J. Behav. Addict. 2018, 7, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Calado, F.; Griffiths, M. Problem gambling worldwide: An update and systematic review of empirical research (2000–2015). J. Behav. Addict. 2016, 5, 592–613. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Hwang, I.; LaBrie, R.; Petukhova, M.; Sampson, N.A.; Winters, K.C.; Shaffer, H.J. DSM-IV pathological gambling in the National Comorbidity Survey Replication. Psychol. Med. 2008, 38, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Petry, N.M.; Stinson, F.S.; Grant, B.F. Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 2005, 66, 564–574. [Google Scholar] [CrossRef]
- Ioannidis, K.; Hook, R.; Wickham, K.; Grant, J.E.; Chamberlain, S.R. Impulsivity in Gambling Disorder and problem gambling: A meta-analysis. Neuropsychopharmacology 2019, 44, 1354–1361. [Google Scholar] [CrossRef]
- Lorains, F.K.; Cowlishaw, S.; Thomas, S.A. Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys. Addiction 2011, 106, 490–498. [Google Scholar] [CrossRef]
- Fernie, B.A.; Caselli, G.; Giustina, L.; Donato, G.; Marcotriggiani, A.; Spada, M.M. Desire thinking as a predictor of gambling. Addict. Behav. 2014, 39, 793–796. [Google Scholar] [CrossRef]
- Antons, S.; Brand, M.; Potenza, M.N. Neurobiology of cue-reactivity, craving, and inhibitory control in non-substance addictive behaviors. J. Neurol. Sci. 2020, 415, 116952. [Google Scholar] [CrossRef] [PubMed]
- Brand, M.; Wegmann, E.; Stark, R.; Müller, A.; Wölfling, K.; Robbins, T.W.; Potenza, M.N. The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: Update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors. Neurosci. Biobehav. Rev. 2019, 104, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mallorquí-Bagué, N.; Mestre-Bach, G.; Testa, G. Craving in gambling disorder: A systematic review. J. Behav. Addict. 2023, 12, 53–79. [Google Scholar] [CrossRef] [PubMed]
- Hawker, C.; Merkouris, S.; Youssef, G.; Dowling, N. Exploring the associations between gambling cravings, self-efficacy, and gambling episodes: An Ecological Momentary Assessment study. Addict. Behav. 2021, 112, 106574. [Google Scholar] [CrossRef]
- de Castro, V.; Fong, T.; Rosenthal, R.J.; Tavares, H. A comparison of craving and emotional states between pathological gamblers and alcoholics. Addict. Behav. 2007, 32, 1555–1564. [Google Scholar] [CrossRef]
- Quintero, M.J.; Navas, J.F.; Perales, J.C. The associative underpinnings of negative urgency and its role in problematic gambling behavior. Addict. Behav. 2020, 111, 106533. [Google Scholar] [CrossRef]
- Potenza, M.N.; Balodis, I.M.; Derevensky, J.; Grant, J.E.; Petry, N.M.; Verdejo-Garcia, A.; Yip, S.W. Gambling disorder. Nat. Rev. Dis. Prim. 2019, 5, 51. [Google Scholar] [CrossRef]
- Koob, G.F.; Volkow, N.D. Neurobiology of addiction: A neurocircuitry analysis. Lancet Psychiatry 2016, 3, 760–773. [Google Scholar] [CrossRef]
- Potenza, M.N. The neurobiology of pathological gambling and drug addiction: An overview and new findings. Philos. Trans. R. Soc. B: Biol. Sci. 2008, 363, 3181–3189. [Google Scholar] [CrossRef]
- Kober, H.; Lacadie, C.M.; Wexler, E.B.; Malison, R.T.; Sinha, R.; Potenza, M.N. Brain Activity During Cocaine Craving and Gambling Urges: An fMRI Study. Neuropsychopharmacology 2016, 41, 628–637. [Google Scholar] [CrossRef]
- Koehler, S.; Hasselmann, E.; Wüstenberg, T.; Heinz, A.; Romanczuk-Seiferth, N. Higher volume of ventral striatum and right prefrontal cortex in pathological gambling. Anat. Embryol. 2015, 220, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Luijten, M.; Schellekens, A.F.; Kühn, S.; Machielse, M.W.; Sescousse, G. Disruption of reward processing in addiction: An image-based meta-analysis of functional magnetic resonance imaging studies. JAMA Psychiatry 2017, 74, 387–398. [Google Scholar] [CrossRef]
- Potenza, M.N.; Steinberg, M.A.; Skudlarski, P.; Fulbright, R.K.; Lacadie, C.M.; Wilber, M.K.; Rounsaville, B.J.; Gore, J.C.; Wexler, B.E. Gambling urges in pathological gambling: A functional magnetic resonance imaging study. Arch. Gen. Psychiatry 2003, 60, 828–836. [Google Scholar] [CrossRef]
- Reuter, J.; Raedler, T.; Rose, M.; Hand, I.; Gläscher, J.; Büchel, C. Pathological gambling is linked to reduced activation of the mesolimbic reward system. Nat. Neurosci. 2005, 8, 147–148. [Google Scholar] [CrossRef] [PubMed]
- Potenza, M.N.; Leung, H.-C.; Blumberg, H.P.; Peterson, B.S.; Fulbright, R.K.; Lacadie, C.M.; Skudlarski, P.; Gore, J.C. An fMRI Stroop Task Study of Ventromedial Prefrontal Cortical Function in Pathological Gamblers. Am. J. Psychiatry 2003, 160, 1990–1994. [Google Scholar] [CrossRef] [PubMed]
- Limbrick-Oldfield, E.H.; Mick, I.; Cocks, E.R.; McGonigle, J.; Sharman, S.P.; Goldstone, A.P.; Stokes, A.P.R.; Waldman, A.; Erritzoe, D.; Bowden-Jones, H.; et al. Neural substrates of cue reactivity and craving in gambling disorder. Transl. Psychiatry 2017, 7, e992. [Google Scholar] [CrossRef]
- Rahman, A.S.; Xu, J.; Potenza, M.N. Hippocampal and Amygdalar Volumetric Differences in Pathological Gambling: A Preliminary Study of the Associations with the Behavioral Inhibition System. Neuropsychopharmacology 2014, 39, 738–745. [Google Scholar] [CrossRef]
- Braun, B.; Ludwig, M.; Sleczka, P.; Bühringer, G.; Kraus, L. Gamblers seeking treatment: Who does and who doesn’t? J. Behav. Addict. 2014, 3, 189–198. [Google Scholar] [CrossRef]
- Slutske, W.S. Natural Recovery and Treatment-Seeking in Pathological Gambling: Results of Two U.S. National Surveys. Am. J. Psychiatry 2006, 163, 297–302. [Google Scholar] [CrossRef]
- Suurvali, H.; Hodgins, D.; Toneatto, T.; Cunningham, J. Treatment seeking among Ontario problem gamblers: Results of a population survey. Psychiatr. Serv. 2008, 59, 1343–1346. [Google Scholar] [CrossRef]
- Maniaci, G.; La Cascia, C.; Picone, F.; Lipari, A.; Cannizzaro, C.; La Barbera, D. Predictors of early dropout in treatment for gambling disorder: The role of personality disorders and clinical syndromes. Psychiatry Res. 2017, 257, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.; Murphy, R.; Turner, J.; Sharman, S. Predictors of Dropout in Disordered Gamblers in UK Residential Treatment. J. Gambl. Stud. 2020, 36, 373–386. [Google Scholar] [CrossRef]
- Aragay, N.; Jiménez-Murcia, S.; Granero, R.; Fernández-Aranda, F.; Ramos-Grille, I.; Cardona, S.; Garrido, G.; Islam, M.A.; Menchón, J.M.; Vallès, V. Pathological gambling: Understanding relapses and dropouts. Compr. Psychiatry 2015, 57, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Murcia, S.; Álvarez-Moya, E.M.; Granero, R.; Aymami, M.N.; Gómez-Peña, M.; Jaurrieta, N.; Sans, B.; Rodriguez-Marti, J.; Vallejo, J. Cognitive–behavioral group treatment for pathological gambling: Analysis of effectiveness and predictors of therapy outcome. Psychother. Res. 2007, 17, 544–552. [Google Scholar] [CrossRef]
- Merkouris, S.S.; Thomas, A.C.; Shandley, K.A.; Rodda, S.N.; Oldenhof, E.; Dowling, N.A. An Update on Gender Differences in the Characteristics Associated with Problem Gambling: A Systematic Review. Curr. Addict. Rep. 2016, 3, 254–267. [Google Scholar] [CrossRef]
- Melville, K.M.; Casey, L.M.; Kavanagh, D. Psychological treatment dropout among pathological gamblers. Clin. Psychol. Rev. 2007, 27, 944–958. [Google Scholar] [CrossRef]
- Pickering, D.; Keen, B.; Entwistle, G.; Blaszczynski, A. Measuring treatment outcomes in gambling disorders: A systematic review. Addiction 2018, 113, 411–426. [Google Scholar] [CrossRef]
- Ribeiro, E.O.; Afonso, N.H.; Morgado, P. Non-pharmacological treatment of gambling disorder: A systematic review of randomized controlled trials. BMC Psychiatry 2021, 21, 105. [Google Scholar] [CrossRef]
- Ekhtiari, H.; Tavakoli, H.; Addolorato, G.; Baeken, C.; Bonci, A.; Campanella, S.; Castelo-Branco, L.; Challet-Bouju, G.; Clark, V.P.; Claus, E.; et al. Transcranial electrical and magnetic stimulation (tES and TMS) for addiction medicine: A consensus paper on the present state of the science and the road ahead. Neurosci. Biobehav. Rev. 2019, 104, 118–140. [Google Scholar] [CrossRef]
- Kennedy, N.I.; Lee, W.H.; Frangou, S. Efficacy of non-invasive brain stimulation on the symptom dimensions of schizophrenia: A meta-analysis of randomized controlled trials. Eur. Psychiatry 2018, 49, 69–77. [Google Scholar] [CrossRef]
- Vergallito, A.; Gallucci, A.; Pisoni, A.; Punzi, M.; Caselli, G.; Ruggiero, G.M.; Sassaroli, S.; Lauro, L.J.R. Effectiveness of noninvasive brain stimulation in the treatment of anxiety disorders: A meta-analysis of sham or behaviour-controlled studies. J. Psychiatry Neurosci. 2021, 46, E592–E614. [Google Scholar] [CrossRef] [PubMed]
- Gao, T.; Du, J.; Tian, S.; Liu, W. A meta-analysis of the effects of non-invasive brain stimulation on obsessive-compulsive disorder. Psychiatry Res. 2022, 312, 114530. [Google Scholar] [CrossRef] [PubMed]
- Razza, L.B.; Palumbo, P.; Moffa, A.H.; Carvalho, A.F.; Solmi, M.; Loo, C.K.; Brunoni, A.R. A systematic review and meta-analysis on the effects of transcranial direct current stimulation in depressive episodes. Depression Anxiety 2020, 37, 594–608. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Classen, J.; Gerloff, C.; Celnik, P.; Wassermann, E.M.; Hallett, M.; Cohen, L.G. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology 1997, 48, 1398–1403. [Google Scholar] [CrossRef]
- Pascual-Leone, A.; Valls-Solé, J.; Wassermann, E.M.; Hallett, M. Responses to rapid-rate transcranial magnetic stimulation of the human motor cortex. Brain 1994, 117, 847–858. [Google Scholar] [CrossRef]
- Fiocchi, S.; Chiaramello, E.; Luzi, L.; Ferrulli, A.; Bonato, M.; Roth, Y.; Zangen, A.; Ravazzani, P.; Parazzini, M. Deep Transcranial Magnetic Stimulation for the Addiction Treatment: Electric Field Distribution Modeling. IEEE J. Electromagn. RF Microwaves Med. Biol. 2018, 2, 242–248. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A.; Paulus, W.; Hummel, F.; Boggio, P.S.; Fregni, F.; et al. Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 2008, 1, 206–223. [Google Scholar] [CrossRef]
- Chen, B.T.; Yau, H.-J.; Hatch, C.; Kusumoto-Yoshida, I.; Cho, S.L.; Hopf, F.W.; Bonci, A. Rescuing cocaine-induced prefrontal cortex hypoactivity prevents compulsive cocaine seeking. Nature 2013, 496, 359–362. [Google Scholar] [CrossRef]
- Uylings, H.B.; Groenewegen, H.J.; Kolb, B. Do rats have a prefrontal cortex? Behav. Brain Res. 2003, 146, 3–17. [Google Scholar] [CrossRef]
- Farovik, A.; Dupont, L.M.; Arce, M.; Eichenbaum, H. Medial prefrontal cortex supports recollection, but not familiarity, in the rat. J. Neurosci. 2008, 28, 13428–13434. [Google Scholar] [CrossRef]
- Papaleo, F.; Yang, F.; Garcia, S.; Chen, J.; Lu, B.; Crawley, J.N.; Weinberger, D.R. Dysbindin-1 modulates prefrontal cortical activity and schizophrenia-like behaviors via dopamine/D2 pathways. Mol. Psychiatry 2012, 17, 85–98. [Google Scholar] [CrossRef] [PubMed]
- Balleine, B.W.; Dickinson, A. Goal-directed instrumental action: Contingency and incentive learning and their cortical substrates. Neuropharmacology 1998, 37, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.J.; Sayette, A.M.; Fiez, A.J. Prefrontal responses to drug cues: A neurocognitive analysis. Nat. Neurosci. 2004, 7, 211–214. [Google Scholar] [CrossRef]
- Rorie, A.E.; Newsome, W.T. A general mechanism for decision-making in the human brain? Trends Cogn. Sci. 2005, 9, 41–43. [Google Scholar] [CrossRef]
- Pettorruso, M.; Miuli, A.; Di Natale, C.; Montemitro, C.; Zoratto, F.; De Risio, L.; D’Andrea, G.; Dannon, P.N.; Martinotti, G.; di Giannantonio, M. Non-invasive brain stimulation targets and approaches to modulate gambling-related decisions: A systematic review. Addict. Behav. 2021, 112, 106657. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, C.A.; Mammis, A. Neuromodulation Therapies for Alcohol Addiction: A Literature Review. Neuromodul. Technol. Neural Interface 2018, 21, 144–148. [Google Scholar] [CrossRef]
- Coles, A.S.; Kozak, K.; George, T.P. A review of brain stimulation methods to treat substance use disorders. Am. J. Addict. 2018, 27, 71–91. [Google Scholar] [CrossRef]
- Luigjes, J.; Segrave, R.; de Joode, N.; Figee, M.; Denys, D. Efficacy of Invasive and Non-Invasive Brain Modulation Interventions for Addiction. Neuropsychol. Rev. 2019, 29, 116–138. [Google Scholar] [CrossRef]
- Rachid, F. Neurostimulation techniques in the treatment of cocaine dependence: A review of the literature. Addict. Behav. 2018, 76, 145–155. [Google Scholar] [CrossRef]
- Mostafavi, S.-A.; Khaleghi, A.; Mohammadi, M.R. Noninvasive brain stimulation in alcohol craving: A systematic review and meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 101, 109938. [Google Scholar] [CrossRef]
- Martinotti, G.; Miuli, A.; Stigliano, G.; Pettorruso, M.; di Giannantonio, M. Transcranial Magnetic Stimulation to treat Substance Use Disorders and Behavioral addictions: The state of the art. J. Ital. Soc. Psychiatry 2021, 7, 40–46. [Google Scholar] [CrossRef]
- Trojak, B.; Sauvaget, A.; Fecteau, S.; Lalanne, L.; Chauvet-Gelinier, J.-C.; Koch, S.; Bulteau, S.; Zullino, D.; Achab, S. Outcome of Non-Invasive Brain Stimulation in Substance Use Disorders: A Review of Randomized Sham-Controlled Clinical Trials. J. Neuropsychiatry 2017, 29, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Gay, A.; Cabe, J.; De Chazeron, I.; Lambert, C.; Defour, M.; Bhoowabul, V.; Charpeaud, T.; Tremey, A.; Llorca, P.-M.; Pereira, B.; et al. Repetitive Transcranial Magnetic Stimulation (rTMS) as a Promising Treatment for Craving in Stimulant Drugs and Behavioral Addiction: A Meta-Analysis. J. Clin. Med. 2022, 11, 624. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Sun, Y.; Ku, Y. Effects of Non-invasive Brain Stimulation on Stimulant Craving in Users of Cocaine, Amphetamine, or Methamphetamine: A Systematic Review and Meta-Analysis. Front. Neurosci. 2019, 13, 1–9. [Google Scholar] [CrossRef]
- Kim, H.J.; Kang, N. Bilateral transcranial direct current stimulation attenuated symptoms of alcohol use disorder: A systematic review and meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 108, 110160. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; Di Lazzaro, V.; Filipović, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.C.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef]
- Fregni, F.; El-Hagrassy, M.M.; Pacheco-Barrios, K.; Carvalho, S.; Leite, J.; Simis, M.; Brunelin, J.; Nakamura-Palacios, E.M.; Marangolo, P.; Venkatasubramanian, G.; et al. Evidence-Based Guidelines and Secondary Meta-Analysis for the Use of Transcranial Direct Current Stimulation in Neurological and Psychiatric Disorders. Int. J. Neuropsychopharmacol. 2021, 24, 256–313. [Google Scholar] [CrossRef]
- Zucchella, C.; Mantovani, E.; Federico, A.; Lugoboni, F.; Tamburin, S. Non-invasive Brain Stimulation for Gambling Disorder: A Systematic Review. Front. Neurosci. 2020, 14, 729. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Minozzi, S.; Cinquini, M.; Gianola, S.; Gonzalez-Lorenzo, M.; Banzi, R. The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application. J. Clin. Epidemiol. 2020, 126, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, R.D.; Hedeker, D.R.; Davis, J.M. Estimation of Effect Size From a Series of Experiments Involving Paired Comparisons. J. Educ. Stat. 1993, 18, 271–279. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Viechtbauer, W.; Cheung, M.W.-L. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef]
- Follmann, D.; Elliott, P.; Suh, I.; Cutler, J. Variance imputation for overviews of clinical trials with continuous response. J. Clin. Epidemiol. 1992, 45, 769–773. [Google Scholar] [CrossRef]
- Galli, G.; Vadillo, M.; Sirota, M.; Feurra, M.; Medvedeva, A. A systematic review and meta-analysis of the effects of transcranial direct current stimulation (tDCS) on episodic memory. Brain Stimul. 2019, 12, 231–241. [Google Scholar] [CrossRef]
- Holgado, D.; Vadillo, M.A.; Sanabria, D. The effects of transcranial direct current stimulation on objective and subjective indexes of exercise performance: A systematic review and meta-analysis. Brain Stimul. 2019, 12, 242–250. [Google Scholar] [CrossRef]
- Zack, M.; Cho, S.S.; Parlee, J.; Jacobs, M.; Li, C.; Boileau, I.; Strafella, A. Effects of High Frequency Repeated Transcranial Magnetic Stimulation and Continuous Theta Burst Stimulation on Gambling Reinforcement, Delay Discounting, and Stroop Interference in Men with Pathological Gambling. Brain Stimul. 2016, 9, 867–875. [Google Scholar] [CrossRef]
- Olkin, I.; Gleser, L. Stochastically dependent effect sizes. Handb. Res. Synth. Meta Anal. 2009, 2, 357–376. [Google Scholar]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-on Guide; Chapman and Hall: London, UK; CRC Press: Boca Raton, FL, USA, 2021. [Google Scholar]
- Field, A.P. Meta-Analysis in Clinical Psychology Research. In The Oxford Handbook of Research Strategies for Clinical Psychology; Comer, J.S., Kendall, P.C., Eds.; Oxford University Press: New York, NY, USA, 2013; p. 31. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- IntHout, J.; Ioannidis, A.J.P.; Rovers, M.; Goeman, J.J. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef]
- Benussi, A.; Alberici, A.; Cantoni, V.; Manenti, R.; Brambilla, M.; Dell’Era, V.; Gazzina, S.; Manes, M.; Cristillo, V.; Padovani, A.; et al. Modulating risky decision-making in Parkinson’s disease by transcranial direct current stimulation. Eur. J. Neurol. 2017, 24, 751–754. [Google Scholar] [CrossRef]
- Kapogiannis, D.; Mooshagian, E.; Campion, P.; Grafman, J.; Zimmermann, T.J.; Ladt, K.C.; Wassermann, E.M. Reward processing abnormalities in Parkinson’s disease. Mov. Disord. 2011, 26, 1451–1457. [Google Scholar] [CrossRef]
- Marras, A.; Gavazzi, G.; Grassi, G.; Rathi, Y.; Mascalchi, M.; Makris, N.; Camprodon, J.A.; Pallanti, S. Abstract #59: Modulating Inhibitory Control Networks in Gambling Disorder with Theta Burst Stimulation. Brain Stimul. 2019, 12, e21. [Google Scholar] [CrossRef]
- Pettorruso, M.; Montemitro, C.; di Giannantonio, M. rTMS and cognitive control in gambling disorder. Brain Stimul. 2019, 12, 532. [Google Scholar] [CrossRef]
- Martinotti, G.; Pettorruso, M. Brain stimulation and gambling disorder: New therapeutic perspectives. J. Behav. Addict. 2018, 7, 111. [Google Scholar]
- Aksu, S.; Soyata, A.; Işçen, P.; Içellioğlu, S.; Saçar, K.; Aşçı, G.; Karamürsel, S. Transcranial direct current stimulation may enhance decision making in gambling disorder: A preliminary double-blind sham-controlled study. Brain Stimul. 2017, 10, 481. [Google Scholar] [CrossRef]
- Hauer, L.; Scarano, G.I.; Brigo, F.; Golaszewski, S.; Lochner, P.; Trinka, E.; Sellner, J.; Nardone, R. Effects of repetitive transcranial magnetic stimulation on nicotine consumption and craving: A systematic review. Psychiatry Res. 2019, 281, 112562. [Google Scholar] [CrossRef]
- Chowdhury, N.S.; Livesey, E.J.; Blaszczynski, A.; Harris, J.A. Motor cortex dysfunction in problem gamblers. Addict. Biol. 2021, 26, e12871. [Google Scholar] [CrossRef]
- Quoilin, C.; Grandjean, J.; Duque, J. Considering Motor Excitability During Action Preparation in Gambling Disorder: A Transcranial Magnetic Stimulation Study. Front. Psychiatry 2020, 11, 639. [Google Scholar] [CrossRef]
- Bouchard, A.E.; Dickler, M.; Renauld, E.; Lenglos, C.; Ferland, F.; Rouillard, C.; Leblond, J.; Fecteau, S. Concurrent transcranial direct current stimulation and resting state functional magnetic resonance imaging in patients with Gambling Disorder. Brain Connect. 2021, 10, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Dickler, M.; Lenglos, C.; Renauld, E.; Ferland, F.; Edden, R.A.; Leblond, J.; Fecteau, S. Online effects of transcranial direct current stimulation on prefrontal metabolites in gambling disorder. Neuropharmacology 2018, 131, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Del Mauro, L.; Vicente, S.S.; Piccitto, N.; Silva, A.; Matoshi, A.; Petronella, R.; Iuris, L.; Inghilleri, D.; Chianese, D.; Cappelletti, L.; et al. Add-on Treatment for Gambling Disorder: Promising Results from a tDCS Study. 2023. Available online: https://osf.io/ufd93/ (accessed on 17 March 2023).
- Soyata, A.Z.; Aksu, S.; Woods, A.J.; Işçen, P.; Saçar, K.T.; Karamürsel, S. Effect of transcranial direct current stimulation on decision making and cognitive flexibility in gambling disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 269, 275–284. [Google Scholar] [CrossRef]
- Martinotti, G.; Lupi, M.; Montemitro, C.; Miuli, A.; Di Natale, C.; Spano, M.C.; Mancini, V.; Lorusso, M.; Stigliano, G.; Tambelli, A.; et al. Transcranial Direct Current Stimulation Reduces Craving in Substance Use Disorders: A Double-blind, Placebo-Controlled Study. J. ECT 2019, 35, 207–211. [Google Scholar] [CrossRef]
- Sauvaget, A.; Bulteau, S.; Guilleux, A.; Leboucher, J.; Pichot, A.; Valrivière, P.; Vanelle, J.M.; Sébille-Rivain, V.; Grall-Bronnec, M. Both active and sham low-frequency rTMS single sessions over the right DLPFC decrease cue-induced cravings among pathological gamblers seeking treatment: A randomized, double-blind, sham-controlled crossover trial. J. Behav. Addict 2018, 7, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Gay, A.; Boutet, C.; Sigaud, T.; Kamgoue, A.; Sevos, J.; Brunelin, J.; Massoubre, C. A single session of repetitive transcranial magnetic stimulation of the prefrontal cortex reduces cue-induced craving in patients with gambling disorder. Eur. Psychiatry 2017, 41, 68–74. [Google Scholar] [CrossRef]
- Cardullo, S.; Perez, L.J.G.; Marconi, L.; Terraneo, A.; Gallimberti, L.; Bonci, A.; Madeo, G. Clinical Improvements in Comorbid Gambling/Cocaine Use Disorder (GD/CUD) Patients Undergoing Repetitive Transcranial Magnetic Stimulation (rTMS). J. Clin. Med. 2019, 8, 768. [Google Scholar] [CrossRef]
- Pettorruso, M.; Martinotti, G.; Montemitro, C.; De Risio, L.; Spagnolo, P.A.; Gallimberti, L.; Fanella, F.; Bonci, A.; Di Giannantonio, M. Brainswitch Study Group Multiple Sessions of High-Frequency Repetitive Transcranial Magnetic Stimulation as a Potential Treatment for Gambling Addiction: A 3-Month, Feasibility Study. Eur. Addict. Res. 2020, 26, 52–56. [Google Scholar] [CrossRef]
- Rosenberg, O.; Klein, L.D.; Dannon, P.N. Deep transcranial magnetic stimulation for the treatment of pathological gambling. Psychiatry Res. 2013, 206, 111–113. [Google Scholar] [CrossRef]
- Salerno, L.; Grassi, E.; Makris, N.; Pallanti, S. A Theta Burst Stimulation on Pre-SMA: Proof-of-Concept of Transcranial Magnetic Stimulation in Gambling Disorder. J. Gambl. Stud. 2022, 38, 1529–1537. [Google Scholar] [CrossRef] [PubMed]
- Antal, A.; Alekseichuk, I.; Bikson, M.; Brockmöller, J.; Brunoni, A.R.; Chen, R.; Cohen, L.G.; Dowthwaite, G.; Ellrich, J.; Flöel, A.; et al. Low intensity transcranial electric stimulation: Safety, ethical, legal regulatory and application guidelines. Clin. Neurophysiol. 2017, 128, 1774–1809. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Antal, A.; Bestmann, S.; Bikson, M.; Brewer, C.; Brockmöller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin. Neurophysiol. 2021, 132, 269–306. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin. Neurophysiol. 2009, 120, 2008–2039. [Google Scholar] [CrossRef]
- Fischman, M.W.; Foltin, R.W. Utility of subjective-effects measurements in assessing abuse liability of drugs in humans. Addiction 1991, 86, 1563–1570. [Google Scholar] [CrossRef]
- Kim, S.W.; Grant, J.E.; Potenza, M.N.; Blanco, C.; Hollander, E. The Gambling Symptom Assessment Scale (G-SAS): A reliability and validity study. Psychiatry Res. 2009, 166, 76–84. [Google Scholar] [CrossRef]
- Pascucci, M.; Pettorruso, M.; Righino, E.; Villella, C.; Ciciarelli, C.; Di Cesare, A.; Chiappini, S.; Testa, R.; Conte, G.; Dannon, P. P-76-Evaluation of an Italian sample of gamblers with dannon ainhold gambling scale: Preliminary study. Eur. Psychiatry 2012, 27, 1. [Google Scholar] [CrossRef]
- Raylu, N.; Oei, T.P.S. The gambling urge scale: Development, confirmatory factor validation, and psychometric properties. Psychol. Addict. Behav. 2004, 18, 100. [Google Scholar] [CrossRef]
- Drummond, D.C.; Phillips, T.S. Alcohol urges in alcohol-dependent drinkers: Further validation of the Alcohol Urge Questionnaire in an untreated community clinical population. Addiction 2002, 97, 1465–1472. [Google Scholar] [CrossRef]
- Young, M.M.; Wohl, M.J.A. The Gambling Craving Scale: Psychometric validation and behavioral outcomes. Psychol. Addict. Behav. 2009, 23, 512–522. [Google Scholar] [CrossRef]
- Schippers, G.M.; Broekman, T.; Buchholz, A.; Koeter, M.W.J.; Brink, W.V.D. Measurements in the Addictions for Triage and Evaluation (MATE): An instrument based on the World Health Organization family of international classifications. Addiction 2010, 105, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Bonfiglio, N.S.; Renati, R.; Agus, M.; Penna, M.P. Validation of a substance craving questionnaire (SCQ) in Italian population. Addict. Behav. Rep. 2019, 9, 100172. [Google Scholar] [CrossRef]
- Weiss, R.D.; Griffin, M.L.; Hufford, C.; Muenz, L.R.; Najavits, L.M.; Jansson, S.B.; Kogan, J.; Thompson, H.J. Early Prediction of Initiation of Abstinence from Cocaine:Use of a Craving Questionnaire. Am. J. Addict. 1997, 6, 224–231. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Hyde, J.; Carr, H.; Kelley, N.; Seneviratne, R.; Reed, C.; Parlatini, V.; Garner, M.; Solmi, M.; Rosson, S.; Cortese, S.; et al. Efficacy of neurostimulation across mental disorders: Systematic review and meta-analysis of 208 randomized controlled trials. Mol. Psychiatry 2022, 27, 2709–2719. [Google Scholar] [CrossRef] [PubMed]
- Tatti, E.; Phillips, A.L.; Paciorek, R.; Romanella, S.M.; Dettore, D.; Di Lorenzo, G.; Ruffini, G.; Rossi, S.; Santarnecchi, E. Boosting psychological change: Combining non-invasive brain stimulation with psychotherapy. Neurosci. Biobehav. Rev. 2022, 142, 104867. [Google Scholar] [CrossRef]
- Dedoncker, J.; Baeken, C.; De Raedt, R.; Vanderhasselt, M.-A. Combined transcranial direct current stimulation and psychological interventions: State of the art and promising perspectives for clinical psychology. Biol. Psychol. 2021, 158, 107991. [Google Scholar] [CrossRef]
- Sathappan, A.V.; Luber, B.M.; Lisanby, S.H. The Dynamic Duo: Combining noninvasive brain stimulation with cognitive interventions. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 89, 347–360. [Google Scholar] [CrossRef]
- Jansen, J.M.; Daams, J.G.; Koeter, M.W.J.; Veltman, D.J.; van den Brink, W.; Goudriaan, A.E. Effects of non-invasive neurostimulation on craving: A meta-analysis. Neurosci. Biobehav. Rev. 2013, 37, 2472–2480. [Google Scholar] [CrossRef]
- Maiti, R.; Mishra, B.R.; Hota, D. Effect of High-Frequency Transcranial Magnetic Stimulation on Craving in Substance Use Disorder: A Meta-Analysis. J. Neuropsychiatry 2017, 29, 160–171. [Google Scholar] [CrossRef]
- Zhang, J.J.Q.; Fong, K.N.K.; Ouyang, R.; Siu, A.M.H.; Kranz, G.S. Effects of repetitive transcranial magnetic stimulation (rTMS) on craving and substance consumption in patients with substance dependence: A systematic review and meta-analysis. Addiction 2019, 114, 2137–2149. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Zilverstand, A.; Gui, W.; Li, H.J.; Zhou, X. Effects of single-session versus multi-session non-invasive brain stimulation on craving and consumption in individuals with drug addiction, eating disorders or obesity: A meta-analysis. Brain Stimul. 2019, 12, 606–618. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Qin, J.; He, Q.; Zou, Z. A meta-analysis of transcranial direct current stimulation on substance and food craving: What effect do modulators have? Front. Psychiatry 2020, 11, 598. [Google Scholar] [CrossRef] [PubMed]
- Gomis-Vicent, E.; Thoma, V.; Turner, J.J.; Hill, K.P.; Pascual-Leone, A. Review: Non-Invasive Brain Stimulation in Behavioral Addictions: Insights from Direct Comparisons With Substance Use Disorders. Am. J. Addict. 2019, 28, 431–454. [Google Scholar] [CrossRef]
- Batista, E.K.; Klauss, J.; Fregni, F.; Nitsche, M.A.; Nakamura-Palacios, E.M. A Randomized Placebo-Controlled Trial of Targeted Prefrontal Cortex Modulation with Bilateral tDCS in Patients with Crack-Cocaine Dependence. Int. J. Neuropsychopharmacol. 2015, 18, pyv066. [Google Scholar] [CrossRef]
- Klauss, J.; Anders, Q.S.; Felippe, L.V.; Nitsche, M.A.; Nakamura-Palacios, E.M. Multiple Sessions of Transcranial Direct Current Stimulation (tDCS) Reduced Craving and Relapses for Alcohol Use: A Randomized Placebo-Controlled Trial in Alcohol Use Disorder. Front. Pharmacol. 2018, 9, 716. [Google Scholar] [CrossRef]
- Boggio, P.S.; Sultani, N.; Fecteau, S.; Merabet, L.; Mecca, T.; Pascual-Leone, A.; Basaglia, A.; Fregni, F. Prefrontal cortex modulation using transcranial DC stimulation reduces alcohol craving: A double-blind, sham-controlled study. Drug Alcohol Depend. 2008, 92, 55–60. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Sampaio-Junior, B.; Moffa, A.H.; Aparício, L.V.; Gordon, P.; Klein, I.; Rios, R.M.; Razza, L.B.; Loo, C.; Padberg, F.; et al. Noninvasive brain stimulation in psychiatric disorders: A primer. Rev. Bras. de Psiquiatr. 2018, 41, 70–81. [Google Scholar] [CrossRef]
- O’reilly, R.C. The What and How of prefrontal cortical organization. Trends Neurosci. 2010, 33, 355–361. [Google Scholar] [CrossRef]
- Banich, M.T. Executive function: The search for an integrated account. Curr. Dir. Psychol. Sci. 2009, 18, 89–94. [Google Scholar] [CrossRef]
- Rodrigo, A.H.; Di Domenico, S.I.; Ayaz, H.; Gulrajani, S.; Lam, J.; Ruocco, A.C. Differentiating functions of the lateral and medial prefrontal cortex in motor response inhibition. Neuroimage 2014, 85, 423–431. [Google Scholar] [CrossRef]
- Schulze, L.; Feffer, K.; Lozano, C.; Giacobbe, P.; Daskalakis, Z.J.; Blumberger, D.M.; Downar, J. Number of pulses or number of sessions? An open-label study of trajectories of improvement for once-vs. twice-daily dorsomedial prefrontal rTMS in major depression. Brain Stimul. 2018, 11, 327–336. [Google Scholar] [CrossRef]
- Roth, Y.; Tendler, A.; Arikan, M.K.; Vidrine, R.; Kent, D.; Muir, O.; MacMillan, C.; Casuto, L.; Grammer, G.; Sauve, W.; et al. Real-world efficacy of deep TMS for obsessive-compulsive disorder: Post-marketing data collected from twenty-two clinical sites. J. Psychiatr. Res. 2021, 137, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, D.; Rajak, B.L.; Gupta, M.; Mukherjee, A. Increasing number of therapy sessions of repetitive transcranial magnetic stimulation improves motor development by reducing muscle spasticity in cerebral palsy children. Ann. Indian Acad. Neurol. 2019, 22, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Teng, S.; Guo, Z.; Peng, H.; Xing, G.; Chen, H.; He, B.; McClure, M.; Mu, Q. High-frequency repetitive transcranial magnetic stimulation over the left DLPFC for major depression: Session-dependent efficacy: A meta-analysis. Eur. Psychiatry 2017, 41, 75–84. [Google Scholar] [CrossRef]
- Vergallito, A.; Riva, P.; Pisoni, A.; Lauro, L.J.R. Modulation of negative emotions through anodal tDCS over the right ventrolateral prefrontal cortex. Neuropsychologia 2018, 119, 128–135. [Google Scholar] [CrossRef]
- Abend, R.; Sar-El, R.; Gonen, T.; Jalon, I.; Vaisvaser, S.; Bar-Haim, Y.; Hendler, T. Modulating Emotional Experience Using Electrical Stimulation of the Medial-Prefrontal Cortex: A Preliminary tDCS-fMRI Study. Neuromodulation Technol. Neural Interface 2019, 22, 884–893. [Google Scholar] [CrossRef]
- Bartley, A.C.; Bloch, M.H. Meta-analysis: Pharmacological treatment of pathological gambling. Expert Rev. Neurother. 2013, 13, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Turi, Z.; Bjørkedal, E.; Gunkel, L.; Antal, A.; Paulus, W.; Mittner, M. Evidence for Cognitive Placebo and Nocebo Effects in Healthy Individuals. Sci. Rep. 2018, 8, 17443. [Google Scholar] [CrossRef]
- Rabipour, S.; Wu, A.D.; Davidson, P.S.; Iacoboni, M. Expectations may influence the effects of transcranial direct current stimulation. Neuropsychologia 2018, 119, 524–534. [Google Scholar] [CrossRef] [PubMed]
- Braga, M.; Barbiani, D.; Andani, M.E.; Villa-Sánchez, B.; Tinazzi, M.; Fiorio, M. The Role of Expectation and Beliefs on the Effects of Non-Invasive Brain Stimulation. Brain Sci. 2021, 11, 1526. [Google Scholar] [CrossRef]
- Chen, X.; Zou, K.; Abdullah, N.; Whiteside, N.; Sarmanova, A.; Doherty, M.; Zhang, W. The placebo effect and its determinants in fibromyalgia: Meta-analysis of randomised controlled trials. Clin. Rheumatol. 2017, 36, 1623–1630. [Google Scholar] [CrossRef]
- Dollfus, S.; Lecardeur, L.; Morello, R.; Etard, O. Placebo Response in Repetitive Transcranial Magnetic Stimulation Trials of Treatment of Auditory Hallucinations in Schizophrenia: A Meta-Analysis. Schizophr. Bull. 2016, 42, 301–308. [Google Scholar] [CrossRef]
- Burke, M.J.; Kaptchuk, T.J.; Pascual-Leone, A. Challenges of differential placebo effects in contemporary medicine: The example of brain stimulation. Ann. Neurol. 2018, 85, 12–20. [Google Scholar] [CrossRef]
- Razza, L.B.; Moffa, A.H.; Moreno, M.L.; Carvalho, A.F.; Padberg, F.; Fregni, F.; Brunoni, A.R. A systematic review and meta-analysis on placebo response to repetitive transcranial magnetic stimulation for depression trials. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 81, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Weatherill, M.; Tibus, E.O.; Rodriguez, A.D. Motivation as a predictor of aphasia treatment outcomes: A scoping review. Top. Lang. Disord. 2022, 42, 252–265. [Google Scholar] [CrossRef] [PubMed]
- Marker, I.; Norton, P.J. The efficacy of incorporating motivational interviewing to cognitive behavior therapy for anxiety disorders: A review and meta-analysis. Clin. Psychol. Rev. 2018, 62, 1–10. [Google Scholar] [CrossRef]
- Wager, T.D.; Atlas, L.Y. The neuroscience of placebo effects: Connecting context, learning and health. Nat. Rev. Neurosci. 2015, 16, 403–418. [Google Scholar] [CrossRef]
- Nower, L.; Blaszczynski, A. Recovery in pathological gambling: An imprecise concept. Subst. Use Misuse 2008, 43, 1844–1864. [Google Scholar] [CrossRef]
- Pisoni, A.; Mattavelli, G.; Papagno, C.; Rosanova, M.; Casali, A.G.; Lauro, L.J.R. Cognitive Enhancement Induced by Anodal tDCS Drives Circuit-Specific Cortical Plasticity. Cereb. Cortex 2018, 28, 1132–1140. [Google Scholar] [CrossRef]
- Romei, V.; Thut, G.; Silvanto, J. Information-Based Approaches of Noninvasive Transcranial Brain Stimulation. Trends Neurosci. 2016, 39, 782–795. [Google Scholar] [CrossRef] [PubMed]
- Wagner, T.; Fregni, F.; Fecteau, S.; Grodzinsky, A.; Zahn, M.; Pascual-Leone, A. Transcranial direct current stimulation: A computer-based human model study. Neuroimage 2007, 35, 1113–1124. [Google Scholar] [CrossRef]
- Bortoletto, M.; Pellicciari, M.C.; Rodella, C.; Miniussi, C. The Interaction With Task-induced Activity is More Important Than Polarization: A tDCS Study. Brain Stimul. 2015, 8, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Silvanto, J.; Bona, S.; Marelli, M.; Cattaneo, Z. On the Mechanisms of Transcranial Magnetic Stimulation (TMS): How Brain State and Baseline Performance Level Determine Behavioral Effects of TMS. Front. Psychol. 2018, 9, 741. [Google Scholar] [CrossRef]
- Silvanto, J.; Muggleton, N.; Walsh, V. State-dependency in brain stimulation studies of perception and cognition. Trends Cogn. Sci. 2008, 12, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Li, L.M.; Violante, I.R.; Leech, R.; Ross, E.; Hampshire, A.; Opitz, A.; Rothwell, J.C.; Carmichael, D.W.; Sharp, D.J. Brain state and polarity dependent modulation of brain networks by transcranial direct current stimulation. Hum. Brain Mapp. 2019, 40, 904–915. [Google Scholar] [CrossRef]
- Lauro, L.J.; Rosanova, M.; Mattavelli, G.; Convento, S.; Pisoni, A.; Opitz, A.; Bolognini, N.; Vallar, G. TDCS increases cortical excitability: Direct evidence from TMS–EEG. Cortex 2014, 58, 99–111. [Google Scholar] [CrossRef]
- Lauro, L.J.R.; Pisoni, A.; Rosanova, M.; Casarotto, S.; Mattavelli, G.; Bolognini, N.; Vallar, G. Localizing the effects of anodal tDCS at the level of cortical sources: A Reply to Bailey et al., 2015. Cortex 2016, 74, 323–328. [Google Scholar] [CrossRef]
- Vergallito, A.; Varoli, E.; Pisoni, A.; Mattavelli, G.; Del Mauro, L.; Feroldi, S.; Vallar, G.; Romero Lauro, L.J. State-dependent effectiveness of cathodal transcranial direct current stimulation on cortical excitability. bioRxiv 2023. [Google Scholar] [CrossRef]
- Varoli, E.; Pisoni, A.; Mattavelli, G.; Vergallito, A.; Gallucci, A.; Mauro, L.D.; Rosanova, M.; Bolognini, N.; Vallar, G.; Lauro, L.J.R. Tracking the Effect of Cathodal Transcranial Direct Current Stimulation on Cortical Excitability and Connectivity by Means of TMS-EEG. Front. Neurosci. 2018, 12, 319. [Google Scholar] [CrossRef]
- Carmi, L.; Tendler, A.; Bystritsky, A.; Hollander, E.; Blumberger, D.M.; Daskalakis, J.; Ward, H.; Lapidus, K.; Goodman, W.; Casuto, L.; et al. Efficacy and Safety of Deep Transcranial Magnetic Stimulation for Obsessive-Compulsive Disorder: A Prospective Multicenter Randomized Double-Blind Placebo-Controlled Trial. Am. J. Psychiatry 2019, 176, 931–938. [Google Scholar] [CrossRef] [PubMed]
- McCalley, D.M.; Kaur, N.; Wolf, J.P.; Contreras, I.E.; Book, S.W.; Smith, J.P.; Hanlon, C.A. Medial Prefrontal Cortex Theta Burst Stimulation Improves Treatment Outcomes in Alcohol Use Disorder: A Double-Blind, Sham-Controlled Neuroimaging Study. Biol. Psychiatry Glob. Open Sci. 2022, 3, 301–310. [Google Scholar] [CrossRef]
- Li, L.M.; Uehara, K.; Hanakawa, T. The contribution of interindividual factors to variability of response in transcranial direct current stimulation studies. Front. Cell. Neurosci. 2015, 9, 181. [Google Scholar] [CrossRef] [PubMed]
- Vergallito, A.; Feroldi, S.; Pisoni, A.; Romero Lauro, L.J. Inter-Individual Variability in tDCS Effects: A Narrative Review on the Contribution of Stable, Variable, and Contextual Factors. Brain Sci. 2022, 12, 522. [Google Scholar] [CrossRef] [PubMed]





| Cochrane Risk of Bias 2 Tool | ||||||
|---|---|---|---|---|---|---|
| References | Randomization Process | Deviations from Intended Interventions | Missing Outcome Data | Outcome Measures | Reported Results Selection | Overall Judgment |
| Gay et al. [102] | Low | Low | Low | Low | Some concerns | Some concerns |
| Martinotti et al. [100] | Some concerns | Low | Low | Low | Some concerns | Some concerns |
| Sauvaget et al. [101] | Some concerns | Low | Low | Low | Some concerns | Some concerns |
| Soyata et al. [99] | Some concerns | Low | Low | Low | Some concerns | Some concerns |
| Zack et al. [81] | Some concerns | Low | Low | Low | Some concerns | Some concerns |
| National Institutes of Health (NIH) Quality Assessment Tool | |
|---|---|
| References | Overall Judgment |
| Cardullo et al. [103] | Fair |
| Del Mauro et al. [98] | Good |
| Pettorruso et al. [104] | Good |
| Rosenberg et al. [105] | Poor |
| Salerno et al. [106] | Fair |
| Authors | Sample | Age (Mean ± SD) | Education (Mean ± SD) | Diagnosis and Criteria | Gambling Preferences (N) | Non-Drug Interventions | Medications |
|---|---|---|---|---|---|---|---|
| Cardullo et al. [103] | 7 (7 M) | 42.1 ± 5.7 | 12 ± 3.2 | CUD comorbidity with GD, DSM-5 criteria | Slot machines (6) Online poker (1) | NR | Stable pharmacological therapy throughout treatment |
| Del Mauro et al. [98] | 18 (16 M) | 41.6 ± 14.8 | 10.8 ± 3.3 | GD, DSM-5 criteria | NR | Psychological and educational support | Nine patients were under stable therapy during treatment |
| Gay et al. [102] | 22 (14 M) | 51 ± 13.7 | 10.9 ± 1.4 | GD, DSM-5 criteria | Slot machines (9) Scratch cards (7) Horserace betting (5) Sports betting (1) | NR | Nine patients were under stable pharmacological therapy before (1 month) and during treatment. |
| Martinotti et al. * [100] | 4 GD/34 total sample | 37.2 ± 10.4 (total sample) | NR | GD—no criteria reported | NR | NR | Twenty-two patients (total sample) were under stable pharmacotherapy |
| Pettorruso et al. [104] | 8 (7 M) | 40.6 ± 11.2 | 13.5 ± 3.1 | GD, DSM-5 criteria | NR | Weekly psychosocial support | Four patients were under stable (6 months) pharmacological treatment. |
| Rosenberg et al. [105] | 5 (5 M) | 37.8 ± 10.3 | 14.8 ± 2.7 | GD, DSM-IV-TR criteria | Internet gambling (1) Slot machines (3) Scratching tickets (1) | None | One patient was under stable pharmacological therapy during the treatment |
| Salerno et al. [106] | 6 (5 M) | 45.7 | NR | GD, DSM-5 criteria | NR | NR | NR |
| Sauvaget et al. * [101] | 30 (27 M) | Range: 28–56 | NR | GD, DSM-IV criteria | Eight participants usually gambled online | NR | Stable (at least 7 days before treatment) |
| Soyata et al. * [99] | 20 (20 M) | 37.2 ± 10.3 | 13.4 ± 3.2 | GD, DSM-5 criteria | NR | NR | NR |
| Zack et al. [81] | 9 (9 M) | 43.2 ± 13.2 | NR | PG, DSM-IV criteria | NR | NR | No medication allowed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Mauro, L.; Vergallito, A.; Gattavara, G.; Juris, L.; Gallucci, A.; Vedani, A.; Cappelletti, L.; Farneti, P.M.; Romero Lauro, L.J. Betting on Non-Invasive Brain Stimulation to Treat Gambling Disorder: A Systematic Review and Meta-Analysis. Brain Sci. 2023, 13, 698. https://doi.org/10.3390/brainsci13040698
Del Mauro L, Vergallito A, Gattavara G, Juris L, Gallucci A, Vedani A, Cappelletti L, Farneti PM, Romero Lauro LJ. Betting on Non-Invasive Brain Stimulation to Treat Gambling Disorder: A Systematic Review and Meta-Analysis. Brain Sciences. 2023; 13(4):698. https://doi.org/10.3390/brainsci13040698
Chicago/Turabian StyleDel Mauro, Lilia, Alessandra Vergallito, Gaia Gattavara, Lucrezia Juris, Alessia Gallucci, Anna Vedani, Laura Cappelletti, Pietro Maria Farneti, and Leonor J. Romero Lauro. 2023. "Betting on Non-Invasive Brain Stimulation to Treat Gambling Disorder: A Systematic Review and Meta-Analysis" Brain Sciences 13, no. 4: 698. https://doi.org/10.3390/brainsci13040698