
Influence of Cannabinoid Treatment on Trajectories of Patient-Related Outcomes in Chronic Pain: Pain Intensity, Emotional Distress, Tolerability and Physical Disability

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Inclusion Criteria
2.2. Data Assessment and Measurement
2.2.1. PROM: Pain Intensity
2.2.2. PROM: Emotional Distress
2.2.3. PROM: Tolerability of Pain
- “Not relevant, I have no pain at all”;
- “I can tolerate may pain well”;
- “I can hardly tolerate my pain”;
- “I am unable to tolerate my pain any longer”.
2.2.4. PROM: Pain-Associated Disability
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Patients
3.2. Cannabinoid Therapy
3.3. Change in the Use of Opioids
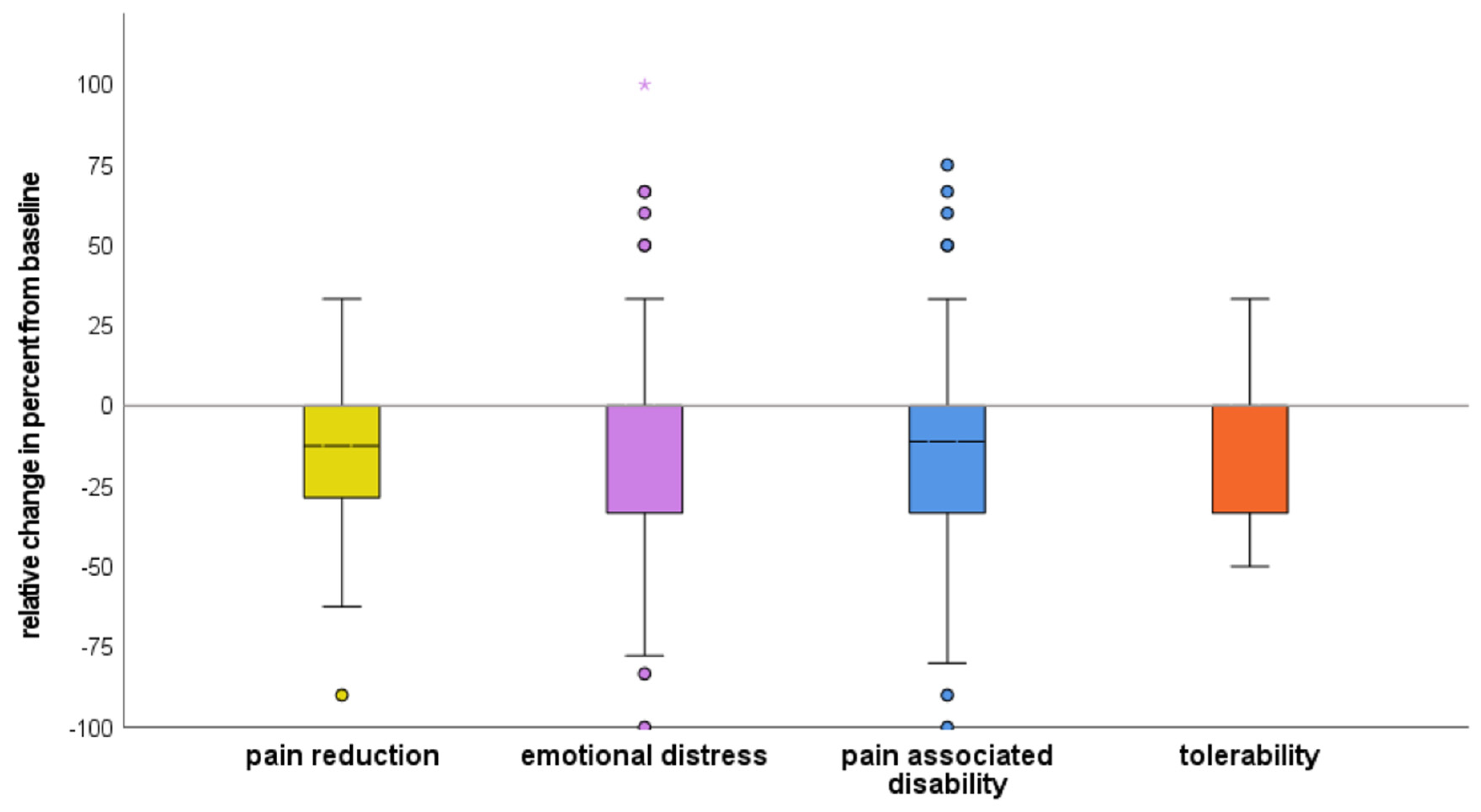
3.4. Reported Effects on Health Status (PROMs)
3.4.1. Pain Intensity
3.4.2. Pain-Associated Disability
3.4.3. Emotional Distress
3.4.4. Tolerability of Pain
3.4.5. Overlap of Responses in the Four PROM Trajectories
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schäfer, M.; Tafelski, S. Cannabis and cannabinoids for the treatment of acute and chronic pain [Cannabis und Cannabinoide zur Therapie akuter und chronischer Schmerzen]. Die Anaesthesiol. 2021, 70, 551–562. [Google Scholar]
- Petzke, F.; Enax-Krumova, E.K.; Häuser, W. Efficacy, tolerability and safety of cannabinoids for chronic neuropathic pain: A systematic review of randomized controlled studies [Wirksamkeit, Verträglichkeit und Sicherheit von Cannabinoiden bei neuropathischen Schmerzsyndromen. Eine systematische Übersichtsarbeit von randomisierten, kontrollierten Studien]. Schmerz 2016, 30, 62–88. [Google Scholar] [PubMed]
- Balestra, A.M.; Chalk, K.; Spies, C.; Denke, C.; Krampe, H.; Tafelski, S. Living with chronic pain during the COVID-19 pandemic: A qualitative analysis. J. Pain Res. 2022, 15, 969–981. [Google Scholar] [CrossRef] [PubMed]
- Pogatzki-Zahn, E.; Schnabel, K.; Kaiser, U. Patient-reported outcome measures for acute and chronic pain: Current knowledge and future directions. Curr. Opin. Anesthesiol. 2019, 32, 616–622. [Google Scholar] [CrossRef]
- Kaiser, U.; Kopkow, C.; Deckert, S.; Sabatowski, R.; Schmitt, J. Validation and application of a core set of patient-relevant outcome domains to assess the effectiveness of multimodal pain therapy (VAPAIN): A study protocol. BMJ Open 2015, 5, e008146. [Google Scholar] [CrossRef]
- Turk, D.C.; Dworkin, R.H.; Allen, R.R.; Bellamy, N.; Brandenburg, N.; Carr, D.B.; Cleeland, C.; Dionne, R.; Farrar, J.T.; Galer, B.S.; et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain 2003, 106, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.D.; MacCallum, C.; Margolese, S.; Walsh, Z.; Wright, P.; Daeninck, P.J.; Mandarino, E.; Lacasse, G.; Kaur Deol, J.; de Freitas, L.; et al. External review panel. Clinical practice guidelines for cannabis and cannabinoid-based medicines in the management of chronic pain and co-occurring conditions. Cannabis Cannabinoid Res. 2023, X, 1–19. [Google Scholar] [CrossRef]
- Mücke, M.; Phillips, T.; Radbruch, L.; Petzke, F.; Häuser, W. Cannabis-based medicines for chronic neuropathic pain in adults. Cochrane Database Syst. Rev. 2018, 3, CD012182. [Google Scholar] [CrossRef]
- Frettlöh, J.; Maier, C.; Gockel, H.; Zenz, M.; Hüppe, M. Characterization of chronic pain patients in German pain centers: Core data from more than 10,000 patients [Patientenkollektiv deutscher schmerztherapeutischer Einrichtungen Kerndaten von mehr als 10.000 Patienten]. Schmerz 2009, 23, 576–591. [Google Scholar] [CrossRef]
- Denecke, H.; Glier, B.; Klinger, R.; Nilges, P.; Redegeld, M.; Weiß, L. Quality assurance in therapy of chronic pain. Results obtained by a taskforce of the German Section of the Association for the Study of Pain on psychological assessment of chronic pain: VI. Instruments for the assessment of disability VII. Psychological instruments for the assessment of pain relevant aspects of social interaction and communication. [Qualitätssicherung in der Therapie chronischen Schmerzes Ergebnisse einer Arbeitsgruppe der DGSS zur psychologischen Diagnostik VI. Verfahren zur Erfassung von Behinderung/Beeinträchtigung VII. Verfahren zur Erfassung schmerzrelevanter interaktioneller Aspekte in Familie und Partnerschaft]. Schmerz 1995, 9, 242–247. [Google Scholar]
- Von Korff, M.; Ormel, J.; Keefe, F.J.; Dworkin, S.F. Grading the severity of chronic pain. Pain 1992, 50, 133–149. [Google Scholar] [CrossRef] [PubMed]
- Arnold, B.; Lutz, J.; Nilges, P.; Pfingsten, M.; Rief, W.; Böger, A.; Brinkschmidt, T.; Casser, H.-R.; Irnich, D.; Kaiser, U.; et al. Chronische Schmerzstörung mit somatischen und psychischen Faktoren (F45.41). Schmerz 2017, 31, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Bilbao, A.; Spanagel, R. Medical cannabinoids: A pharmacology-based systematic review and meta-analysis for all relevant medical indications. BMC Med. 2022, 20, 259. [Google Scholar] [CrossRef]
- Bialas, P.; Fitzcharles, M.A.; Klose, P.; Häuser, W. Long-term observational studies with cannabis-based medicines for chronic non-cancer pain: A systematic review and meta-analysis of effectiveness and safety. Eur. J. Pain 2022, 26, 1221–1233. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on the Health Effects of Marijuana: An Evidence Review and Research Agenda. The National Academies Collection: Reports funded by National Institutes of Health. In The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research; National Academies Press: Washington, DC, USA, 2017. [Google Scholar]
- Boehnke, K.F.; Litinas, E.; Clauw, D.J. Medical cannabis use is associated with decreased opiate medication use in a retrospective cross-sectional survey of patients with chronic pain. J. Pain 2016, 17, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Gastmeier, K.; Gastmeier, A.; Rottmann, F.; Herdegen, T.; Böhm, R. Cannabinoids reduce opioid use in older patients with pain. Retrospective three-year analysis of data from a general practice [Cannabinoide reduzieren den Opioidverbrauch bei älteren Schmerzpatienten]. Schmerz 2022, 37, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Zeraatkar, D.; Cooper, M.A.; Agarwal, A.; Vernooij, R.W.M.; Leung, G.; Loniewski, K.; Dookie, J.E.; Ahmed, M.M.; Hong, B.Y.; Hong, C.; et al. Long-term and serious harms of medical cannabis and cannabinoids for chronic pain: A systematic review of non-randomised studies. BMJ Open 2022, 12, e054282. [Google Scholar] [CrossRef]
- Sestan-Pesa, M.; Shanabrough, M.; Horvath, T.L.; Miletta, M.C. Impaired Ghrelin Signaling does not Lead to Alterations of Anxiety-like Behaviors in Adult Mice Chronically Exposed to THC during Adolescence. Biomedicines 2023, 11, 144. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Ablin, J.; Trabelsi, A.; Fitzcharles, M.A.; Marotto, D.; Häuser, W. Cannabinoids in the treatment of rheumatic diseases: Pros and cons. Autoimmun. Rev. 2019, 18, 102409. [Google Scholar] [CrossRef]
- Kafil, T.S.; Nguyen, T.M.; MacDonald, J.K.; Chande, N. Cannabis for the treatment of Crohn’s disease. Cochrane Database Syst. Rev. 2018, 11, CD012853. [Google Scholar] [CrossRef]
- Starowicz, K.; Finn, D.P. Cannabinoids and pain: Sites and mechanisms of action. Adv. Pharmacol. 2017, 80, 437–475. [Google Scholar] [CrossRef]
- Krebs, E.E.; Carey, T.S.; Weinberger, M. Accuracy of the pain numeric rating scale as a screening test in primary care. J. Gen. Intern. Med. 2007, 22, 1453–1458. [Google Scholar] [CrossRef]
- Schenk, S.; Grothus, S.; Genent, D.; Selent, F.; Zernikow, B.; Wager, J. [Interdisciplinary multimodal inpatient pain treatment for young adults. Influence of autonomy on effectiveness] Interdisziplinäre multimodale stationäre Schmerztherapie für junge Erwachsene. Schmerz 2020, 34, 41–51. [Google Scholar] [CrossRef]
- Elbers, S.; Wittink, H.; Konings, S.; Kaiser, U.; Kleijnen, J.; Pool, J.; Köke, A.; Smeets, R. Longitudinal outcome evaluations of Interdisciplinary Multimodal Pain Treatment programmes for patients with chronic primary musculoskeletal pain: A systematic review and meta-analysis. Eur. J. Pain 2022, 26, 310–335. [Google Scholar] [CrossRef]
- Bigalke, S.; Maeßen, T.V.; Schnabel, K.; Kaiser, U.; Segelcke, D.; Meyer-Friessem, C.H.; Liedgens, H.; Machacek, P.A.; Zahn, P.K.; Pogatzki-Zahn, E.M. Assessing outcome in postoperative pain trials: Are we missing the point? A systematic review of pain-related outcome domains reported in studies early after total knee arthroplasty. Pain 2021, 162, 1914–1934. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N = 64 | |
|---|---|
| Age (years), mean ± standard deviation | 62.1 ± 16.2 |
| Median [25–75% quartiles] | 66 (51–75) |
| Min–max | 22–90 |
| Female sex, N (%) | 30 (47%) |
| Primary indication diagnosis for cannabinoids | |
| Chronic pain with somatic and psychologic factors | 33 (51.6%) |
| Malignancy | 19 (29.7%) |
| Neuropathic pain | 18 (28.1%) |
| Concomitant pharmacologic treatment | |
| Co-analgesics (gabapentinoids, antidepressants) | 43 (67.2%) |
| Opioids | 35 (54.7%) |
| Before Treatment (M ± SD) | Under Treatment (M ± SD) | Relative Reduction | p–Value | |
|---|---|---|---|---|
| Mean pain intensity | 6.7 ± 1.8 | 5.6 ± 2.0 | −14.9 ± 22.6% | <0.001 * |
| Pain-associated disability | 6.9 ± 2.2 | 5.8 ± 2.4 | −9.2 ± 43.5% | <0.001 * |
| Emotional distress | 5.9 ± 2.5 | 5.1 ± 2.6 | −7.0 ± 46.5% | 0.007 * |
| Tolerability of pain | 3.3 ± 0.7 | 2.9 ± 0.8 | −11 ± 23.4% | <0.001 * |
| Variables | p-Value | Exp (B) Odds Ratio | 95% CI for Exp (B) | |
|---|---|---|---|---|
| Lower | Upper | |||
| Patient age | 0.031 * | 1.065 | 1.006 | 1.127 |
| Female sex | 0.407 | 0.498 | 0.096 | 2.585 |
| Cancer pain | 0.948 | 1.059 | 0.189 | 5.934 |
| Neuropathic pain | 0.238 | 3.536 | 0.434 | 28.796 |
| Psychologic comorbidity | 0.185 | 4.212 | 0.501 | 35.385 |
| Duration of chronic pain in months | 0.045 * | 1.025 | 1.001 | 1.051 |
| Concomitant co-analgesic use | 0.335 | 0.442 | 0.084 | 2.321 |
| Concomitant opioid use | 0.458 | 1.884 | 0.354 | 10.018 |
| Cannabinoid type (THC/CBD compound versus THC) | 0.060 | 5.454 | 0.934 | 31.840 |
| Variables | p-Value | Exp (B) Odds Ratio | 95% CI for Exp (B) | |
|---|---|---|---|---|
| Lower | Upper | |||
| Patient age | 0.251 | 1.024 | 0.983 | 1.068 |
| Female sex | 0.144 | 2.989 | 0.688 | 12.983 |
| Cancer pain | 0.877 | 1.122 | 0.262 | 4.802 |
| Neuropathic pain | 0.440 | 0.568 | 0.135 | 2.386 |
| Psychologic comorbidity | 0.151 | 3.834 | 0.612 | 24.014 |
| Duration of chronic pain in months | 0.217 | 1.014 | 0.992 | 1.035 |
| Concomitant co-analgesic use | 0.118 | 0.318 | 0.076 | 1.336 |
| Concomitant opioid use | 0.904 | 1.088 | 0.278 | 4.255 |
| Cannabinoid type (THC/CBD compound versus THC) | 0.008 ** | 9.091 | 1.800 | 45.916 |
| Variables | p-Value | Exp (B) Odds Ratio | 95% CI for Exp (B) | |
|---|---|---|---|---|
| Lower | Upper | |||
| Patient age | 0.212 | 1.028 | 0.984 | 1.074 |
| Female sex | 0.922 | 1.068 | 0.284 | 4.015 |
| Cancer pain | 0.976 | 1.022 | 0.252 | 4.142 |
| Neuropathic pain | 0.111 | 3.778 | 0.736 | 19.390 |
| Psychologic comorbidity | 0.996 | 1.003 | 0.231 | 4.365 |
| Duration of chronic pain in months | 0.207 | 1.013 | 0.993 | 1.033 |
| Concomitant co-analgesic use | 0.326 | 0.512 | 0.135 | 1.948 |
| Concomitant opioid use | 0.160 | 2.589 | 0.687 | 9.759 |
| Cannabinoid type (THC/CBD compound versus THC) | 0.975 | 0.976 | 0.208 | 4.578 |
| Variables | p-Value | Exp (B) Odds Ratio | 95% CI for Exp (B) | |
|---|---|---|---|---|
| Lower | Upper | |||
| Patient age | 0.733 | 1.008 | 0.963 | 1.055 |
| Female sex | 0.835 | 1.164 | 0.278 | 4.873 |
| Cancer pain | 0.063 | 4.410 | 0.924 | 21.036 |
| Neuropathic pain | 0.935 | 0.938 | 0.202 | 4.357 |
| Psychologic comorbidity | 0.368 | 2.158 | 0.404 | 11.516 |
| Duration of chronic pain in months | 0.123 | 1.017 | 0.996 | 1.038 |
| Concomitant co-analgesic use | 0.134 | 3.449 | 0.682 | 17.438 |
| Concomitant opioid use | 0.019 * | 6.297 | 1.347 | 29.264 |
| Cannabinoid type (THC/CBD compound versus THC) | 0.911 | 1.097 | 0.215 | 5.595 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balestra, A.M.; Chalk, K.; Denke, C.; Mohammed, N.; Fritzsche, T.; Tafelski, S. Influence of Cannabinoid Treatment on Trajectories of Patient-Related Outcomes in Chronic Pain: Pain Intensity, Emotional Distress, Tolerability and Physical Disability. Brain Sci. 2023, 13, 680. https://doi.org/10.3390/brainsci13040680
Balestra AM, Chalk K, Denke C, Mohammed N, Fritzsche T, Tafelski S. Influence of Cannabinoid Treatment on Trajectories of Patient-Related Outcomes in Chronic Pain: Pain Intensity, Emotional Distress, Tolerability and Physical Disability. Brain Sciences. 2023; 13(4):680. https://doi.org/10.3390/brainsci13040680
Chicago/Turabian StyleBalestra, Anna Marie, Katharina Chalk, Claudia Denke, Nashwan Mohammed, Thomas Fritzsche, and Sascha Tafelski. 2023. "Influence of Cannabinoid Treatment on Trajectories of Patient-Related Outcomes in Chronic Pain: Pain Intensity, Emotional Distress, Tolerability and Physical Disability" Brain Sciences 13, no. 4: 680. https://doi.org/10.3390/brainsci13040680