
Risk and Adversity Factors in Adult Patients with Comorbid Attention Deficit Hyperactivity Disorder (ADHD), Binge Eating Disorder (BED), and Borderline Personality Disorder (BPD): A Naturalistic Exploratory Study


Abstract
:1. Introduction
1.1. Attention Deficit Hyperactivity Disorder (ADHD)
1.2. Binge Eating Disorder (BED)
1.3. Borderline Personality Disorder (BPD)
1.4. Rationale
2. Objectives
3. Materials and Methods
3.1. Study Design
3.2. Study Setting and Population
3.3. Inclusion and Exclusion Criteria
3.4. Data Collection and Analysis
3.5. Statistical Analysis
4. Results
5. Discussion
Limitations and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Song, P.; Zha, M.; Yang, Q.; Zhang, Y.; Li, X.; Rudan, I. The prevalence of adult attention-deficit hyperactivity disorder: A global systematic review and meta-analysis. J. Glob. Health 2021, 11, 04009. [Google Scholar] [CrossRef] [PubMed]
- Thapar, A.; Cooper, M. Attention deficit hyperactivity disorder. Lancet 2016, 387, 1240–1250. [Google Scholar] [CrossRef] [PubMed]
- Sadek, J. A Clinician’s Guide to Adhd; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Epstein, J.N.; Loren, R.E. Changes in the Definition of ADHD in DSM-5: Subtle but Important. Neuropsychiatry 2013, 3, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Steadman, K.M.; Knouse, L.E. Is the Relationship Between ADHD Symptoms and Binge Eating Mediated by Impulsivity? J. Atten. Disord. 2016, 20, 907–912. [Google Scholar] [CrossRef]
- Giel, K.E.; Bulik, C.M.; Fernandez-Aranda, F.; Hay, P.; Keski-Rahkonen, A.; Schag, K.; Schmidt, U.; Zipfel, S. Binge eating disorder. Nat. Rev. Dis. Prim. 2022, 8, 16. Available online: https://doi-org.ezproxy.library.dal.ca/10.1038/s41572-022-00344-y (accessed on 16 October 2022). [CrossRef] [PubMed]
- Kornstein, S.; Kunovac, J.; Herman, B.; Culpepper, L. Recognizing binge-eating disorder in the clinical setting: A review of the literature. Prim. Care Companion CNS Disord. 2016, 18, 24032. [Google Scholar] [CrossRef]
- Ellison, W.D.; Rosenstein, L.K.; Morgan, T.A.; Zimmerman, M. Community and Clinical Epidemiology of Borderline Personality Disorder. Psychiatr. Clin. N. Am. 2018, 41, 561–573. [Google Scholar] [CrossRef]
- Capusan, A.J.; Yao, S.; Kuja-Halkola, R.; Bulik, C.M.; Thornton, L.M.; Bendtsen, P.; Marteinsdottir, I.; Thorsell, A.; Larsson, H. Genetic and environmental aspects in the association between attention-deficit hyperactivity disorder symptoms and binge-eating behavior in adults: A twin study. Psychol. Med. 2017, 47, 2866–2878. [Google Scholar] [CrossRef]
- Cortese, S.; Bernardina, B.D.; Mouren, M.C. Attention-deficit/hyperactivity disorder (ADHD) and binge eating. Nutr. Rev. 2007, 65, 404–411. [Google Scholar] [CrossRef]
- Hanson, J.; Phillips, L.; Hughes, S.; Corson, K. Attention-deficit hyperactivity disorder symptomatology, binge eating disorder symptomatology, and body mass index among college students. J. Am. Coll. Health 2019, 68, 543–549. [Google Scholar] [CrossRef]
- Nazar, B.P.; Suwwan, R.; de Sousa Pinna, C.M.; Duchesne, M.; Freitas, S.R.; Sergeant, J.; Mattos, P. Influence of attention-deficit/hyperactivity disorder on binge eating behaviors and psychiatric comorbidity profile of obese women. Compr. Psychiatry 2014, 55, 572–578. [Google Scholar] [CrossRef]
- Reinblatt, S.P.; Leoutsakos, J.-M.S.; Mahone, E.M.; Forrester, S.; Wilcox, H.C.; Riddle, M.A. Association between binge eating and attention-deficit/hyperactivity disorder in two pediatric community mental health clinics. Int. J. Eat. Disord. 2015, 48, 505–511. [Google Scholar] [CrossRef]
- Bernardi, S.; Faraone, S.V.; Cortese, S.; Kerridge, B.T.; Pallanti, S.; Wang, S.; Blanco, C. The lifetime impact of attention deficit hyperactivity disorder: Results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Psychol. Med. 2012, 42, 875–887. [Google Scholar] [CrossRef] [PubMed]
- Philipsen, A.; Limberger, M.F.; Lieb, K.; Feige, B.; Kleindienst, N.; Ebner-Priemer, U.; Barth, J.; Schmahl, C.; Bohus, M. Attention-deficit hyperactivity disorder as a potentially aggravating factor in borderline personality disorder. Br. J. Psychiatry 2008, 192, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Sansone, R.A.; Chu, J.W.; Wiederman, M.W.; Lam, C. Eating disorder symptoms and borderline personality symptomatology. Eat. Weight. Disord. 2013, 16, e81–e85. [Google Scholar] [CrossRef] [PubMed]
- Shaker, N.M.; Azzam, L.A.; Zahran, R.M.; Hashem, R.E. Frequency of binge eating behavior in patients with borderline personality disorder and its relation to emotional regulation and impulsivity. Eat. Weight. Disord. 2022, 27, 2497–2506. [Google Scholar] [CrossRef]
- Miller, D.J.; Derefinko, K.J.; Lynam, D.R.; Milich, R.; Fillmore, M.T. Impulsivity and Attention Deficit-Hyperactivity Disorder: Subtype Classification Using the UPPS Impulsive Behavior Scale. J. Psychopathol. Behav. Assess. 2010, 32, 323–332. [Google Scholar] [CrossRef]
- Nazar, B.P.; Bernardes, C.; Peachey, G.; Sergeant, J.; Mattos, P.; Treasure, J. The risk of eating disorders comorbid with attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Int. J. Eat. Disord. 2016, 49, 1045–1057. [Google Scholar] [CrossRef]
- Streeter, B.; Sadek, J. Developmental Risk, Adversity Experiences and ADHD Clinical Profiles: A Naturalistic Exploratory Study. Brain Sci. 2022, 12, 919. [Google Scholar] [CrossRef]
- Rutter, M.; Cox, A.; Tupling, C.; Berger, M.; Yule, W. Attainment and adjustment in two geographical areas. I—The prevalence of psychiatric disorder. Br. J. Psychiatry J. Ment. Sci. 1975, 126, 493–509. [Google Scholar] [CrossRef]
- Banerjee, T.D.; Middleton, F.; Faraone, S.V. Environmental risk factors for attention-deficit hyperactivity disorder. Acta Paediatr. 2007, 96, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Milberger, S.; Faraone, S.V.; Kiely, K.; Guite, J.; Mick, E.; Ablon, S.; Warburton, R.; Reed, E. Family-Environment Risk Factors for Attention-Deficit Hyperactivity Disorder: A Test of Rutter’s Indicators of Adversity. Arch. Gen. Psychiatry 1995, 52, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Famularo, R.; Kinschreff, R.; Fenton, T. Psychiatric Diagnoses of Maltreated Children: Preliminary Findings. J. Am. Acad. Child Adolesc. Psychiatry 1992, 31, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Harold, G.T.; Leve, L.D.; Barrett, D.; Elam, K.; Neiderhiser, J.M.; Natsuaki, M.N.; Shaw, D.S.; Reiss, D.; Thapar, A. Biological and rearing mother influences on child ADHD symptoms: Revisiting the developmental interface between nature and nurture. J. Child Psychol. Psychiatry Allied Discip. 2013, 54, 1038–1046. [Google Scholar] [CrossRef]
- Bozzatello, P.; Garbarini, C.; Rocca, P.; Bellino, S. Borderline Personality Disorder: Risk Factors and Early Detection. Diagnostics 2021, 11, 2142. [Google Scholar] [CrossRef]
- Hilbert, A.; Pike, K.M.; Goldschmidt, A.B.; Wilfley, D.E.; Fairburn, C.G.; Dohm, F.A.; Walsh, B.T.; Striegel Weissman, R. Risk factors across the eating disorders. Psychiatry Res. 2014, 220, 500–506. [Google Scholar] [CrossRef]
- Pike, K.M.; Wilfley, D.; Hilbert, A.; Fairburn, C.G.; Dohm, F.A.; Striegel-Moore, R.H. Antecedent life events of binge-eating disorder. Psychiatry Res. 2006, 142, 19–29. [Google Scholar] [CrossRef]
- Babinski, L.M.; Hartsough, C.S.; Lambert, N.M. Childhood conduct problems, hyperactivity-impulsivity, and inattention as predictors of adult criminal activity. J. Child Psychol. Psychiatry Allied Discip. 1999, 40, 347–355. [Google Scholar] [CrossRef]
- Engelhardt, P.E.; Nobes, G.; Pischedda, S. The Relationship between Adult Symptoms of Attention-Deficit/Hyperactivity Disorder and Criminogenic Cognitions. Brain Sci. 2019, 9, 128. [Google Scholar] [CrossRef]
- Mansoor, M.; Rauf Butt, S.; Satnarine, T.; Ratna, P.; Sarker, A.; Srinivas Ramesh, A.; Munoz Tello, C.; Jamil, D.; Hoang-Vu Tran, H.; Khan, S. The Association between Borderline Personality Disorder and Criminal Activity and Self-harm, Including Suicidal Behavior: A Systematic Review. J. Med. Health Stud. 2022, 3, 08–19. [Google Scholar] [CrossRef]
- Biederman, J.; Mick, E.; Faraone, S.V. Age-dependent decline of symptoms of attention deficit hyperactivity disorder: Impact of remission definition and symptom type. Am. J. Psychiatry 2000, 157, 816–818. [Google Scholar] [CrossRef] [PubMed]
- Mazzeo, S.E.; Bulik, C.M. Environmental and genetic risk factors for eating disorders: What the clinician needs to know. Child Adolesc. Psychiatr. Clin. N. Am. 2009, 18, 67–82. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Study (N = 100) | Control (N = 50) | Comorbidity (N = 50) |
|---|---|---|---|
| Age | |||
| Range | 18–29 | 18–29 | 18–29 |
| Mean | 23.95 | 23.56 | 24.34 |
| SD | 3.36 | 3.30 | 3.42 |
| Education | |||
| <Grade 12 | 5 | 1 | 4 |
| Grade 12 | 49 | 24 | 25 |
| Undergraduate | 43 | 23 | 20 |
| Postgraduate | 3 | 2 | 1 |
| Sex | |||
| Male | 50 | 25 | 25 |
| Female | 50 | 25 | 25 |
| Major Diagnosis | |||
| ADHD | 50 | 50 | 0 |
| ADHD, BPD, BED | 50 | 0 | 50 |
| ADHD Presentation | |||
| Inattentive | 62 | 30 | 32 |
| Hyperactive-impulsive | 22 | 11 | 11 |
| Combined | 7 | 5 | 2 |
| Unspecified | 9 | 4 | 5 |
| Comorbid Disorders | |||
| Generalized anxiety disorder (GAD) | 89 | 39 | 50 |
| Substance use disorder (SUD) | 6 | 1 | 5 |
| Obsessive compulsive disorder (OCD) | 4 | 0 | 4 |
| Major depressive disorder (MDD) | 4 | 2 | 2 |
| Specific learning disorder (SLD) | 1 | 1 | 0 |
| Oppositional defiant disorder (ODD) | 1 | 0 | 1 |
| Tourette syndrome (TS) | 1 | 1 | 0 |
| Gambling addiction | 1 | 0 | 1 |
| Anorexia nervosa (AN) | 1 | 1 | 0 |
| Psychosis | 1 | 0 | 1 |
| Risk Factor | Study (N = 100) | Control (N = 50) | Comorbidity (N = 50) |
|---|---|---|---|
| Bullying | 61 | 22 | 39 |
| Family issues | 50 | 14 | 36 |
| Trouble with the law | 24 | 6 | 18 |
| Complicated birth | 23 | 11 | 12 |
| Poverty | 22 | 4 | 18 |
| Physical abuse | 19 | 4 | 15 |
| Sexual abuse | 16 | 5 | 11 |
| Delayed milestones | 11 | 8 | 3 |
| <Grade 12 education | 5 | 1 | 4 |
| CPT Scoring | Study (N = 100) | Control (N = 100) | Comorbidity (N = 50) |
|---|---|---|---|
| CPT score < 60 | 65 | 34 | 31 |
| Auditory score < 60 | 48 | 23 | 25 |
| Visual score < 60 | 50 | 26 | 24 |
| CPT Scoring | Control (N = 100) | Comorbidity (N = 50) | p-Value |
|---|---|---|---|
| CPT score < 60 | 34 | 31 | 0.529368 |
| Auditory score < 60 | 23 | 25 | 0.688921 |
| Visual score < 60 | 26 | 24 | 0.689157 |
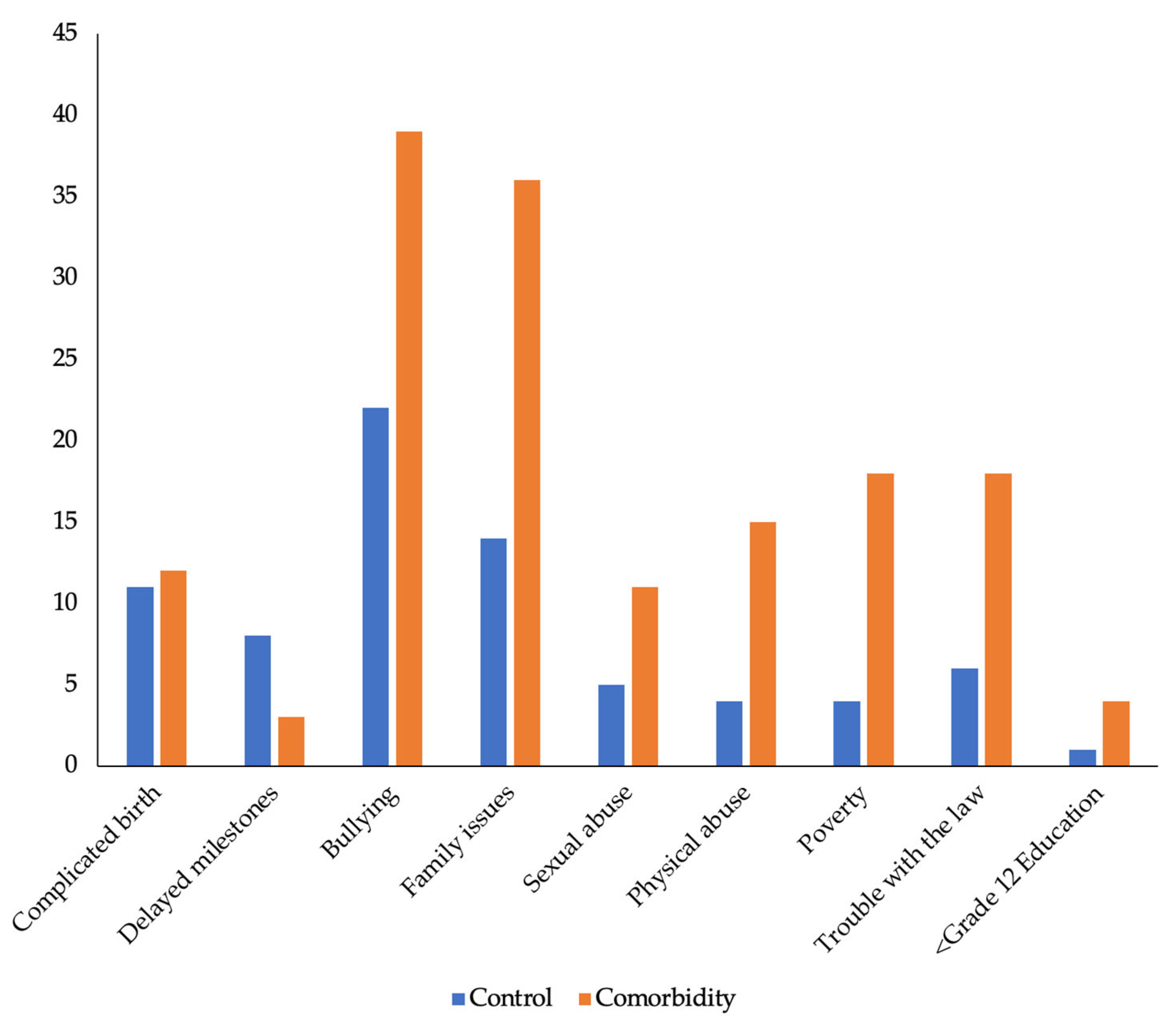
| Risk Factor | Control (N = 50) | Comorbidity (N = 50) | p-Value |
|---|---|---|---|
| Bullying | 22 | 39 | 0.000491 |
| Family issues | 14 | 36 | 0.000011 |
| Trouble with the law | 6 | 18 | 0.004958 |
| Complicated birth | 11 | 12 | 0.812173 |
| Poverty | 4 | 18 | 0.000726 |
| Physical abuse | 4 | 15 | 0.005048 |
| Sexual abuse | 5 | 11 | 0.101707 |
| Delayed milestones | 8 | 3 | 0.110041 |
| <Grade 12 education | 1 | 4 | 0.307434 |
| Overall Risk Factors | Control (N = 50) | Comorbidity (N = 50) | p-Value |
|---|---|---|---|
| </=3 risk factors | 39 | 19 | |
| >/=4 risk factors | 11 | 31 | 0.000051 |
| Statistical Measure | Control (N = 50) Risk Factors | Comorbidities | Comorbidity (N = 50) Risk Factors | Comorbidities |
|---|---|---|---|---|
| Mean | 2.46 | 0.9 | 3.98 | 1.28 |
| SD | 1.29693516 | 0.50507627 | 1.47758766 | 0.57285536 |
| SE | 0.18341433 | 0.20896245 | 0.07142857 | 0.08101398 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryan, D.; Sadek, J. Risk and Adversity Factors in Adult Patients with Comorbid Attention Deficit Hyperactivity Disorder (ADHD), Binge Eating Disorder (BED), and Borderline Personality Disorder (BPD): A Naturalistic Exploratory Study. Brain Sci. 2023, 13, 669. https://doi.org/10.3390/brainsci13040669
Ryan D, Sadek J. Risk and Adversity Factors in Adult Patients with Comorbid Attention Deficit Hyperactivity Disorder (ADHD), Binge Eating Disorder (BED), and Borderline Personality Disorder (BPD): A Naturalistic Exploratory Study. Brain Sciences. 2023; 13(4):669. https://doi.org/10.3390/brainsci13040669
Chicago/Turabian StyleRyan, Derek, and Joseph Sadek. 2023. "Risk and Adversity Factors in Adult Patients with Comorbid Attention Deficit Hyperactivity Disorder (ADHD), Binge Eating Disorder (BED), and Borderline Personality Disorder (BPD): A Naturalistic Exploratory Study" Brain Sciences 13, no. 4: 669. https://doi.org/10.3390/brainsci13040669