
The Role of Decompressive Craniectomy on Functional Outcome, Mortality and Seizure Onset after Traumatic Brain Injury
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
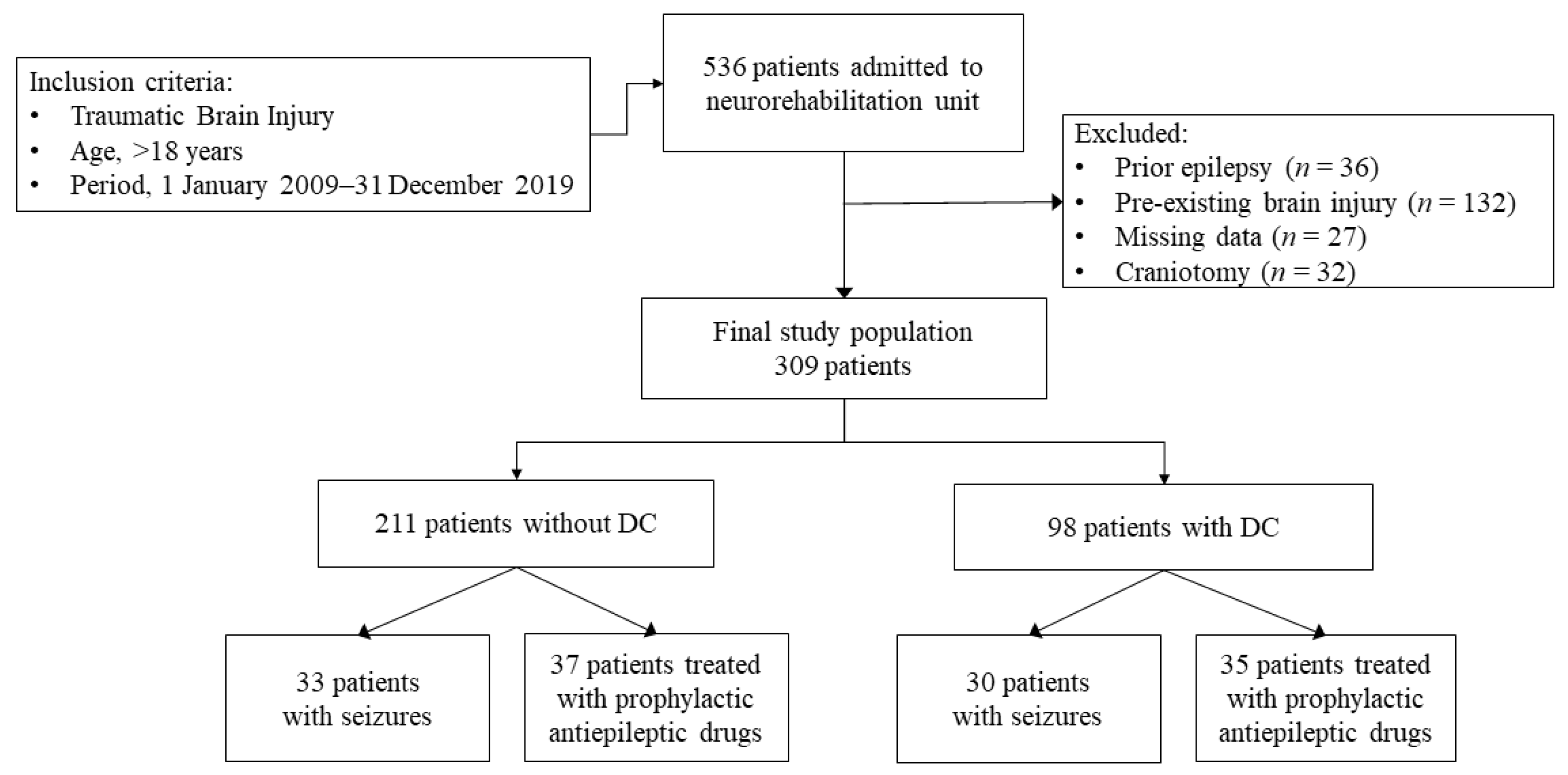
2.1. Study Design and Population
2.2. Variables, Data Sources and Measurements
2.3. Seizures and Antiepileptic Drugs
2.4. Neurological and Functional Assessment
2.5. Statistical Analysis
3. Results
3.1. Clinical and Functional Characteristics
3.2. Functional Outcome
3.3. Mortality
3.4. Seizures and Primary Prophylactic AED Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peeters, W.; van den Brande, R.; Polinder, S.; Brazinova, A.; Steyerberg, E.W.; Lingsma, H.F.; Maas, A.I. Epidemiology of traumatic brain injury in Europe. Acta Neurochir. 2015, 157, 1683–1696. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, R.; Fiest, K.M.; McChesney, J.; Kwon, C.S.; Jette, N.; Frolkis, A.D.; Atta, C.; Mah, S.; Dhaliwal, H.; Reid, A.; et al. The International Incidence of Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Can. J. Neurol. Sci. 2016, 43, 774–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, A.I.; Stocchetti, N.; Bullock, R. Moderate and severe traumatic brain injury in adults. Lancet Neurol. 2008, 7, 728–741. [Google Scholar] [CrossRef]
- Dinet, V.; Petry, K.G.; Badaut, J. Brain-Immune Interactions and Neuroinflammation after Traumatic Brain Injury. Front. Neurosci. 2019, 13, 1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najem, D.; Rennie, K.; Ribecco-Lutkiewicz, M.; Ly, D.; Haukenfrers, J.; Liu, Q.; Nzau, M.; Fraser, D.D.; Bani-Yaghoub, M. Traumatic brain injury: Classification, models, and markers. Biochem. Cell Biol. 2018, 96, 391–406. [Google Scholar] [CrossRef] [PubMed]
- Mele, C.; Pingue, V.; Caputo, M.; Zavattaro, M.; Pagano, L.; Prodam, F.; Nardone, A.; Aimaretti, G.; Marzullo, P. Neuroinflammation and Hypothalamo-Pituitary Dysfunction: Focus of Traumatic Brain Injury. Int. J. Mol. Sci. 2021, 22, 2686. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, J.D.; Hammond, F.M. Traumatic brain injury as a chronic health condition. Arch. Phys. Med. Rehabil. 2013, 94, 1199–1201. [Google Scholar] [CrossRef]
- Jaeger, M.; Soehle, M.; Meixensberger, J. Effects of decompressive craniectomy on brain tissue oxygen in patients with intracranial hypertension. J. Neurol. Neurosurg. Psychiatry 2003, 74, 513–515. [Google Scholar] [CrossRef]
- Hutchinson, P.J.; Kolias, A.G.; Tajsic, T.; Adeleye, A.; Aklilu, A.T.; Apriawan, T.; Bajamal, A.H.; Barthélemy, E.J.; Devi, B.I.; Bhat, D.; et al. Consensus statement from the International Consensus Meeting on the Role of Decompressive Craniectomy in the Management of Traumatic Brain Injury: Consensus statement. Acta Neurochir. 2019, 161, 1261–1274. [Google Scholar] [CrossRef] [Green Version]
- Dujovny, M.; Fernandez, P.; Alperin, N.; Betz, W.; Misra, M.; Mafee, M. Post-cranioplasty cerebrospinal fluid hydrodynamic changes: Magnetic resonance imaging quantitative analysis. Neurol. Res. 1997, 19, 311–316. [Google Scholar] [CrossRef]
- Winkler, P.A.; Stummer, W.; Linke, R.; Krishnan, K.G.; Tatsch, K. Influence of cranioplasty on postural blood flow regulation, cerebrovascular reserve capacity, and cerebral glucose metabolism. J. Neurosurg. 2000, 93, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Jasey, N.; Ward, I.; Lequerica, A.; Chiaravalloti, N.D. The therapeutic value of cranioplasty in individuals with brain injury. Brain Inj. 2018, 32, 318–324. [Google Scholar] [CrossRef]
- Huang, Y.H.; Liao, C.C.; Chen, W.F.; Ou, C.Y. Characterization of acute post-craniectomy seizures in traumatically brain-injured patients. Seizure 2015, 25, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.F.; Wen, L.; Shen, F.; Li, G.; Lou, R.; Liu, W.G.; Zhan, R.Y. Surgical complications secondary to decompressive craniectomy in patients with a head injury: A series of 108 consecutive cases. Acta Neurochir. 2008, 150, 1241–1247. [Google Scholar] [CrossRef]
- Honeybul, S.; Ho, K.M. Long-term complications of decompressive craniectomy for head injury. J. Neurotrauma 2011, 28, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Hunt, R.F.; Boychuk, J.A.; Smith, B.N. Neural circuit mechanisms of post-traumatic epilepsy. Front. Cell Neurosci. 2013, 18, 7:89. [Google Scholar] [CrossRef] [Green Version]
- Fisher, R.S.; Acevedo, C.; Arzimanoglou, A.; Bogacz, A.; Cross, J.H.; Elger, C.E.; Engel JJr Forsgren, L.; French, J.A.; Glynn, M.; Hesdorffer, D.C.; et al. ILAE official report: A practical clinical definition of epilepsy. Epilepsia 2014, 55, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fordington, S.; Manford, M. A review of seizures and epilepsy following traumatic brain injury. J. Neurol. 2020, 267, 3105–3111. [Google Scholar] [CrossRef] [PubMed]
- Christensen, J.; Pedersen, M.G.; Pedersen, C.B.; Sidenius, P.; Olsen, J.; Vestergaard, M. Long-term risk of epilepsy after traumatic brain injury in children and young adults: A population-based cohort study. Lancet 2009, 373, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Krumholz, A.; Shinnar, S.; French, J.; Gronseth, G.; Wiebe, S. Evidence-based guideline: Management of an unprovoked first seizure in adults: Report of the Guideline Development Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology 2015, 85, 1526–1527. [Google Scholar] [CrossRef] [Green Version]
- Holtkamp, M.; Beghi, E.; Benninger, F.; Kälviäinen, R.; Rocamora, R.; Christensen, H.; European Stroke Organisation. European Stroke Organisation guidelines for the management of post-stroke seizures and epilepsy. Eur. Stroke J. 2017, 2, 103–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowe, A.S.; Goodwin, H.; Brophy, G.M.; Bushwitz, J.; Castle, A.; Deen, D.; Johnson, D.; Lesch, C.; Liang, N.; Potter, E.; et al. Seizure prophylaxis in neurocritical care: A review of evidence-based support. Pharmacotherapy 2014, 34, 396–409. [Google Scholar] [CrossRef]
- Moavero, R.; Santarone, M.E.; Galasso, C.; Curatolo, P. Cognitive and behavioral effects of new antiepileptic drugs in pediatric epilepsy. Brain Dev. 2017, 39, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Devinsky, O.; Vezzani, A.; O’Brien, T.J.; Jette, N.; Scheffer, I.E.; de Curtis, M.; Perucca, P. Epilepsy. Nat. Rev. Dis. Primers 2018, 4, 18024. [Google Scholar] [CrossRef]
- Steinhoff, B.J.; Klein, P.; Klitgaard, H.; Laloyaux, C.; Moseley, B.D.; Ricchetti-Masterson, K.; Rosenow, F.; Sirven, J.I.; Smith, B.; Stern, J.M.; et al. Behavioral adverse events with brivaracetam, levetiracetam, perampanel, and topiramate: A systematic review. Epilepsy Behav. 2021, 118, 107939. [Google Scholar] [CrossRef]
- Miziak, B.; Borowicz-Reutt, K.; Rola, R.; Blaszczyk, B.; Czuczwar, M.; Czuczwar, S.J. The Prophylactic Use of Antiepileptic Drugs in Patients Scheduled for Neurosurgery. Curr. Pharm. Des. 2017, 23, 6411–6427. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, V.; Dahlin, R.; Hariri, O.; Quadri, S.A.; Farr, S.; Miulli, D.; Siddiqi, J. Anti-epileptic prophylaxis in traumatic brain injury: A retrospective analysis of patients undergoing craniotomy versus decompressive craniectomy. Surg. Neurol. Int. 2015, 6, 8. [Google Scholar] [PubMed]
- Marshall, L.F.; Marshall, S.B.; Klauber, M.R.; Clark, M.V.B.; Eisenberg, H.M.; Jane, J.A.; Luerssen, T.G.; Marmarou, A.; Foulkes, M.A. A new classification of head injury based on computerized tomography. J. Neurosurg. 1991, 75, S14–S20. [Google Scholar] [CrossRef] [Green Version]
- Kanner, A.M.; Ashman, E.; Gloss, D.; Harden, C.; Bourgeois, B.; Bautista, J.F.; Abou-Khalil, B.; Burakgazi-Dalkilic, E.; Park, E.L.; Stem, J.; et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy: Report of the American Epilepsy Society and the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Epilepsy Curr. 2018, 18, 260–268. [Google Scholar] [PubMed]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the Functional Independence Measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Mackintosh, S. Functional independence measure. Aust. J. Physiother. 2009, 55, 65. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, A.W.; Linacre, J.M.; Wright, B.D.; Hamilton, B.B.; Granger, C. Relationships between impairment and physical disability as measured by the functional independence measure. Arch. Phys. Med. Rehabil. 1993, 74, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Wieloch, T.; Nikolich, K. Mechanisms of neural plasticity following brain injury. Curr. Opin. Neurobiol. 2006, 16, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Hawryluk, G.W.J.; Rubiano, A.M.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kisoon, N.; Shutter, L.; et al. Guidelines for the Management of Severe Traumatic Brain Injury: 2020 Update of the Decompressive Craniectomy Recommendations. Neurosurgery 2020, 87, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Tsoucalas, G.; Kousoulis, A.A.; Mariolis-Sapsakos, T.; Sgantzos, M. Trepanation practices in asclepieia: Systematizing a neurosurgical innovation. World Neurosurg. 2017, 103, 501–503. [Google Scholar] [CrossRef] [PubMed]
- MRC CRASH Trial Collaborators; Perel, P.; Arango, M.; Clayton, T.; Edwards, P.; Komolafe, E.; Poccock, S.; Roberts, I.; Shakur, H.; Steyerberg, E.; et al. Predicting outcome after traumatic brain injury: Practical prognostic models based on large cohort of international patients. BMJ 2008, 336, 425–429. [Google Scholar] [PubMed] [Green Version]
- Cooper, D.J.; Rosenfeld, J.V.; Murray, L.; Arabi, Y.M.; Davies, A.R.; Ponsford, J.; Seppelt, I.; Reilly, P.; Wiegers, E.; Wolfe, R.; et al. Patient Outcomes at Twelve Months after Early Decompressive Craniectomy for Diffuse Traumatic Brain Injury in the Randomized DECRA Clinical Trial. J. Neurotrauma 2020, 37, 810–816. [Google Scholar] [CrossRef] [Green Version]
- Hutchinson, P.J.; Kolias, A.G.; Timofeev, I.S.; Corteen, E.A.; Czosnyka, M.; Timothy, J.; Anderson, I.; Bulters, D.O.; Belli, A.; Eynon, A.; et al. Trial of decompressive craniectomy for traumatic intracranial hypertension. N. Engl. J. Med. 2016, 375, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- Cooper, D.J.; Rosenfeld, J.V.; Murray, L.; Arabi, Y.M.; Davies, A.R.; D’Urso, P.; Kossmann, T.; Ponsford, J.; Seppelt, I.; Reilly, P.; et al. Decompressive craniectomy in diffuse traumatic brain injury. N. Engl. J. Med. 2011, 364, 1493–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, R.F.; Magnotti, L.J.; Croce, M.A.; Hargraves, B.B.; Fischer, P.E.; Schroeppel, T.J.; Zarzaur, B.L.; Muhlbauer, M.; Timmons, S.D.; Fabian, T.C. Impact of decompressive craniectomy on functional outcome after severe traumatic brain injury. J Trauma 2009, 66, 1570–1576. [Google Scholar] [CrossRef] [PubMed]
- Shlosberg, D.; Benifla, M.; Kaufer, D.; Friedman, A. Blood-brain barrier breakdown as a therapeutic target in traumatic brain injury. Nat. Rev. Neurol. 2010, 6, 393–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitkänen, A.; O’Brien, T.J.; Staba, R. Preface—Practical and theoretical considerations for performing a multi-center preclinical biomarker discovery study of post-traumatic epileptogenesis: Lessons learned from the EpiBioS4Rx consortium. Epilepsy Res. 2019, 156, 106080. [Google Scholar] [CrossRef] [PubMed]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery 2017, 80, 6–15. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Whole Population (n = 309) | DC | p | ||
|---|---|---|---|---|---|
| No (n = 211, 68.3%) | Yes (n = 98, 31.7%) | ||||
| n (%) | n (%) | n (%) | |||
| Age (years) | ≤65 | 183 (59.2) | 126 (59.7) | 57 (58.2) | 0.805 |
| >65 | 126 (40.8) | 85 (40.3) | 41 (41.8) | ||
| Sex | Male | 242 (78.3) | 171 (81.0) | 71 (72.4) | 0.103 |
| Female | 67 (21.7) | 40 (20.0) | 27 (27.6) | ||
| Subarachnoid hemorrhage | 121 (39.1) | 88 (41.8) | 33 (33.7) | 0.060 | |
| Cerebral edema | 53 (17.6) | 34 (16.11) | 19 (19.4) | 0.517 | |
| Intraparenchymal hematoma | 172 (55.7) | 99 (46.9) | 73 (74.5) | <0.0001 | |
| Extracranial traumatic complications | 183 (59.2) | 118 (55.9) | 65 (66.3) | 0.106 | |
| Patients with seizures | 63 (20.4) | 33 (15.6) | 30 (30.6) | 0.016 | |
| Type of seizures | ASS | 22 (7.1) | 14 (6.6) | 8 (8.2) | 0.894 |
| US | 32 (10.4) | 15 (7.1) | 17 (17.3) | 0.018 | |
| ASS + US | 9 (2.9) | 4 (1.9) | 5 (5.1) | 0.047 | |
| Prophylaxis with AEDs | I generation | 17 (5.5) | 9 (4.3) | 8 (8.7) | 0.183 |
| II generation | 55 (17.8) | 28 (13.3) | 27 (27.6) | 0.003 | |
| Adapted Marshall classification (Data available for 289 patients) | Diffuse injury I | 97 (31.4) | 91 (43.1) | 1 (1.0) | <0.0001 |
| Diffuse injury II | 53 (17.1) | 48 (22.7) | 2 (2.0) | <0.0001 | |
| Diffuse injury III (swelling) | 61 (19.7) | 44 (20.8) | 17 (17.3) | 0.540 | |
| Diffuse injury IV (shift) | 78 (25.2) | 10 (4.7) | 68 (69.4) | <0.0001 | |
| Evacuated lesion | 0 (0.0) | 0 (0.0) | 8 (8.2) | <0.0001 | |
| Non evacuated lesion | 0 (0.0) | 0 (0.0) | 0 (0.0) | n.a. | |
| GCSoA (Data available for 247 patients) | Mild | 28 (11.3) | 24 (15.1) | 4 (4.5) | 0.011 |
| Moderate | 53 (21.5) | 39 (24.5) | 14 (15.9) | 0.145 | |
| Severe | 166 (67.2) | 96 (60.4) | 70 (79.5) | 0.002 | |
| GCS T0 | Mild | 113 (36.5) | 91 (43.1) | 22 (22.5) | <0.0001 |
| Moderate | 126 (40.8) | 88 (41.8) | 38 (38.8) | 0.488 | |
| Severe | 70 (22.6) | 31 (14.7) | 39 (39.8) | <0.0001 | |
| GCS T1 | Mild | 200 (74.4) | 158 (81.9) | 42 (55.3) | <0.0001 |
| Moderate | 41 (15.2) | 23 (11.9) | 18 (23.7) | 0.02 | |
| Severe | 28 (10.4) | 12 (6.2) | 16 (21.0) | 0.0003 | |
| FIM T0 (median (IQR)) total score | 19 (18–56) | 26 (18–65) | 18 (18–22) | 0.001 | |
| FIM T1 (median (IQR)) total score | 82 (23–117) | 104 (40–122) | 28 (18–91) | <0.0001 | |
| Mortality within 6 months | 41 (13.3) | 18 (8.5) | 23 (23.5) | 0.026 | |
| Regression Model | FIM T1 (R2 = 0.542) | ΔFIM (R2 = 0.250) | ||
|---|---|---|---|---|
| Independent Variables | Beta | p-Value | Beta | p-Value |
| Sex (M = 0, F = 1) | 0.06 | 0.306 | 0.07 | 0.296 |
| Age >65 years | −0.13 | 0.030 | −0.17 | 0.028 |
| Adapted Marshall classification | −0.14 | 0.055 | −0.20 | 0.031 |
| Glasgow Coma Scale on arrival (mild = 1, moderate = 2, severe = 3) | −0.06 | 0.340 | −0.08 | 0.319 |
| Glasgow Coma Scale on admission (mild = 1, moderate = 2, severe = 3) | −0.25 | 0.002 | −0.30 | 0.003 |
| FIM total score on admission | 0.37 | <0.0001 | −0.36 | <0.0001 |
| Extracranial traumatic complications | −0.04 | 0.526 | −0.07 | 0.360 |
| Decompressive craniectomy | −0.08 | 0.262 | −0.09 | 0.310 |
| Acute symptomatic seizures | −0.06 | 0.286 | −0.07 | 0.310 |
| Unprovoked seizures | −0.14 | 0.020 | −0.20 | 0.007 |
| I generation prophylactic AEDs | −0.01 | 0.855 | −0.01 | 0.857 |
| II generation prophylactic AEDs | −0.01 | 0.832 | −0.02 | 0.784 |
| Regression Model | Death during Rehabilitation (Dependent Variable) (No = 0, Yes = 1) | ||
|---|---|---|---|
| Independent Variables | OR | 95% CI | p-Value |
| Sex (M = 0, F = 1) | 0.904 | 0.345–2.634 | 0.836 |
| Age >65 years | 6.185 | 2.464–15.526 | <0.0001 |
| Adapted Marshall classification | 1.258 | 0.787–2.013 | 0.338 |
| GCS on arrival (mild = 1, moderate = 2, severe = 3) | 0.804 | 0.399–1.622 | 0.543 |
| GCS on admission (mild = 0, moderate = 1, severe = 2) | 2.648 | 1.360–5.155 | 0.004 |
| Extracranial traumatic complications | 0.626 | 0.249–1.572 | 0.319 |
| Decompressive craniectomy | 2.046 | 0.663–6.311 | 0.213 |
| Acute symptomatic seizures | 0.721 | 0.157–3.319 | 0.674 |
| Unprovoked seizures | 0.502 | 0.148–1.700 | 0.268 |
| Prophylaxis with AEDs | 0.611 | 0.232–1.612 | 0.320 |
| Regression Model | Acute Symptomatic Seizure | Unprovoked Seizures | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Values | OR | 95% CI | p Values | |
| Sex (M = 0, F = 1) | 1.098 | 0.402–3.000 | 0.855 | 0.778 | 0.296–2.040 | 0.609 |
| Age >65 years | 1.235 | 0.493–3.090 | 0.652 | 0.872 | 0.381–1.995 | 0.746 |
| Adapted Marshall classification | 1.203 | 0.769–1.882 | 0.419 | 0.922 | 0.623–1.365 | 0.686 |
| GCS on arrival (mild = 0, moderate = 1, severe = 2) | 1.071 | 0.539–2.128 | 0.844 | 0.742 | 0.397–1.389 | 0.351 |
| GCS on admission (mild = 0, moderate = 1, severe = 2) | 0.836 | 0.458–1.526 | 0.559 | 1.486 | 0.851–2.595 | 0.164 |
| Decompressive craniectomy | 1.594 | 0.511–4.977 | 0.422 | 3.431 | 1.233–9.542 | 0.018 |
| ASS | n.a. | n.a. | n.a. | 3.204 | 1.176–8.734 | 0.023 |
| Prophylaxis with AEDs | 0.392 | 0.090–1.154 | 0.082 | 0.907 | 0.373–2.205 | 0.830 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pingue, V.; Boetto, V.; Bassetto, A.; Nava, M.; Nardone, A.; Mele, C. The Role of Decompressive Craniectomy on Functional Outcome, Mortality and Seizure Onset after Traumatic Brain Injury. Brain Sci. 2023, 13, 581. https://doi.org/10.3390/brainsci13040581
Pingue V, Boetto V, Bassetto A, Nava M, Nardone A, Mele C. The Role of Decompressive Craniectomy on Functional Outcome, Mortality and Seizure Onset after Traumatic Brain Injury. Brain Sciences. 2023; 13(4):581. https://doi.org/10.3390/brainsci13040581
Chicago/Turabian StylePingue, Valeria, Valentina Boetto, Anna Bassetto, Maruska Nava, Antonio Nardone, and Chiara Mele. 2023. "The Role of Decompressive Craniectomy on Functional Outcome, Mortality and Seizure Onset after Traumatic Brain Injury" Brain Sciences 13, no. 4: 581. https://doi.org/10.3390/brainsci13040581