
Correlation between Blood Type 0 and Risk of Chronic Subdural Hematoma Recurrence: A Single Center Retrospective Cohort Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Inclusion Criteria
2.2. Surgical Procedure
2.3. Radiological Evaluation
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics and Demographic Data
3.2. Patient-Related and Disease-Related Factors Associated with Recurrence of cSDH
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adhiyaman, V.; Chattopadhyay, I.; Irshad, F.; Curran, D.; Abraham, S. Increasing incidence of chronic subdural haematoma in the elderly. QJM 2017, 110, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Rauhala, M.; Helén, P.; Huhtala, H.; Heikkilä, P.; Iverson, G.L.; Niskakangas, T.; Öhman, J.; Luoto, T.M. Chronic subdural hematoma-incidence, complications, and financial impact. Acta Neurochir. 2020, 162, 2033–2043. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.I.; Balser, D.S.; Mikheev, A.; Offen, S.; Huang, J.H.; Babb, J.; Rusinek, H.; Samadani, U. Cerebral atrophy is associated with development of chronic subdural haematoma. Brain Inj. 2012, 26, 1731–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aspegren, O.P.; Åstrand, R.; Lundgren, M.I.; Romner, B. Anticoagulation therapy a risk factor for the development of chronic subdural hematoma. Clin. Neurol. Neurosurg. 2013, 115, 981–984. [Google Scholar] [CrossRef]
- Bartek, J.; Sjåvik, K.; Dhawan, S.; Sagberg, L.M.; Kristiansson, H.; Ståhl, F.; Förander, P.; Chen, C.C.; Jakola, A.S. Clinical Course in Chronic Subdural Hematoma Patients Aged 18–49 Compared to Patients 50 Years and Above: A Multicenter Study and Meta-Analysis. Front. Neurol. 2019, 10, 311. [Google Scholar] [CrossRef] [Green Version]
- Gökmen, M.; Sucu, H.K.; Ergin, A.; Gökmen, A.; Bezircio Lu, H. Randomized comparative study of burr-hole craniostomy versus twist drill craniostomy; surgical management of unilateral hemispheric chronic subdural hematomas. Zentralbl. Neurochir. 2008, 69, 129–133. [Google Scholar] [CrossRef]
- Hirai, S.; Yagi, K.; Hara, K.; Kanda, E.; Matsubara, S.; Uno, M. Postoperative recurrence of chronic subdural hematoma is more frequent in patients with blood type A. J. Neurosurg. 2021, 135, 1203–1207. [Google Scholar] [CrossRef]
- Dubinski, D.; Won, S.-Y.; Behmanesh, B.; Kashefiolasl, S.; Geisen, C.; Seifert, V.; Senft, C.; Konczalla, J. Influence of ABO blood type on the outcome after non-aneurysmal subarachnoid hemorrhage. Acta Neurochir. 2018, 160, 761–766. [Google Scholar] [CrossRef]
- Dubinski, D.; Won, S.-Y.; Behmanesh, B.; Brawanski, N.; Geisen, C.; Seifert, V.; Senft, C.; Konczalla, J. The clinical relevance of ABO blood type in 100 patients with acute subdural hematoma. PLoS ONE 2018, 13, e0204331. [Google Scholar] [CrossRef]
- Ward, S.E.; O’Sullivan, J.M.; O’Donnell, J.S. The relationship between ABO blood group, von Willebrand factor, and primary hemostasis. Blood 2020, 136, 2864–2874. [Google Scholar] [CrossRef]
- Preston, A.E.; Barr, A. The plasma concentration of factor VIII in the normal population. II. The effects of age, sex and blood group. Br. J. Haematol. 1964, 10, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Mehic, D.; Hofer, S.; Jungbauer, C.; Kaider, A.; Haslacher, H.; Eigenbauer, E.; Rejtő, J.; Schwartz, D.; Jilma, B.; Ay, C.; et al. Association of ABO blood group with bleeding severity in patients with bleeding of unknown cause. Blood Adv. 2020, 4, 5157–5164. [Google Scholar] [CrossRef] [PubMed]
- Toi, H.; Kinoshita, K.; Hirai, S.; Takai, H.; Hara, K.; Matsushita, N.; Matsubara, S.; Otani, M.; Muramatsu, K.; Matsuda, S.; et al. Present epidemiology of chronic subdural hematoma in Japan: Analysis of 63,358 cases recorded in a national administrative database. J. Neurosurg. 2018, 128, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Xin, W.; Li, Q.; Gao, Y.; Zhang, J. A Grading System For The Prediction Of Unilateral Chronic Subdural Hematoma Recurrence After Initial Single Burr Hole Evacuation. Risk Manag. Healthc. Policy 2019, 12, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osuka, K.; Ohmichi, Y.; Ohmichi, M.; Nakura, T.; Iwami, K.; Watanabe, Y.; Miyachi, S. Sequential Expression of Chemokines in Chronic Subdural Hematoma Fluids after Trepanation Surgery. J. Neurotrauma 2021, 38, 1979–1987. [Google Scholar] [CrossRef]
- Quan, W.; Zhang, Z.; Tian, Q.; Wen, X.; Yu, P.; Wang, D.; Cui, W.; Zhou, L.; Park, E.; Baker, A.J.; et al. A rat model of chronic subdural hematoma: Insight into mechanisms of revascularization and inflammation. Brain Res. 2015, 1625, 84–96. [Google Scholar] [CrossRef]
- Moeller, A.; Weippert-Kretschmer, M.; Prinz, H.; Kretschmer, V. Influence of ABO blood groups on primary hemostasis. Transfusion 2001, 41, 56–60. [Google Scholar] [CrossRef]
- Franchini, M.; Crestani, S.; Rossi, C.; Frattini, F.; Mengoli, C.; Giacomini, I.; Luppi, M.; Bonfanti, C. O blood group and the risk of major bleeding: A single-center survey. J. Thromb. Thrombolysis 2013, 35, 65–66. [Google Scholar] [CrossRef]
- Dentali, F.; Pomero, F.; Annoni, F.; Giraudo, A.V.; Maresca, A.M.; Fenoglio, L.; Franchini, M.; Bono, G. Role of ABO blood group as a prognostic factor in patients with spontaneous intracerebral hemorrhage. J. Thromb. Haemost. 2013, 11, 187–189. [Google Scholar] [CrossRef]
- Hamou, H.; Alzaiyani, M.; Pjontek, R.; Kremer, B.; Albanna, W.; Ridwan, H.; Clusmann, H.; Hoellig, A.; Veldeman, M. Risk factors of recurrence in chronic subdural hematoma and a proposed extended classification of internal architecture as a predictor of recurrence. Neurosurg. Rev. 2022, 45, 2777–2786. [Google Scholar] [CrossRef]
- Gazzeri, R.; Laszlo, A.; Faiola, A.; Colangeli, M.; Comberiati, A.; Bolognini, A.; Callovini, G. Clinical investigation of chronic subdural hematoma: Relationship between surgical approach, drainage location, use of antithrombotic drugs and postoperative recurrence. Clin. Neurol. Neurosurg. 2020, 191, 105705. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Loos, F.; Dünisch, P.; Sakr, Y.; Safatli, D.A.; Kalff, R.; Ewald, C. Risk factors for reoperation after initial burr hole trephination in chronic subdural hematomas. Clin. Neurol. Neurosurg. 2015, 138, 66–71. [Google Scholar] [CrossRef] [PubMed]
- García-Pallero, M.Á.; Pulido-Rivas, P.; Pascual-Garvi, J.M.; Sola, R.G. Hematomas subdurales cronicos. Arquitectura interna del hematoma como predictor de recidiva. Rev. Neurol. 2014, 59, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.I.; Kim, S.O.; Won, Y.S.; Kwon, Y.J.; Choi, C.S. Clinical Analysis of Risk Factors for Recurrence in Patients with Chronic Subdural Hematoma Undergoing Burr Hole Trephination. Korean J. Neurotrauma 2014, 10, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Jang, K.-M.; Kwon, J.-T.; Hwang, S.-N.; Park, Y.-S.; Nam, T.-K. Comparison of the Outcomes and Recurrence with Three Surgical Techniques for Chronic Subdural Hematoma: Single, Double Burr Hole, and Double Burr Hole Drainage with Irrigation. Korean J. Neurotrauma 2015, 11, 75–80. [Google Scholar] [CrossRef] [Green Version]
- Goto, H.; Ishikawa, O.; Nomura, M.; Tanaka, K.; Nomura, S.; Maeda, K. Magnetic resonance imaging findings predict the recurrence of chronic subdural hematoma. Neurol. Med. Chir. 2015, 55, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Doku, G.N.; Agbozo, W.K.; Annor, R.A.; Kisseh, G.D.; Owusu, M.A. Frequency of ABO/Rhesus (D) blood groupings and ethnic distribution in the Greater-Accra region of Ghana, towards effective blood bank inventory. Int. J. Immunogenet. 2019, 46, 67–73. [Google Scholar] [CrossRef]
- Ou, Y.; Yu, X.; Wu, L.; Zhang, D.; Liu, W. Recurrence of Chronic Subdural Hematoma Is Independent of ABO Blood Type: A Retrospective Cohort Study. Front. Neurol. 2022, 13, 833958. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (N = 229) | cSDH without Recurrence 182 (79.5%) | cSDH with Recurrence 47 (20.5%) | p Value |
|---|---|---|---|
| Age (yrs.), median [q1–q3] | 80 [78–83] | 78 [76–81] | 0.901 |
| Sex | 0.729 | ||
| Female | 60 (33.0%) | 14 (29.8%) | |
| Male | 122 (67.0%) | 33 (70.2%) | |
| Site of hematoma | 0.838 | ||
| Left | 69 (37.9%) | 20 (42.6%) | |
| Right | 61 (33.5%) | 15 (31.9%) | |
| Both | 52 (28.6%) | 12 (25.5%) | |
| Type of hematoma | 0.739 | ||
| Chronic | 147 (80.8%) | 40 (85.1%) | |
| Hygroma | 1 (0.5%) | 0 (0%) | |
| Sub-acute | 34 (18.7%) | 7 (14.9%) | |
| Midline shift pre-surgery | 137 (75.3%) | 35 (74.5%) | 1.000 |
| Blood loss intraoperative, mL, median [q1–q3] | 85 [82–89] | 100 [94–101] | |
| Length of stay, in days, median [q1–q3] | 6 [4–7] | 5 [3–6] | |
| Postoperative subdural drain | 170 (93.4%) | 43 (91.5%) | 0.748 |
| Anti-thrombotic therapy | |||
| ASS/Plavix | 72 (39.6%) | 19 (40.4%) | 1.000 |
| Oral anticoagulation | 51 (28.0%) | 12 (25.5%) | 0.909 |
| Neurological symptoms pre-surgery | |||
| Epilepsy | 20 (11.0%) | 7 (14.9%) | 0.0654 |
| Headache | 53 (29.1%) | 13 (27.7%) | 1.000 |
| Vigilance | 42 (23.1%) | 12 (25.5%) | 0.704 |
| Paresis | 87 (47.8%) | 26 (55.3%) | 0.414 |
| In-hospital complications | |||
| Pneumonia | 5 (2.7%) | 2 (4.3%) | 0.714 |
| UTI | 6 (3.3%) | 1 (2.1%) | 0.890 |
| Mortality | 4 (2.2%) | 2 (4.3%) | 0.605 |
| Blood type | |||
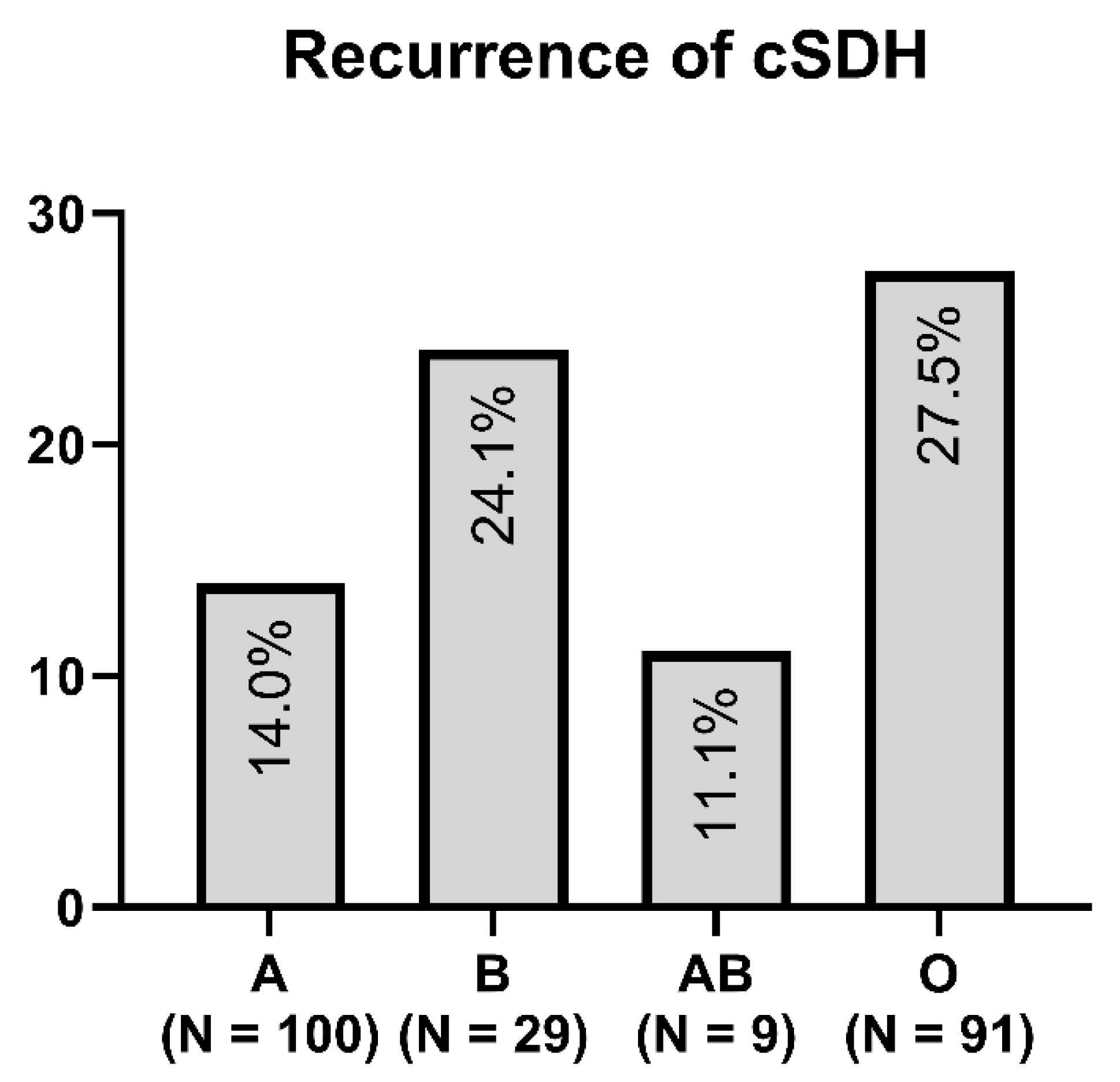
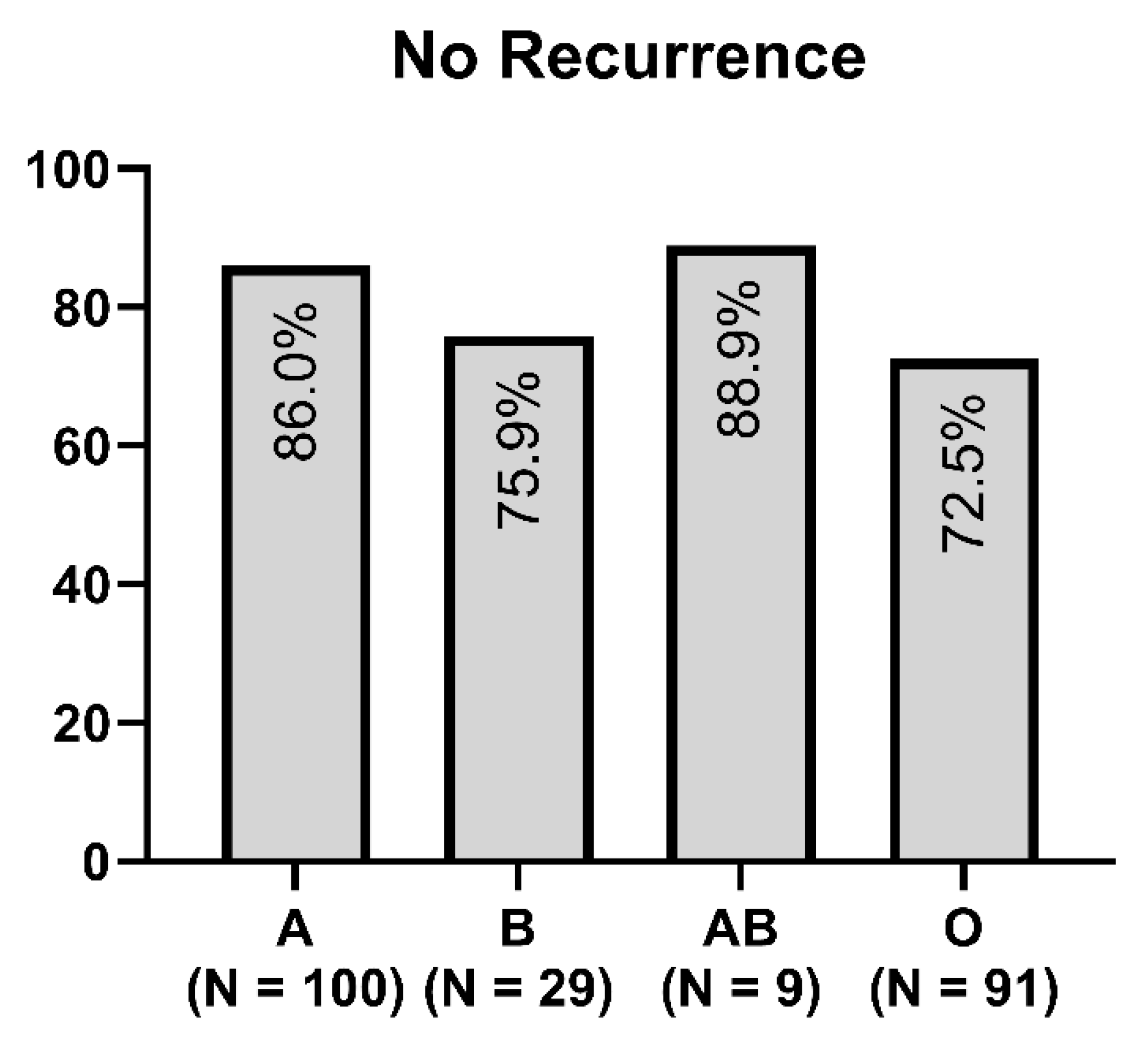
| A | 86 (47.2%) | 14 (29.8%) | 0.614 |
| B | 22 (12.1%) | 7 (14.9%) | 0.889 |
| AB | 8 (4.4%) | 1 (2.1%) | 0.726 |
| O | 66 (36.3%) | 25 (53.2%) | 0.004 * |
| Comorbidities | |||
| Hypertonia | 123 (67.6%) | 30 (63.8%) | 0.728 |
| Malignancy | 23 (12.6%) | 11 (23.4%) | 0.104 |
| Diabetes mellitus | 36 (19.8%) | 15 (31.9%) | 0.080 |
| Cardiac | 80 (43.9%) | 20 (42.5%) | 0.909 |
| Alcohol | 1 (0.5%) | 4 (8.5%) | 0.007 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamed, M.; Lampmann, T.; Salemdawod, A.; Asoglu, H.; Houedjissin, N.; Thudium, M.; Asadeh, L.; Schmeel, F.C.; Schuch, F.; Vatter, H.; et al. Correlation between Blood Type 0 and Risk of Chronic Subdural Hematoma Recurrence: A Single Center Retrospective Cohort Study. Brain Sci. 2023, 13, 567. https://doi.org/10.3390/brainsci13040567
Hamed M, Lampmann T, Salemdawod A, Asoglu H, Houedjissin N, Thudium M, Asadeh L, Schmeel FC, Schuch F, Vatter H, et al. Correlation between Blood Type 0 and Risk of Chronic Subdural Hematoma Recurrence: A Single Center Retrospective Cohort Study. Brain Sciences. 2023; 13(4):567. https://doi.org/10.3390/brainsci13040567
Chicago/Turabian StyleHamed, Motaz, Tim Lampmann, Abdallah Salemdawod, Harun Asoglu, Naomi Houedjissin, Marcus Thudium, Lakghomi Asadeh, Frederic Carsten Schmeel, Fabiane Schuch, Hartmut Vatter, and et al. 2023. "Correlation between Blood Type 0 and Risk of Chronic Subdural Hematoma Recurrence: A Single Center Retrospective Cohort Study" Brain Sciences 13, no. 4: 567. https://doi.org/10.3390/brainsci13040567