

Delay and Acceleration Threshold of Movement Perception in Patients Suffering from Vertigo or Dizziness
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Age-related dizziness was defined by age > 75 years old and spontaneous dizziness, no evident deficit of canal or otolith function, and no identifiable neurologic abnormality.
- Bilateral vestibulopathy (BVP) was defined according to the Barany Society criteria: A horizontal angular vestibulo-ocular reflex (VOR) gain on both sides < 0.6 (angular velocity 150–300°/s) and/or the sum of the maximal peak velocities of the slow-phase caloric-induced nystagmus for stimulation with warm and cold water irrigations on each side < 6°/s and/or the horizontal angular VOR gain < 0.1 during sinusoidal stimulation on a rotatory chair (0.1 Hz, Vmax = 50°/s) and/or a phase lead > 68 degrees with a time constant of <5 s [16].
- Cured benign paroxysmal positional vertigo (BPPV) was defined according to von Breven et al. [17].
- Central disorders were defined as vertigo, dizziness, or unsteadiness associated to abnormal ocular pursuit control and/or gaze nystagmus and/or dysmetric saccades and/or absent ocular fixation and/or abnormalities of central vestibular pathways on MRI [18].
- Persistent postural-perceptual dizziness (PPPD) was defined by unsteadiness > 3 months, exacerbation by upright position, self- or visual-environment movements, significant functional handicap, and symptoms not better explained by any other disorder [9].
- Acute unilateral vestibular loss defined by a canal paresis on bicaloric test (>30% asymmetry of the sum of the 2 stimulations measured by the slow-phase velocity of the nystagmus on videonystagmography) and video head impulse test (vHIT, gain < 0.7 on at least one canal on the same side) for less than 30 days.
- Compensated unilateral vestibular loss was defined by a duration > 30 days, no rotatory vertigo and no spontaneous nystagmus.
- Probable Meniere’s disease was defined according to the Meniere’s disease diagnostic criteria [19].
- Vestibular migraine was defined according to Barany Society criteria [20].
- The control subgroup comprised healthy adult volunteers without any vestibular or auditory complaints or past medical history. This group did not undergo audiovestibular workup and was only tested on the swinging bed.
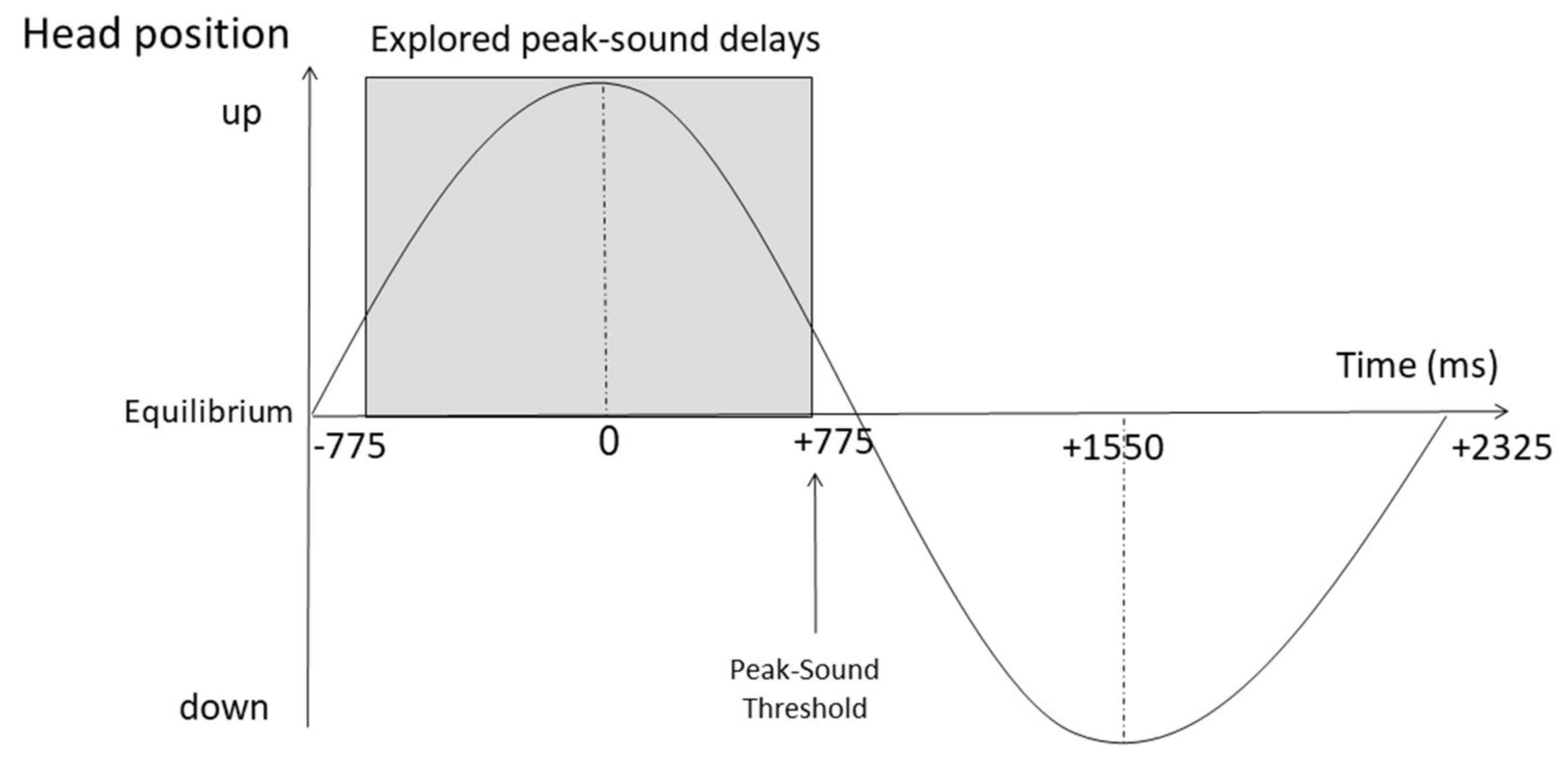
2.1. Experimental Set-Up
2.2. Statistical Tests
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colledge, N.R.; Wilson, J.A.; Macintyre, C.C.; MacLennan, W.J. The prevalence and characteristics of dizziness in an elderly community. Age Ageing 1994, 23, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Pothula, V.B.; Chew, F.; Lesser, T.H.; Sharma, A.K. Falls and vestibular impairment. Clin. Otolaryngol. Allied Sci. 2004, 29, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Hong, T.; Mitchell, P.; Burlutsky, G.; Samarawickrama, C.; Wang, J.J. Visual impairment and the incidence of falls and fractures among older people: Longitudinal findings from the Blue Mountains Eye Study. Investig. Opthalmol. Vis. Sci. 2014, 55, 7589–7593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohn, J.; Kim, S. Falls study: Proprioception, postural stability, and slips. Bio-Med. Mater. Eng. 2015, 26, S693–S703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiam, N.T.; Li, C.; Agrawal, Y. Hearing loss and falls: A systematic review and meta-analysis. Laryngoscope 2016, 126, 2587–2596. [Google Scholar] [CrossRef]
- Setti, A.; Burke, K.E.; Kenny, R.A.; Newell, F.N. Is inefficient multisensory processing associated with falls in older people? Exp. Brain Res. 2011, 209, 375–384. [Google Scholar] [CrossRef]
- Barra, J.; Pérennou, D.; Thilo, K.V.; Gresty, M.A.; Bronstein, A.M. The awareness of body orientation modulates the perception of visual vertical. Neuropsychologia 2012, 50, 2492–2498. [Google Scholar] [CrossRef]
- Lempert, T. Vestibular migraine. Semin. Neurol. 2013, 33, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Staab, J.P.; Eckhardt-Henn, A.; Horii, A.; Jacob, R.; Strupp, M.; Brandt, T.; Bronstein, A. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): Consensus document of the committee for the Classification of Vestibular Disorders of the Bárány Society. J. Vestib. Res. 2017, 27, 191–208. [Google Scholar] [CrossRef] [Green Version]
- Seemungal, B.M. The Components of Vestibular Cognition–Motion Versus Spatial Perception. Multisens. Res. 2015, 28, 507–524. [Google Scholar] [CrossRef]
- Veits, C. Zur Drehprüfung. Zbl Hals-Nas-U Ohrenheilk 1931, 29, 368–376. [Google Scholar]
- Van Egmond, A.A.J.; Groen, J.J.; Jongkees, L.B.W. The turning test with small regulable stimuli: Cupulometry. J. Laryngol. Otol. 1948, 62, 63. [Google Scholar] [CrossRef]
- Bàràny, R. Untersuchungen uber den vom Vestibularapparat des Ohres reflektorisch ausgelosten rhytmischen Nystagmus und seine Begleiterscheinungen. Mon. Ohrenheilk. 1906, 40, 193–297. [Google Scholar]
- Barnett-Cowan, M. Vestibular perception is slow: A review. Multisens. Res. 2013, 26, 387–403. [Google Scholar] [CrossRef]
- Guyon, M.; Chea, C.; Laroche, D.; Fournel, I.; Baudet, A.; Toupet, M.; Bozorg Grayeli, A. Measuring threshold and latency of motion perception on a swinging bed. PLoS ONE 2021, 16, e0252914. [Google Scholar] [CrossRef]
- Strupp, M.; Kim, J.S.; Murofushi, T.; Straumann, D.; Jen, J.C.; Rosengren, S.M.; Della Santina, C.C.; Kingma, H. Bilateral vestibulopathy: Diagnostic criteria consensus document of the classification committee of the Bárány society. J. Vestib. Res. 2017, 27, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Von Brevern, M.; Bertholon, P.; Brandt, T.; Fife, T.; Imai, T.; Nuti, D.; Newman-Toker, D. Benign paroxysmal positional vertigo: Diagnostic criteria Consensus document of the Committee for the Classification of Vestibular Disorders of the Bárány Society. Acta Otorrinolaringológica Española 2017, 68, 349–360. [Google Scholar] [CrossRef]
- Choi, J.Y.; Kim, J.S. Nystagmus and central vestibular disorders. Curr. Opin. Neurol. 2017, 30, 98–106. [Google Scholar] [CrossRef]
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.H.; Goebel, J.A.; Magnusson, M.; Mandalà, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F.; et al. Diagnostic criteria for Meniere’s disease. J. Vestib. Res. 2015, 25, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lempert, T.; Olesen, J.; Furman, J.; Waterston, J.; Seemungal, B.; Carey, J.; Bisdorff, A.; Versino, M.; Evers, S.; Newman-Toker, D. Vestibular migraine: Diagnostic criteria. J. Vestib. Res. 2012, 22, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Yelnik, A.; Bonan, I. Clinical tools for assessing balance disorders. Neurophysiol. Clin. 2008, 38, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Hyndman, D.; Ashburn, A. “Stops walking when talking” as a predictor of falls in people with stroke living in the community. J. Neurol. Neurosurg. Psychiatry 2004, 75, 994–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett-Cowan, M.; Harris, L.R. Perceived timing of vestibular stimulation relative to touch, light and sound. Exp. Brain Res. 2009, 198, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Schulze, H.H.; Vorberg, D. Linear Phase Correction Models for Synchronization: Parameter Identification and Estimation of Parameters. Brain Cogn. 2002, 48, 80–97. [Google Scholar] [CrossRef] [Green Version]
- Richter, D.; Ekman, M.; De Lange, F.P. Suppressed Sensory Response to Predictable Object Stimuli throughout the Ventral Visual Stream. J. Neurosci. 2018, 38, 7452–7461. [Google Scholar] [CrossRef] [Green Version]
- Toma, S.; Sciutti, A.; Papaxanthis, C.; Pozzo, T. Visuomotor adaptation to a visual rotation is gravity dependent. J. Neurophysiol. 2015, 113, 1885–1895. [Google Scholar] [CrossRef] [Green Version]
- Wing, A.M.; Doumas, M.; Welchman, A.E. Combining multisensory temporal information for movement synchronisation. Exp. Brain Res. 2010, 200, 277–282. [Google Scholar] [CrossRef]
- Lacquaniti, F.; Bosco, G.; Gravano, S.; Indovina, I.; La Scaleia, B.; Maffei, V.; Zago, M. Gravity in the Brain as a Reference for Space and Time Perception. Multisens. Res. 2015, 28, 397–426. [Google Scholar] [CrossRef]
- Hasson, U. The neurobiology of uncertainty: Implications for statistical learning. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2017, 372, 20160048. [Google Scholar] [CrossRef] [Green Version]
- Van Ombergen, A.; Heine, L.; Jillings, S.; Roberts, R.E.; Jeurissen, B.; Van Rompaey, V.; Mucci, V.; Vanhecke, S.; Sijbers, J.; Vanhevel, F.; et al. Altered functional brain connectivity in patients with visually induced dizziness. Neuroimage Clin. 2017, 14, 538–545. [Google Scholar] [CrossRef]
- Wurthmann, S.; Naegel, S.; Schulte Steinberg, B.; Theysohn, N.; Diener, H.C.; Kleinschnitz, C.; Obermann, M.; Holle, D. Cerebral gray matter changes in persistent postural perceptual dizziness. J. Psychosom. Res. 2017, 103, 95–101. [Google Scholar] [CrossRef]
- Espinosa-Sanchez, J.M.; Lopez-Escamez, J.A. New insights into pathophysiology of vestibular migraine. Front. Neurol. 2015, 6, 12. [Google Scholar] [CrossRef] [Green Version]
- Obermann, M.; Wurthmann, S.; Steinberg, B.S.; Theysohn, N.; Diener, H.C.; Naegel, S. Central vestibular system modulation in vestibular migraine. Cephalalgia 2014, 34, 1053–1061. [Google Scholar] [CrossRef]
- Lewis, R.F.; Priesol, A.J.; Nicoucar, K.; Lim, K.; Merfeld, D.M. Dynamic tilt thresholds are reduced in vestibular migraine. J. Vestib. Res. 2011, 21, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Hausmann, M.; Slabbekoorn, D.; Van Goozen, S.H.M.; Cohen-Kettenis, P.T.; Güntürkün, O. Sex Hormones Affect Spatial Abilities During the Menstrual Cycle. Behav. Neurosci. 2000, 114, 1245–1250. [Google Scholar] [CrossRef]
- Rahman, Q.; Wilson, G.D.; Abrahams, S. Biosocial factors, sexual orientation and neurocognitive functioning. Psychoneuroendocrinology 2004, 29, 867–881. [Google Scholar] [CrossRef]
- Egsgaard, L.L.; Petrini, L.; Christoffersen, G.; Arendt-Nielsen, L. Cortical responses to the mirror box illusion: A high-resolution EEG study. Exp. Brain Res. 2011, 215, 345–357. [Google Scholar] [CrossRef]
- Toupet, M.; Van Nechel, C.; Bozorg Grayeli, A. Subjective Visual Vertical Tilt Attraction to the Side of Rod Presentation: Effects of Age, Sex, and Vestibular Disorders. Otol. Neurotol. 2015, 36, 1074–1080. [Google Scholar] [CrossRef]
- Kingma, H. Thresholds for perception of direction of linear acceleration as a possible evaluation of the otolith function. BMC Ear Nose Throat Disord. 2005, 5, 5. [Google Scholar] [CrossRef] [Green Version]
- Gianna, C.; Heimbrand, S.; Gresty, M. Thresholds for detection of motion direction during passive lateral whole-body acceleration in normal subjects and patients with bilateral loss of labyrinthine function. Brain Res. Bull. 1996, 40, 443–447. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | n | Age (Mean ± SEM) | Sex Ratio (Male/Female) |
|---|---|---|---|
| Age-related dizziness | 4 | 89 ± 2.3 | 0.3 |
| Bilateral vestibulopathy | 19 | 66 ± 2.4 | 1.4 |
| Cured Benign Paroxysmal Positional Vertigo | 95 | 63 ± 1.7 | 0.3 |
| Central Disorders | 10 | 63 ± 5.1 | 0.4 |
| Persistent Perceptual-Postural Dizziness | 48 | 56 ± 2.9 | 0.5 |
| Acute Unilateral Loss | 5 | 54 ± 9.5 | 4 |
| Compensated Unilateral loss | 13 | 52 ± 5.8 | 0.9 |
| Meniere’s Disease | 32 | 52 ± 3.4 | 0.4 |
| Vestibular Migraine | 14 | 41 ± 4.0 | 0.4 |
| Control | 16 | 40 ± 5.1 | 0.8 |
| Total | 256 | 58 ± 1.2 | 0.5 |
| Parameters | Groups | Test |
|---|---|---|
| Average peak-sound threshold (PST, m/s) and acceleration thresholds (cm/s2) | Preliminary study controls (n = 30) vs. Current study controls (n = 16) | Mann–Whitney test |
| Iterative measures of PST | Iteration 1 (n = 238), iteration 2 (n = 231), iteration 3 (n = 229) | Mixed-effects model for repeated measures (MMRM) Global Cronbach’s alpha |
| Iterative measures of PST, effect of gender | Women (n = 162) vs. men (n = 76) Subgroups: iterations 1, 2, and 3 | MMRM |
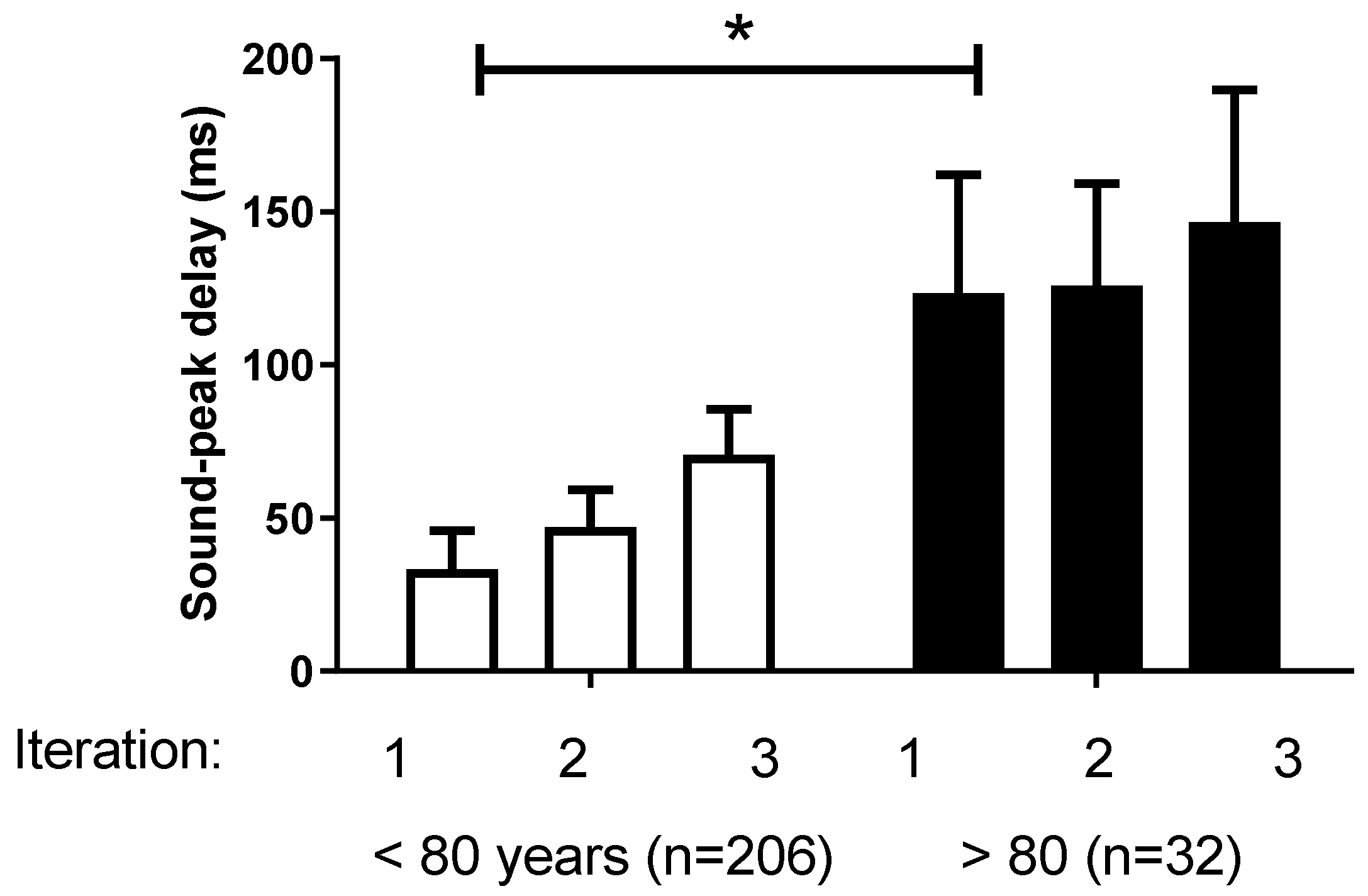
| Iterative measures of PST, effect of age | Subjects < 80 years (n = 206) vs. subjects >80 years (n = 32) Subgroups: iterations 1, 2, and 3 | MMRM |
| Average PST, effect of falls | Nonfallers (n = 160) vs. fallers (n = 67) | Mann–Whitney test |
| Average PST, effect of stop-talking-when-walking (STWW) test | Negative (n = 210) vs. positive (n = 28) STWW test | Mann–Whitney test |
| Average PST, effect of timed unipodal-stance performance | Subgroups: stance > 5 s (n = 199) vs. stance < 5 s (n = 32) vs. impossible (n = 7) | Kruskal–Wallis test |
| Peak-sound threshold, effect of etiology | Etiology categories: Control (n = 16) Cured BPPV (n = 86) Central (n = 8) Acute UL (n = 5) Comp. UL (n = 13) BVP (n = 10) Meniere (n = 30) PPPD (n = 44) VM (n = 14) Age-Related (n = 3) Subgroups: iterations 1, 2, and 3 | MMRM followed by Tukey’s posttest for multiple comparisons and p-value adjustment. |
| Acceleration threshold, effect of gender | Women (n = 159) vs. men (n = 77) | Mann–Whitney test |
| Acceleration threshold, effect of age | Subjects < 70 years (n = 68) vs. subjects > 70 years (n = 152) | Mann–Whitney test |
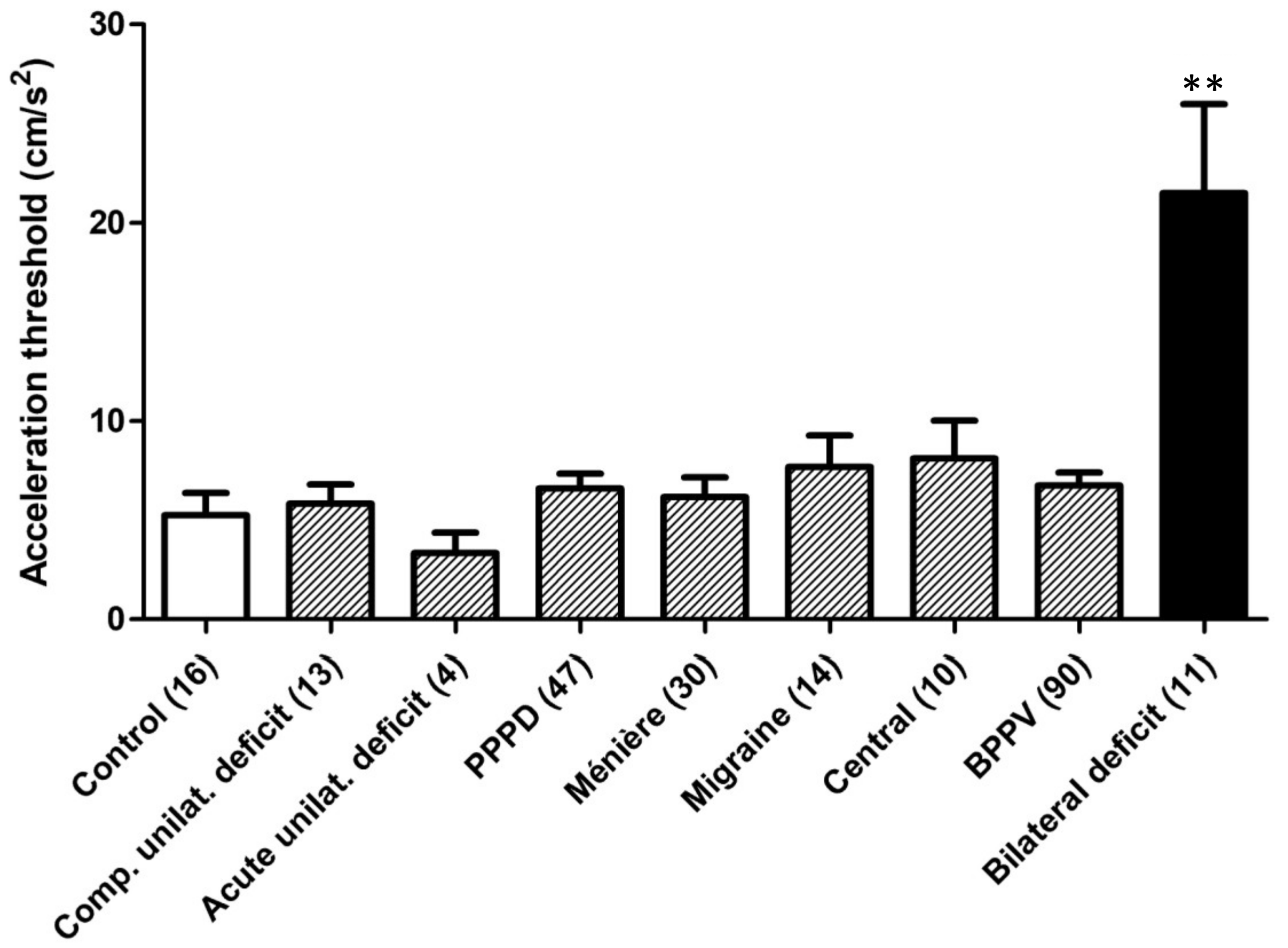
| Acceleration threshold, effect of etiology | Etiology categories: Control (n = 16) Cured BPPV (n = 90) Central (n = 10) Acute UL (n = 4) Comp. UL (n = 13) BVP (n = 11) Meniere (n = 30) PPPD (n = 47) VM (n = 14) | Kruskall–Wallis test followed by Dunn’s test for multiple comparisons to control group |
| Acceleration threshold, effect of falls | Nonfallers (n = 160) vs. fallers (n = 66) | Mann–Whitney test |
| Acceleration threshold, effect of STWW test | Negative (n = 209) vs. positive (n = 26) STWW test | Mann–Whitney test |
| Acceleration threshold, effect of timed unipodal-stance performance | Timed unipodal-stance performance, stance > 5 s (n = 197) vs. stance < 5 s (n = 30) vs. impossible (n = 8) | Kruskall–Wallis test |
| Acceleration threshold | Correlation to PST (n = 220) | Pearson correlation test |
| Etiology | Iteration 1 | Iteration 2 | Iteration 3 | Average PST | Min | Max |
|---|---|---|---|---|---|---|
| Control | 41 ± 54.2 (16) | 53 ± 32.4 (16) | 38 ± 42.0 (16) | 44 ± 35.9 (16) | −217 | 283 |
| Cured BPPV | 33 ± 16.11 (90) | 41 ± 18.3 (86) | 58 ± 20.0 (86) | 44 ± 16.1 (90) | −233 | 633 |
| Central | −22 ± 42.6 (9) | 44 ± 42.0 (9) | 31 ± 51.7 (8) | 19 ± 35.6 (9) | −167 | 167 |
| Acute UL | 130 ± 114.7 (5) | 170 ± 75.2 (5) | 190± 96.7 (5) | 163 ± 88.3 (5) | −117 | 400 |
| Comp. UL | −4 ± 41.0 (13) | 31 ± 37.8 (13) | −4 ± 36.5 (13) | 8 ± 34.8 (13) | −117 | 317 |
| BVP | −71 ± 49.0 (12) | −123 ± 74.2 (11) | 60 ± 143.5 (10) | −56 ± 72.8 (12) | −367 | 367 |
| Meniere | 5 ± 30.0 (30) | 50 ± 25.3 (30) | 62 ± 30.1 (30) | 39 ± 26.1 (30) | −217 | 550 |
| PPPD | 121 ± 33.4 (45) | 101 ± 28.4 (44) | 142 ± 34.1 (44) | 131 ± 31.3 (45) * | −300 | 750 |
| VM | 104 ± 61.7 (14) | 139 ± 51.9 (14) | 161 ± 60.9 (14) | 135 ± 55.0 (14) | −67 | 550 |
| Age-Related | 138 ± 139.0 (4) | 183 ± 136.4 (3) | 250 ± 175.6 (3) | 146 ± 94.6 (4) | −50 | 367 |
| Total | 45 ± 12.2 (238) | 57 ± 11.6 (231) | 80 ± 14.0 (229) | 61 ± 11.4 (238) | −367 | 750 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toupet, M.; Guigou, C.; Chea, C.; Guyon, M.; Heuschen, S.; Bozorg Grayeli, A. Delay and Acceleration Threshold of Movement Perception in Patients Suffering from Vertigo or Dizziness. Brain Sci. 2023, 13, 564. https://doi.org/10.3390/brainsci13040564
Toupet M, Guigou C, Chea C, Guyon M, Heuschen S, Bozorg Grayeli A. Delay and Acceleration Threshold of Movement Perception in Patients Suffering from Vertigo or Dizziness. Brain Sciences. 2023; 13(4):564. https://doi.org/10.3390/brainsci13040564
Chicago/Turabian StyleToupet, Michel, Caroline Guigou, Cyrielle Chea, Maxime Guyon, Sylvie Heuschen, and Alexis Bozorg Grayeli. 2023. "Delay and Acceleration Threshold of Movement Perception in Patients Suffering from Vertigo or Dizziness" Brain Sciences 13, no. 4: 564. https://doi.org/10.3390/brainsci13040564