
Cardiorespiratory Assessments in Panic Disorder Facilitated by Wearable Devices: A Systematic Review and Brief Comparison of the Wearable Zephyr BioPatch with the Quark-b2 Stationary Testing System
 , , ,
, , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Part 1: Systematic Review
2.1. Materials and Methods
2.1.1. Search Strategy
2.1.2. Inclusion and Exclusion Criteria
2.1.3. Screening and Extraction of Data
2.1.4. Risk-of-Bias Assessment
2.2. Results

| Authors, Year [Ref.] | Pfaltz et al., 2009 [17] | Pfaltz et al., 2010 [16] | Pfaltz et al., 2015 [28] | Rubin et al., 2015 [30]; Cruz et al., 2015 [29] | White et al., 2017 [32] | Mumm et al., 2019 [31] | Tsai et al., 2022 [33] |
|---|---|---|---|---|---|---|---|
| Study design | Cross-sectional comparison study between patients with PD and HCs. Single site | As in Pflatz et al., 2009 [17] | As in Pflatz et al., 2009 [17] | Longitudinal open study (detection-feasibility study). Single site | Sub-analyses of a selected sample from a multicenter longitudinal randomized treatment study # | Secondary analysis of a multicenter randomized controlled study investigating the augmenting effect of DCS compared to a placebo on 12-session CBT with in vivo exposure [34] | Longitudinal open study (development study of a PA ML prediction model). Single site |
| Participants, recruitment, and psychiatric assessment methodology | N = 26 patients with PD (85% F; mean age: 35.5 ± 10.9 years) and 26 HCs (77% F; mean age: 37.1 ± 9.6 years), recruited via local newspaper advertisements. Structured Diagnostic Interview for Mental Disorders (DSM-IV) | As in Pflatz et al., 2009 [17] | N = 19 patients with PD (84% F; mean age: 32.8 ± 9.6 years) and 20 HCs (80% F; mean age: 35 ± 8.3 years) who were selected from the original sample in Pfaltz et al., 2009 [17], based on the completeness of data recorded | N = 10 participants (5 females, 4 males, 1 transmale) recruited from local Meetup groups, Google AdWords, and the website, Craigslist. Each participant self-identified him/herself as suffering from PD | N = 85 patients with PD and AG (59% F; mean age: 33.89 ± 10.51; 43 patients were in the standard in vivo exposure condition, while the others were in the augmented exposure condition). The patients were selected based on data availability from a larger sample # recruited through physician referral and advertisements in media outlets. The DSM-IV TR Composite International Clinical Diagnostic Interview | A subgroup of N = 27 outpatients (from a specialized clinic for anxiety disorders) with AG (with or without PD) § with available HR and HRV recordings during in vivo exposure. No information on sex distribution or age of this subgroup. Clinical diagnosis based on ICD-10 criteria | N = 59 patients with PD (61% F; mean age: 46.2 ± 14.7), recruited from patients referred to a single Hospital in Taiwan. The DSM 5 clinician-administered Mini International Neuropsychiatric Interview |
| Comorbid psychiatric diagnoses. Current medications (number of participants) | AG = 23; MDD = 4; PTSD = 3; social phobia = 3; hypochondria = 1; SSRIs = 7; Benzodiazepines = 4; Analgesic drugs = 3. Exclusion criteria were medical diseases or medications possibly influencing cardiorespiratory functions | As in Pflatz et al., 2009 [17] | AG = 19; MDD = 2; Social phobia = 2; primary insomnia = 1. SSRIs = 4; Benzodiazepines = 2; Noradrenergic and serotonergic antidepressant = 1; Angiotensin II receptor antagonist = 1 | No information available | Exclusion criteria were comorbid psychotic or bipolar I disorder, substance-use disorder, current psychotherapeutic or psychotropic interventions (as screened in the original study #). Medical illnesses (e.g., cardiovascular or neurological) that excluded exposure-based CBT. No information about medications possibly influencing cardiac function | In total, 31 (42%) patients from the entire original sample were taking psychopharmacotherapy (stable for at least 4 weeks; no changes allowed during the study). Patients with severe medical diseases, cardiovascular diseases, or taking medications possibly influencing cardiac function were excluded from the secondary analysis | In total, 51% of patients had at least 1 comorbid psychiatric disorder (mainly AG, GAD, MDD, and PTSD). Current substance-use disorder and “cardiopulmonary incapacity” were among exclusion criteria. No information about any types of medication |
| Setting | Daily life | Daily life | Daily life | Daily life | In vivo exposure therapy (bus rides, suitable for HR collection due to the relatively minor bodily movements). Patients had to assume a seated position to minimize artifacts | Personalized in vivo exposure therapy (e.g., public transportation, elevators, driving cars, etc.) | Daily life |
| Duration of the study | Two 24-h recordings one week apart. Analyses were restricted to data recorded during waking periods (9 a.m.–9 p.m.) | As in Pfaltz et al., 2009 [17] | As in Pfaltz et al., 2009 [17] | Three weeks | The entire treatment comprised 12 CBT sessions and 2 follow-up booster sessions (2 and 4 months later). The sample included in this study completed a total of 233 bus-based exposure exercises | Duration of the entire study: 4 months. Exposure-related HR and HRV (whose aim is relevant to the present review) § were evaluated only during the first exposure in the first exposure session because it was the only exposure without DCS or placebo. | One year |
| Aim | To assess respiratory patterns in patients with PD during physical inactivity *, in comparison with HCs | To assess respiratory pattern in patients with PD compared with HCs using respiratory data stratified for predefined levels of physical activity * | To investigate whether patients with PD presented HR acceleration higher than the metabolic demand (metabolic decoupling, MD) and whether MD was related to phasic and tonic anxiety. The MV and AccM-physical activity were used to index metabolic demand | Proof-of-concept of panic-attack prediction based on physiological data (HR, BR, HRV, Temp). The predictive models were developed by using change-point analysis *** and anomaly-detection algorithms | To cluster the HR responses during exposures (by latent class cluster analysis of the individual raw HR data); to examine changes in intra-individual HR-cluster membership across sessions, and associations between HR-response types and panic-related symptoms | Aim, relevant to the present review: To evaluate HR and HRV changes during the first exposure in the first exposure session § | To build a 7-day PA ML learning prediction model using multiple physiological, clinical, and environmental potential predictors continuously collected during daily life |
| Type of wearable | LifeShirt system (Vivometrics Inc., Ventura, CA, USA) | LifeShirt system (Vivometrics Inc., Ventura, CA, USA) | LifeShirt system (Vivometrics Inc., Ventura, CA, USA) | Zephyr BioPatch (Medtronic, Inc., MN, USA) | Garmin Forerunner 310 XT (Garmin Ltd., Southampton, UK) | Polar RS800CX and accelerometer (Polar Electro Oy, Kempele, Finland) | Garmin Vivosmart 4 (Garmin International, Inc., Olathe, KS, USA) |
| Cardiorespiratory measures | TV, Ttot, MV, f/TV, TV/Ti, Ti/Ttot, Sighs, Sighs%; SD and RMSSD of TV, MV, and Ttot were calculated as indices of respiratory variability | TV, MV, Ttot, Sighs, Sighs%. RMSSD of TV and MV were calculated as indices of respiratory variability | HR, MV. Within-individual pairwise Pearson correlations of minute-by-minute average r (H-Acc), r(H-MV), and r(HR-Acc, MV) were calculated as univariate indices of metabolic coupling | HR, HRV, BR. | HR. Baseline was defined as the tonic, pre-boarding HR levels. Data were segmented into 3 epochs: before, during, and after exposure exercise | HR and two HRV indices (i.e., RMSSD of the NN intervals and HF), which reflect parasympathetic nervous system activity. Only movement-free five-min intervals were used. The HRV indices were calculated using the software, Kubios HRV | Minimum and maximum HR, average HR (during the past 7 days), and the average HR at rest, all in bpm |
| Other physiological or environmental measures of interest | AccM | AccM | AccM | Temp, AccM | GPS location, speed | AccM | Wakefulness and total-, deep-, light-, and REM-sleep duration; floors climbed, distance traveled, steps taken; multiple indices of air quality |
| Clinical measures | Psychometric questionnaires before recordings: RSQ, PDSS, MI, STAI, ASI, BDI. During recordings: self-reported PA occurrence (through a customized electronic diary) | Psychometric questionnaires before recordings: RSQ, PDSS, MI, STAI, ASI, BDI. During recordings: self-reported anxiety every three hours (by a customized electronic diary) | Tonic anxiety: STAI-Trait and ASI before recording; the mean diary-reported anxiety levels during recordings. Phasic anxiety: standard deviation of diary-reported anxiety levels | Self-reported PAs, by a smartphone application | Pre-therapy assessment: MI, BSQ, ACQ; during exposure: self-reported anxiety collected by EMA device | _ | Self-report clinical measures (BDI-II, BAI-II, STAI-S, STAI-T, PDSS-SR) were collected at 2-week intervals, through a mobile app. “PA yes” was defined as scores from 1 to 5 for the first question of the PDSS-SR; “PA no” was defined as scores of 0 |
| Main results | The two groups did not differ in terms of age, gender, body-mass index. No significant respiratory differences between PD group (with or without current medications) and HCs (alpha level was set at 0.05) | No significant respiratory differences between PD group and HCs (alpha level was set at 0.05), except for higher variability (RMSSD) of TV in PD group vs. HCs (p = 0.04) during minimal movement and slow walking. | The rHR-Acc, rHR-MV, and rHR-(Acc, MV) were lower (p = 0.005, 0.009, and 0.002, respectively) in PD group than in HCs, indicating metabolic decoupling in PD, even considering physical-fitness indices ** as covariates. In PD group, HR–Acc coupling was inversely related to ASI (p = 0.02) and phasic daytime anxiety (p = 0.047) (periods with PAs were excluded; alpha level was set at 0.05) | Seven out of ten participants were analyzed. Accounting for AccM-based physical activity, predictive models identified that in pre-panic periods, HR, BR, and Temp were higher and HRV was lower than expected, compared with non-panic periods. Only general descriptive statistics were reported. No statistics concerning the significance and accuracy of the predictive model were provided. | Pre-treatment-scale scores indicated that patients had moderately severe symptoms. Three low-level clusters (3, 4, 6) with a median HR < 91 bpm and four high-level clusters (1, 2, 5, 7) with a median HR > 97 bpm were identified. Clusters 5 and 7 presented increased HR variability and greater pre-boarding HR changes than the others. Low and relatively unvarying HR responses (e.g., cluster 4) were associated with better tolerance of bodily symptoms (p = 0.02) and low self-reported anxiety (p = 0.001) during exposure. | Significant increase in both HRV indices (HF and RMSSD of NN, p = 0.02 and 0.007, respectively) from the beginning to the end of the exposure, indicating higher parasympathetic activity at the end of the exposure (alpha level was set at <0.05) | The Random Forest ML method provided the best performance (accuracy = 81.3%) in predicting PAs one week before their occurrence. Main predictors: BAI-II, BDI-II, and STAI-S and -T scores; Mini International Neuropsychiatric Interview; average and resting HR; and deep-sleep duration (no specifications about values or directionality of predictors were reported) |
| Other findings of interest | In PD group, RSQ scores were correlated negatively with f/TV (p = 0.006) and positively with Ttot and RMSSD of Ttot. (p = 0.01 and 0.05, respectively) | Self-reported anxiety levels during daily life recordings were higher in PD group than HCs (p < 0.001). The two groups did not differ in time spent at different physical activity levels. | Anxiety levels were higher in PD group than HCs (p < 0.001). The two groups did not differ in mean accelerometer measures, MV, and physical fitness indices **. | The PA-related symptoms with highest average severity among participants were anxiety, worry, and shortness of breath; those with lowest severity were hot/cold flashes and fear of dying. | Self-reported anxiety declined across sessions (p = 0.002). The HR-cluster assignments of each participant were not stable across sessions or treatment conditions. Female patients were more commonly assigned to high-variability HR clusters (2, 5, and 7) | During exposure, patients with psychopharmacotherapy presented significantly (p < 0.01) reduced HF HRV and RMSSD of NN than those without psychopharmacotherapy | The prediction performance of the all-feature model was better than that of the physiological–environmental model (accuracy = 0.67%) and the questionnaire model alone (accuracy = 0.77%) |
2.2.1. LifeShirt-System-Based Results
2.2.2. Zephyr-BioPatch-Based Results
2.2.3. Smartwatch-Based Results
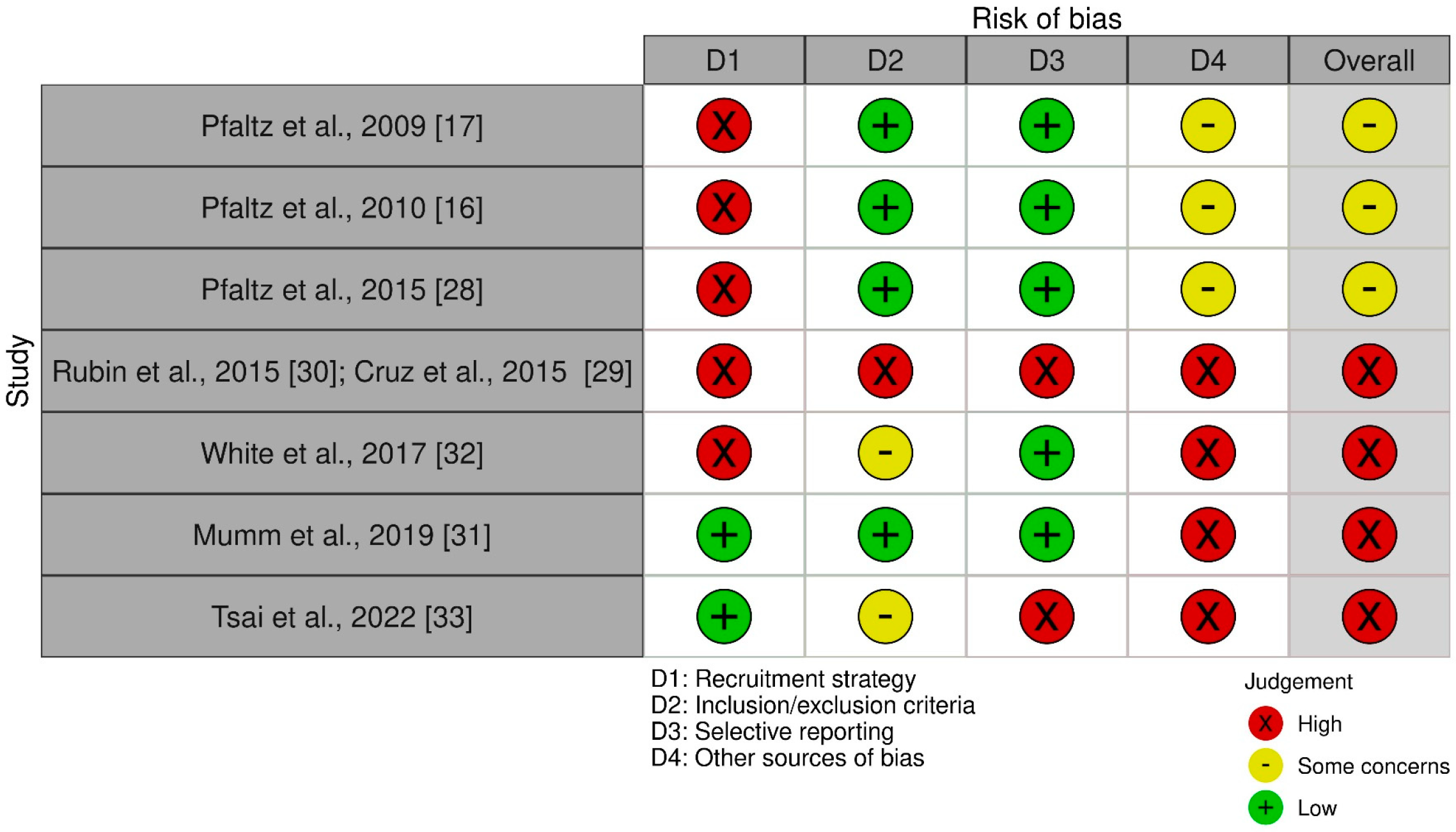
2.2.4. Risk of Bias and Quality of the Reviewed Studies
| Authors, Year [Ref.] | Selection Bias | Reporting Bias | Other Sources of Bias | |||
|---|---|---|---|---|---|---|
| Recruitment Strategy | Inclusion/Exclusion Criteria | Selective Reporting | Power Calculation | Labeling Methodology in PA Prediction Studies | Adjunctive Bias | |
| Pfaltz et al., 2009 [17] | Local newspaper advertisements (H) | Appropriate criteria assessed by clinician-administered psychiatric interview and medical examination. Exclusion criteria related to medications possibly influencing cardiorespiratory functions were present (L) | Relevant information appropriately reported (L) | Power calculation performed. Study powered to detect large effect sizes; possibly missed small–moderate effects (SCs) | _ | _ |
| Pfaltz et al., 2010 [16] | Local newspaper advertisements (H) | As in Pfaltz et al., 2009 [17] (L) | Relevant information appropriately reported (L) | As in Pfaltz et al., 2009 [17] (SCs) | _ | _ |
| Pfaltz et al., 2015 [28] | Local newspaper advertisements (H) | As in Pfaltz et al., 2009 [17] (L) | Relevant information appropriately reported (L) | As in Pfaltz et al., 2009 [17] (SCs) | _ | _ |
| Rubin et al., 2015 [30]; Cruz et al., 2015 [29] | Local Meetup groups, Google AdWords, and the website, Craigslist (H) | Self-reported PD (the sole inclusion criterion); no exclusion criteria (H) | Incomplete reporting of sample features and results. No statistics concerning the results and predictive model were provided (H) | Power calculation was not appropriate for the study | Self-reported experience(s) of PA(s) (H) | _ |
| White et al., 2017 [32] | Mixed recruitment strategy, including physician referral and advertisements in media outlets (H) | Appropriate diagnosis-related criteria assessed by clinician-administered psychiatric interview. Medical-disease-based exclusion criteria were present. Lack of exclusion criteria related to medications possibly influencing cardiac function (SCs) | Relevant information appropriately reported (L) | Power calculation was not appropriate for the study | _ | Lack of healthy control group (H) |
| Mumm et al., 2019 [31] | Selection of patients referred to a specialized clinic for anxiety and related diseases (L) | Appropriate diagnosis-related criteria assessed by clinician-administered psychiatric interview. Exclusion criteria related to medical diseases and medications possibly influencing cardiac function were present (L) | Relevant information appropriately reported (L) | Power calculation was lacking (H) | _ | Lack of healthy control group (H) |
| Tsai et al., 2022 [33] | Selection of patients referred to a hospital (L) | Appropriate diagnosis-related criteria assessed by clinician-administered psychiatric interview. Lack of medication-related exclusion criteria and definition of the exclusion criterion, “cardiopulmonary incapacity” (SCs) | No reporting of current medications, values or directionality of predictors (H) | Power calculation was not appropriate for the study | Self-reported experience(s) of PA(s) (H) | _ |
3. Part 2: Pilot Comparison of Simultaneous Cardiorespiratory Recordings by the Wearable Zephyr BioPatch and the Quark-b2 Stationary Testing System
3.1. Materials and Methods
3.2. Results
4. Discussion
4.1. General Limitations and Comments on the Reviewed Studies
4.2. Critical Wearables-Related Aspects of the Reviewed Studies and Future Research
4.3. Suggestions from the Pilot Comparison of Simultaneous Cardiorespiratory Recordings by the Wearable Zephyr BioPatch and the Quark-b2 Stationary Testing System
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AB | Abdomen |
| B&A | Bland–Altman-plot analysis |
| BR | Breathing rate |
| CBT | Cognitive-behavioral therapy |
| DCS | D-cycloserine |
| DOF | Degrees of freedom |
| ECG | Electrocardiogram |
| HCs | Healthy controls |
| HR | Heart rate |
| HRV | Heart-rate variability |
| IP | Impedance pneumography |
| ML | Machine learning |
| MV | Minute ventilation |
| NL | Nonlinear |
| PA(s) | Panic attack(s) |
| PD | Panic Disorder |
| PPG | Photoplethysmography |
| RC | Rib cage |
| RMP | Respiratory magnetometer plethysmography |
| RIP | Respiratory inductive plethysmography |
| TV | Tidal volume |
References
- Roberson-Nay, R.; Kendler, K.S. Panic Disorder and Its Subtypes: A Comprehensive Analysis of Panic Symptom Heterogeneity Using Epidemiological and Treatment Seeking Samples. Psychol. Med. 2011, 41, 2411–2421. [Google Scholar] [CrossRef] [Green Version]
- Roberson-Nay, R.; Latendresse, S.J.; Kendler, K.S. A Latent Class Approach to the External Validation of Respiratory and Non-Respiratory Panic Subtypes. Psychol. Med. 2012, 42, 461–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leibold, N.K.; Schruers, K.R. Assessing Panic: Bridging the Gap between Fundamental Mechanisms and Daily Life Experience. Front. Neurosci. 2018, 12, 785. [Google Scholar] [CrossRef]
- Caldirola, D.; Perna, G. Toward a Personalized Therapy for Panic Disorder: Preliminary Considerations from a Work in Progress. Neuropsychiatr. Dis. Treat. 2019, 15, 1957–1970. [Google Scholar] [CrossRef] [Green Version]
- Leibold, N.K.; Van Den Hove, D.L.A.; Viechtbauer, W.; Buchanan, G.F.; Goossens, L.; Lange, I.; Knuts, I.; Lesch, K.P.; Steinbusch, H.W.M.; Schruers, K.R.J. CO2 Exposure as Translational Cross-Species Experimental Model for Panic. Transl. Psychiatry 2016, 6, e885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinaugh, D.J.; Ward, M.J.; Toner, E.R.; Brown, M.L.; Losiewicz, O.M.; Bui, E.; Orr, S.P. Assessing Vulnerability to Panic: A Systematic Review of Psychological and Physiological Responses to Biological Challenges as Prospective Predictors of Panic Attacks and Panic Disorder. Gen. Psychiatry 2019, 32, e100140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perna, G.; Caldirola, D. Is Panic Disorder a Disorder of Physical Fitness? A Heuristic Proposal. F1000Research 2018, 7, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, M.; Caldirola, D.; Di Chiaro, N.V.; Riva, A.; Daccò, S.; Pompili, M.; Perna, G. Are Respiratory Abnormalities Specific for Panic Disorder? A Meta-Analysis. Neuropsychobiology 2014, 70, 52–60. [Google Scholar] [CrossRef]
- Grassi, M.; Caldirola, D.; Vanni, G.; Guerriero, G.; Piccinni, M.; Valchera, A.; Perna, G. Baseline Respiratory Parameters in Panic Disorder: A Meta-Analysis. J. Affect. Disord. 2013, 146, 158–173. [Google Scholar] [CrossRef]
- Caldirola, D.; Schruers, K.R.; Nardi, A.E.; De Berardis, D.; Fornaro, M.; Perna, G. Is There Cardiac Risk in Panic Disorder? An Updated Systematic Review. J. Affect. Disord. 2016, 194, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Shahimi, N.H.; Lim, R.; Mat, S.; Goh, C.H.; Tan, M.P.; Lim, E. Association between Mental Illness and Blood Pressure Variability: A Systematic Review. Biomed. Eng. Online 2022, 21, 19. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.C.; Su, M.I.; Liu, C.W.; Huang, Y.C.; Huang, W.L. Heart Rate Variability in Patients with Anxiety Disorders: A Systematic Review and Meta-Analysis. Psychiatry Clin. Neurosci. 2022, 76, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Meuret, A.E.; Rosenfield, D.; Wilhelm, F.H.; Zhou, E.; Conrad, A.; Ritz, T.; Roth, W.T. Do Unexpected Panic Attacks Occur Spontaneously? Biol. Psychiatry 2011, 70, 985–991. [Google Scholar] [CrossRef] [Green Version]
- Hoehn-Saric, R.; McLeod, D.R.; Funderburk, F.; Kowalski, P. Somatic Symptoms and Physiologic Responses in Generalized Anxiety Disorder and Panic Disorder: An Ambulatory Monitor Study. Arch. Gen. Psychiatry 2004, 61, 913–921. [Google Scholar] [CrossRef]
- Gündüz, N.; Aslan, E.A.; Eren, F.; Turan, H.S.; Öztürk, M.; Tural, Ü. Analysis of 24-Hour Heart Rate Variability among Panic Disorder Patients without Previous Drug Treatment and Comorbid Disorders. Turk Psikiyatr. Derg. 2019, 30, 236–244. [Google Scholar] [CrossRef]
- Pfaltz, M.C.; Grossman, P.; Michael, T.; Margraf, J.; Wilhelm, F.H. Physical Activity and Respiratory Behavior in Daily Life of Patients with Panic Disorder and Healthy Controls. Int. J. Psychophysiol. 2010, 78, 42–49. [Google Scholar] [CrossRef]
- Pfaltz, M.C.; Michael, T.; Grossman, P.; Blechert, J.; Wilhelm, F.H. Respiratory Pathophysiology of Panic Disorder: An Ambulatory Monitoring Study. Psychosom. Med. 2009, 71, 869–876. [Google Scholar] [CrossRef]
- Herhaus, B.; Siepmann, M.; Kahaly, G.J.; Conrad, R.; Petrowski, K. Effect of a Biofeedback Intervention on Heart Rate Variability in Individuals with Panic Disorder: A Randomized Controlled Trial. Psychosom. Med. 2022, 84, 199–209. [Google Scholar] [CrossRef]
- Perna, G.; Grassi, M.; Caldirola, D.; Nemeroff, C.B. The Revolution of Personalized Psychiatry: Will Technology Make It Happen Sooner? Psychol. Med. 2018, 48, 705–713. [Google Scholar] [CrossRef] [Green Version]
- Torous, J.; Bucci, S.; Bell, I.H.; Kessing, L.V.; Faurholt-Jepsen, M.; Whelan, P.; Carvalho, A.F.; Keshavan, M.; Linardon, J.; Firth, J. The Growing Field of Digital Psychiatry: Current Evidence and the Future of Apps, Social Media, Chatbots, and Virtual Reality. World Psychiatry 2021, 20, 318–335. [Google Scholar] [CrossRef]
- Grossman, P.; Wilhelm, F.H.; Brutsche, M. Accuracy of Ventilatory Measurement Employing Ambulatory Inductive Plethysmography during Tasks of Everyday Life. Biol. Psychol. 2010, 84, 121–128. [Google Scholar] [CrossRef]
- Monaco, V.; Stefanini, C. Assessing the Tidal Volume through Wearables: A Scoping Review. Sensors 2021, 21, 4124. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, A.; Spirandeli, A.F.; Moraes, R.; Zarzoso, V. Respiratory Waveform Estimation from Multiple Accelerometers: An Optimal Sensor Number and Placement Analysis. IEEE J. Biomed. Health Inform. 2019, 23, 1507–1515. [Google Scholar] [CrossRef]
- Gaidhani, A.; Moon, K.S.; Ozturk, Y.; Lee, S.Q.; Youm, W. Extraction and Analysis of Respiratory Motion Using Wearable Inertial Sensor System during Trunk Motion. Sensors 2017, 17, 2932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elgendi, M.; Menon, C. Assessing Anxiety Disorders Using Wearable Devices: Challenges and Future Directions. Brain Sci. 2019, 9, 50. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Aliverti, A. Wearable Technology: Role in Respiratory Health and Disease. Breathe 2017, 13, e27–e36. [Google Scholar] [CrossRef] [Green Version]
- Pfaltz, M.C.; Kolodyazhniy, V.; Blechert, J.; Margraf, J.; Grossman, P.; Wilhelm, F.H. Metabolic Decoupling in Daily Life in Patients with Panic Disorder and Agoraphobia. J. Psychiatr. Res. 2015, 68, 377–383. [Google Scholar] [CrossRef]
- Cruz, L.; Rubin, J.; Abreu, R.; Ahern, S.; Eldardiry, H.; Bobrow, D.G. A Wearable and Mobile Intervention Delivery System for Individuals with Panic Disorder. In Proceedings of the MUM ’15: Proceedings of the 14th International Conference on Mobile and Ubiquitous Multimedia, Linz, Austria, 30 November–2 December 2015; pp. 175–182. [Google Scholar]
- Rubin, J.; Eldardiry, H.; Abreu, R.; Ahern, S.; Du, H.; Pattekar, A.; Bobrow, D.G. Towards a Mobile and Wearable System for Predicitng Panic Attacks. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing, UbiComp, Osaka, Japan, 7 September 2015; pp. 529–533. [Google Scholar]
- Mumm, J.L.M.; Pyrkosch, L.; Plag, J.; Nagel, P.; Petzold, M.B.; Bischoff, S.; Fehm, L.; Fydrich, T.; Ströhle, A. Heart Rate Variability in Patients with Agoraphobia with or without Panic Disorder Remains Stable during CBT but Increases Following In-Vivo Exposure. J. Anxiety Disord. 2019, 64, 16–23. [Google Scholar] [CrossRef]
- White, A.J.; Kleinböhl, D.; Lang, T.; Hamm, A.O.; Gerlach, A.L.; Alpers, G.W. Identifying Patterns in Complex Field Data. Clustering Heart Rate Responses of Agoraphobic Patients Undertaking Situational Exposure. Z. Psychol. 2017, 225, 268–284. [Google Scholar]
- Tsai, C.H.; Chen, P.C.; Liu, D.S.; Kuo, Y.Y.; Hsieh, T.T.; Chiang, D.L.; Lai, F.; Wu, C.T. Panic Attack Prediction Using Wearable Devices and Machine Learning: Development and Cohort Study. JMIR Med. Inform. 2022, 10, e33063. [Google Scholar] [CrossRef] [PubMed]
- Pyrkosch, L.; Mumm, J.; Alt, I.; Fehm, L.; Fydrich, T.; Plag, J.; Ströhle, A. Learn to Forget: Does Post-Exposure Administration of d-Cycloserine Enhance Fear Extinction in Agoraphobia? J. Psychiatr. Res. 2018, 105, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Gloster, A.T.; Wittchen, H.U.; Einsle, F.; Lang, T.; Helbig-Lang, S.; Fydrich, T.; Fehm, L.; Hamm, A.O.; Richter, J.; Alpers, G.W.; et al. Psychological Treatment for Panic Disorder with Agoraphobia: A Randomized Controlled Trial to Examine the Role of Therapist-Guided Exposure in Situ in CBT. J. Consult. Clin. Psychol. 2011, 79, 406–420. [Google Scholar] [CrossRef]
- Houssein, A.; Ge, D.; Gastinger, S.; Dumond, R.; Prioux, J. Estimation of Respiratory Variables from Thoracoabdominal Breathing Distance: A Review of Different Techniques and Calibration Methods. Physiol. Meas. 2019, 40, 03TR01. [Google Scholar] [CrossRef]
- McKenna, V.S.; Huber, J.E. The Accuracy of Respiratory Calibration Methods for Estimating Lung Volume during Speech Breathing: A Comparison of Four Methods Across Three Adult Cohorts. J. Speech Lang. Hear. Res. 2019, 62, 2632–2644. [Google Scholar] [CrossRef] [PubMed]
- Redmond, C. Transthoracic Impedance Measurements in Patient Monitoring. Appl. Eng. Analog. Devices 2013. [Google Scholar]
- Hamm, A.O.; Richter, J.; Pané-Farré, C.; Westphal, D.; Wittchen, H.U.; Vossbeck-Elsebusch, A.N.; Gerlach, A.L.; Gloster, A.T.; Ströhle, A.; Lang, T.; et al. Panic Disorder with Agoraphobia from a Behavioral Neuroscience Perspective: Applying the Research Principles Formulated by the Research Domain Criteria (RDoC) Initiative. Psychophysiology 2016, 53, 312–322. [Google Scholar] [CrossRef]
- Castaneda, D.; Esparza, A.; Ghamari, M.; Soltanpur, C.; Nazeran, H. A Review on Wearable Photoplethysmography Sensors and Their Potential Future Applications in Health Care. Int. J. Biosens. Bioelectron. 2018, 4, 195–202. [Google Scholar] [CrossRef] [Green Version]
- Reali, P.; Lolatto, R.; Coelli, S.; Tartaglia, G.; Bianchi, A.M. Information Retrieval from Photoplethysmographic Sensors: A Comprehensive Comparison of Practical Interpolation and Breath-Extraction Techniques at Different Sampling Rates. Sensors 2022, 22, 1428. [Google Scholar] [CrossRef]
- Caldirola, D.; Bellodi, L.; Caumo, A.; Migliarese, G.; Perna, G. Approximate Entropy of Respiratory Patterns in Panic Disorder. Am. J. Psychiatry 2004, 161, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Giavarina, D. Understanding Bland Altman Analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [Green Version]
- Bland, M.J.; Altman, D.G. Statistical Methods for Assessing Agreement between Two Methods of Clinical Measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Parker, R.A.; Weir, C.J.; Rubio, N.; Rabinovich, R.; Pinnock, H.; Hanley, J.; McCloughan, L.; Drost, E.M.; Mantoani, L.C.; MacNee, W.; et al. Application of Mixed Effects Limits of Agreement in the Presence of Multiple Sources of Variability: Exemplar from the Comparison of Several Devices to Measure Respiratory Rate in COPD Patients. PLoS ONE 2016, 11, e0168321. [Google Scholar] [CrossRef] [Green Version]
- Caldwell, A.R. SimplyAgree: An R Package and Jamovi Module for Simplifying Agreement and Reliability Analyses. J. Open Source Softw. 2022, 7, 4148. [Google Scholar] [CrossRef]
- Sackner, M.A.; Watson, H.; Belsito, A.S.; Feinerman, D.; Suarez, M.; Gonzalez, G.; Bizousky, F.; Krieger, B. Calibration of Respiratory Inductive Plethysmograph during Natural Breathing. J. Appl. Physiol. 1989, 66, 410–420. [Google Scholar] [CrossRef]
- Romei, M.; Mauro, A.L.; D’Angelo, M.G.; Turconi, A.C.; Bresolin, N.; Pedotti, A.; Aliverti, A. Effects of Gender and Posture on Thoraco-Abdominal Kinematics during Quiet Breathing in Healthy Adults. Respir. Physiol. Neurobiol. 2010, 172, 184–191. [Google Scholar] [CrossRef]
- Mannée, D.C.; de Jongh, F.; van Helvoort, H. Telemonitoring Techniques for Lung Volume Measurement: Accuracy, Artifacts and Effort. Front. Digit. Health 2020, 2, 559483. [Google Scholar] [CrossRef]
- Raoufy, M.R.; Hajizadeh, S.; Gharibzadeh, S.; Mani, A.R.; Eftekhari, P.; Masjedi, M.R. Nonlinear Model for Estimating Respiratory Volume Based on Thoracoabdominal Breathing Movements. Respirology 2013, 18, 108–116. [Google Scholar] [CrossRef]
- Dumond, R.; Gastinger, S.; Rahman, H.A.; Le Faucheur, A.; Quinton, P.; Kang, H.; Prioux, J. Estimation of Respiratory Volume from Thoracoabdominal Breathing Distances: Comparison of Two Models of Machine Learning. Eur. J. Appl. Physiol. 2017, 117, 1533–1555. [Google Scholar] [CrossRef]
- Houssein, A.; Ge, D.; Gastinger, S.; Dumond, R.; Prioux, J. A Novel Algorithm for Minute Ventilation Estimation in Remote Health Monitoring with Magnetometer Plethysmography. Comput. Biol. Med. 2021, 130, 104189. [Google Scholar] [CrossRef]
- Mannée, D.; De Jongh, F.; Van Helvoort, H. The Accuracy of Tidal Volume Measured with a Smart Shirt during Tasks of Daily Living in Healthy Subjects: Cross-Sectional Study. JMIR Form. Res. 2021, 5, e30916. [Google Scholar] [CrossRef]
- Bricout, A.; Fontecave-Jallon, J.; Colas, D.; Gerard, G.; Pepin, J.L.; Gumery, P.Y. Adaptive Accelerometry Derived Respiration: Comparison with Respiratory Inductance Plethysmography during Sleep. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; Volume 2019, pp. 6714–6717. [Google Scholar] [CrossRef]
- Fekr, A.R.; Radecka, K.; Zilic, Z. Design and Evaluation of an Intelligent Remote Tidal Volume Variability Monitoring System in E-Health Applications. IEEE J. Biomed. Health Inform. 2015, 19, 1532–1548. [Google Scholar] [CrossRef]
- Fekr, A.R.; Radecka, K.; Zilic, Z. Tidal Volume Variability and Respiration Rate Estimation Using a Wearable Accelerometer Sensor. In Proceedings of the 4th International Conference on Wireless Mobile Communication and Healthcare—“Transforming Healthcare through Innovations in Mobile and Wireless Technologies”, Athens, Greece, 3–5 November 2014. [Google Scholar] [CrossRef]
- De la Fuente, C.; Weinstein, A.; Guzman-Venegas, R.; Arenas, J.; Cartes, J.; Soto, M.; Carpes, F.P. Use of Accelerometers for Automatic Regional Chest Movement Recognition during Tidal Breathing in Healthy Subjects. J. Electromyogr. Kinesiol. 2019, 47, 105–112. [Google Scholar] [CrossRef]
- Yoon, J.W.; Noh, Y.S.; Kwon, Y.S.; Kim, W.K.; Yoon, H.R. Improvement of Dynamic Respiration Monitoring through Sensor Fusion of Accelerometer and Gyro-Sensor. J. Electr. Eng. Technol. 2014, 9, 334–343. [Google Scholar] [CrossRef] [Green Version]
- Niccolai, V.; Van Duinen, M.A.; Griez, E.J. Respiratory Patterns in Panic Disorder Reviewed: A Focus on Biological Challenge Tests. Acta Psychiatr. Scand. 2009, 120, 167–177. [Google Scholar] [CrossRef]
- Avila, A.; Claes, J.; Buys, R.; Azzawi, M.; Vanhees, L.; Cornelissen, V. Home-Based Exercise with Telemonitoring Guidance in Patients with Coronary Artery Disease: Does It Improve Long-Term Physical Fitness? Eur. J. Prev. Cardiol. 2020, 27, 367–377. [Google Scholar] [CrossRef]
- Fonseka, L.N.; Woo, B.K.P. Consumer Wearables and the Integration of New Objective Measures in Oncology: Patient and Provider Perspectives. JMIR mHealth uHealth 2021, 9, e28664. [Google Scholar] [CrossRef]
- Chow, H.W.; Yang, C.C. Accuracy of Optical Heart Rate Sensing Technology in Wearable Fitness Trackers for Young and Older Adults: Validation and Comparison Study. JMIR mHealth uHealth 2020, 8, e14707. [Google Scholar] [CrossRef]
- Boudreaux, B.D.; Hebert, E.P.; Hollander, D.B.; Williams, B.M.; Cormier, C.L.; Naquin, M.R.; Gillan, W.W.; Gusew, E.E.; Kraemer, R.R. Validity of Wearable Activity Monitors during Cycling and Resistance Exercise. Med. Sci. Sports Exerc. 2018, 50, 624–633. [Google Scholar] [CrossRef]
- Reddy, R.K.; Pooni, R.; Zaharieva, D.P.; Senf, B.; El Youssef, J.; Dassau, E.; Doyle, F.J.; Clements, M.A.; Rickels, M.R.; Patton, S.R.; et al. Accuracy of Wrist-Worn Activity Monitors during Common Daily Physical Activities and Types of Structured Exercise: Evaluation Study. JMIR mHealth uHealth 2018, 6, e10338. [Google Scholar] [CrossRef]
- Tedesco, S.; Sica, M.; Ancillao, A.; Timmons, S.; Barton, J.; O’Flynn, B. Accuracy of Consumer-Level and Research-Grade Activity Trackers in Ambulatory Settings in Older Adults. PLoS ONE 2019, 14, e0216891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moscato, S.; Lo Giudice, S.; Massaro, G.; Chiari, L. Wrist Photoplethysmography Signal Quality Assessment for Reliable Heart Rate Estimate and Morphological Analysis. Sensors 2022, 22, 5831. [Google Scholar] [CrossRef] [PubMed]
- Sbrollini, A.; Catena, R.; Carbonari, F.; Bellini, A.; Sacchetti, M.; Burattini, L.; Morettini, M. Estimation of Tidal Volume during Exercise Stress Test from Wearable-Device Measures of Heart Rate and Breathing Rate. Appl. Sci. 2022, 12, 5441. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caldirola, D.; Daccò, S.; Grassi, M.; Alciati, A.; Sbabo, W.M.; De Donatis, D.; Martinotti, G.; De Berardis, D.; Perna, G. Cardiorespiratory Assessments in Panic Disorder Facilitated by Wearable Devices: A Systematic Review and Brief Comparison of the Wearable Zephyr BioPatch with the Quark-b2 Stationary Testing System. Brain Sci. 2023, 13, 502. https://doi.org/10.3390/brainsci13030502
Caldirola D, Daccò S, Grassi M, Alciati A, Sbabo WM, De Donatis D, Martinotti G, De Berardis D, Perna G. Cardiorespiratory Assessments in Panic Disorder Facilitated by Wearable Devices: A Systematic Review and Brief Comparison of the Wearable Zephyr BioPatch with the Quark-b2 Stationary Testing System. Brain Sciences. 2023; 13(3):502. https://doi.org/10.3390/brainsci13030502
Chicago/Turabian StyleCaldirola, Daniela, Silvia Daccò, Massimiliano Grassi, Alessandra Alciati, William M. Sbabo, Domenico De Donatis, Giovanni Martinotti, Domenico De Berardis, and Giampaolo Perna. 2023. "Cardiorespiratory Assessments in Panic Disorder Facilitated by Wearable Devices: A Systematic Review and Brief Comparison of the Wearable Zephyr BioPatch with the Quark-b2 Stationary Testing System" Brain Sciences 13, no. 3: 502. https://doi.org/10.3390/brainsci13030502