

The Impact of Motor-Cognitive Dual-Task Training on Physical and Cognitive Functions in Parkinson’s Disease
{kind=link}
Abstract
:1. Introduction
2. Construction of Motor-Cognitive Dual-Task Training
3. Effects of Dual-Task Training on Cognitive and Physical Function
3.1. Motor Symptom
3.2. Single Task Gait
3.3. Dual-Task Gait
3.4. Balance and Fall
3.5. FoG
3.6. Cognitive Function
4. Advantages and Enhancement of Dual-Task Training
4.1. Dual-Task vs. Single-Task Training
4.2. Enhancement of Dual-Task Training
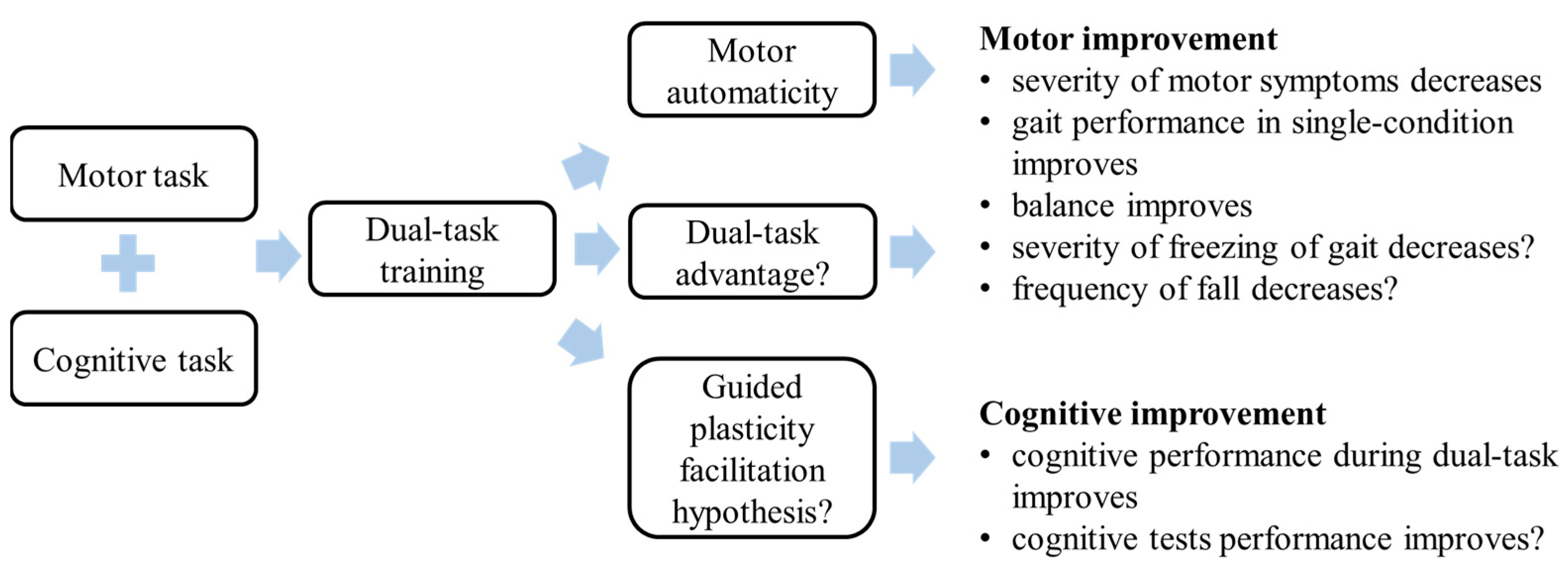
5. Mechanism of Dual-Task Training
5.1. Motor Automaticity
5.2. Dual-Task Practice Advantage
5.3. Guided Plasticity Facilitation Hypothesis
6. Future Studies
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Samii, A.; Nutt, J.G.; Ransom, B.R. Parkinson’s disease. Lancet 2004, 363, 1783–1793. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.S.; Gao, C.; Tan, Y.Y.; Chen, S.D. Prevalence of freezing of gait in Parkinson’s disease: A systematic review and meta-analysis. J. Neurol. 2021, 268, 4138–4150. [Google Scholar] [CrossRef] [PubMed]
- Okuma, Y. Freezing of gait and falls in Parkinson’s disease. J. Park. Dis. 2014, 4, 255–260. [Google Scholar] [CrossRef]
- Aarsland, D.; Batzu, L.; Halliday, G.M.; Geurtsen, G.J.; Ballard, C.; Ray Chaudhuri, K.; Weintraub, D. Parkinson disease-associated cognitive impairment. Nat. Rev. Dis. Prim. 2021, 7, 47. [Google Scholar] [CrossRef] [PubMed]
- Rochester, L.; Hetherington, V.; Jones, D.; Nieuwboer, A.; Willems, A.M.; Kwakkel, G.; Van Wegen, E. Attending to the task: Interference effects of functional tasks on walking in Parkinson’s disease and the roles of cognition, depression, fatigue, and balance. Arch. Phys. Med. Rehabil. 2004, 85, 1578–1585. [Google Scholar] [CrossRef]
- de Souza Fortaleza, A.C.; Mancini, M.; Carlson-Kuhta, P.; King, L.A.; Nutt, J.G.; Chagas, E.F.; Freitas, I.F.J.; Horak, F.B. Dual task interference on postural sway, postural transitions and gait in people with Parkinson’s disease and freezing of gait. Gait Posture 2017, 56, 76–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbruzzese, G.; Marchese, R.; Avanzino, L.; Pelosin, E. Rehabilitation for Parkinson’s disease: Current outlook and future challenges. Park. Relat. Disord. 2016, 22 (Suppl. 1), S60–S64. [Google Scholar] [CrossRef]
- Herold, F.; Hamacher, D.; Schega, L.; Müller, N.G. Thinking While Moving or Moving While Thinking—Concepts of Motor-Cognitive Training for Cognitive Performance Enhancement. Front. Aging Neurosci. 2018, 10, 228. [Google Scholar] [CrossRef] [Green Version]
- Zhu, X.; Yin, S.; Lang, M.; He, R.; Li, J. The more the better? A meta-analysis on effects of combined cognitive and physical intervention on cognition in healthy older adults. Ageing Res. Rev. 2016, 31, 67–79. [Google Scholar] [CrossRef]
- Perumal, V.; Melam, G.R.; Alhusaini, A.A.; Buragadda, S.; Sharma, N. Instruction prioritization in task-based balance training for individuals with idiopathic Parkinson’s disease. Somatosens. Mot. Res. 2017, 34, 27–33. [Google Scholar] [CrossRef]
- Fernandes, Â.; Rocha, N.; Santos, R.; Tavares, J.M. Effects of dual-task training on balance and executive functions in Parkinson’s disease: A pilot study. Somatosens. Mot. Res. 2015, 32, 122–127. [Google Scholar] [CrossRef] [Green Version]
- Salazar, R.D.; Ren, X.; Ellis, T.D.; Toraif, N.; Barthelemy, O.J.; Neargarder, S.; Cronin-Golomb, A. Dual tasking in Parkinson’s disease: Cognitive consequences while walking. Neuropsychology 2017, 31, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Radder, D.L.M.; Lígia Silva de Lima, A.; Domingos, J.; Keus, S.H.J.; van Nimwegen, M.; Bloem, B.R.; de Vries, N.M. Physiotherapy in Parkinson’s Disease: A Meta-Analysis of Present Treatment Modalities. Neurorehabilit. Neural Repair 2020, 34, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Hvingelby, V.S.; Glud, A.N.; Sørensen, J.C.H.; Tai, Y.; Andersen, A.S.M.; Johnsen, E.; Moro, E.; Pavese, N. Interventions to improve gait in Parkinson’s disease: A systematic review of randomized controlled trials and network meta-analysis. J. Neurol. 2022, 269, 4068–4079. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, T.; Liu, H.; Jiang, Y.; Wang, Z.; Zhuang, J. Dual-task training on gait, motor symptoms, and balance in patients with Parkinson’s disease: A systematic review and meta-analysis. Clin. Rehabil. 2020, 34, 1355–1367. [Google Scholar] [CrossRef]
- Conradsson, D.; Löfgren, N.; Nero, H.; Hagströmer, M.; Ståhle, A.; Lökk, J.; Franzén, E. The Effects of Highly Challenging Balance Training in Elderly With Parkinson’s Disease: A Randomized Controlled Trial. Neurorehabilit. Neural Repair 2015, 29, 827–836. [Google Scholar] [CrossRef] [Green Version]
- Chua, L.K.; Chung, Y.C.; Bellard, D.; Swan, L.; Gobreial, N.; Romano, A.; Glatt, R.; Bonaguidi, M.A.; Lee, D.J.; Jin, Y.; et al. Gamified Dual-Task Training for Individuals with Parkinson Disease: An Exploratory Study on Feasibility, Safety, and Efficacy. Int. J. Environ. Res. Public Health 2021, 18, 12384. [Google Scholar] [CrossRef]
- Rosenfeldt, A.B.; Penko, A.L.; Streicher, M.C.; Zimmerman, N.M.; Koop, M.M.; Alberts, J.L. Improvements in temporal and postural aspects of gait vary following single- and multi-modal training in individuals with Parkinson’s disease. Park. Relat. Disord. 2019, 64, 280–285. [Google Scholar] [CrossRef]
- Penko, A.L.; Barkley, J.E.; Rosenfeldt, A.B.; Alberts, J.L. Multimodal Training Reduces Fall Frequency as Physical Activity Increases in Individuals With Parkinson’s Disease. J. Phys. Act. Health 2019, 16, 1085–1091. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.C.; Chen, C.C.; Weng, Y.H.; Chiou, W.D.; Chang, Y.J.; Lu, C.S. The efficacy of cognitive-cycling dual-task training in patients with early-stage Parkinson’s disease: A pilot study. NeuroRehabilitation 2020, 47, 415–426. [Google Scholar] [CrossRef]
- Clerici, I.; Maestri, R.; Bonetti, F.; Ortelli, P.; Volpe, D.; Ferrazzoli, D.; Frazzitta, G. Land Plus Aquatic Therapy Versus Land-Based Rehabilitation Alone for the Treatment of Freezing of Gait in Parkinson Disease: A Randomized Controlled Trial. Phys. Ther. 2019, 99, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Fok, P.; Farrell, M.; McMeeken, J. The effect of dividing attention between walking and auxiliary tasks in people with Parkinson’s disease. Hum. Mov. Sci. 2012, 31, 236–246. [Google Scholar] [CrossRef]
- Wollesen, B.; Rudnik, S.; Gulberti, A.; Cordes, T.; Gerloff, C.; Poetter-Nerger, M. A feasibility study of dual-task strategy training to improve gait performance in patients with Parkinson’s disease. Sci. Rep. 2021, 11, 12416. [Google Scholar] [CrossRef] [PubMed]
- Canning, C.G.; Ada, L.; Woodhouse, E. Multiple-task walking training in people with mild to moderate Parkinson’s disease: A pilot study. Clin. Rehabil. 2008, 22, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Strouwen, C.; Molenaar, E.; Münks, L.; Keus, S.H.J.; Zijlmans, J.C.M.; Vandenberghe, W.; Bloem, B.R.; Nieuwboer, A. Training dual tasks together or apart in Parkinson’s disease: Results from the DUALITY trial. Mov. Disord. Off. J. Mov. Disord. Soc. 2017, 32, 1201–1210. [Google Scholar] [CrossRef]
- Killane, I.; Fearon, C.; Newman, L.; McDonnell, C.; Waechter, S.M.; Sons, K.; Lynch, T.; Reilly, R.B. Dual Motor-Cognitive Virtual Reality Training Impacts Dual-Task Performance in Freezing of Gait. IEEE J. Biomed. Health Inform. 2015, 19, 1855–1861. [Google Scholar] [CrossRef] [PubMed]
- King, L.A.; Mancini, M.; Smulders, K.; Harker, G.; Lapidus, J.A.; Ramsey, K.; Carlson-Kuhta, P.; Fling, B.W.; Nutt, J.G.; Peterson, D.S.; et al. Cognitively Challenging Agility Boot Camp Program for Freezing of Gait in Parkinson Disease. Neurorehabilit. Neural Repair 2020, 34, 417–427. [Google Scholar] [CrossRef]
- San Martín Valenzuela, C.; Moscardó, L.D.; López-Pascual, J.; Serra-Añó, P.; Tomás, J.M. Effects of Dual-Task Group Training on Gait, Cognitive Executive Function, and Quality of Life in People With Parkinson Disease: Results of Randomized Controlled DUALGAIT Trial. Arch. Phys. Med. Rehabil. 2020, 101, 1849–1856.e1841. [Google Scholar] [CrossRef]
- Pereira-Pedro, K.P.; de Oliveira, I.M.; Mollinedo-Cardalda, I.; Cancela-Carral, J.M. Effects of Cycling Dual-Task on Cognitive and Physical Function in Parkinson’s Disease: A Randomized Double-Blind Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 7847. [Google Scholar] [CrossRef]
- Sarasso, E.; Agosta, F.; Piramide, N.; Gardoni, A.; Canu, E.; Leocadi, M.; Castelnovo, V.; Basaia, S.; Tettamanti, A.; Volontè, M.A.; et al. Action Observation and Motor Imagery Improve Dual Task in Parkinson’s Disease: A Clinical/fMRI Study. Mov. Disord. Off. J. Mov. Disord. Soc. 2021, 36, 2569–2582. [Google Scholar] [CrossRef]
- Schabrun, S.M.; Lamont, R.M.; Brauer, S.G. Transcranial Direct Current Stimulation to Enhance Dual-Task Gait Training in Parkinson’s Disease: A Pilot RCT. PLoS ONE 2016, 11, e0158497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strouwen, C.; Molenaar, E.A.; Münks, L.; Keus, S.H.; Bloem, B.R.; Rochester, L.; Nieuwboer, A. Dual tasking in Parkinson’s disease: Should we train hazardous behavior? Expert Rev. Neurother. 2015, 15, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Cameron, I.G.; Watanabe, M.; Pari, G.; Munoz, D.P. Executive impairment in Parkinson’s disease: Response automaticity and task switching. Neuropsychologia 2010, 48, 1948–1957. [Google Scholar] [CrossRef]
- Wu, T.; Hallett, M. A functional MRI study of automatic movements in patients with Parkinson’s disease. Brain A J. Neurol. 2005, 128, 2250–2259. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Hallett, M.; Chan, P. Motor automaticity in Parkinson’s disease. Neurobiol. Dis. 2015, 82, 226–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.; Liu, J.; Zhang, H.; Hallett, M.; Zheng, Z.; Chan, P. Attention to Automatic Movements in Parkinson’s Disease: Modified Automatic Mode in the Striatum. Cereb. Cortex 2015, 25, 3330–3342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuckovic, M.G.; Li, Q.; Fisher, B.; Nacca, A.; Leahy, R.M.; Walsh, J.P.; Mukherjee, J.; Williams, C.; Jakowec, M.W.; Petzinger, G.M. Exercise elevates dopamine D2 receptor in a mouse model of Parkinson’s disease: In vivo imaging with [(1)(8)F] fallypride. Mov. Disord. Off. J. Mov. Disord. Soc. 2010, 25, 2777–2784. [Google Scholar] [CrossRef] [Green Version]
- Fisher, B.E.; Li, Q.; Nacca, A.; Salem, G.J.; Song, J.; Yip, J.; Hui, J.S.; Jakowec, M.W.; Petzinger, G.M. Treadmill exercise elevates striatal dopamine D2 receptor binding potential in patients with early Parkinson’s disease. Neuroreport 2013, 24, 509–514. [Google Scholar] [CrossRef]
- Johansson, M.E.; Cameron, I.G.M.; Van der Kolk, N.M.; de Vries, N.M.; Klimars, E.; Toni, I.; Bloem, B.R.; Helmich, R.C. Aerobic Exercise Alters Brain Function and Structure in Parkinson’s Disease: A Randomized Controlled Trial. Ann. Neurol. 2022, 91, 203–216. [Google Scholar] [CrossRef]
- Albrecht, F.; Pereira, J.B.; Mijalkov, M.; Freidle, M.; Johansson, H.; Ekman, U.; Westman, E.; Franzen, E. Effects of a Highly Challenging Balance Training Program on Motor Function and Brain Structure in Parkinson’s Disease. J. Park. Dis. 2021, 11, 2057–2071. [Google Scholar] [CrossRef]
- Strobach, T. The dual-task practice advantage: Empirical evidence and cognitive mechanisms. Psychon. Bull. Rev. 2020, 27, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Silsupadol, P.; Shumway-Cook, A.; Lugade, V.; van Donkelaar, P.; Chou, L.S.; Mayr, U.; Woollacott, M.H. Effects of single-task versus dual-task training on balance performance in older adults: A double-blind, randomized controlled trial. Arch. Phys. Med. Rehabil. 2009, 90, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Hirst, W.; Spelke, E.S.; Reaves, C.C.; Caharack, G.; Neisser, U. Dividing attention without alternation or automaticity. J. Exp. Psychol. Gen. 1980, 109, 98–117. [Google Scholar] [CrossRef]
- Liepelt, R.; Strobach, T.; Frensch, P.; Schubert, T. Improved intertask coordination after extensive dual-task practice. Q. J. Exp. Psychol. 2011, 64, 1251–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bherer, L.; Gagnon, C.; Langeard, A.; Lussier, M.; Desjardins-Crepeau, L.; Berryman, N.; Bosquet, L.; Vu, T.T.M.; Fraser, S.; Li, K.Z.H.; et al. Synergistic Effects of Cognitive Training and Physical Exercise on Dual-Task Performance in Older Adults. J Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 1533–1541. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Liu, J.; Hallett, M.; Zheng, Z.; Chan, P. Cerebellum and integration of neural networks in dual-task processing. Neuroimage 2013, 65, 466–475. [Google Scholar] [CrossRef] [Green Version]
- Geroin, C.; Nonnekes, J.; de Vries, N.M.; Strouwen, C.; Smania, N.; Tinazzi, M.; Nieuwboer, A.; Bloem, B.R. Does dual-task training improve spatiotemporal gait parameters in Parkinson’s disease? Park. Relat. Disord. 2018, 55, 86–91. [Google Scholar] [CrossRef]
- Fabel, K.; Wolf, S.A.; Ehninger, D.; Babu, H.; Leal-Galicia, P.; Kempermann, G. Additive effects of physical exercise and environmental enrichment on adult hippocampal neurogenesis in mice. Front. Neurosci. 2009, 3, 50. [Google Scholar] [CrossRef] [Green Version]
- Lu, B.; Nagappan, G.; Lu, Y. BDNF and synaptic plasticity, cognitive function, and dysfunction. Handb. Exp. Pharmacol. 2014, 220, 223–250. [Google Scholar] [CrossRef]
- Hernandez-Vara, J.; Saez-Francas, N.; Lorenzo-Bosquet, C.; Corominas-Roso, M.; Cuberas-Borros, G.; Lucas-Del Pozo, S.; Carter, S.; Armengol-Bellapart, M.; Castell-Conesa, J. BDNF levels and nigrostriatal degeneration in “drug naive” Parkinson’s disease patients. An “in vivo” study using I-123-FP-CIT SPECT. Park. Relat. Disord. 2020, 78, 31–35. [Google Scholar] [CrossRef]
- Walsh, J.J.; Tschakovsky, M.E. Exercise and circulating BDNF: Mechanisms of release and implications for the design of exercise interventions. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2018, 43, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Gonzalez, D.; Hernandez-Martinez, A.; Valenzuela, P.L.; Morales, J.S.; Soriano-Maldonado, A. Effects of physical exercise on plasma brain-derived neurotrophic factor in neurodegenerative disorders: A systematic review and meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 2021, 128, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, E.; Roeben, B.; Granert, O.; Hanert, A.; Liepelt-Scarfone, I.; Leks, E.; Otterbein, S.; Saraykin, P.; Busch, J.H.; Synofzik, M.; et al. Effects of exergaming on hippocampal volume and brain-derived neurotrophic factor levels in Parkinson’s disease. Eur. J. Neurol. 2022, 29, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Vaynman, S.; Ying, Z.; Gomez-Pinilla, F. Hippocampal BDNF mediates the efficacy of exercise on synaptic plasticity and cognition. Eur. J. Neurosci. 2004, 20, 2580–2590. [Google Scholar] [CrossRef]
- Angelucci, F.; Piermaria, J.; Gelfo, F.; Shofany, J.; Tramontano, M.; Fiore, M.; Caltagirone, C.; Peppe, A. The effects of motor rehabilitation training on clinical symptoms and serum BDNF levels in Parkinson’s disease subjects. Can. J. Physiol. Pharm. 2016, 94, 455–461. [Google Scholar] [CrossRef] [Green Version]
- Kempermann, G.; Gast, D.; Gage, F.H. Neuroplasticity in old age: Sustained fivefold induction of hippocampal neurogenesis by long-term environmental enrichment. Ann. Neurol. 2002, 52, 135–143. [Google Scholar] [CrossRef]
- Heisz, J.J.; Clark, I.B.; Bonin, K.; Paolucci, E.M.; Michalski, B.; Becker, S.; Fahnestock, M. The Effects of Physical Exercise and Cognitive Training on Memory and Neurotrophic Factors. J. Cogn. Neurosci. 2017, 29, 1895–1907. [Google Scholar] [CrossRef]
- Angelucci, F.; Peppe, A.; Carlesimo, G.A.; Serafini, F.; Zabberoni, S.; Barban, F.; Shofany, J.; Caltagirone, C.; Costa, A. A pilot study on the effect of cognitive training on BDNF serum levels in individuals with Parkinson’s disease. Front. Hum. Neurosci. 2015, 9, 130. [Google Scholar] [CrossRef] [Green Version]
- Brauer, S.G.; Morris, M.E. Can people with Parkinson’s disease improve dual tasking when walking? Gait Posture 2010, 31, 229–233. [Google Scholar] [CrossRef]
- Duncan, R.P.; Earhart, G.M. Randomized controlled trial of community-based dancing to modify disease progression in Parkinson disease. Neurorehabilit. Neural Repair 2012, 26, 132–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Bruin, N.; Doan, J.B.; Turnbull, G.; Suchowersky, O.; Bonfield, S.; Hu, B.; Brown, L.A. Walking with music is a safe and viable tool for gait training in Parkinson’s disease: The effect of a 13-week feasibility study on single and dual task walking. Park. Dis. 2010, 2010, 483530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa-Ribeiro, A.; Andrade, S.; Ferrer, M.L.V.; Silva, O.; Salvador, M.L.S.; Smaili, S.; Lindquist, A.R.R. Can Task Specificity Impact tDCS-Linked to Dual Task Training Gains in Parkinson’s Disease? A Protocol for a Randomized Controlled Trial. Front. Aging Neurosci. 2021, 13, 684689. [Google Scholar] [CrossRef] [PubMed]
- Wong-Yu, I.S.; Mak, M.K. Multi-dimensional balance training programme improves balance and gait performance in people with Parkinson’s disease: A pragmatic randomized controlled trial with 12-month follow-up. Park. Relat. Disord. 2015, 21, 615–621. [Google Scholar] [CrossRef]
- Ali, N.; Tian, H.; Thabane, L.; Ma, J.; Wu, H.; Zhong, Q.; Gao, Y.; Sun, C.; Zhu, Y.; Wang, T. The Effects of Dual-Task Training on Cognitive and Physical Functions in Older Adults with Cognitive Impairment; A Systematic Review and Meta-Analysis. J. Prev. Alzheimer’s Dis. 2022, 9, 359–370. [Google Scholar] [CrossRef]
- Feng, Y.S.; Yang, S.D.; Tan, Z.X.; Wang, M.M.; Xing, Y.; Dong, F.; Zhang, F. The benefits and mechanisms of exercise training for Parkinson’s disease. Life Sci. 2020, 245, 117345. [Google Scholar] [CrossRef] [PubMed]
- Machado, S.; Teixeira, D.; Monteiro, D.; Imperatori, C.; Murillo-Rodriguez, E.; da Silva Rocha, F.P.; Yamamoto, T.; Amatriain-Fernández, S.; Budde, H.; Carta, M.G.; et al. Clinical applications of exercise in Parkinson’s disease: What we need to know? Expert Rev. Neurother. 2022, 22, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Johansson, H.; Ekman, U.; Rennie, L.; Peterson, D.S.; Leavy, B.; Franzen, E. Dual-Task Effects During a Motor-Cognitive Task in Parkinson’s Disease: Patterns of Prioritization and the Influence of Cognitive Status. Neurorehabilit. Neural Repair 2021, 35, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Strouwen, C.; Molenaar, E.; Münks, L.; Broeder, S.; Ginis, P.; Bloem, B.R.; Nieuwboer, A.; Heremans, E. Determinants of Dual-Task Training Effect Size in Parkinson Disease: Who Will Benefit Most? J. Neurol. Phys. 2019, 43, 3–11. [Google Scholar] [CrossRef]
- Kim, R.; Park, S.; Yoo, D.; Jun, J.S.; Jeon, B. Association of Physical Activity and APOE Genotype With Longitudinal Cognitive Change in Early Parkinson Disease. Neurology 2021, 96, e2429–e2437. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, Y.; Yang, T.; Shang, H. The Impact of Motor-Cognitive Dual-Task Training on Physical and Cognitive Functions in Parkinson’s Disease. Brain Sci. 2023, 13, 437. https://doi.org/10.3390/brainsci13030437
Xiao Y, Yang T, Shang H. The Impact of Motor-Cognitive Dual-Task Training on Physical and Cognitive Functions in Parkinson’s Disease. Brain Sciences. 2023; 13(3):437. https://doi.org/10.3390/brainsci13030437
Chicago/Turabian StyleXiao, Yi, Tianmi Yang, and Huifang Shang. 2023. "The Impact of Motor-Cognitive Dual-Task Training on Physical and Cognitive Functions in Parkinson’s Disease" Brain Sciences 13, no. 3: 437. https://doi.org/10.3390/brainsci13030437