
The Resting State of Taiwan EEG Normative Database: Z-Scores of Patients with Major Depressive Disorder as the Cross-Validation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Material
- (1)
- Psychological questionnaires: Demographic data (e.g., age and sex), BDI-II, and BAI were measured. The BDI-II includes 21 items scored on a four-point Likert scale to assess depressive symptoms. The total score of the BDI–II ranges from 0 to 63, and a higher BDI-II score indicates more depressive symptoms [29]. The Chinese version of the BDI–II was translated by Chen [30], where Cronbach’s α was 0.94, split-half reliability was 0.91, and the BDI-II correlated with the Chinese Health Questionnaire was 0.69 [31] (Lu et al., 2002). The BAI includes 21 items scored on a four-point Likert scale to assess anxiety symptoms. The total score ranges from 0 to 63, with higher BAI scores indicating more anxiety symptoms [32] (Beck et al., 1988). The Chinese version of the BDI–II was translated by Lin [33], where Cronbach’s α was 0.95, the split-half reliability was 0.91, and the BAI correlated with the Hamilton Anxiety Scale was 0.72 [34]. The BDI-II and BAI, which have good psychometric characteristics, were used to assess depression and anxiety in clinical practice;
- (2)
- EEG recording: EEG raw signals were recorded using the BrainMaster Discovery 24 with impedance lid amplifier equipment and BrainAvatar 4.0 software (BrainMaster Technologies, Inc., Bedford, Ohio). A 19-channel EEG cap (Electro-Cap International, Inc., Eaton Ohio) based on the international 10−20 system, including Fp1, Fp2, Fz, F3, F4, F7, F8, Cz, C3, C4, T3, T4, T5, T6, Pz, P3, P4, O1, and O2, was connected to the BrainMaster equipment to measure the raw EEG signals. A linked-ear reference, impedance below 5 kΩ, 0–100 Hz of the bandpass filter of 60 Hz, notch filter, and sampling rate of 256 Hz were applied during the EEG recording.
2.3. Data Reduction, EEG Processing, and Statistical Analysis
3. Results
3.1. Participants’ Demographic Characteristics between the HC Group and the MDD Group
3.2. Reliability and Validity in the Taiwan Normative Database
3.3. The Z-Scores and Absolute Value Z-Scores in the MDD Group
3.4. Correlations between Depression, Anxiety, and Z-Scores in the MDD Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| BDI-II (Depression) | BAI (Anxiety) | ||||||
|---|---|---|---|---|---|---|---|
| Cognitive Depression | Somatic Depression | Total Depression Score | Cognitive Anxiety | Somatic Anxiety | Total Anxiety Score | ||
| delta | Fz | −0.09 | −0.11 | −0.10 | −0.06 | −0.09 | −0.08 |
| F3 | 0.00 | −0.11 | −0.03 | −0.03 | −0.08 | −0.06 | |
| F4 | −0.06 | −0.15 * | −0.09 | −0.08 | −0.07 | −0.09 | |
| F7 | −0.13 | −0.11 | −0.13 | −0.07 | −0.11 | −0.09 | |
| F8 | −0.05 | −0.08 | −0.07 | −0.13 | −0.09 | −0.12 | |
| Cz | −0.03 | −0.10 | −0.05 | −0.06 | −0.10 | −0.09 | |
| C3 | −0.05 | −0.12 | −0.07 | −0.07 | −0.11 | −0.10 | |
| C4 | −0.03 | −0.08 | −0.05 | −0.03 | −0.06 | −0.05 | |
| Pz | −0.05 | −0.11 | −0.07 | −0.06 | −0.09 | −0.09 | |
| P3 | −0.03 | −0.09 | −0.05 | −0.06 | −0.11 | −0.09 | |
| P4 | −0.01 | −0.11 | −0.03 | −0.04 | −0.11 | −0.08 | |
| T3 | −0.05 | −0.14 | −0.08 | −0.16 * | −0.12 | −0.16 * | |
| T4 | −0.07 | −0.14 * | −0.10 | −0.08 | −0.08 | −0.09 | |
| T5 | 0.01 | −0.09 | −0.02 | −0.04 | −0.04 | −0.04 | |
| T6 | 0.00 | −0.10 | −0.03 | −0.06 | −0.07 | −0.07 | |
| O1 | 0.03 | −0.03 | 0.02 | 0.08 | 0.00 | 0.05 | |
| O2 | 0.05 | −0.07 | 0.03 | −0.01 | −0.05 | −0.04 | |
| theta | Fz | −0.02 | −0.05 | −0.03 | −0.02 | −0.04 | −0.03 |
| F3 | −0.01 | −0.05 | −0.02 | −0.02 | −0.03 | −0.03 | |
| F4 | −0.01 | −0.08 | −0.02 | −0.01 | −0.02 | −0.02 | |
| F7 | −0.04 | −0.05 | −0.05 | −0.02 | −0.06 | −0.05 | |
| F8 | 0.03 | −0.03 | 0.02 | −0.01 | 0.00 | −0.01 | |
| Cz | 0.02 | −0.04 | 0.01 | 0.00 | −0.03 | −0.02 | |
| C3 | 0.01 | −0.04 | 0.00 | −0.01 | −0.03 | −0.02 | |
| C4 | 0.01 | −0.05 | 0.00 | 0.00 | −0.02 | −0.01 | |
| Pz | 0.02 | −0.05 | 0.00 | 0.00 | −0.02 | −0.01 | |
| P3 | 0.04 | −0.03 | 0.02 | 0.01 | 0.00 | 0.01 | |
| P4 | 0.01 | −0.05 | 0.00 | −0.01 | −0.01 | −0.01 | |
| T3 | 0.01 | −0.02 | 0.00 | −0.03 | −0.08 | −0.06 | |
| T4 | 0.02 | −0.05 | 0.01 | −0.01 | −0.02 | −0.01 | |
| T5 | 0.05 | −0.04 | 0.03 | 0.00 | 0.05 | 0.03 | |
| T6 | 0.01 | −0.04 | 0.00 | 0.00 | 0.01 | 0.00 | |
| O1 | 0.05 | −0.01 | 0.04 | 0.03 | 0.00 | 0.02 | |
| O2 | 0.05 | −0.01 | 0.04 | 0.02 | 0.03 | 0.03 | |
| alpha | Fz | 0.00 | 0.00 | 0.00 | −0.02 | 0.05 | 0.01 |
| F3 | −0.02 | −0.03 | −0.02 | −0.03 | 0.03 | 0.00 | |
| F4 | −0.03 | −0.06 | −0.04 | −0.03 | 0.05 | 0.01 | |
| F7 | 0.00 | −0.02 | 0.00 | −0.03 | 0.04 | 0.00 | |
| F8 | 0.02 | 0.00 | 0.02 | −0.02 | 0.04 | 0.01 | |
| Cz | −0.04 | −0.05 | −0.05 | −0.06 | −0.01 | −0.04 | |
| C3 | −0.04 | −0.06 | −0.05 | −0.06 | −0.01 | −0.04 | |
| C4 | −0.03 | −0.07 | −0.04 | −0.06 | 0.00 | −0.04 | |
| Pz | −0.02 | −0.05 | −0.03 | −0.04 | 0.02 | −0.02 | |
| P3 | −0.01 | −0.07 | −0.03 | −0.07 | 0.03 | −0.02 | |
| P4 | 0.00 | −0.07 | −0.02 | −0.06 | 0.06 | 0.00 | |
| T3 | 0.05 | 0.02 | 0.05 | −0.04 | 0.02 | −0.01 | |
| T4 | 0.01 | −0.05 | −0.01 | −0.04 | 0.03 | −0.01 | |
| T5 | 0.05 | −0.01 | 0.04 | −0.03 | 0.06 | 0.01 | |
| T6 | 0.03 | −0.03 | 0.02 | −0.01 | 0.12 | 0.06 | |
| O1 | 0.06 | −0.01 | 0.05 | 0.03 | 0.08 | 0.06 | |
| O2 | 0.08 | 0.00 | 0.07 | 0.05 | 0.12 | 0.10 | |
| beta | Fz | 0.04 | 0.05 | 0.04 | 0.02 | 0.10 | 0.06 |
| F3 | 0.04 | 0.03 | 0.04 | 0.03 | 0.12 | 0.08 | |
| F4 | 0.01 | −0.01 | 0.01 | 0.01 | 0.11 | 0.06 | |
| F7 | 0.05 | 0.05 | 0.06 | 0.02 | 0.08 | 0.05 | |
| F8 | 0.09 | 0.06 | 0.09 | 0.02 | 0.10 | 0.07 | |
| Cz | −0.01 | 0.02 | 0.00 | 0.00 | 0.09 | 0.05 | |
| C3 | 0.04 | 0.03 | 0.04 | 0.03 | 0.13 | 0.09 | |
| C4 | 0.01 | −0.01 | 0.01 | 0.00 | 0.11 | 0.06 | |
| Pz | 0.02 | 0.01 | 0.02 | 0.04 | 0.16 * | 0.11 | |
| P3 | 0.05 | 0.03 | 0.05 | 0.05 | 0.19 ** | 0.13 * | |
| P4 | 0.04 | 0.02 | 0.04 | 0.05 | 0.17* | 0.12 | |
| T3 | 0.04 | 0.08 | 0.06 | 0.00 | 0.09 | 0.05 | |
| T4 | 0.02 | 0.01 | 0.02 | 0.00 | 0.10 | 0.05 | |
| T5 | 0.12 | 0.08 | 0.12 | 0.06 | 0.19 ** | 0.14 * | |
| T6 | 0.08 | 0.02 | 0.07 | 0.08 | 0.16 * | 0.13 * | |
| O1 | 0.11 | 0.05 | 0.11 | 0.12 | 0.19 ** | 0.17 * | |
| O2 | 0.15 * | 0.04 | 0.14 * | 0.12 | 0.21 ** | 0.18 ** | |
| high- | Fz | 0.07 | 0.11 | 0.08 | 0.06 | 0.11 | 0.09 |
| beta | F3 | 0.08 | 0.10 | 0.09 | 0.07 | 0.12 | 0.10 |
| F4 | 0.04 | 0.08 | 0.06 | 0.06 | 0.12 | 0.10 | |
| F7 | 0.11 | 0.11 | 0.12 | 0.04 | 0.13 | 0.09 | |
| F8 | 0.14 * | 0.13 | 0.15 * | 0.08 | 0.15 * | 0.12 | |
| Cz | 0.06 | 0.11 | 0.08 | 0.07 | 0.14 * | 0.12 | |
| C3 | 0.06 | 0.12 | 0.08 | 0.05 | 0.13 | 0.10 | |
| C4 | 0.03 | 0.08 | 0.05 | 0.03 | 0.08 | 0.06 | |
| Pz | 0.05 | 0.08 | 0.06 | 0.04 | 0.16 * | 0.11 | |
| P3 | 0.05 | 0.09 | 0.07 | 0.05 | 0.13 | 0.10 | |
| P4 | 0.07 | 0.12 | 0.08 | 0.04 | 0.15 * | 0.11 | |
| T3 | 0.03 | 0.17 * | 0.07 | 0.03 | 0.06 | 0.05 | |
| T4 | 0.04 | 0.11 | 0.06 | 0.07 | 0.09 | 0.09 | |
| T5 | 0.14 * | 0.17 * | 0.16 * | 0.12 | 0.18 ** | 0.16 * | |
| T6 | 0.07 | 0.09 | 0.08 | 0.06 | 0.15 * | 0.11 | |
| O1 | 0.10 | 0.08 | 0.11 | 0.05 | 0.11 | 0.09 | |
| O2 | 0.07 | 0.06 | 0.07 | 0.01 | 0.11 | 0.06 | |
References
- John, E.R.; Karmel, B.Z.; Corning, W.C.; Easton, P.; Brown, D.; Ahn, H.; John, M.; Harmony, T.; Prichep, L.; Toro, A.; et al. Neurometrics: Numerical taxonomy identifies different profiles of brain functions within groups of behaviorally similar people. Science 1977, 196, 1393–1410. [Google Scholar] [CrossRef]
- John, E.R.; Prichep, L.S.; Easton, P. Normative data banks and neurometrics. Basic concepts, methods, results of norm construction, In Methods of Analysis of Brain Electrical and Magnetic Signals; Gevins, A.S., Remond, A., Eds.; Elsevier: Amsterdam, The Netherlands; New York, NY, USA, 1987; pp. 449–495. [Google Scholar]
- Sterman, M.B.; Kaiser, D. Comodulation: A new QEEG analysis metric for assessment of structural and functional disorders of the central nervous system. J. Neurother. 2001, 4, 73–83. [Google Scholar] [CrossRef] [Green Version]
- Bosch-Bayard, J.; Galan, L.; Aubert Vazquez, E.; Virues Alba, T.; Valdes-Sosa, P.A. Resting state healthy EEG: The first wave of the Cuban normative database. Front. Neurosci. 2020, 14, 555119. [Google Scholar] [CrossRef]
- Keizer, A.W. Standardization and personalized medicine using quantitative EEG in clinical settings. Clin. EEG Neurosci. 2021, 52, 82–89. [Google Scholar] [CrossRef]
- Ko, J.; Park, U.; Kim, D.; Kang, S.W. Quantitative electroencephalogram standardization: A sex-and age-differentiated normative database. Front. Neurosci. 2021, 15, 766781. [Google Scholar] [CrossRef]
- Thatcher, R.W.; Walker, R.A.; Biver, C.J.; North, D.N.; Curtin, R. Quantitative EEG normative databases: Validation and clinical correlation. J. Neurother. 2003, 7, 87–121. [Google Scholar] [CrossRef] [Green Version]
- Deslandes, A.; Veiga, H.; Cagy, M.; Fiszman, A.; Piedade, R.; Ribeiro, P. Quantitative electroencephalography (qEEG) to discriminate primary degenerative dementia from major depressive disorder (depression). Arq. Neuro-Psiquiatr. 2004, 62, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Siever, D.; Collura, T. Audio-visual entrainment: Physiological mechanisms and clinical outcomes. In Rhythmic Stimulation Procedures in Neuromodulation; Evans, J.R., Turner, R.P., Eds.; Academic Press: San Diego, CA, USA, 2017; pp. 51–95. [Google Scholar]
- Thatcher, R.W. Latest developments in live z-score training: Symptom check list, phase reset, and LORETA z-score biofeedback. J. Neurother. 2013, 17, 69–87. [Google Scholar] [CrossRef] [Green Version]
- Hammer, B.U.; Colbert, A.P.; Brown, K.A.; Ilioi, E.C. Neurofeedback for insomnia: A pilot study of z-score SMR and individualized protocols. Appl. Psychophysiol. Biofeedback 2011, 36, 251–264. [Google Scholar] [CrossRef]
- Martínez-Briones, B.J.; Bosch-Bayard, J.; Biscay-Lirio, R.J.; Silva-Pereyra, J.; Albarrán-Cárdenas, L.; Fernández, T. Effects of neurofeedback on the working memory of children with learning disorders-an EEG power-spectrum analysis. Brain Sci. 2021, 11, 957. [Google Scholar] [CrossRef]
- Bekker, M.; Balt, K.; Bipath, P.; Jordaan, J.; du Toit, P. The effect of infra-slow fluctuation neurofeedback training on a cohort of insomnia participants. NeuroRegulation 2021, 8, 137–148. [Google Scholar] [CrossRef]
- Thatcher, R.W.; Biver, C.J.; North, D.M. History and technical foundations of z score EEG biofeedback. In Z Score Neurofeedback; Thatcher, R.W., Lubar, J.F., Eds.; Academic Press: San Diego, CA, USA, 2015; pp. 1–21. [Google Scholar]
- Thatcher, R.W.; Lubar, J.F. History of the scientific standards of QEEG normative databases. In Introduction to Quantitative EEG and Neurofeedback: Advanced Theory and Applications; Budzynski, T.H., Budzynski, H.K., Evans, J.R., Abarbanel, A., Eds.; Academic Press: San Diego, CA, USA, 2009; pp. 29–59. [Google Scholar]
- Thatcher, R.W. Handbook of Quantitative Electroencephalography and EEG Biofeedback; ANI Publishing: Petersburg, Russia, 2016. [Google Scholar]
- Collura, T.F. Quantitative EEG and live z-score neurofeedback-current clinical and scientific context. Biofeedback 2017, 45, 25–29. [Google Scholar] [CrossRef]
- Lin, I.M.; Chen, T.C.; Lin, H.Y.; Wang, S.Y.; Sung, J.L.; Yen, C.W. Electroencephalogram patterns in patients comorbid with major depressive disorder and anxiety symptoms: Proposing a hypothesis based on hypercortical arousal and not frontal or parietal alpha asymmetry. J. Affect. Disord. 2021, 282, 945–952. [Google Scholar] [CrossRef]
- Lin, I.M.; Yu, H.E.; Yeh, Y.C.; Huang, M.F.; Wu, K.T.; Ke, C.L.K.; Lin, P.Y.; Yen, C.F. Prefrontal lobe and posterior cingulate cortex activations in patients with major depressive disorder by using standardized weighted low-resolution electromagnetic tomography. J. Pers. Med. 2021, 11, 1054. [Google Scholar] [CrossRef]
- Coutin-Churchman, P.; Anez, Y.; Uzcategui, M.; Alvarez, L.; Vergara, F.; Mendez, L.; Fleitas, R. Quantitative spectral analysis of EEG in psychiatry revisited: Drawing signs out of numbers in a clinical setting. Clin. Neurophysiol. 2003, 114, 2294–2306. [Google Scholar] [CrossRef]
- Grin-Yatsenko, V.A.; Baas, I.; Ponomarev, V.A.; Kropotov, J.D. EEG power spectra at early stages of depressive disorders. J. Clin. Neurophysiol. 2009, 26, 401–406. [Google Scholar] [CrossRef]
- Fingelkurts, A.A.; Fingelkurts, A.A.; Rytsälä, H.; Suominen, K.; Isometsä, E.; Kähkönen, S. Composition of brain oscillations in ongoing EEG during major depression disorder. Neurosci. Res. 2006, 56, 133–144. [Google Scholar] [CrossRef]
- Yadollahpour, A.; Nasrollahi, H. Quantitative electroencephalography for objective and differential diagnosis of depression: A comprehensive review. Glob. J. Health Sci. 2016, 8, 249–256. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, M.; Mori, T.; Endo, S. EEG power and coherence in presenile and senile depression. Characteristic findings related to differences between anxiety type and retardation type. Nihon Ika Daigaku Zasshi 1995, 62, 176–185. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.W.; Yu, Y.W.Y.; Chen, M.C.; Chen, T.J. Cortical mechanisms of the symptomatology in major depressive disorder: A resting EEG study. J. Affect. Disord. 2011, 131, 243–250. [Google Scholar] [CrossRef]
- Pizzagalli, D.A.; Nitschke, J.B.; Oakes, T.R.; Hendrick, A.M.; Horras, K.A.; Larson, C.L.; Abercrombie, H.C.; Schaefer, S.M.; Koger, J.V.; Benca, R.M.; et al. Brain electrical tomography in depression: The importance of symptom severity, anxiety, and melancholic features. Biol. Psychiatry 2002, 52, 73–85. [Google Scholar] [CrossRef]
- Saletu, B.; Anderer, P.; Saletu-Zyhlarz, G.M. EEG topography and tomography (LORETA) in diagnosis and pharmacotherapy of depression. Clin. EEG Neurosci. 2010, 41, 203–210. [Google Scholar] [CrossRef]
- Sachs, G.; Anderer, P.; Dantendorfer, K.; Saletu, B. EEG mapping in patients with social phobia. Psychiatry Res. 2004, 131, 237–247. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory Manual, 2nd ed.; Pyschologcial Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Chen, H.Y. Beck Depression Inventory Version II; Chinese Behavioral Science Corporation: Taipei, Taiwan, 2000. (In Chinese) [Google Scholar]
- Lu, M.L.; Che, H.H.; Chang, S.W.; Shen, W.W. Reliability and Validity of the Chinese Version of the Beck Depression Inventory-II. Taiwan. J. Psychiatry 2002, 16, 301–310. [Google Scholar]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef]
- Lin, Y.C. Beck Anxiety Inventory; Chinese Behavioral Science Corporation: Taipei, Taiwan, 2000. (In Chinese) [Google Scholar]
- Che, H.H.; Lu, M.L.; Chen, H.C.; Chang, S.W.; Lee, Y.J. Validation of the Chinese version of the Beck Anxiety Inventory. Formos. J. Med. 2006, 10, 447–454. [Google Scholar] [CrossRef]
- Cautin, R.L.; Lilienfeld, S.O. The Encyclopedia of Clinical Psychology; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Bruder, G.; Fong, R.; Tenke, C.E.; Leite, P.; Towey, J.P.; Stewart, J.E.; McGrath, P.J.; Quitkin, F.M. Regional brain asymmetries in major depression with or without an anxiety disorder: A quantitative electroencephalographic study. Biol. Psychiatry 1997, 41, 939–948. [Google Scholar] [CrossRef]
- Heller, W.; Etienne, M.A.; Miller, G.A. Patterns of perceptual asymmetry in depression and anxiety: Implications for neuropsychological models of emotion and psychopathology. J. Abnorm. Psychol. 1995, 104, 327–333. [Google Scholar] [CrossRef]
- Heller, W.; Nitschke, J.B.; Etienne, M.A.; Miller, G.A. Patterns of regional brain activity differentiate types of anxiety. J. Abnorm. Psychol. 1997, 106, 376. [Google Scholar] [CrossRef]
- Begić, D.; Popović-Knapić, V.; Grubišin, J.; Kosanović-Rajačić, B.; Filipčić, I.; Telarović, I.; Jakovljević, M. Quantitative electroencephalography in schizophrenia and depression. Psychiatr. Danub. 2011, 23, 355–362. [Google Scholar]
- Knott, V.; Mahoney, C.; Kennedy, S.; Evans, K. EEG power, frequency, asymmetry and coherence in male depression. Psychiatry Res. 2001, 106, 123–140. [Google Scholar] [CrossRef]
- Newson, J.J.; Thiagarajan, T.C. EEG frequency bands in psychiatric disorders: A review of resting state studies. Front. Hum. Neurosci. 2019, 12, 521. [Google Scholar] [CrossRef] [Green Version]
- Mumtaz, W.; Xia, L.; Ali, S.S.A.; Yasin, M.A.M.; Hussain, M.; Malik, A.S. Electroencephalogram (EEG)-based computer-aided technique to diagnose major depressive disorder (MDD). Biomed. Signal Process. Control. 2017, 31, 108–115. [Google Scholar] [CrossRef]
- Davidson, R.J. Anterior electrophysiological asymmetries, emotion, and depression: Conceptual and methodological conundrums. Psychophysiology 1998, 35, 607–614. [Google Scholar] [CrossRef]
- Henriques, J.B.; Davidson, R.J. Left frontal hypoactivation in depression. J. Abnorm. Psychol. 1991, 100, 535–545. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-5); The American Psychiatric Publishing: Washington, DC, USA, 2003. [Google Scholar]
- Arns, M.; Etkin, A.; Hegerl, U.; Williams, L.M.; DeBattista, C.; Palmer, D.M.; Fitzgerald, P.B.; Harris, A.; deBeuss, R.; Gordon, E. Frontal and rostral anterior cingulate (rACC) theta EEG in depression: Implications for treatment outcome? Eur. Neuropsychopharmacol. 2015, 25, 1190–1200. [Google Scholar] [CrossRef]



| John [1] | John [2] | Sterman & Kaiser [3] | Thatcher [7] | Bosch-Bayard [4] | Keizer [5] | Ko [6] | This Study | ||
|---|---|---|---|---|---|---|---|---|---|
| Country | USA | USA | USA | USA | Cuban | Netherlands | Koran | Taiwan | |
| Name of database | Neurometrics | BrainDx | SKIL/SKIL3 | NeuroGuide | qEEG pro | ISB-NormDB | |||
| FDA-approved | Yes | Yes | No | Yes | No | Yes | Yes (KFDA) | No | |
| Years of data collection | 1979−1987, 2000 | 1988−1990 | 2004−2013 | 2014−2019 | 2012−2022 | ||||
| Sample size | 782 | 464 | 135 SKIL/ 175 SKIL3 | EC625/EO625 in 2003; EC727/EC727 in 2013 | 211 | EC1482/ EO1232 | 1289 | 260 | |
| Age (y) | 6−90 | 16−80 | 18−55 | 2 months−82.6 | 5−80 | 6−83 | 4.5−81 | 20−70 | |
| Sex (M/F) | 108M/27F for SKIL | 355M/270F | 105M/106F | EC:955/527 EO:799/432 | 553M/ 736F | 130M/ 130F | |||
| Children, n (years old) | 356 (6−16) | 310 | 30 (6−11) SKIL3 | 458 (6−16) | 0 | ||||
| Adults, n (years old) | 426 (16−90) | 154 (16−80) | 135(18−55) SKIL/115 adults (20−75), 30 teenagers SKIL3 | 167(16−82)/ 155(14−82) | 260 (20−70) | ||||
| EEG placement | 10−20 | 10−20 | 10−20 | 10−20 | 10−20 | 10−20 | 10−20 | 10−20 | |
| Channels | 19 | 19 | 19 | 19 | 19 | 19 | 19 | 19 | |
| Reference | Linked-ear | Linked-ear | Linked-ear | Linked-ear | Monopolar linked ear | Linked-ear | Linked-ear | ||
| Sampling rate (Hz/s) | 256 | ≥ 100 | 256 | 128(8%) & 256(92%) | 250 | 256 | |||
| Impedance (KΩ) | 5 | 5 | 5 | 5,10 | 5 | 5 | 5 | ||
| EC/EO | EC | EC | EC/EO/Task | EC/EO | 5EC/3EO/ 3HV | EC/EO | 4EC/4EO | EC | |
| Recording time | 20−30 m resting state | 20−30 m resting state | 2−4 m resting state | 58.6 s−40 m | 10−12 m | 10 m resting state | 8 m resting state | 5 m resting state | |
| Frequency bands (Hz) | 0.5−25 | 0.5−50 | 1−20 | 0.3−30 | 0.5−30 | 1−45 | 1−45.5 | 1−40 | |
| delta | 1.5−3.5 | 1.5−3.5 | 1−3 | 1−3.5 | 1−4 | 1−3 | 1−4 | 1−4 | |
| theta | 3.5−7.5 | 3.5−7.5 | 3−7 | 3.5−7.5 | 4−8 | 4−7 | 4−8 | 4−8 | |
| alpha | 7.5−12.5 | 7.5−12.5 | 7−12 | 7.5−12.5 | 8−12 | 8−12 | 8−12 | 8−12 | |
| beta | 13.5−25 | 13.5−25 | 12−15 | 12.5−19 | 12−25 | 13−20 | 12−30 | 12−25 | |
| high-beta | Beat 2:25−35 | 15−20 | 25−30 | 21−30 | 25−30 | ||||
| Deartifacting | Manual | Manual | Manual/ Automatic | Manual | Manual | Automatic | Automatic | Manual | |
| HC Group (n = 260) | MDD Group (n = 221) | ||||
|---|---|---|---|---|---|
| M (SD) | M (SD) | t /χ2 | p | ||
| Age, years old | 40.63 (14.11) | 41.09 (14.02) | t = −0.35 | 0.726 | |
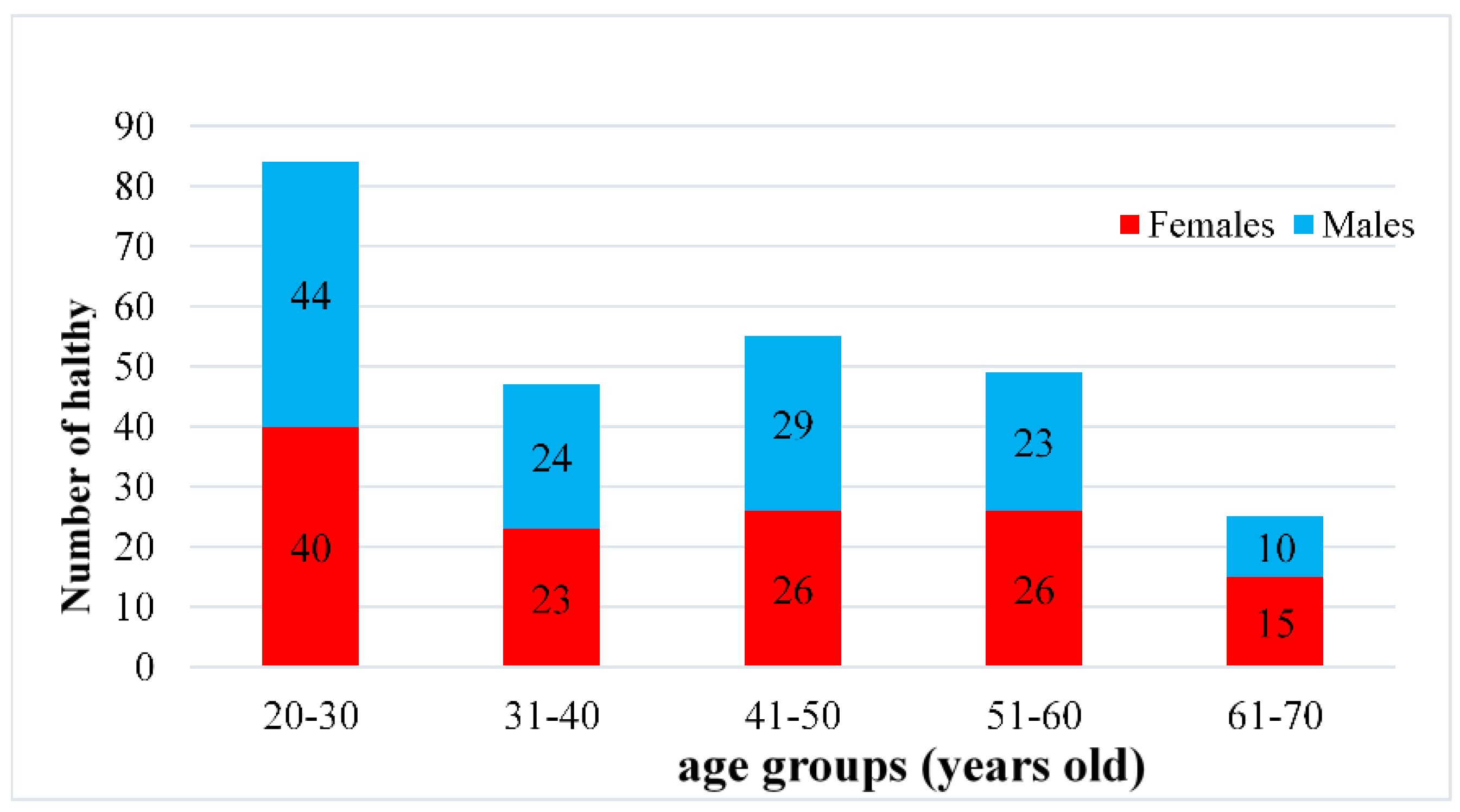
| 20–30, n (F/M) | 84 (40/44) | 65 (41/24) | |||
| 31–40, n (F/M) | 47 (23/24) | 39 (33/6) | |||
| 41–50, n (F/M) | 55 (26/29) | 55 (43/12) | |||
| 51–60, n (F/M) | 49 (26/23) | 37 (28/9) | |||
| 61–70, n (F/M) | 25 (15/10) | 25 (18/7) | |||
| Sex | Females (F) | 130 a | 163 b | χ 2 = 28.32 *** | <0.001 |
| Males (M) | 130 a | 58 b | |||
| Education | Primary school | 2 (0.76%) a | 6 (2.71%) a | χ 2 = 61.21 *** | <0.001 |
| Junior high school | 4 (1.54%) a | 20 (9.05%) b | |||
| Senior/vocation high school | 32 (12.31%) a | 66 (29.86%) b | |||
| Junior college | 33 (12.69%) a | 32 (14.48%) a | |||
| University | 113 (43.46%) a | 77 (34.84%) a | |||
| Graduate school | 76 (29.23%) a | 20 (9.05%) b | |||
| BDI-II | 4.23 (3.52) | 31.93 (10.50) | t = −37.47 *** | <0.001 | |
| BAI | 1.95 (1.93) | 22.28 (9.91) | t = −30.00 *** | <0.001 | |
| Frontal Lobe | Central Area | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Fz | F3 | F4 | F7 | F8 | Cz | C3 | C4 | ||
| delta | 0.83 *** | 0.89 *** | 0.88 *** | 0.81 *** | 0.88 *** | 0.90 *** | 0.90 *** | 0.90 *** | |
| theta | 0.84 *** | 0.85 *** | 0.84 *** | 0.83 *** | 0.85 *** | 0.86 *** | 0.85 *** | 0.86 *** | |
| alpha | 0.85 *** | 0.85 *** | 0.85 *** | 0.87 *** | 0.85 *** | 0.84 *** | 0.84 *** | 0.83 *** | |
| beta | 0.86 *** | 0.88 *** | 0.89 *** | 0.89 *** | 0.91 *** | 0.85 *** | 0.87 *** | 0.88 *** | |
| high-beta | 0.87 *** | 0.89 *** | 0.91 *** | 0.84 *** | 0.87 *** | 0.90 *** | 0.89 *** | 0.83 *** | |
| Parietal lobe | Temporal lobe | Occipital lobe | |||||||
| Pz | P3 | P4 | T3 | T4 | T5 | T6 | O1 | O2 | |
| delta | 0.90 *** | 0.92 *** | 0.88 *** | 0.87 *** | 0.86 *** | 0.89 *** | 0.87 *** | 0.82 *** | 0.88 *** |
| theta | 0.85 *** | 0.85 *** | 0.87 *** | 0.88 *** | 0.89 *** | 0.82 *** | 0.89 *** | 0.86 *** | 0.88 *** |
| alpha | 0.82 *** | 0.79 *** | 0.82 *** | 0.85 *** | 0.83 *** | 0.72 *** | 0.80 *** | 0.71 *** | 0.76 *** |
| beta | 0.87 *** | 0.86 *** | 0.89 *** | 0.90 *** | 0.90 *** | 0.86 *** | 0.88 *** | 0.83 *** | 0.85 *** |
| high-beta | 0.89 *** | 0.88 *** | 0.90 *** | 0.84 *** | 0.83 *** | 0.92 *** | 0.91 *** | 0.86 *** | 0.89 *** |
| Z-Scores | |||||
|---|---|---|---|---|---|
| Delta | Theta | Alpha | Beta | High-Beta | |
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |
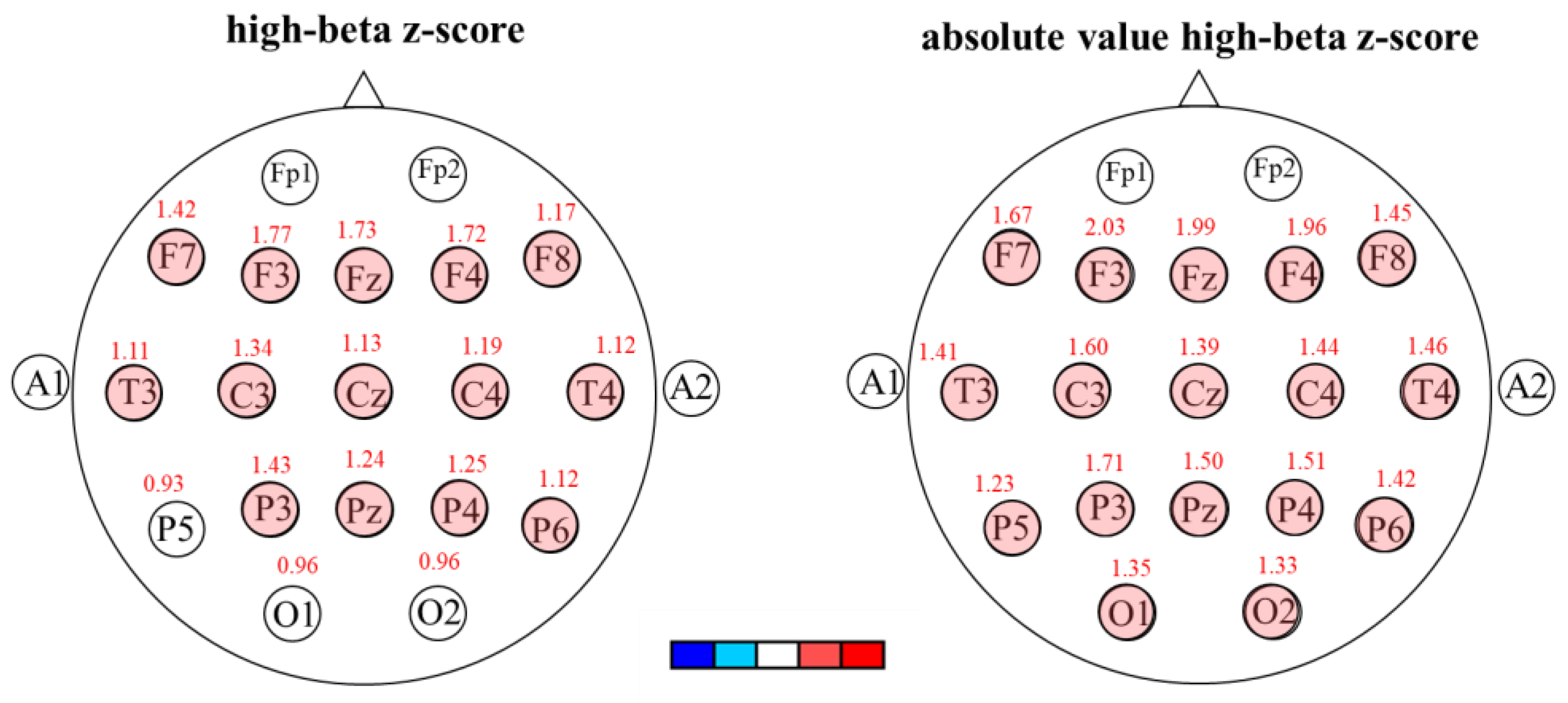
| Fz | −0.11(1.41) | −0.03(1.30) | 0.07(1.22) | 1.22(2.45) | 1.73(3.05) |
| F3 | −0.08(1.13) | −0.02(1.24) | 0.09(1.23) | 1.21(2.42) | 1.77(2.97) |
| F4 | −0.17(1.04) | −0.03(1.30) | 0.06(1.24) | 1.26(2.54) | 1.72(2.89) |
| F7 | −0.08(1.12) | −0.06(1.12) | 0.06(1.14) | 1.02(1.94) | 1.42(2.43) |
| F8 | −0.15(1.01) | −0.10(1.17) | 0.03(1.21) | 0.90(1.98) | 1.17(2.22) |
| Cz | −0.18(0.99) | −0.06(1.20) | 0.05(1.23) | 1.12(2.48) | 1.13(2.10) |
| C3 | −0.15(1.00) | −0.01(1.23) | 0.08(1.26) | 0.86(1.93) | 1.34(2.44) |
| C4 | −0.16(1.02) | 0.00(1.29) | 0.11(1.25) | 0.88(2.00) | 1.19(2.46) |
| Pz | −0.09(1.08) | −0.05(1.00) | 0.02(1.16) | 0.72(1.99) | 1.24(2.39) |
| P3 | −0.11(1.08) | −0.04(1.03) | 0.05(1.25) | 0.67(1.84) | 1.43(2.93) |
| P4 | −0.09(1.10) | −0.02(1.03) | 0.06(1.23) | 0.70(1.87) | 1.25(2.41) |
| T3 | −0.20(0.89) | −0.04(1.20) | 0.12(1.24) | 0.95(1.91) | 1.11(2.16) |
| T4 | −0.19(1.20) | −0.11(1.17) | 0.06(1.25) | 0.93(2.08) | 1.12(2.34) |
| T5 | −0.16(0.97) | −0.03(1.28) | 0.09(1.53) | 0.67(1.78) | 0.93(1.85) |
| T6 | −0.10(1.04) | 0.03(1.25) | 0.14(1.52) | 0.95(2.33) | 1.12(2.01) |
| O1 | −0.02(1.59) | 0.00(1.04) | 0.08(1.46) | 0.67(1.91) | 0.96(2.19) |
| O2 | −0.08(0.94) | −0.03(0.89) | 0.07(1.24) | 0.57(1.61) | 0.96(2.12) |
| Absolute value z-scores | |||||
| delta | theta | alpha | beta | high-beta | |
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | |
| |Fz| | 0.86(1.13) | 0.77(1.05) | 0.87(0.87) | 1.60(2.22) | 1.99(2.89) |
| |F3| | 0.77(0.83) | 0.74(0.99) | 0.87(0.88) | 1.57(2.20) | 2.03(2.80) |
| |F4| | 0.75(0.73) | 0.77(1.04) | 0.87(0.88) | 1.62(2.33) | 1.96(2.72) |
| |F7| | 0.78(0.81) | 0.68(0.90) | 0.80(0.81) | 1.30(1.77) | 1.67(2.27) |
| |F8| | 0.77(0.66) | 0.73(0.92) | 0.84(0.87) | 1.25(1.77) | 1.45(2.05) |
| |Cz| | 0.75(0.68) | 0.74(0.94) | 0.85(0.88) | 1.51(2.27) | 1.39(1.93) |
| |C3| | 0.73(0.69) | 0.74(0.98) | 0.85(0.93) | 1.24(1.70) | 1.60(2.27) |
| |C4| | 0.71(0.75) | 0.79(1.03) | 0.84(0.94) | 1.26(1.78) | 1.44(2.33) |
| |Pz| | 0.78(0.75) | 0.65(0.76) | 0.80(0.84) | 1.19(1.74) | 1.50(2.23) |
| |P3| | 0.78(0.75) | 0.66(0.79) | 0.81(0.95) | 1.13(1.60) | 1.71(2.78) |
| |P4| | 0.76(0.81) | 0.69(0.77) | 0.83(0.91) | 1.14(1.63) | 1.51(2.26) |
| |T3| | 0.71(0.57) | 0.76(0.93) | 0.80(0.96) | 1.32(1.68) | 1.41(1.98) |
| |T4| | 0.84(0.87) | 0.77(0.89) | 0.82(0.95) | 1.36(1.83) | 1.46(2.15) |
| |T5| | 0.71(0.67) | 0.71(1.06) | 0.85(1.27) | 1.06(1.58) | 1.23(1.67) |
| |T6| | 0.75(0.73) | 0.83(0.92) | 0.95(1.19) | 1.39(2.10) | 1.42(1.81) |
| |O1| | 0.85(1.35) | 0.68(0.78) | 0.80(1.22) | 1.17(1.65) | 1.35(1.97) |
| |O2| | 0.65(0.68) | 0.61(0.65) | 0.79(0.96) | 1.04(1.35) | 1.33(1.91) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.-C.; Lin, I.-M. The Resting State of Taiwan EEG Normative Database: Z-Scores of Patients with Major Depressive Disorder as the Cross-Validation. Brain Sci. 2023, 13, 351. https://doi.org/10.3390/brainsci13020351
Wu Y-C, Lin I-M. The Resting State of Taiwan EEG Normative Database: Z-Scores of Patients with Major Depressive Disorder as the Cross-Validation. Brain Sciences. 2023; 13(2):351. https://doi.org/10.3390/brainsci13020351
Chicago/Turabian StyleWu, Yin-Chen, and I-Mei Lin. 2023. "The Resting State of Taiwan EEG Normative Database: Z-Scores of Patients with Major Depressive Disorder as the Cross-Validation" Brain Sciences 13, no. 2: 351. https://doi.org/10.3390/brainsci13020351