
Usefulness and Reliability of the Bispectral Index during Balanced Anesthesia for Neurovascular Surgery in New Zealand White Rabbits
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Animals
2.3. Anesthetic Management
2.4. Bis Positioning and Recording
- Time point 0 (TP0): depth of anesthesia deemed adequate to maintain the trachea intubated in absence of surgical stimuli.
- Time point 1 (TP1): depth of anesthesia deemed adequate to start the surgery.
- Time point 2 (TP2): surgical incision.
- Time point 3 (TP3): 1 min after right carotid clamping (RCC).
- Time point 4 (TP4): 1 min after left carotid clamping (LCC).
- Time point 4A (TP4A): 1 min after left carotid opening (LCO).
- Time point 5 (TP5): end of surgery.
- Time point 6 (TP6): end of anesthesia (ETIso 0.3%).
- Time point 7 (TP7): tracheal extubation.
2.5. Antinociception
2.6. Statistical Analysis
3. Results
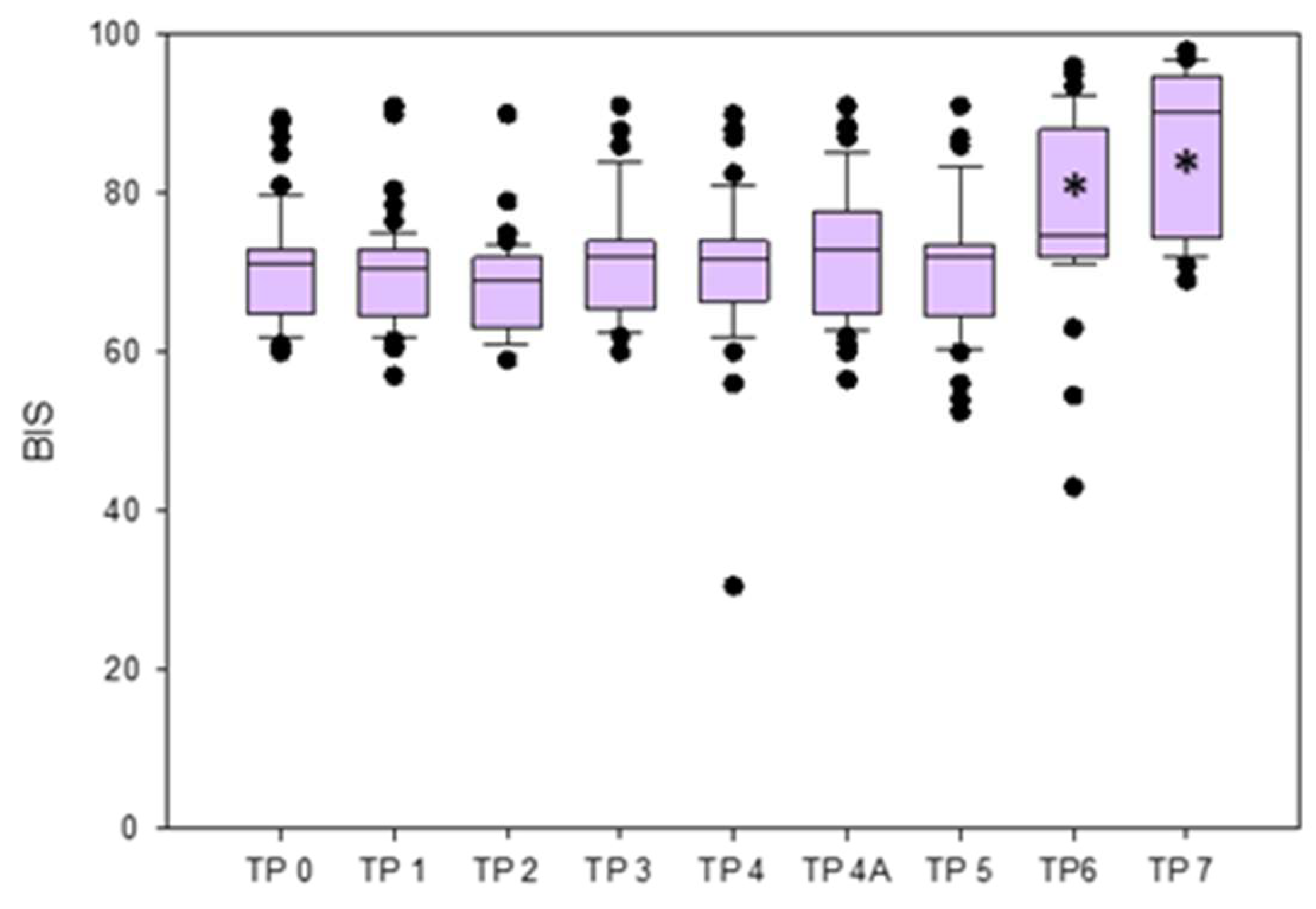
- The BIS was significantly lower at TPs 0, 1, 2, 3, 4, 4A, and 5 compared to TP7, and at TPs 0, 1, 2, 3, 4, 4A, and 5 compared to TP 6. No significant differences were found between TP3 (RCC) and TP4 (LCC), and between TP4 (LCC) and TP4A (LCO) when analyzed separately (Figure 3).
- The EMG values were significantly lower at TPs 0, 1, 2, 3, 4, 4A, 5, and 6 compared to TP7, and at TPs 2, 3, 4, 4A, and 5 compared to TP0. Values were significantly lower at TPs 3, 4, 4a, and 5 compared to TP6, while those at TPs 3, 4, 4A were significantly lower compared to TP1.
- The BSR remained 0 in all rabbits at all TPs, except for one rabbit that showed a sudden increase of BSR (value 44), accompanied by a BIS decrease, immediately after the LCC (TP4).
- The SQI results are reported in Supplementary Materials (Table S1).

4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Constant, I.; Sabourdin, N. Monitoring Depth of Anesthesia: From Consciousness to Nociception. A Window on Subcortical Brain Activity. Pediatr. Anesthesia 2015, 25, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Short, T.G.; Campbell, D.; Frampton, C.; Chan, M.T.V.; Myles, P.S.; Corcoran, T.B.; Sessler, D.I.; Mills, G.H.; Cata, J.P.; Painter, T.; et al. Anaesthetic Depth and Complications after Major Surgery: An International, Randomised Controlled Trial. Lancet 2019, 394, 1907–1914. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.; Antunes, L. Electroencephalogram-Based Anaesthetic Depth Monitoring in Laboratory Animals. Lab. Anim. 2012, 46, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Bruhn, J.; Myles, P.S.; Sneyd, R.; Struys, M.M.R.F. Depth of Anaesthesia Monitoring: What’s Available, What’s Validated and What’s Next? Br. J. Anaesth. 2006, 97, 85–94. [Google Scholar] [CrossRef]
- Johansen, J.W.; Sebel, P.S.; Fisher, D.M. Development and Clinical Application of Electroencephalographic Bispectrum Monitoring. Anesthesiology 2000, 93, 1336–1344. [Google Scholar] [CrossRef]
- Rampil, I.J. A Primer for EEG Signal Processing in Anesthesia. Anesthesiology 1998, 89, 980–1002. [Google Scholar] [CrossRef]
- Sigl, J.C.; Chamoun, N.G. An Introduction to Bispectral Analysis for the Electroencephalogram. J. Clin. Monit. Comput. 1994, 10, 392–404. [Google Scholar] [CrossRef]
- Monk, T.G.; Weldon, B.C. Does Depth of Anesthesia Monitoring Improve Postoperative Outcomes? Curr. Opin. Anaesthesiol. 2011, 24, 665–670. [Google Scholar] [CrossRef]
- Campagnol, D.; Neto, F.J.T.; Monteiro, E.R.; Beier, S.L.; Aguiar, A.J.A. Use of Bispectral Index to Monitor Depth of Anesthesia in Isoflurane-Anesthetized Dogs. Am. J. Vet. Res. 2007, 68, 1300–1307. [Google Scholar] [CrossRef]
- March, P.A.; Muir, W.W. Bispectral Analysis of the Electroencephalogram: A Review of Its Development and Use in Anesthesia. Veter. Anaesth. Analg. 2005, 32, 241–255. [Google Scholar] [CrossRef]
- Martín-Cancho, M.F.; Lima, J.R.; Luis, L.; Crisóstomo, V.; Carrasco-Jiménez, M.S.; Usón-Gargallo, J. Relationship of Bispectral Index Values, Haemodynamic Changes and Recovery Times during Sevoflurane or Propofol Anaesthesia in Rabbits. Lab. Anim. 2006, 40, 28–42. [Google Scholar] [CrossRef]
- Romanov, A.; Moon, R.-S.; Wang, M.; Joshi, S. Paradoxical Increase in the Bispectral Index during Deep Anesthesia in New Zealand White Rabbits. J. Am. Assoc. Lab. Anim. Sci. 2014, 53, 74–80. [Google Scholar]
- Saritas, Z.K.; Korkmaz, M.; Saritas, T.B.; Sivaci, G.R. Comparison of the Depth of Anesthesia Produced with Dexmedetomidine-Sevoflurane or Medetomidine-Sevoflurane by Using Bispectral Index Monitoring. Acta Sci. Vet. 2014, 42, 1–8. [Google Scholar]
- Silva, A.; Campos, S.; Monteiro, J.; Venâncio, C.; Costa, B.; de Pinho, P.G.; Antunes, L. Performance of Anesthetic Depth Indexes in Rabbits under Propofol Anesthesia. Anesthesiology 2011, 115, 303–314. [Google Scholar] [CrossRef]
- Saritas, T.B.; Saritas, Z.K.; Korkmaz, M.; Sivaci, G.R. Comparison of Bispectral Index and Vital Parameters in Rabbits Receiving Propofol or Isoflurane Anesthesia. Acta Sci. Vet. 2013, 1137, 1–8. [Google Scholar]
- Haga, H.A.; Tevik, A.; Moerch, H. Bispectral Index as an Indicator of Anaesthetic Depth during Isoflurane Anaesthesia in the Pig. Vet. Anaesth. Analg. 1999, 26, 3–7. [Google Scholar] [CrossRef]
- Greene, S.A.; Benson, G.J.; Tranquilli, W.J.; Grimm, K.A. Effect of Isoflurane, Atracurium, Fentanyl, and Noxious Stimulation on Bispectral Index in Pigs. Comp. Med. 2004, 54, 397–403. [Google Scholar]
- Haga, H.A.; Dolvik, N.I. Evaluation of the Bispectral Index as an Indicator of Degree of Central Nervous System Depression in Isoflurane-Anesthetized Horses. Am. J. Vet. Res. 2002, 63, 438–442. [Google Scholar] [CrossRef]
- Yamashita, K.; Akashi, N.; Katayama, Y.; Uchida, Y.; Umar, M.A.; Itami, T.; Inoue, H.; Sams, R.A.; Muir, W.W. III. Evaluation of Bispectral Index (BIS) as an Indicator of Central Nervous System Depression in Horses Anesthetized with Propofol. J. Vet. Med. Sci. 2009, 71, 1465–1471. [Google Scholar] [CrossRef]
- Navarrete-Calvo, R.; Morgaz, J.; Gómez-Villamandos, R.J.; Quirós-Carmona, S.; Domínguez, J.M.; Ruiz-López, P.; Granados, M.M. Comparison of Bispectral Index and Spectral Entropy during Isoflurane and Medetomidine General Anaesthesia in Horses. Equine Vet. J. 2020, 52, 678–684. [Google Scholar] [CrossRef]
- Antognini, J.F.; Wang, X.W.; Carstens, E. Isoflurane Anaesthetic Depth in Goats Monitored Using the Bispectral Index of the Electroencephalogram. Vet. Res. Commun. 2000, 24, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Martin-Jurado, O.; Vogt, R.; Kutter, A.P.N.; Bettschart-Wolfensberger, R.; Hatt, J.-M. Effect of Inhalation of Isoflurane at End-Tidal Concentrations Greater than, Equal to, and Less than the Minimum Anesthetic Concentration on Bispectral Index in Chickens. Am. J. Vet. Res. 2008, 69, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Bard, J.W. The BIS Monitor: A Review and Technology Assessment. AANA J. 2001, 69, 477–483. [Google Scholar] [PubMed]
- Boztu, N.; Bigat, Z.; Akyuz, M.; Demir, S.; Ertok, E. Does Using the Bispectral Index (BIS) During Craniotomy Affect the Quality of Recovery? J. Neurosurg. Anesthesiol. 2006, 18, 1–4. [Google Scholar] [CrossRef]
- Myles, P.S.; Daly, D.; Silvers, A.; Cairo, S. Prediction of Neurological Outcome Using Bispectral Index Monitoring in Patients with Severe Ischemic-Hypoxic Brain Injury Undergoing Emergency Surgery. Anesthesiology 2009, 110, 1106–1115. [Google Scholar] [CrossRef]
- Estruch-Pérez, M.J.; Ausina-Aguilar, A.; Barberá-Alacreu, M.; Sánchez-Morillo, J.; Solaz-Roldán, C.; Morales-Suárez-Varela, M.M. Bispectral Index Changes in Carotid Surgery. Ann. Vasc. Surg. 2010, 24, 393–399. [Google Scholar] [CrossRef]
- McGrail, K.M. Intraoperative Use of Electroencephalography as an Assessment of Cerebral Blood Flow. Neurosurg. Clin. N. Am. 1996, 7, 685–692. [Google Scholar] [CrossRef]
- Mérat, S.; Lévecque, J.-P.; Gulluche, Y.L.; Diraison, Y.; Brinquin, L.; Hoffmann, J.-J. Intérêt Potentiel Du BIS Pour Détecter Une Souffrance Cérébrale Importante. Can. J. Anaesth. 2001, 48, 1066. [Google Scholar] [CrossRef]
- Wanderer, S.; Waltenspuel, C.; Grüter, B.E.; Strange, F.; Sivanrupan, S.; Remonda, L.; Widmer, H.R.; Casoni, D.; Andereggen, L.; Fandino, J.; et al. Arterial Pouch Microsurgical Bifurcation Aneurysm Model in the Rabbit. J. Vis. Exp. 2020, 159, e61157. [Google Scholar] [CrossRef]
- Marbacher, S.; Erhardt, S.; Schläppi, J.-A.; Coluccia, D.; Remonda, L.; Fandino, J.; Sherif, C. Complex Bilobular, Bisaccular, and Broad-Neck Microsurgical Aneurysm Formation in the Rabbit Bifurcation Model for the Study of Upcoming Endovascular Techniques. Am. J. Neuroradiol. 2011, 32, 772–777. [Google Scholar] [CrossRef]
- Fan, J.; Chen, Y.; Yan, H.; Niimi, M.; Wang, Y.; Liang, J. Principles and Applications of Rabbit Models for Atherosclerosis Research. J. Atheroscler. Thromb. 2017, 25, RV17018. [Google Scholar] [CrossRef]
- Boillat, G.; Franssen, T.; Wanderer, S.; Rey, J.; Casoni, D.; Andereggen, L.; Marbacher, S.; Gruter, B.E. Anatomical Variations of the Common Carotid Arteries and Neck Structures of the New Zealand White Rabbit and Its Implication for the Development of Preclinical Extracranial Aneurysm Models. Brain Sci. 2023, 13, 222. [Google Scholar] [CrossRef]
- Lysakowski, C.; Dumont, L.; Pellégrini, M.; Clergue, F.; Tassonyi, E. Effects of Fentanyl, Alfentanil, Remifentanil and Sufentanil on Loss of Consciousness and Bispectral Index during Propofol Induction of Anaesthesia. Br. J. Anaesth. 2001, 86, 523–527. [Google Scholar] [CrossRef]
- Nakayama, M.; Ichinose, H.; Yamamoto, S.; Kanaya, N.; Namiki, A. The Effect of Fentanyl on Hemodynamic and Bispectral Index Changes during Anesthesia Induction with Propofol. J. Clin. Anesth. 2002, 14, 146–149. [Google Scholar] [CrossRef]
- Murphy, K.L.; Roughan, J.V.; Baxter, M.G.; Flecknell, P.A. Anaesthesia with a Combination of Ketamine and Medetomidine in the Rabbit: Effect of Premedication with Buprenorphine. Vet. Anaesth. Analg. 2010, 37, 222–229. [Google Scholar] [CrossRef]
- Monte, V.D.; Staffieri, F.; Meo, A.D.; Vannucci, J.; Bufalari, A. Comparison of Ketamine–Dexmedetomidine–Methadone and Tiletamine–Zolazepam–Methadone Combinations for Short-Term Anaesthesia in Domestic Pigs. Vet. J. 2015, 205, 364–368. [Google Scholar] [CrossRef]
- Schnellbacher, R.W.; Carpenter, J.W.; Mason, D.E.; KuKanich, B.; Beaufrère, H.; Boysen, C. Effects of Lidocaine Administration via Continuous Rate Infusion on the Minimum Alveolar Concentration of Isoflurane in New Zealand White Rabbits (Oryctolagus Cuniculus). Am. J. Vet. Res. 2013, 74, 1377–1384. [Google Scholar] [CrossRef]
- Corrêa, J.M.X.; Niella, R.V.; de Oliveira, J.N.S.; Junior, A.C.S.; Marques, C.S.d.C.; Pinto, T.M.; da Silva, E.B.; Beier, S.L.; Silva, F.L.; de Lavor, M.S.L. Antinociceptive and Analgesic Effect of Continuous Intravenous Infusion of Maropitant, Lidocaine and Ketamine Alone or in Combination in Cats Undergoing Ovariohysterectomy. Acta Vet. Scand. 2021, 63, 49. [Google Scholar] [CrossRef]
- Soares, P.C.L.R.; Corrêa, J.M.X.; Niella, R.V.; de Oliveira, J.N.S.; Costa, B.A.; Junior, A.C.S.; Sena, A.S.; Pinto, T.M.; Munhoz, A.D.; Martins, L.A.F.; et al. Continuous Infusion of Ketamine and Lidocaine Either with or without Maropitant as an Adjuvant Agent for Analgesia in Female Dogs Undergoing Mastectomy. Vet. Med. Int. 2021, 2021, 4747301. [Google Scholar] [CrossRef]
- Bazin, P.; Padley, J.; Ho, M.; Stevens, J.; Ben-Menachem, E. The Effect of Intravenous Lidocaine Infusion on Bispectral Index during Major Abdominal Surgery. J. Clin. Monit. Comput. 2018, 32, 533–539. [Google Scholar] [CrossRef]
- Renna, M.; Wigmore, T.; Mofeez, A.; Gillbe, C. Biasing Effect of The Electromyogram nn Bis: A Controlled Study During High-Dose Fentanyl Induction. J. Clin. Monit. Comput. 2002, 17, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Sharbrough, F.M.; Messick, J.M.; Sundt, T.M. Correlation of Continuous Electroencephalograms with Cerebral Blood Flow Measurements During Carotid Endarterectomy. Stroke 1973, 4, 674–683. [Google Scholar] [CrossRef]
- Bonhomme, V.; Desiron, Q.; Lemineur, T.; Brichant, J.F.; Dewandre, P.-Y.; Hans, P. Bispectral Index Profile During Carotid Cross Clamping. J. Neurosurg. Anesth. 2007, 19, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Deogaonkar, A.; Vivar, R.; Bullock, R.E.; Price, K.; Chambers, I.; Mendelow, A.D. Bispectral Index Monitoring May Not Reliably Indicate Cerebral Ischaemia during Awake Carotid Endarterectomy. Br. J. Anaesth. 2005, 94, 800–804. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.X. Bilateral Bispectral Index Monitoring to Detect Cerebral Hypoperfusion during Carotid Endarterectomy under General Anesthesia. Saudi J. Anaesth. 2018, 12, 125–127. [Google Scholar] [CrossRef]
- Clute, H.L.; Levy, W.J. Electroencephalographic Changes During Brief Cardiac Arrest in Humans. Anesthesiology 1990, 73, 821–825. [Google Scholar] [CrossRef]
- Scremin, O.U.; Sonnenschein, R.R.; Rubinstein, E.H. Cerebrovascular Anatomy and Blood Flow Measurements in the Rabbit. J. Cereb. Blood Flow Metab. 1982, 2, 55–66. [Google Scholar] [CrossRef]
- Bruhn, J.; Bouillon, T.W.; Shafer, S.L. Electromyographic Activity Falsely Elevates the Bispectral Index. Anesthesiology 2000, 92, 1485–1487. [Google Scholar] [CrossRef]
- Jensen, E.W.; Litvan, H.; Struys, M.; Vazquez, P.M. Pitfalls and Challenges When Assessing the Depth of Hypnosis during General Anaesthesia by Clinical Signs and Electronic Indices. Acta Anaesthesiol. Scand. 2004, 48, 1260–1267. [Google Scholar] [CrossRef]
- Kim, D.; Yoo, J.; Kim, J.-Y.; Ahn, S.; Kim, S.; Min, S. Influence of Electrocautery-Induced Electromagnetic Interference on Quantitative Electroencephalographic Monitoring of Hypnosis during General Anesthesia: Comparison between the ADMS® and the BIS VISTATM. Korean J. Anesthesiol. 2018, 71, 368–373. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, B.-C.; Kim, Y.H. Falsely Increased Bispectral Index Values by Convective Air Warming System during Kidney Transplantation. Pak. J. Med Sci. 2016, 32, 793–795. [Google Scholar] [CrossRef]
- Vivien, B.; Maria, S.D.; Ouattara, A.; Langeron, O.; Coriat, P.; Riou, B. Overestimation of Bispectral Index in Sedated Intensive Care Unit Patients Revealed by Administration of Muscle Relaxant. Anesthesiology 2003, 99, 9–17. [Google Scholar] [CrossRef]
- Riker, R.R.; Fraser, G.L.; Simmons, L.E.; Wilkins, M.L. Validating the Sedation-Agitation Scale with the Bispectral Index and Visual Analog Scale in Adult ICU Patients after Cardiac Surgery. Intensive Care Med. 2001, 27, 853–858. [Google Scholar] [CrossRef]
- Coleman, R.M.; Tousignant-Laflamme, Y.; Ouellet, P.; Parenteau-Goudreault, É.; Cogan, J.; Bourgault, P. The Use of the Bispectral Index in the Detection of Pain in Mechanically Ventilated Adults in the Intensive Care Unit: A Review of the Literature. Pain Res. Manag. 2015, 20, e33–e37. [Google Scholar] [CrossRef]
- Brocas, E.; Dupont, H.; Paugam-Burtz, C.; Servin, F.; Mantz, J.; Desmonts, J.-M. Bispectral Index Variations during Tracheal Suction in Mechanically Ventilated Critically Ill Patients: Effect of an Alfentanil Bolus. Intensive Care Med. 2002, 28, 211–213. [Google Scholar] [CrossRef]
- Guignard, B.; Menigaux, C.; Dupont, X.; Fletcher, D.; Chauvin, M. The Effect of Remifentanil on the Bispectral Index Change and Hemodynamic Responses After Orotracheal Intubation. Anesth. Analg. 2000, 90, 161–167. [Google Scholar] [CrossRef]
- García, P.S.; Kreuzer, M.; Hight, D.; Sleigh, J.W. Effects of Noxious Stimulation on the Electroencephalogram during General Anaesthesia: A Narrative Review and Approach to Analgesic Titration. Br. J. Anaesth. 2021, 126, 445–457. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time Point | ETIso | BIS | EMG | BSR | ||
|---|---|---|---|---|---|---|
| TP0 | 0.49 (0.37–0.65) | 71 (65–73) | TP0 vs. TP7 p < 0.001 TP0 vs. TP6 p < 0.001 | 43 (41.2–44) | TP0 vs. TP7 p = 0.037 | 0 (0–0) |
| TP1 | 0.76 (0.64–0.99) | 70.5 (64.5–73) | TP1 vs. TP7 p < 0.001 TP1 vs. TP6 p < 0.001 | 42 (40.5–42) | TP1 vs. TP7 p < 0.001 | 0 (0–0) |
| TP2 | 0.93 (0.69–1.17) | 69 (63–72) | TP2 vs. TP7 p < 0.001 TP2 vs. TP6 p < 0.001 | 41 (40–42) | TP2 vs. TP7 p < 0.001 TP2 vs. TP6 p = 0.029 | 0 (0–0) |
| TP3 | 1.29 (1.03–1.39) | 72 (65.5–74) | TP3 vs. TP7 p < 0.001 TP3 vs. TP6 p < 0.001 | 39 (38–40) | TP3 vs. TP7 p < 0.001 TP3 vs. TP6 p < 0.001 TP3 vs. TP0 p < 0.001 | 0 (0–0) |
| TP4 | 1.36 (1.16–1.45) | 71.7 (66.5–74) | TP4 vs. TP7 p < 0.001 TP4 vs. TP6 p < 0.001 | 38 (37–39) | TP4 vs. TP7 p < 0.001 TP3 vs. TP6 p < 0.001 TP4 vs. TP0 p < 0.001 | 0 (0–0) |
| TP4A | 1.34 (1.28–1.41) | 73 (64.7–77.7) | TP4A vs. TP6 p = 0.019 | 38 (36–40) | TP4A vs. TP7 p < 0.001 TP4A vs. TP6 p < 0.001 TP4 vs. TP0 p < 0.001 | 0 (0–0) |
| TP5 | 1.31 (1.27–1.39) | 72 (64.5–73.6) | TP5 vs. TP7 p < 0.001 TP5 vs. TP6 p < 0.001 | 40 (38–44) | TP5 vs. TP7 p < 0.001 TP5 vs. TP6 p = 0.046 TP5 vs. TP0 p = 0.007 | 0 (0–0) |
| TP6 | 0.3 | 74.7 (72–88.1) | 43 (40–47.2) | TP6 vs. TP7 p < 0.005 | 0 (0–0) | |
| TP7 | 0 | 90.2 (74.5–94.7) | 49 (47–52) | 0 (0–0) | ||
| Fentanyl Bolus (n = 61) | Before | After |
|---|---|---|
| BIS | 73 (68.3–83.6) | 72 (64.8–81.1) A |
| EMG | 39 (38–40) | 39 (38–40) |
| SQI | 95 (87.5–97) | 95.5 (87–98.5) |
| BSR | 0 (0–0) | 0 (0–0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrucci, M.; Spadavecchia, C.; Wanderer, S.; Boillat, G.; Marbacher, S.; García Casalta, L.G.; Casoni, D. Usefulness and Reliability of the Bispectral Index during Balanced Anesthesia for Neurovascular Surgery in New Zealand White Rabbits. Brain Sci. 2023, 13, 327. https://doi.org/10.3390/brainsci13020327
Petrucci M, Spadavecchia C, Wanderer S, Boillat G, Marbacher S, García Casalta LG, Casoni D. Usefulness and Reliability of the Bispectral Index during Balanced Anesthesia for Neurovascular Surgery in New Zealand White Rabbits. Brain Sciences. 2023; 13(2):327. https://doi.org/10.3390/brainsci13020327
Chicago/Turabian StylePetrucci, Mariafrancesca, Claudia Spadavecchia, Stefan Wanderer, Gwendoline Boillat, Serge Marbacher, Luisana Gisela García Casalta, and Daniela Casoni. 2023. "Usefulness and Reliability of the Bispectral Index during Balanced Anesthesia for Neurovascular Surgery in New Zealand White Rabbits" Brain Sciences 13, no. 2: 327. https://doi.org/10.3390/brainsci13020327