
Needs and Quality of Life of Caregivers of Patients with Prolonged Disorders of Consciousness

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
1.1. Impact of Prolonged Disorders of Consciousness on Caregivers
1.2. Impact of the Caregiver’s Profile
1.3. Impact of the Patient’s Profile
1.4. Objectives
2. Methods
2.1. Recruitment
2.2. Assessments
2.3. Statistical Analyses
3. Results
3.1. Description of the Sample
3.1.1. Socio-Demographic Variables
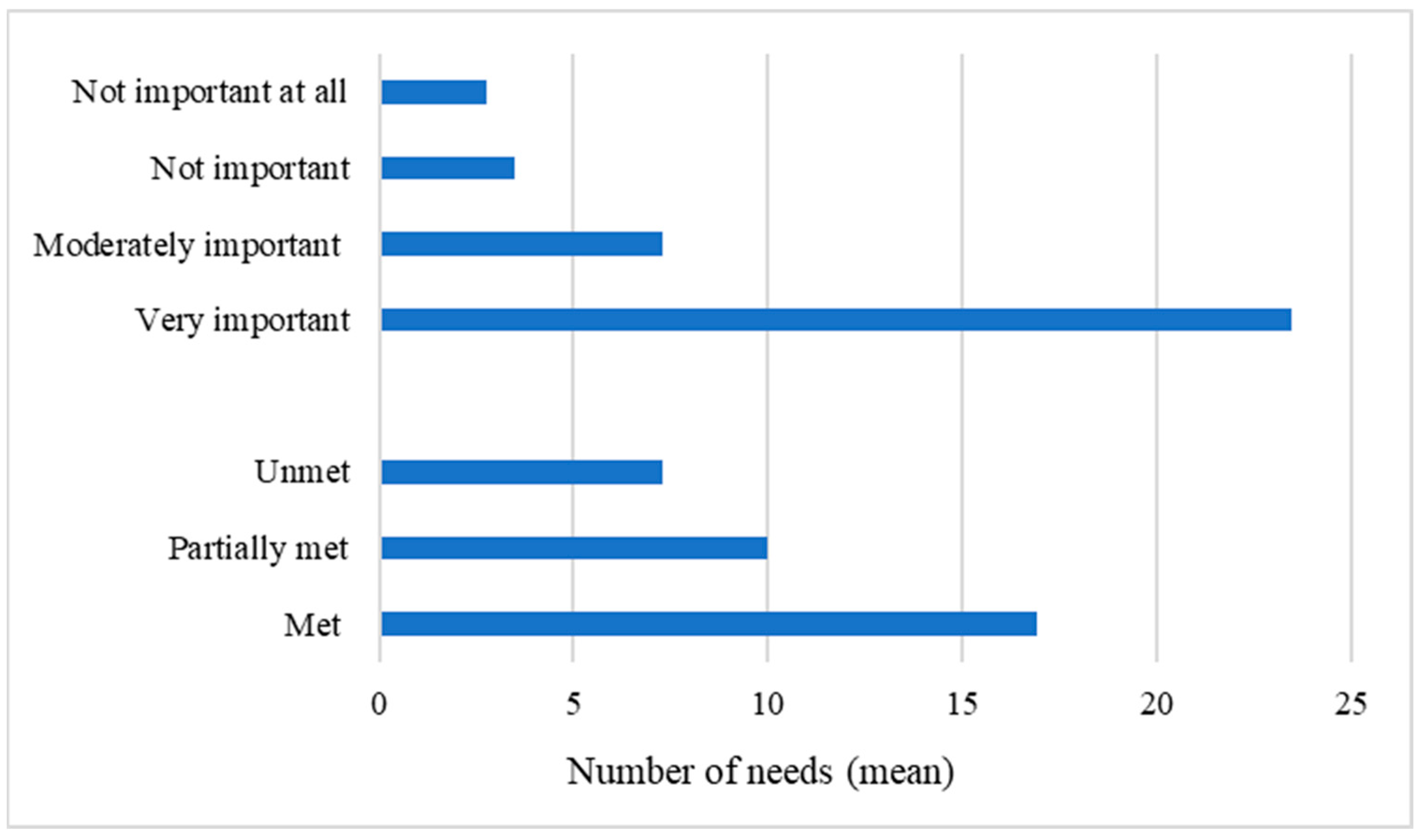
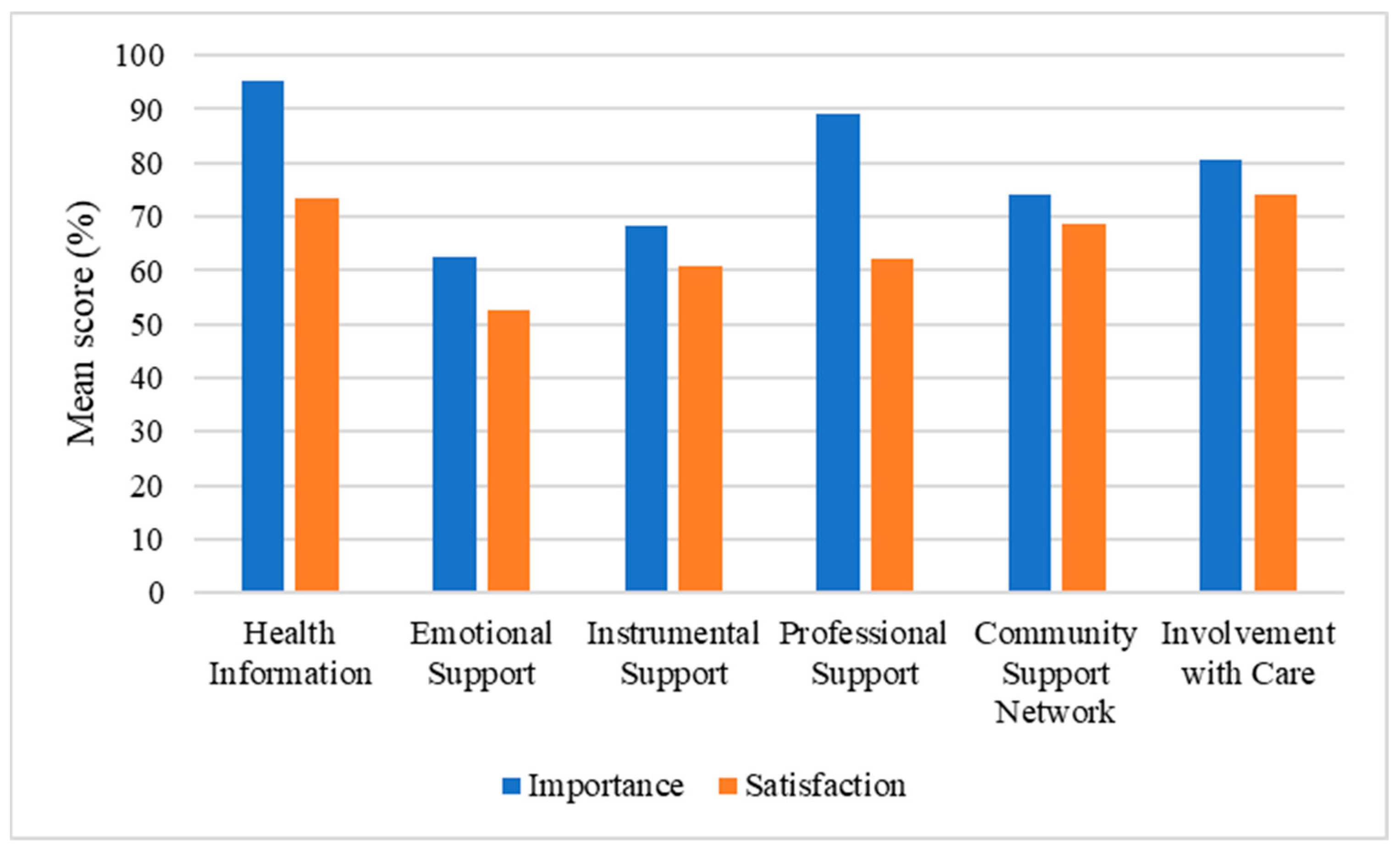
3.1.2. Caregivers’ Needs
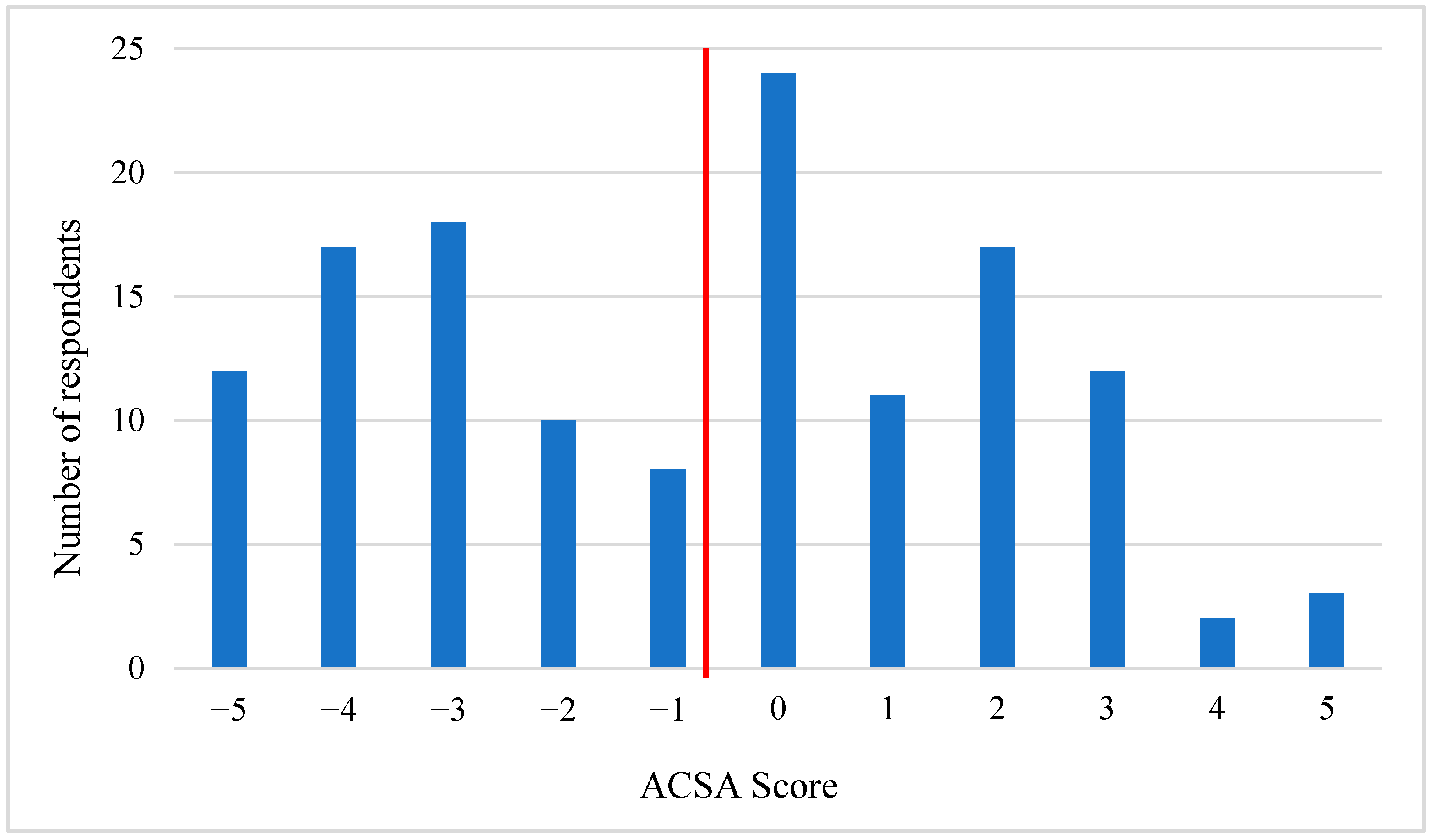
3.1.3. Caregivers’ QoL and Opinions about End-of-Life Decisions
3.2. Characteristics of Caregivers Depending on Their QoL and Psychological Distress
3.3. Differences Linked to Other Socio-Demographic and Medical Factors
4. Discussion
4.1. Caregivers’ Needs and QOL
4.2. Differences According to the Level of QoL
4.3. Differences According to the Level of Emotional Distress and Other Factors
4.4. Limitations
4.5. Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pistarini, C.; Maggioni, G. Disorders of Consciousness. In Clinical Pathways in Stroke Rehabilitation: Evidence-Based Clinical Practice Recommendations; Platz, T., Ed.; Springer International Publishing: Cham, Switzerland, 2021; pp. 57–70. ISBN 978-3-030-58505-1. [Google Scholar]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.F.; et al. Practice Guideline Update Recommendations Summary: Disorders of Consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Arch. Phys. Med. Rehabil. 2018, 99, 1699–1709. [Google Scholar] [CrossRef]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zeman, A.; et al. Unresponsive Wakefulness Syndrome: A New Name for the Vegetative State or Apallic Syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Bruno, M.-A.; Vanhaudenhuyse, A.; Thibaut, A.; Moonen, G.; Laureys, S. From Unresponsive Wakefulness to Minimally Conscious PLUS and Functional Locked-in Syndromes: Recent Advances in Our Understanding of Disorders of Consciousness. J. Neurol. 2011, 258, 1373–1384. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Fins, J.J.; Laureys, S.; Schiff, N.D. Disorders of Consciousness after Acquired Brain Injury: The State of the Science. Nat. Rev. Neurol. 2014, 10, 99–114. [Google Scholar] [CrossRef]
- Laureys, S.; Pellas, F.; Van Eeckhout, P.; Ghorbel, S.; Schnakers, C.; Perrin, F.; Berré, J.; Faymonville, M.-E.; Pantke, K.-H.; Damas, F.; et al. The Locked-in Syndrome: What Is It like to Be Conscious but Paralyzed and Voiceless? Prog. Brain Res. 2005, 150, 495–511. [Google Scholar] [CrossRef]
- Maiser, S.; Kabir, A.; Sabsevitz, D.; Peltier, W. Locked-In Syndrome: Case Report and Discussion of Decisional Capacity. J. Pain Symptom Manag. 2016, 51, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Chinner, A.; Pauli, R.; Cruse, D. The Impact of Prolonged Disorders of Consciousness on Family Caregivers’ Quality of Life—A Scoping Review. Neuropsychol. Rehabil. 2021, 32, 1643–1666. [Google Scholar] [CrossRef]
- Magnani, F.G.; Leonardi, M.; Sattin, D. Caregivers of People with Disorders of Consciousness: Which Burden Predictors? Neurol. Sci. 2020, 41, 2773–2779. [Google Scholar] [CrossRef]
- Munce, S.E.P.; Webster, F.; Christian, J.; Gonzalez-Lara, L.E.; Owen, A.M.; Weijer, C. Experiences of Family of Individuals in a Locked in, Minimally Conscious State, or Vegetative State with the Health Care System. Brain Inj. 2021, 35, 8–14. [Google Scholar] [CrossRef]
- Proia-Lelouey, N.; Boissel, A. Being a Caregiver of a Relative with a Prolonged Disorder of Consciousness Living at Home: A Scoping Review. Neuropsychol. Rehabil. 2022, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Ennis, N.; Rosenbloom, B.N.; Canzian, S.; Topolovec-Vranic, J. Depression and Anxiety in Parent versus Spouse Caregivers of Adult Patients with Traumatic Brain Injury: A Systematic Review. Neuropsychol. Rehabil. 2013, 23, 1–18. [Google Scholar] [CrossRef]
- Giovannetti, A.M.; Leonardi, M.; Pagani, M.; Sattin, D.; Raggi, A. Burden of Caregivers of Patients in Vegetative State and Minimally Conscious State. Acta Neurol. Scand. 2013, 127, 10–18. [Google Scholar] [CrossRef]
- Giovannetti, A.M.; Covelli, V.; Sattin, D.; Leonardi, M. Caregivers of Patients with Disorder of Consciousness: Burden, Quality of Life and Social Support. Acta Neurol. Scand. 2015, 132, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Lugo, Z.; Pellas, F.; Blandin, V.; Laureys, S.; Gosseries, O. Assessment of Needs, Psychological Impact and Quality of Life in Families of Patients with Locked-in Syndrome. Brain Inj. 2017, 31, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Norup, A.; Petersen, J.; Mortensen, E.L. Relatives of Patients with Severe Brain Injury: Growth Curve Analysis of Anxiety and Depression the First Year after Injury. Brain Inj 2015, 29, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Soeterik, S.M.; Connolly, S.; Playford, E.D.; Duport, S.; Riazi, A. The Psychological Impact of Prolonged Disorders of Consciousness on Caregivers: A Systematic Review of Quantitative Studies. Clin. Rehabil. 2017, 31, 1374–1385. [Google Scholar] [CrossRef]
- Doser, K.; Norup, A. Family Needs in the Chronic Phase after Severe Brain Injury in Denmark. Brain Inj. 2014, 28, 1230–1237. [Google Scholar] [CrossRef]
- Leonardi, M.; Giovannetti, A.M.; Pagani, M.; Raggi, A.; Sattin, D.; on behalf of the National Consortium Functioning and Disability in Vegetative and in Minimal Conscious State Patients. Burden and Needs of 487 Caregivers of Patients in Vegetative State and in Minimally Conscious State: Results from a National Study. Brain Inj. 2012, 26, 1201–1210. [Google Scholar] [CrossRef]
- Pagani, M.; Giovannetti, A.M.; Covelli, V.; Sattin, D.; Raggi, A.; Leonardi, M. Physical and Mental Health, Anxiety and Depressive Symptoms in Caregivers of Patients in Vegetative State and Minimally Conscious State. Clin. Psychol. Psychother. 2014, 21, 420–426. [Google Scholar] [CrossRef]
- Romaniello, C.; Farinelli, M.; Matera, N.; Bertoletti, E.; Pedone, V.; Northoff, G. Anxious Attachment Style and Hopelessness as Predictors of Burden in Caregivers of Patients with Disorders of Consciousness: A Pilot Study. Brain Inj. 2015, 29, 466–472. [Google Scholar] [CrossRef]
- Doser, K.; Norup, A. Caregiver Burden in Danish Family Members of Patients with Severe Brain Injury: The Chronic Phase. Brain Inj. 2016, 30, 334–342. [Google Scholar] [CrossRef]
- Corallo, F.; Bonanno, L.; Lo Buono, V.; De Salvo, S.; Rifici, C.; Bramanti, A.; Marino, S. Psychological Distress of Family Members of Vegetative and Minimally Conscious State Patients. Acta Med. Mediterr. 2015, 31, 297–302. [Google Scholar]
- Moretta, P.; Estraneo, A.; De Lucia, L.; Cardinale, V.; Loreto, V.; Trojano, L. A Study of the Psychological Distress in Family Caregivers of Patients with Prolonged Disorders of Consciousness during In-Hospital Rehabilitation. Clin. Rehabil. 2014, 28, 717–725. [Google Scholar] [CrossRef]
- Steppacher, I.; Kissler, J. A Problem Shared Is a Problem Halved? Comparing Burdens Arising for Family Caregivers of Patients with Disorders of Consciousness in Institutionalized versus at Home Care. BMC Psychol. 2018, 6, 58. [Google Scholar] [CrossRef] [PubMed]
- Demotte, R. Politique de La Santé à Mener à l’égard Des Patients En État Végétatif Persistant Ou En État Pauci-Relationnel. 2004. [Google Scholar]
- Serio, C.D.; Kreutzer, J.S.; Witol, A.D. Family Needs after Traumatic Brain Injury: A Factor Analytic Study of the Family Needs Questionnaire. Brain Inj. 1997, 11, 1–10. [Google Scholar] [CrossRef]
- Norup, A.; Perrin, P.B.; Cuberos-Urbano, G.; Anke, A.; Andelic, N.; Doyle, S.T.; Cristina Quijano, M.; Caracuel, A.; Mar, D.; Guadalupe Espinosa Jove, I.; et al. Family Needs after Brain Injury: A Cross Cultural Study. NeuroRehabilitation 2015, 36, 203–214. [Google Scholar] [CrossRef]
- Heymans, M.W.; Eekhout, I. Missing Data in Questionnaires. In Applied Missing Data Analysis with SPSS and (R)Studio; Heymans and Eekhout: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Bernheim, J.L. How to Get Serious Answers to the Serious Question: ‘How Have You Been?’: Subjective Quality of Life (QOL) as an Individual Experiential Emergent Construct. Bioethics 1999, 13, 272–287. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Pisa, F.E.; Biasutti, E.; Drigo, D.; Barbone, F. The Prevalence of Vegetative and Minimally Conscious States: A Systematic Review and Methodological Appraisal. J. Head Trauma Rehabil. 2014, 29, E23–E30. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.T. How Many Patients in a Prolonged Disorder of Consciousness Might Need a Best Interests Meeting about Starting or Continuing Gastrostomy Feeding? Clin. Rehabil. 2018, 32, 1551–1564. [Google Scholar] [CrossRef]
- Cameron, J.; Chu, L.M.; Matte, A.; Tomlinson, G.; Chan, L.; Thomas, C.; Friedrich, J.O.; Mehta, S.; Lamontagne, F.; Levasseur, M.; et al. One-Year Outcomes in Caregivers of Critically Ill Patients. N. Engl. J. Med. 2016, 374, 1831–1841. [Google Scholar] [CrossRef]
- Rohleder, P.; Lambie, J.; Hale, E. A Qualitative Study of the Emotional Coping and Support Needs of Children Living with a Parent with a Brain Injury. Brain Inj. 2017, 31, 199–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruno, M.-A.; Bernheim, J.L.; Ledoux, D.; Pellas, F.; Demertzi, A.; Laureys, S. A Survey on Self-Assessed Well-Being in a Cohort of Chronic Locked-in Syndrome Patients: Happy Majority, Miserable Minority. BMJ Open 2011, 1, e000039. [Google Scholar] [CrossRef] [PubMed]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-Regulation Strategies across Psychopathology: A Meta-Analytic Review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef]
- Milaniak, I.; Wilczek-Rużyczka, E.; Wierzbicki, K.; Sadowski, J.; Kapelak, B.; Przybyłowski, P. Role of Personal Resources in Depression and Stress in Heart Transplant Recipients. Transplant. Proc. 2016, 48, 1761–1766. [Google Scholar] [CrossRef] [PubMed]
- Berg, J.A.; Woods, N.F. Global Women’s Health: A Spotlight on Caregiving. Nurs. Clin. North Am. 2009, 44, 375–384. [Google Scholar] [CrossRef]
- Seedat, S.; Rondon, M. Women’s Wellbeing and the Burden of Unpaid Work. BMJ 2021, 374, n1972. [Google Scholar] [CrossRef]
- Pope, N.; Giger, J.; Lee, J.; Ely, G. Predicting Personal Self-Care in Informal Caregivers. Soc. Work. Health Care 2017, 56, 822–839. [Google Scholar] [CrossRef]
- Cameron, C.; Pirozzo, S.; Tooth, L. Long-Term Care of People below Age 65 with Severe Acquired Brain Injury: Appropriateness of Aged Care Facilities. Aust. N. Z. J. Public Health 2001, 25, 261–264. [Google Scholar] [CrossRef]
- Corallo, F.; Bonanno, L.; De Salvo, S.; Giorgio, A.; Rifici, C.; Buono, V.L.; Bramanti, P.; Marino, S. Effects of Counseling on Psychological Measures in Caregivers of Patients with Disorders of Consciousness. Am. J. Health Behav. 2015, 39, 772–778. [Google Scholar] [CrossRef]
- Simpson, G.K.; Anderson, M.I.; Jones, K.F.; Genders, M.; Gopinath, B. Do Spirituality, Resilience and Hope Mediate Outcomes among Family Caregivers after Traumatic Brain Injury or Spinal Cord Injury? A Structural Equation Modelling Approach. NeuroRehabilitation 2020, 46, 3–15. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. BDI-II, Beck Depression Inventory: Manual; Psychological Corp.; Harcourt Brace: San Antonio, TX, USA; Boston, MA, USA, 1996; ISBN 978-0-15-801838-6. [Google Scholar]
- Spielberger, C.; Gorsuch, R.; Lushene, R.; Vagg, P.; Jacobs, G. Manual for the State-Trait Anxiety Inventory (Form Y1–Y2); 1983; Volume IV. [Google Scholar]
- Cruzado, J.A.; Elvira de la Morena, M.J. Coping and Distress in Caregivers of Patients with Disorders of Consciousness. Brain Inj. 2013, 27, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, S.; Gius, E.; Bastianelli, A. How the Burden of Caring for a Patient in a Vegetative State Changes in Relation to Different Coping Strategies. Brain Inj. 2014, 28, 92–96. [Google Scholar] [CrossRef]
- Corallo, F.; Bonanno, L.; Lo Buono, V.; De Salvo, S.; Rifici, C.; Bramanti, A.; Marino, S. Coping Strategies in Caregivers of Disorders of Consciousness Patients. Neurol. Sci. 2018, 39, 1375–1381. [Google Scholar] [CrossRef] [PubMed]
- Pagani, M.; Giovannetti, A.M.; Covelli, V.; Sattin, D.; Leonardi, M. Caregiving for Patients in Vegetative and Minimally Conscious States: Perceived Burden as a Mediator in Caregivers’ Expression of Needs and Symptoms of Depression and Anxiety. J. Clin. Psychol. Med. Settings 2014, 21, 214–222. [Google Scholar] [CrossRef]
- Jaglal, S.B.; Guilcher, S.J.T.; Bereket, T.; Kwan, M.; Munce, S.; Conklin, J.; Versnel, J.; Packer, T.; Verrier, M.; Marras, C.; et al. Development of a Chronic Care Model for Neurological Conditions (CCM-NC). BMC Health Serv. Res. 2014, 14, 409. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-H.; Xu, Z.-P. Psychological Crisis Intervention for the Family Members of Patients in a Vegetative State. Clinics 2012, 67, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Smart, C.M.; Giacino, J.T. Exploring Caregivers’ Knowledge of and Receptivity toward Novel Diagnostic Tests and Treatments for Persons with Post-Traumatic Disorders of Consciousness. NeuroRehabilitation 2015, 37, 117–130. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Impact on the Caregiver’s QoL and Needs | ||
|---|---|---|
| Characteristics linked to the caregiver | Gender | - Female: ↗ depression, ↗ anxiety, ↗ prolonged grief disorder [9,16,17,20]. - No difference in burden [21]. |
| Age | - Young age: ↗ prolonged grief disorder [17]. - No link between age and depression [17]. | |
| Relationship with the patient | - Spouses: ↗ anxiety, ↗ burden [16,22]. - No difference in burden [12]. | |
| Presence of psychological distress | - ↘ QoL [8,14,17]. | |
| High number of unmet needs | - ↘ QoL [15]. | |
| Characteristics linked to the patient | Age | - Younger patient: ↗ prolonged grief disorder, ↗ anxiety [16,17]. |
| Time since brain injury | - ↗ need for social support shortly after the brain injury, and ↗ financial, social and marital negative consequences over time [10]. - ↘ QoL, ↘ number of needs, ↘ social support over time [8,17]. - Evolution of distress and burden variable [16,17]. - No link between burden and time since brain injury [13]. | |
| Diagnosis/level of consciousness | - MCS (compared to UWS): ↗ need for help, supportive assistance [23] and emotional and social supports [13]. - Higher level of consciousness: ↘ anxiety [16]. - No differences in burden, psychological symptoms, and needs [13,17,24]. | |
| Care setting | - ↗ or ↘ of anxiety when relative kept at home [11]. - No difference in burden, distress or grief according to the care setting [17,25]. - No influence in burden [14]. | |
| Caregivers’ Characteristics | N = 177 |
|---|---|
| Age (years) | |
| Mean (SD) Range | 52.25 (13.14) 21–86 |
| Gender, N (%) | |
| Women | 100 (56.5) |
| Men | 73 (41.2) |
| Other | 2 (1.1) |
| Unspecified | 2 (1.1) |
| Relationship to the patient, N (%) | |
| Wife/husband/partner | 58 (32.8) |
| Father/mother | 84 (47.5) |
| Son/daughter | 16 (9.0) |
| Brother/sister | 15 (8.5) |
| Other | 2 (1.1) |
| Unspecified | 2 (1.1) |
| Employment status, N (%) | |
| Actively working | 106 (59.9) |
| Not actively working (i.e., retired, housewife/househusband, student, unemployed) | 59 (33.3) |
| Unspecified | 12 (6.8) |
| Patients’ characteristics | |
| Age (years) | |
| Mean (SD) | 42.69 (15.25) |
| Range | 5–79 |
| Level of consciousness, N (%) | |
| Coma | 2 (1.1) |
| UWS | 25 (14.1) |
| MCS | 89 (50.3) |
| EMCS | 16 (9.0) |
| LIS | 5 (2.8) |
| Unspecified (no answer or multiple answers) | 40 (22.6) |
| Time since brain injury (months) | |
| Mean (SD) | 43.77 (64.01) |
| Range | 1–356 |
| Care setting, N (%) | |
| Home | 38 (21.5) |
| Rehabilitation center | 58 (32.8) |
| Nursing home | 74 (41.8) |
| General hospital | 2 (1.1) |
| Combination of two places | 1 (0.6) |
| Unspecified | 4 (2.3) |
| Need | Importance (%) | Satisfaction (%) |
|---|---|---|
| Mean (SD) | Mean (SD) | |
| Health Information | 95.40 (10.77) | 73.29 (25.69) |
| Emotional Support | 62.67 (24.60) | 52.76 (30.06) |
| Instrumental Support | 68.38 (26.18) | 60.75 (30.05) |
| Professional Support | 89.19 (15.03) | 62.22 (29.72) |
| Community Support Network | 74.25 (21.76) | 68.59 (26.56) |
| Involvement with Care | 80.56 (21.22) | 74.01 (28.02) |
| N = 177 | |
|---|---|
| Anxiety, N (%) | |
| Absent | 37 (20.9) |
| Moderate | 91 (51.4) |
| Extreme | 28 (15.8) |
| Unspecified | 7 (4.0) |
| Depressive thoughts, N (%) | |
| Frequent | 28 (15.8) |
| Occasional | 111 (62.7) |
| Absent | 32 (18.1) |
| Unspecified | 6 (3.4) |
| Quality of life (Anamnestic Comparative Self-Assessment Scale) | |
| Mean (SD) | −0.81 (2.69) |
| Range | −5.0–5.0 |
| Missing data (N, (%)) | 43 (24.3) |
| Opinion regarding patient’s euthanasia, N (%) | |
| Never considered | 87 (49.2) |
| Considered for a while but not anymore | 52 (29.4) |
| Desired | 26 (14.7) |
| Unspecified | 12 (6.8) |
| Opinion regarding patient’s therapy, N (%) | |
| No limit to therapy | 85 (48.0) |
| Do not reanimate | 51 (28.8) |
| Do not add any therapy or extend the ongoing therapy | 13 (7.3) |
| Progressive discontinuation of therapy | 6 (3.4) |
| Unspecified/undecided | 22 (12.4) |
| Impact on the Caregiver’s QoL and Needs | ||
|---|---|---|
| Characteristics linked to the caregiver | Gender | - Female: ↗ importance of instrumental support. |
| Age | - No difference noted on all the variables. | |
| Relationship with the patient | - Spouses and parents: ↗ importance of involvement in care. | |
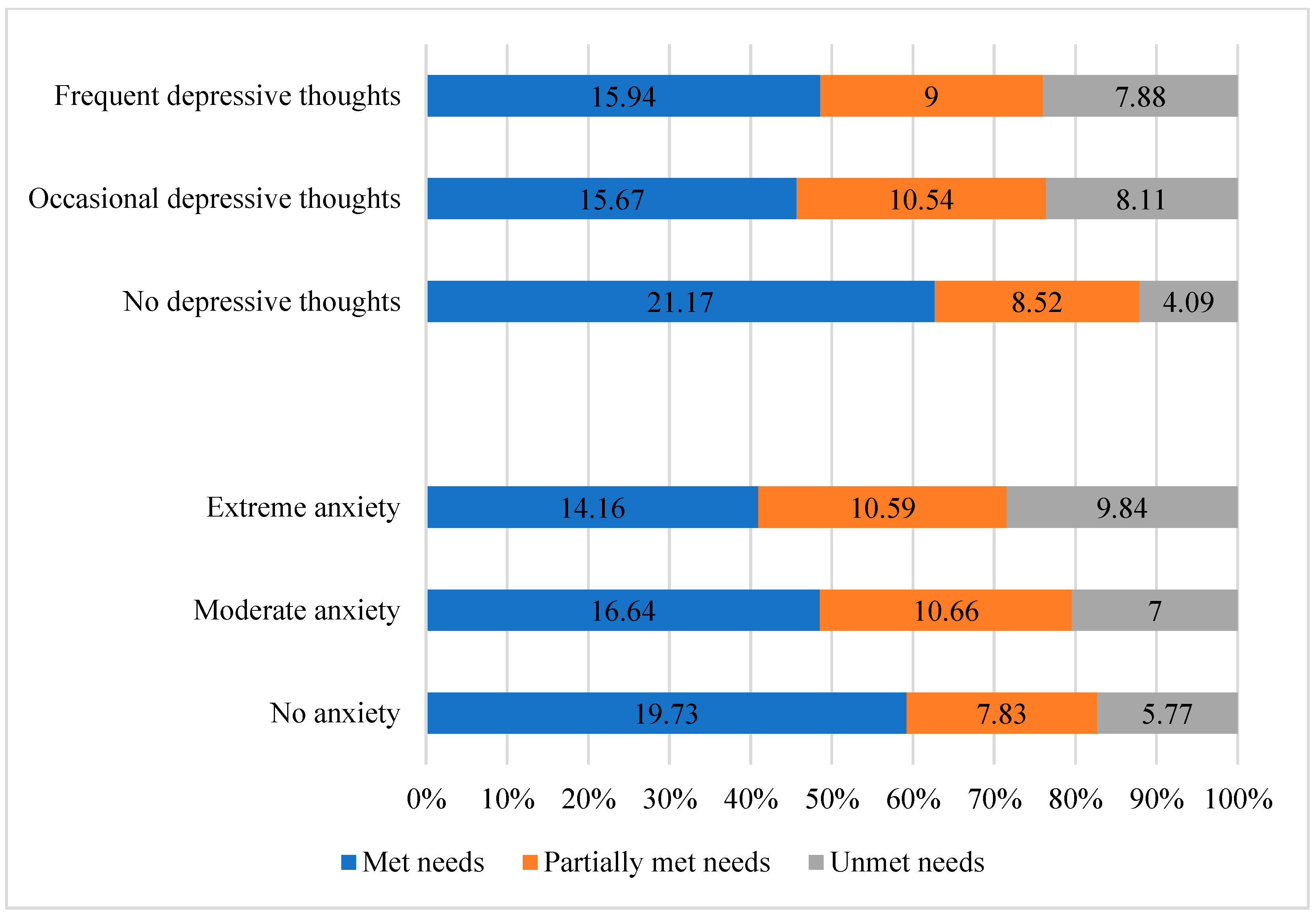
| Presence of psychological distress | - ↗ consideration of euthanasia. - ↗ number of unmet needs. - ↗ importance of emotional and professional supports. - ↘ satisfaction of the needs for instrumental support and involvement in care (when higher anxiety), and of the need for professional support (when more frequent depressive thoughts). | |
| High number of unmet needs | - ↘ QoL. - ↗ anxiety, ↗ depressive thoughts. | |
| Characteristics linked to the patient | Age | - No difference noted on all the variables. |
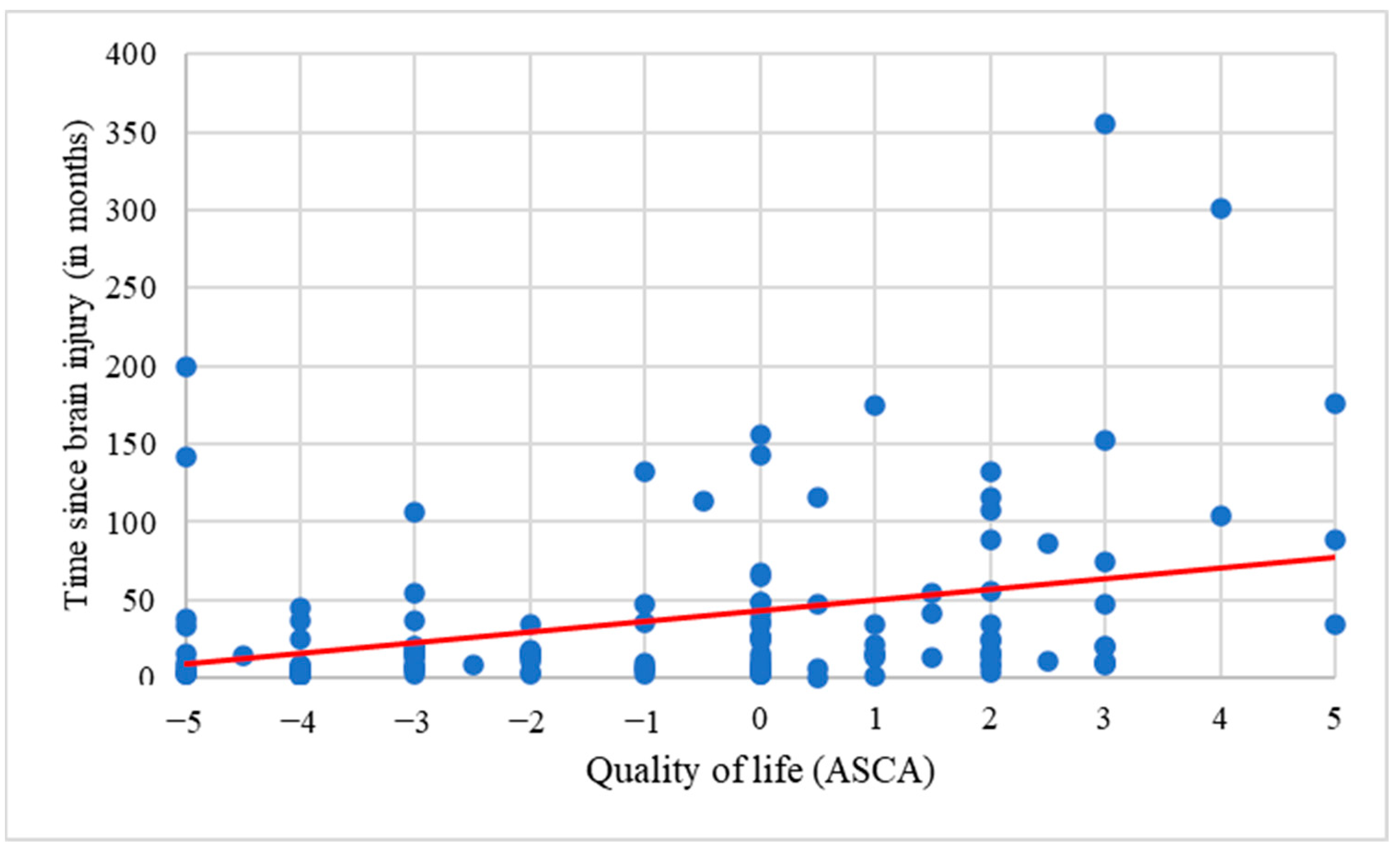
| Time since brain injury | - Longer time: ↗ QoL. | |
| Diagnosis/level of consciousness | - UWS and MCS: ↗ consideration of euthanasia and progressive discontinuation of therapy. | |
| Care setting | - Better QoL when patient at home or in nursing home compared to rehabilitation center. - Nursing home: ↗ consideration of euthanasia. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gosseries, O.; Schnakers, C.; Vanhaudenhuyse, A.; Martial, C.; Aubinet, C.; Charland-Verville, V.; Thibaut, A.; Annen, J.; Ledoux, D.; Laureys, S.; et al. Needs and Quality of Life of Caregivers of Patients with Prolonged Disorders of Consciousness. Brain Sci. 2023, 13, 308. https://doi.org/10.3390/brainsci13020308
Gosseries O, Schnakers C, Vanhaudenhuyse A, Martial C, Aubinet C, Charland-Verville V, Thibaut A, Annen J, Ledoux D, Laureys S, et al. Needs and Quality of Life of Caregivers of Patients with Prolonged Disorders of Consciousness. Brain Sciences. 2023; 13(2):308. https://doi.org/10.3390/brainsci13020308
Chicago/Turabian StyleGosseries, Olivia, Caroline Schnakers, Audrey Vanhaudenhuyse, Charlotte Martial, Charlène Aubinet, Vanessa Charland-Verville, Aurore Thibaut, Jitka Annen, Didier Ledoux, Steven Laureys, and et al. 2023. "Needs and Quality of Life of Caregivers of Patients with Prolonged Disorders of Consciousness" Brain Sciences 13, no. 2: 308. https://doi.org/10.3390/brainsci13020308