

Altered Fractional Amplitude of Low-Frequency Fluctuation in Anxious Parkinson’s Disease
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Imaging Data Acquisition
2.3. Imaging Data Preprocessing
2.4. fALFF Analysis
2.5. Statistical Analysis
3. Results
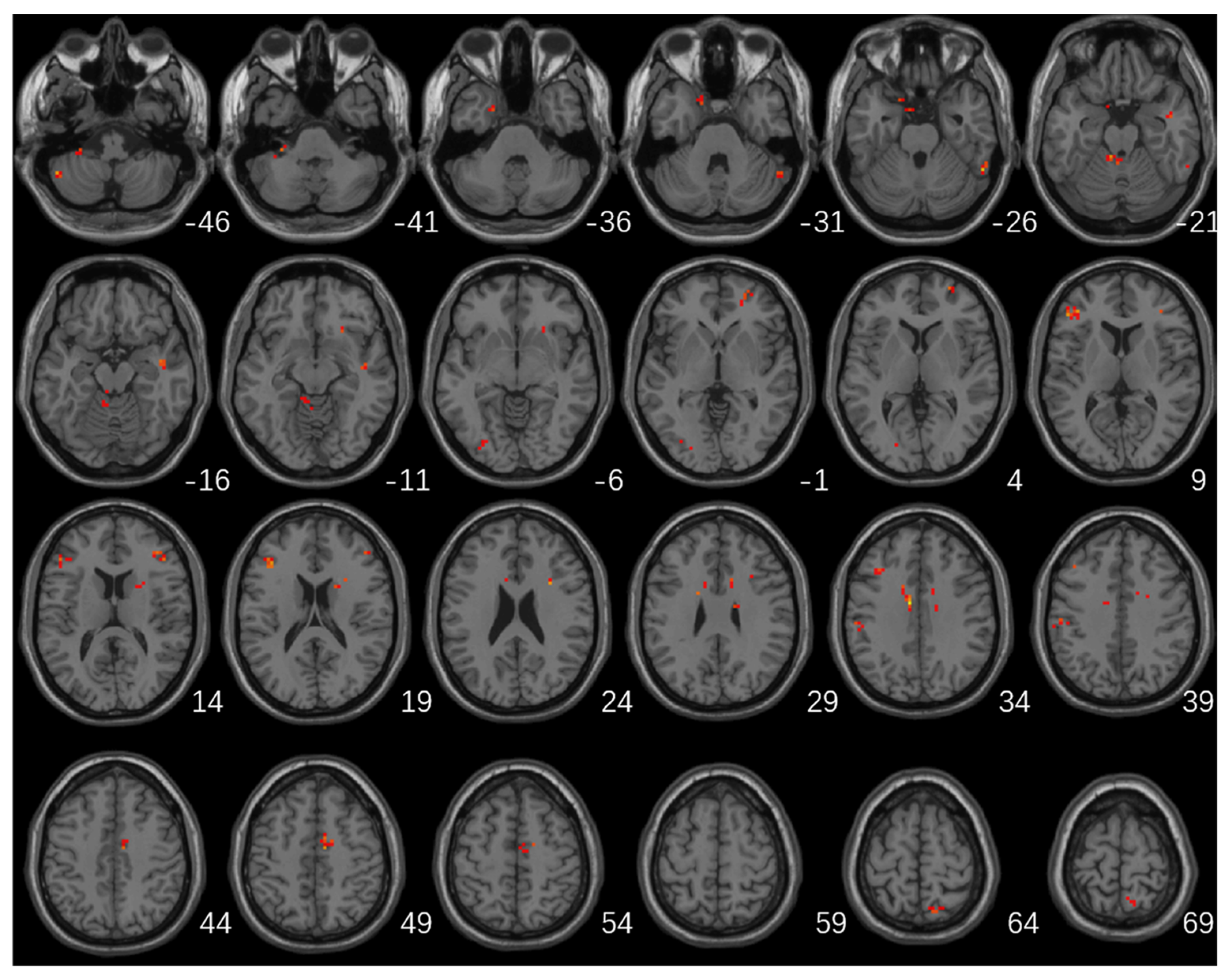
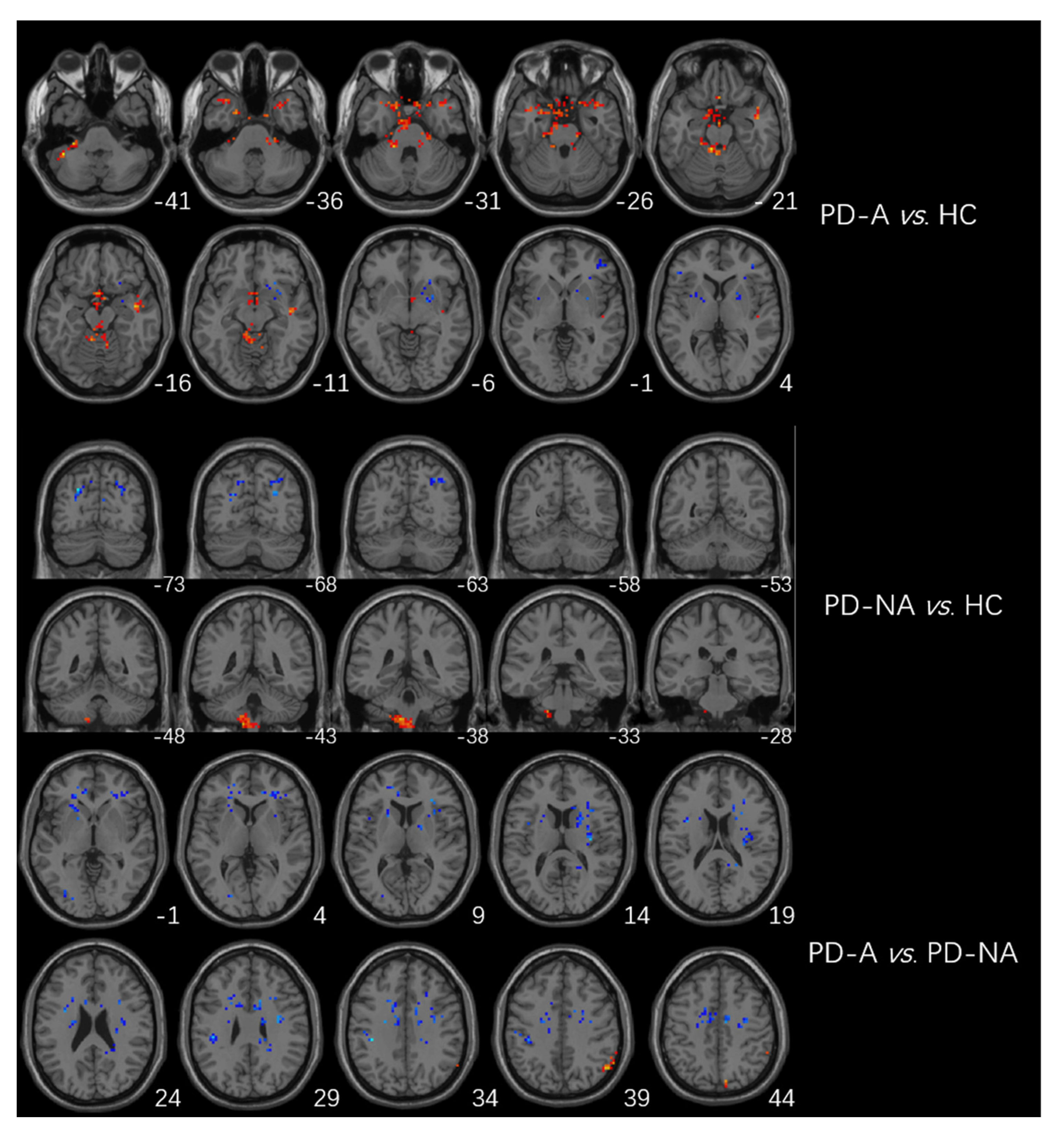
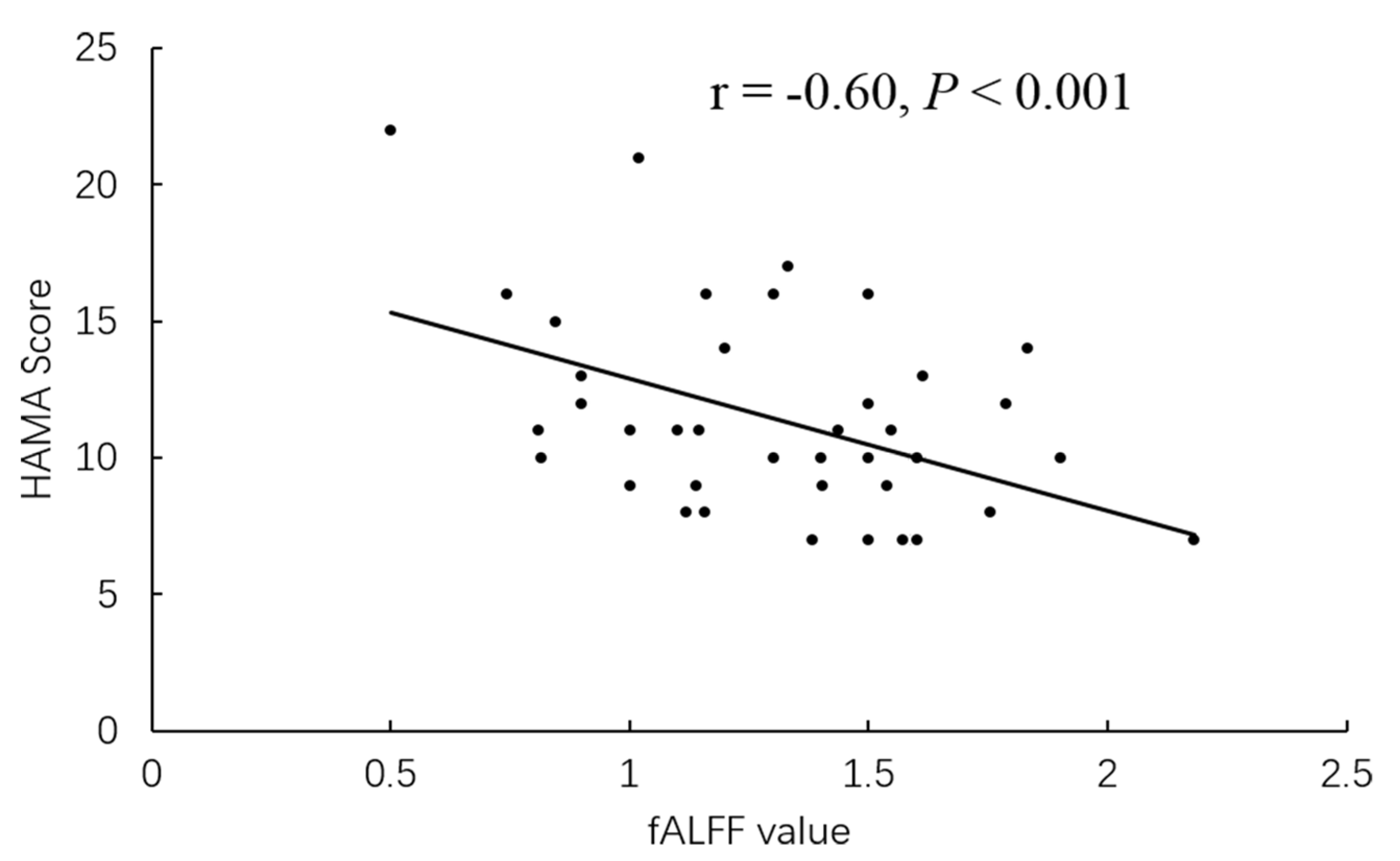
fALFF Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rong, S.; Zhang, P.; He, C.; Li, Y.; Li, X.; Li, R.; Nie, K.; Huang, S.; Wang, L.; Wang, L.; et al. Abnormal Neural Activity in Different Frequency Bands in Parkinson’s Disease With Mild Cognitive Impairment. Front. Aging Neurosci. 2021, 13, 709998. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, J.; Wang, M.; Yuan, Y.; Zhu, L.; Shen, Y.; Zhang, H.; Zhang, K. Alterations of the amplitude of low-frequency fluctuations in anxiety in Parkinson’s disease. Neurosci. Lett. 2018, 668, 19–23. [Google Scholar] [CrossRef]
- Liao, H.; Yi, J.; Cai, S.; Shen, Q.; Liu, Q.; Zhang, L.; Li, J.; Mao, Z.; Wang, T.; Zi, Y.; et al. Changes in Degree Centrality of Network Nodes in Different Frequency Bands in Parkinson’s Disease With Depression and Without Depression. Front. Neurosci. 2021, 15, 638554. [Google Scholar] [CrossRef] [PubMed]
- Forbes, E.J.; Byrne, G.J.; O’Sullivan, J.D.; Yang, J.; Marsh, R.; Dissanayaka, N.N. Defining Atypical Anxiety in Parkinson’s Disease. Mov. Disord. Clin. Pract. 2021, 8, 571–581. [Google Scholar] [CrossRef]
- Wang, X.; Li, J.; Yuan, Y.; Wang, M.; Ding, J.; Zhang, J.; Zhu, L.; Shen, Y.; Zhang, H.; Zhang, K. Altered putamen functional connectivity is associated with anxiety disorder in Parkinson’s disease. Oncotarget 2017, 8, 81377–81386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Callaghan, C.; Shine, J.M.; Lewis, S.J.; Hornberger, M. Neuropsychiatric symptoms in Parkinson’s disease: Fronto-striatal atrophy contributions. Park. Relat. Disord. 2014, 20, 867–872. [Google Scholar] [CrossRef]
- Moonen, A.; Weiss, P.H.; Wiesing, M.; Weidner, R.; Fink, G.R.; Reijnders, J.S.; Weber, W.M.; Leentjens, A.F. An fMRI study into emotional processing in Parkinson’s disease: Does increased medial prefrontal activation compensate for striatal dysfunction. PLoS ONE 2017, 12, e0177085. [Google Scholar] [CrossRef] [Green Version]
- Joling, M.; van den Heuvel, O.A.; Berendse, H.W.; Booij, J.; Vriend, C. Serotonin transporter binding and anxiety symptoms in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2018, 89, 89–94. [Google Scholar] [CrossRef]
- Dan, R.; Růžička, F.; Bezdicek, O.; Růžička, E.; Roth, J.; Vymazal, J.; Goelman, G.; Jech, R. Separate neural representations of depression, anxiety and apathy in Parkinson’s disease. Sci. Rep. 2017, 7, 12164. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Zhang, S.; Yang, H.; Zhang, X.; He, S.; Wang, J.; Li, J. Altered cerebellum functional network on newly diagnosed drug-naïve Parkinson’s disease patients with anxiety. Transl. Neurosci. 2021, 12, 415–424. [Google Scholar] [CrossRef]
- Criaud, M.; Kim, J.H.; Zurowski, M.; Lobaugh, N.; Chavez, S.; Houle, S.; Strafella, A.P. Anxiety in Parkinson’s disease: Abnormal resting activity and connectivity. Brain Res. 2021, 1753, 147235. [Google Scholar] [CrossRef]
- Liang, R.B.; Liu, L.Q.; Shi, W.Q.; Sun, T.; Ge, Q.M.; Li, Q.Y.; Shu, H.Y.; Zhang, L.J.; Shao, Y. Abnormal Fractional Amplitude of Low Frequency Fluctuation Changes in Patients With Dry Eye Disease: A Functional Magnetic Resonance Imaging Study. Front. Hum. Neurosci. 2022, 16, 900409. [Google Scholar] [CrossRef] [PubMed]
- Zi, Y.; Cai, S.; Tan, C.; Wang, T.; Shen, Q.; Liu, Q.; Wang, M.; Li, J.; Zhang, L.; Zhou, F.; et al. Abnormalities in the Fractional Amplitude of Low-Frequency Fluctuation and Functional Connectivity in Parkinson’s Disease With Excessive Daytime Sleepiness. Front. Aging Neurosci. 2022, 14, 826175. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Hu, X.; Song, X.; Li, E.; Liu, J.; Yuan, Y.; Liu, W.; Liu, Y. Altered Resting-State Brain Activity and Connectivity in Depressed Parkinson’s Disease. PLoS ONE 2015, 10, e0131133. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Ma, C.; Luo, Y.; Li, J.; Li, Q.; Liu, Y.; Ding, C.; Qiu, J. Neural basis of uncertain cue processing in trait anxiety. Sci. Rep. 2016, 6, 21298. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.E.; Park, S.A. Physiological and Psychological Effects of Visual Stimulation with Green Plant Types. Int. J. Environ. Res. Public Health 2021, 18, 12932. [Google Scholar] [CrossRef]
- Wolters, A.F.; van de Weijer, S.; Leentjens, A.; Duits, A.A.; Jacobs, H.; Kuijf, M.L. Resting-state fMRI in Parkinson’s disease patients with cognitive impairment: A meta-analysis. Park. Relat. Disord. 2019, 62, 16–27. [Google Scholar] [CrossRef]
- Xing, Y.; Fu, S.; Li, M.; Ma, X.; Liu, M.; Liu, X.; Huang, Y.; Xu, G.; Jiao, Y.; Wu, H.; et al. Regional Neural Activity Changes in Parkinson’s Disease-Associated Mild Cognitive Impairment and Cognitively Normal Patients. Neuropsychiatr. Dis. Treat. 2021, 17, 2697–2706. [Google Scholar] [CrossRef]
- Qiu, Y.H.; Huang, Z.H.; Gao, Y.Y.; Feng, S.J.; Huang, B.; Wang, W.Y.; Xu, Q.H.; Zhao, J.H.; Zhang, Y.H.; Wang, L.M.; et al. Alterations in intrinsic functional networks in Parkinson’s disease patients with depression: A resting-state functional magnetic resonance imaging study. CNS Neurosci Ther. 2021, 27, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Hu, X.; Zhu, Y.; Yuan, Y.; Liu, W.; Chen, H. Aberrant Intra- and Internetwork Functional Connectivity in Depressed Parkinson’s Disease. Sci. Rep. 2017, 7, 2568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.; Zhang, M.; Zhang, H.; Li, X.; Zou, F.; Wang, Y.; Wu, X.; Zhang, H. The spontaneous activity and functional network of the occipital cortex is correlated with state anxiety in healthy adults. Neurosci. Lett. 2020, 715, 134596. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Qiu, Y.; Luo, Y.; Xu, P.; Li, Z.; Zhu, W.; Wu, Q.; Tao, W.; Guan, Q.; Chen, F. The relationship of anxious and depressive symptoms in Parkinson’s disease with voxel-based neuroanatomical and functional connectivity measures. J. Affect. Disord. 2019, 245, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Hiser, J.; Koenigs, M. The Multifaceted Role of the Ventromedial Prefrontal Cortex in Emotion, Decision Making, Social Cognition, and Psychopathology. Biol Psychiatry 2018, 83, 638–647. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Qi, S.; Liu, S.; Liu, X.; Wei, X.; Ming, D. Altered spontaneous neural activity in the precuneus, middle and superior frontal gyri, and hippocampus in college students with subclinical depression. BMC Psychiatry 2021, 21, 280. [Google Scholar] [CrossRef]
- Suda, A.; Osada, T.; Ogawa, A.; Tanaka, M.; Kamagata, K.; Aoki, S.; Hattori, N.; Konishi, S. Functional Organization for Response Inhibition in the Right Inferior Frontal Cortex of Individual Human Brains. Cereb. Cortex 2020, 30, 6325–6335. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, S.; Kumaran, S.S.; Goyal, V.; Kalaivani, M.; Kaloiya, G.S.; Sagar, R.; Mehta, N.; Srivastava, A.K.; Jagannathan, N.R. Frontal lobe metabolic alterations characterizing Parkinson’s disease cognitive impairment. Neurol. Sci. 2021, 42, 1053–1064. [Google Scholar] [CrossRef]
- Oosterwijk, C.S.; Vriend, C.; Berendse, H.W.; van der Werf, Y.D.; van den Heuvel, O.A. Anxiety in Parkinson’s disease is associated with reduced structural covariance of the striatum. J. Affect Disord. 2018, 240, 113–120. [Google Scholar] [CrossRef]
- Moriyama, T.S.; Felicio, A.C.; Chagas, M.H.; Tardelli, V.S.; Ferraz, H.B.; Tumas, V.; Amaro-Junior, E.; Andrade, L.A.F.; Crippa, J.A.; Bressan, R.A. Increased dopamine transporter density in Parkinson’s disease patients with Social Anxiety Disorder. J. Neurol. Sci. 2011, 310, 53–57. [Google Scholar] [CrossRef]
- Ceravolo, R.; Frosini, D.; Poletti, M.; Kiferle, L.; Pagni, C.; Mazzucchi, S.; Volterrani, D.; Bonuccelli, U. Mild affective symptoms in de novo Parkinson’s disease patients: Relationship with dopaminergic dysfunction. Eur. J. Neurol. 2013, 20, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Wee, N.; Wen, M.C.; Kandiah, N.; Chander, R.J.; Ng, A.; Au, W.L.; Tan, L.C. Neural correlates of anxiety symptoms in mild Parkinson’s disease: A prospective longitudinal voxel-based morphometry study. J. Neurol. Sci. 2016, 371, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Cavanna, A.E.; Trimble, M.R. The precuneus: A review of its functional anatomy and behavioural correlates. Brain 2006, 129 Pt 3, 564–583. [Google Scholar] [CrossRef] [Green Version]
- Gill, J.S.; Sillitoe, R.V. Functional Outcomes of Cerebellar Malformations. Front. Cell. Neurosci. 2019, 13, 441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carey, G.; Görmezoğlu, M.; de Jong, J.; Hofman, P.A.; Backes, W.H.; Dujardin, K.; Leentjens, A.F. Neuroimaging of Anxiety in Parkinson’s Disease: A Systematic Review. Mov. Disord. 2021, 36, 327–339. [Google Scholar] [CrossRef]
- Taylor, J.M.; Whalen, P.J. Neuroimaging and Anxiety: The Neural Substrates of Pathological and Non-pathological Anxiety. Curr. Psychiatry Rep. 2015, 17, 49. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | PD-A (n = 41) | PD-NA (n = 39) | HC (n = 40) | F/χ2/t | p |
|---|---|---|---|---|---|
| Gender (M/F) | 17/24 | 17/22 | 16/24 | 0.44 | 0.80 a |
| Age (years) | 65.54 ± 9.6 | 65.62 ± 10.23 | 60.97 ± 8.82 | 2.45 | 0.091 b |
| Disease course (months) | 39.31 ± 27.42 | 40.53 ± 35.37 | - | −0.174 | 0.96 c |
| MDS-UPDRS-score | 28.45 ± 12.92 | 21.80 ± 12.96 | - | 0.75 | 2.32 c |
| Hoehn and Yahr stage | 1.85 ± 0.59 | 1.73 ± 0.55 | - | 1.05 | 0.91 c |
| HAMA score | 11.26 ± 3.70 | 3.12 ± 2.0 | 2.50 ± 1.30 | 12.27 | 0.005 b,* |
| MMSE score | 27.43 ± 1.58 | 28.22 ± 2.15 | 27.78 ± 1.66 | 1.99 | 0.14 b |
| HAMD score | 3.55 ± 1.88 | 3.00 ± 1.48 | 3.45 ± 1.69 | 1.31 | 0.27 b |
| Brain Regions | Coordinates of Maximum | Cluster Size | F | ||
|---|---|---|---|---|---|
| X | Y | Z | |||
| Left superior/middle temporal gyrus | 21 | 3 | −36 | 26 | 8.64 |
| Left cerebellum/cerebellum posterior lobe | −30 | −33 | −42 | 23 | 10.38 |
| Right superior/inferior temporal gyrus | 57 | −51 | −27 | 23 | 13.00 |
| Left middle/inferior occipital lobe | −33 | −81 | −3 | 13 | 8.33 |
| Left inferior frontal gyrus | −39 | 30 | 18 | 29 | 12.44 |
| Right inferior frontal gyrus | 45 | 33 | 15 | 16 | 13.85 |
| Right superior frontal gyrus | 27 | 60 | 3 | 12 | 10.34 |
| Right caudate | 30 | 12 | 24 | 13 | 11.37 |
| Left inferior parietal lobule | −54 | −24 | 36 | 15 | 10.43 |
| Left middle frontal gyrus | −39 | 24 | 36 | 12 | 12.07 |
| Right precuneus | 6 | −63 | 66 | 13 | 9.62 |
| Brain Regions | Coordinates of Maximum | Cluster Size | t-Value | ||
|---|---|---|---|---|---|
| X | Y | Z | |||
| PD-A > HC | |||||
| Left cerebellum/cerebellum posterior lobe | −42 | −45 | −42 | 38 | 4.74 |
| Right middle/superior temporal gyrus | 42 | −6 | −15 | 71 | 4.29 |
| Left middle/superior temporal gyrus | −36 | 17 | −15 | −37 | 4.02 |
| Brainstem/midbrain | −9 | −38 | −21 | 48 | 4.48 |
| PD-A < HC | |||||
| Right inferior frontal gyrus | 39 | 39 | 15 | 24 | −4.21 |
| Left inferior frontal gyrus | −42 | 27 | 18 | 50 | −4.19 |
| Left putamen/caudate | −33 | 9 | 6 | 24 | −3.94 |
| Right putamen/caudate | 18 | 12 | −9 | 24 | −4.23 |
| Left inferior parietal lobule | −54 | −24 | 36 | 22 | −4.36 |
| PD-NA > HC | |||||
| Left cerebellum/cerebellum posterior lobe | −12 | −42 | −60 | 21 | 4.29 |
| PD-NA < HC | |||||
| Right cuneus | 6 | −78 | 21 | 40 | −4.18 |
| Left superior parietal lobe | −24 | −72 | 33 | 18 | −4.99 |
| PD-A > PD-NA | |||||
| Right precuneus | 6 | −72 | 54 | 39 | 3.99 |
| PD-A < PD-NA | |||||
| Left middle/inferior occipital gyrus | −36 | −68 | 12 | 42 | −4.91 |
| Left inferior frontal gyrus | −27 | 27 | −12 | 41 | −3.76 |
| Right inferior frontal gyrus | 30 | 30 | 9 | 40 | −3.95 |
| Left putamen/caudate | −33 | 9 | 6 | 24 | −3.94 |
| Right caudate/putamen | 39 | 12 | 6 | 24 | −4.22 |
| Left inferior parietal lobule | −39 | −30 | 33 | 28 | −4.53 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, P.; Gao, Y.; Hu, Y.; Luo, Y.; Wang, L.; Wang, K.; Tian, H.; Jin, M. Altered Fractional Amplitude of Low-Frequency Fluctuation in Anxious Parkinson’s Disease. Brain Sci. 2023, 13, 87. https://doi.org/10.3390/brainsci13010087
Zhang P, Gao Y, Hu Y, Luo Y, Wang L, Wang K, Tian H, Jin M. Altered Fractional Amplitude of Low-Frequency Fluctuation in Anxious Parkinson’s Disease. Brain Sciences. 2023; 13(1):87. https://doi.org/10.3390/brainsci13010087
Chicago/Turabian StyleZhang, Peiyao, Yunpeng Gao, Yingying Hu, Yuan Luo, Lu Wang, Kang Wang, Hong Tian, and Miao Jin. 2023. "Altered Fractional Amplitude of Low-Frequency Fluctuation in Anxious Parkinson’s Disease" Brain Sciences 13, no. 1: 87. https://doi.org/10.3390/brainsci13010087