
TED—Trazodone Efficacy in Depression: A Naturalistic Study on the Efficacy of Trazodone in an Extended-Release Formulation Compared to SSRIs in Patients with a Depressive Episode—Preliminary Report

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Assessment
- Montgomery–Åsberg Depression Rating Scale (MADRS); Quick Inventory of Depressive Symptomatology (QIDS)—clinician-rated (CR) and self-rated (SR) scales used to evaluate depressive symptoms
- Hamilton Anxiety Rating Scale (HAM-A), used to measure anxiety
- Snaith–Hamilton Pleasure Scale (SHAPS), used to assess the symptoms of anhedonia
- Sheehan Disability Scale (SDS), used to evaluate a patient’s psychosocial functioning
- Athens Insomnia Scale (AIS), used to measure the severity of insomnia
- Clinical Global Impression Scale (CGI), used to assess the severity of symptoms and the treatment response
2.2. Statistical Analysis
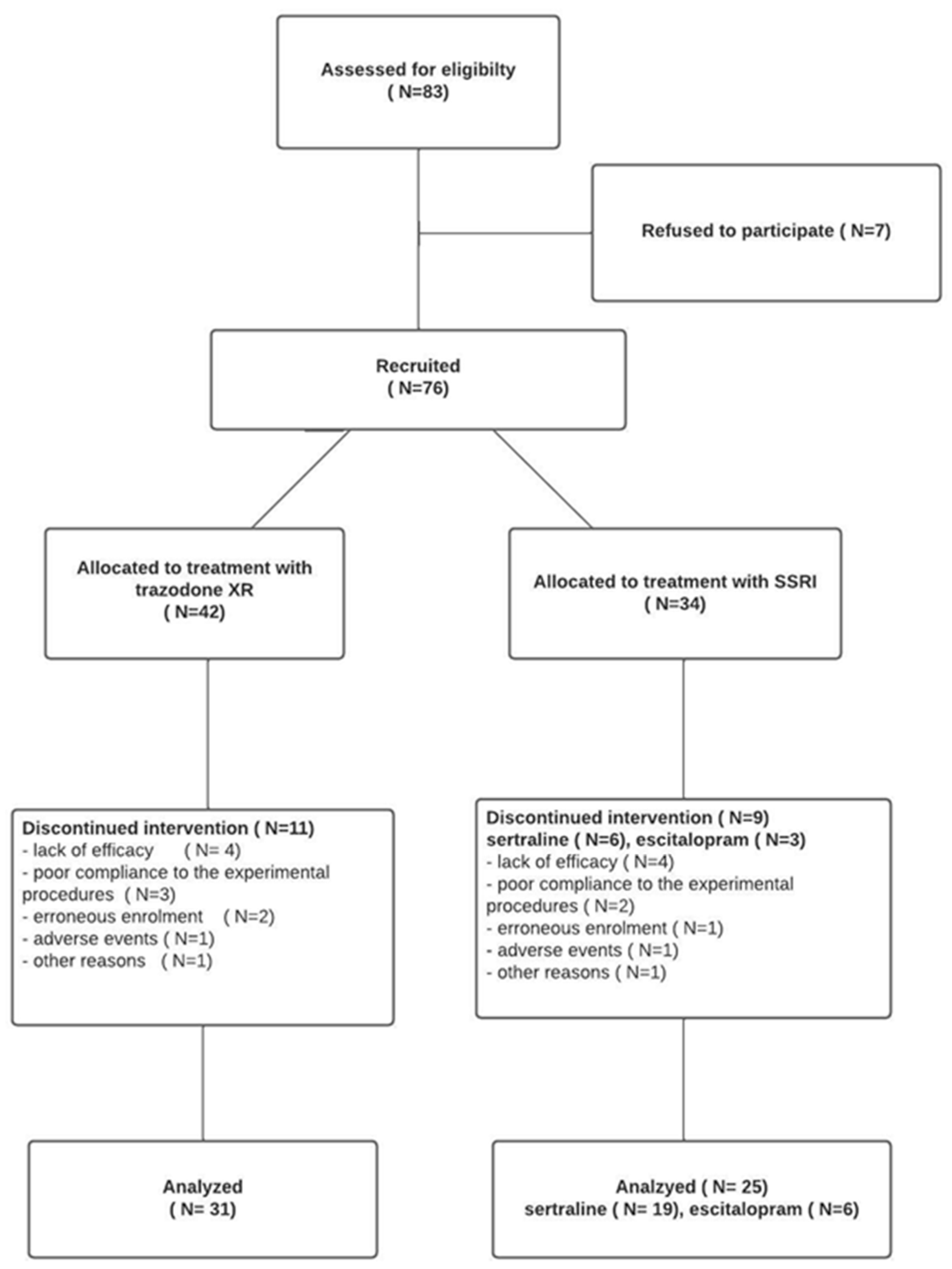
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kessler, R.C. The Costs of Depression. Psychiatr. Clin. North Am. 2012, 35, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Brody, D.J.; Gu, Q. Antidepressant Use among Adults: United States, 2015–2018 Key Findings Data from the National Health and Nutrition Examination Survey; NCHS: Hyattsville, MD, USA, 2015. [Google Scholar]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative Efficacy and Acceptability of 21 Antidepressant Drugs for the Acute Treatment of Adults with Major Depressive Disorder: A Systematic Review and Network Meta-Analysis. Lancet 2018, 391, 1357–1366. [Google Scholar] [CrossRef] [Green Version]
- Pigott, H.E.; Leventhal, A.M.; Alter, G.S.; Boren, J.J. Efficacy and Effectiveness of Antidepressants: Current Status of Research. Psychother. Psychosom. 2010, 79, 267–279. [Google Scholar] [CrossRef]
- Marasine, N.R.; Sankhi, S.; Lamichhane, R.; Marasini, N.R.; Dangi, N.B. Use of Antidepressants among Patients Diagnosed with Depression: A Scoping Review. Biomed Res. Int. 2021, 2021, 6699028. [Google Scholar] [CrossRef]
- Jing, E.; Straw-Wilson, K. Sexual Dysfunction in Selective Serotonin Reuptake Inhibitors (SSRIs) and Potential Solutions: A Narrative Literature Review. Ment. Health Clin. 2016, 6, 191. [Google Scholar] [CrossRef] [PubMed]
- Wichniak, A.; Wierzbicka, A.; Walęcka, M.; Jernajczyk, W. Effects of Antidepressants on Sleep. Curr. Psychiatry Rep. 2017, 19, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treadway, M.T.; Zald, D.H. Reconsidering Anhedonia in Depression: Lessons from Translational Neuroscience. Neurosci. Biobehav. Rev. 2011, 35, 537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siwek, M. Anhedonia w Zaburzeniach Depresyjnych. Psychiatr. I Psychol. Klin. 2017, 17, 216–224. [Google Scholar] [CrossRef]
- Cubała, W.J.; Landowski, J. Trazodone in Common Clinical Practice. Psychiatria (Psychiatry) 2011, 8, 1–6. [Google Scholar]
- Fagiolini, A.; Comandini, A.; Dell’Osso, M.C.; Kasper, S. Rediscovering Trazodone for the Treatment of Major Depressive Disorder. CNS Drugs 2012, 26, 1033–1049. [Google Scholar] [CrossRef] [Green Version]
- Papakostas, G.I.; Fava, M. A Meta-Analysis of Clinical Trials Comparing the Serotonin (5HT)-2 Receptor Antagonists Trazodone and Nefazodone with Selective Serotonin Reuptake Inhibitors for the Treatment of Major Depressive Disorder. Eur. Psychiatry 2007, 22, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Khazaie, H.; Rezaie, L.; Rezaei Payam, N.; Najafi, F. Antidepressant-Induced Sexual Dysfunction during Treatment with Fluoxetine, Sertraline and Trazodone; a Randomized Controlled Trial. Gen. Hosp. Psychiatry 2015, 37, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Fagiolini, A.; Albert, U.; Ferrando, L.; Herman, E.; Muntean, C.; Pálová, E.; Cattaneo, A.; Comandini, A.; di Dato, G.; di Loreto, G.; et al. A Randomized, Double-Blind Study Comparing the Efficacy and Safety of Trazodone Once-a-Day and Venlafaxine Extended-Release for the Treatment of Patients with Major Depressive Disorder. Int. Clin. Psychopharmacol. 2020, 35, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Buoli, M.; Rovera, C.; Pozzoli, S.M.; Fiorentini, A.; Cremaschi, L.; Caldiroli, A.; Altamura, A.C. Is Trazodone More Effective than Clomipramine in Major Depressed Outpatients? A Single-Blind Study with Intravenous and Oral Administration. CNS Spectr. 2019, 24, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Preskorn, S.H.; Macaluso, M.; Trivedi, M. How Commonly Used Inclusion and Exclusion Criteria in Antidepressant Registration Trials Affect Study Enrollment. J. Psychiatr. Pract. 2015, 21, 267–274. [Google Scholar] [CrossRef]
- Samochowiec, J.; Dudek, D.; Kucharska-Mazur, J.; Murawiec, S.; Rymaszewska, J.; Cubała, W.; Heitzman, J.; Szulc, A.; Bała, M.; Gałecki, P. Pharmacological treatment of a depressive episode and recurrent depressive disorder—Guidelines of the Polish Psychiatric Association and the National Consultant for Adult Psychiatry. Psychiatr. Pol. 2021, 55, 235–259. [Google Scholar] [CrossRef]
- RCoreTeam. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austra, 2022. [Google Scholar]
- Fried, E.I. The 52 Symptoms of Major Depression: Lack of Content Overlap among Seven Common Depression Scales. J. Affect. Disord. 2017, 208, 191–197. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Rush, A.J.; Wisniewski, S.R.; Nierenberg, A.A.; Warden, D.; Ritz, L.; Norquist, G.; Howland, R.H.; Lebowitz, B.; McGrath, P.J.; et al. Evaluation of Outcomes with Citalopram for Depression Using Measurement-Based Care in STAR*D: Implications for Clinical Practice. Am. J. Psychiatry 2006, 163, 28–40. [Google Scholar] [CrossRef]
- Cuomo, A.; Ballerini, A.; Bruni, A.C.; Decina, P.; di Sciascio, G.; Fiorentini, A.; Scaglione, F.; Vampini, C.; Fagiolini, A. Clinical Guidance for the Use of Trazodone in Major Depressive Disorder and Concomitant Conditions: Pharmacology and Clinical Practice. Riv. Psichiatr. 2019, 54, 137–149. [Google Scholar] [CrossRef]
- Altamura, A.C.; Mauri, M.C.; Rudas, N.; Carpiniello, B.; Montanini, R.; Perini, M.; Scapicchio, P.L.; Hadjchristos, C.; Carucci, G.; Minervini, M.; et al. Clinical Activity and Tolerability of Trazodone, Mianserin, and Amitriptyline in Elderly Subjects with Major Depression: A Controlled Multicenter Trial. Clin. Neuropharmacol. 1989, 12 (Suppl. 1), S25–S33. [Google Scholar] [CrossRef]
- Ather, S.A.; Ankier, S.I.; Middleton, R.S.W. A Double-Blind Evaluation of Trazodone in the Treatment of Depression in the Elderly. Br. J. Clin. Pract. 1985, 39, 192–199. [Google Scholar] [PubMed]
- Gerner, R.; Estabrook, W.; Steuer, J.; Jarvik, L. Treatment of Geriatric Depression with Trazodone, Imipramine, and Placebo: A Double-Blind Study. J. Clin. Psychiatry 1980, 41, 216–220. [Google Scholar] [PubMed]
- Blacker, R.; Shanks, N.J.; Chapman, N.; Davey, A. The Drug Treatment of Depression in General Practice: A Comparison of Nocte Administration of Trazodone with Mianserin, Dothiepin and Amitriptyline. Psychopharmacology 1988, 95, S18–S24. [Google Scholar] [CrossRef] [PubMed]
- Beasley, C.M.; Dornseif, B.E.; Pultz, J.A.; Bosomworth, J.C.; Sayler, M.E. Fluoxetine versus Trazodone: Efficacy and Activating-Sedating Effects. J. Clin. Psychiatry 1991, 52, 294–299. [Google Scholar]
- Munizza, C.; Olivieri, L.; di Loreto, G.; Dionisio, P. A Comparative, Randomized, Double-Blind Study of Trazodone Prolonged-Release and Sertraline in the Treatment of Major Depressive Disorder. Curr. Med. Res. Opin. 2006, 22, 1703–1713. [Google Scholar] [CrossRef]
- Kasper, S.; Olivieri, L.; di Loreto, G.; Dionisio, P. A Comparative, Randomised, Double-Blind Study of Trazodone Prolonged-Release and Paroxetine in the Treatment of Patients with Major Depressive Disorder. Curr. Med. Res. Opin. 2005, 21, 1139–1146. [Google Scholar] [CrossRef]
- Cunningham, L.A.; Borison, R.L.; Carman, J.S.; Chouinard, G.; Crowder, J.E.; Diamond, B.I.; Fischer, D.E.; Hearst, E. A Comparison of Venlafaxine, Trazodone, and Placebo in Major Depression. J. Clin. Psychopharmacol. 1994, 14, 99–106. [Google Scholar] [CrossRef]
- Weisler, R.H.; Johnston, J.A.; Lineberry, C.G.; Samara, B.; Branconnier, R.J.; Billow, A.A. Comparison of Bupropion and Trazodone for the Treatment of Major Depression. J. Clin. Psychopharmacol. 1994, 14, 170–179. [Google Scholar] [CrossRef]
- van Moffaert, M.; de Wilde, J.; Vereecken, A.; Dierick, M.; Evrard, J.L.; Wilmotte, J.; Mendlewiez, J. Mirtazapine Is More Effective than Trazodone: A Double-Blind Controlled Study in Hospitalized Patients with Major Depression. Int. Clin. Psychopharmacol. 1995, 10, 3–10. [Google Scholar] [CrossRef]
- Demyttenaere, K.; Kiekens, G.; Bruffaerts, R.; Mortier, P.; Gorwood, P.; Martin, L.; di Giannantonio, M. Outcome in Depression (I): Why Symptomatic Remission Is Not Good Enough. CNS Spectr. 2021, 26, 393–399. [Google Scholar] [CrossRef]


{kind=link}
| SSRI (n = 34) | Trazodone XR (n = 42) | p | |
|---|---|---|---|
| Sex (% female) | 64.7 | 61.9 | 0.801 a |
| Age (in years): mean (SD) | 39.1 (12.6) | 35.4 (12.8) | 0.230 b |
| Weight (in kilograms): median (25th; 75th percentile) | 70 (58.5; 76) | 68 (60; 80) | 0.945 c |
| Duration of previous psychiatric treatment (in months): median (25th; 75th percentile) | 0 (0; 9.75) | 12 (0; 60) | 0.044 c |
| Alcohol consumption (% yes) | 69.2 | 76.9 | 0.489 a |
| Smoking (% yes) | 12 | 23.1 | 0.338 a |
| Somatic comorbidities (% yes) | 43.3 | 40 | 0.779 a |
| Psychotherapy (% yes) | 44 | 52.5 | 0.505 a |
| QIDS-CR: mean (SD) | 12.7 (4.1) | 14.8 (4.3) | 0.033 b |
| QIDS-SR: mean (SD) | 13.3 (4.8) | 15.9 (4.6) | 0.049 b |
| MADRS: mean (SD) | 27 (7.8) | 28.7 (7) | 0.345 b |
| SHAPS: median (25th; 75th percentile) | 6 (2; 10.3) | 8 (3.3; 12) | 0.433 c |
| HAMA: mean (SD) | 18.9 (7.3) | 22.9 (7.6) | 0.027 b |
| AIS: mean (SD) | 9.4 (5.4) | 14.5 (6.1) | <0.001 b |
| SDS: mean (SD) | 15.3 (7.8) | 19.8 (8.1) | 0.031 b |
| Time Effect, p | Treatment Effect, p | Time–Treatment Effect, p | Partial Eta Squared for Interaction (with 95% CI) | |
|---|---|---|---|---|
| MDRS | <0.001 | 0.9004 | 0.1724 | 0.03 (0.00–0.06) |
| QIDS-CR | <0.001 | 0.782 | 0.007 | 0.06 (0.01–0.11) |
| QIDS-SR | <0.001 | 0.820 | 0.006 | 0.06 (0.01–0.12) |
| HAM-A | <0.001 | 0.546 | 0.004 | 0.06 (0.01–0.12) |
| AIS | <0.001 | 0.640 | <0.001 | 0.17 (0.09–0.25) |
| SDS | <0.001 | 0.123 | 0.046 | 0.05 (0.00–0.10) |
| SHAPS | <0.001 | 0.643 | 0.145 | 0.03 (0.00–0.06) |
| Baseline Emmean (95% CI) | 2 Weeks Emmean (95% CI) | 4 Weeks Emmean (95% CI) | 8 Weeks Emmean (95% CI) | 12 Weeks Emmean (95% CI) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SSRI | T-XR | p | SSRI | T-XR | p | SSRI | T-XR | p | SSRI | T-XR | p | SSRI | T-XR | p | |
| MDRS | 27.1 (24.2–29.9) | 28.5 (24.2–29.9) | 0.456 | 20.7 (17.6–23.7) | 22.6 (19.9–25.4) | 0.356 | 13.6 (10.5–16.7) | 14.6 (11.9–17.3) | 0.629 | 10.4 (7.1–13.7) | 8.3 (5.5–11.2) | 0.345 | 8.2 (5–11.5) | 5 (2.1–7.9) | 0.152 |
| QIDS-CR | 12.7 (11.1–14.3) | 14.9 (13.4–16.3) | 0.057 | 10 (8.3–11.8) | 11.1 (9.6–12.7) | 0.348 | 7.5 (5.7–9.4) | 7.3 (5.7–8.9) | 0.826 | 6 (4.2–7.9) | 4.4 (2.8–6.1) | 0.206 | 5.2 (3.4–7.1) | 2.7 (1–4.4) | 0.048 |
| QIDS- SR | 13 (11.2–14.8) | 15.6 (13.8–17.4) | 0.044 | 10.6 (8.8–12.4) | 12.8 (11.2–14.4) | 0.082 | 8.7 (6.9–10.5) | 8.2 (6.5–9.8) | 0.682 | 6.7 (4.8–8.6) | 5.5 (3.8–7.3) | 0.364 | 6 (4.1–7.9) | 3.9 (2.1–5.6) | 0.105 |
| HAM-A | 18.9 (16.6–21.2) | 22.8 (20.6–25) | 0.017 | 12.1 (9.7–14.6) | 14.9 (12.72–17.1) | 0.099 | 7.9 (5.4–10.4) | 8.4 (6.2–10.6) | 0.764 | 6.2 (3.7–8.7) | 4.6 (2.3–6.8) | 0.343 | 4.9 (2.4–7.5) | 3.2 (0.9–5.5) | 0.318 |
| AIS | 9.4 (7.8–11.1) | 14.5 (13–16) | <0.001 | 9 (7.3–10.8) | 9.5 (8–11.1) | 0.669 | 8.3 (6.6–10.1) | 5.6 (4–7.2) | 0.025 | 6.1 (4.3–7.9) | 4.3 (2.6–6) | 0.152 | 6 (4.2–7.9) | 3 (1.3–4.7) | 0.017 |
| SDS | 15.5 (12.7–18.4) | 20.3 (17.8–22.8) | 0.014 | 13.3 (10.3–16.3) | 18.2 (15.7–20.7) | 0.014 | 10.8 (7.7–13.8) | 11.6 (9–14.1) | 0.695 | 7.9 (4.9–11) | 9.2 (6.6–11.9) | 0.527 | 6.5 (3.4–9.6) | 6.2 (3.5–8.8) | 0.877 |
| SHAPS | 6.5 (4.9–8) | 7.4 (6–8.8) | 0.400 | 5.4 (3.8–7.1) | 6.5 (5.1–8) | 0.315 | 5.3 (3.7–7) | 3.9 (2.4–5.5) | 0.220 | 3.6 (1.9–5.3) | 2.8 (1.2–4.3) | 0.481 | 3.5 (1.7–5.2) | 2 (0.4–3.6) | 0.210 |
| Time Effect, p | Treatment Effect, p | Time–Treatment Effect, p | Partial Eta Squared for Interaction (with 95% CI) | |
|---|---|---|---|---|
| MDRS | 0.022 | 0.851 | 0.368 | 0.02 (0.00–0.06) |
| QIDS-CR | <0.001 | 0.931 | 0.046 | 0.05 (0.00–0.10) |
| QIDS-SR | <0.001 | 0.534 | 0.065 | 0.05 (0.00–0.11) |
| HAM-A | <0.001 | 0.461 | 0.057 | 0.05 (0.00–0.10) |
| AIS | <0.001 | 0.458 | <0.001 | 0.13 (0.04–0.21) |
| SDS | <0.001 | 0.251 | 0.151 | 0.04 (0.00–0.09) |
| SHAPS | <0.001 | 0.829 | 0.148 | 0.03 (0.00–0.06) |
| SSRI (Mean Change: After 12 Weeks–Baseline Score; 95% CI) | p | Trazodone XR (Mean Change: After 12 Weeks–Baseline Score; 95% CI) | p | |
|---|---|---|---|---|
| MADRS | −19.5 (−23.9; −15) | <0.001 | −24.8 (−29.1; −20.5) | <0.001 |
| QIDS-CR | −7 (−9.62; −4.38) | <0.001 | −12.8 (−15.5; −10.1) | <0.001 |
| QIDS-SR | −6.1 (−9.3; −3) | <0.001 | −12.4 (−16.2; −8.6) | <0.001 |
| HAM-A | −13.5 (−17; −10.1) | <0.001 | −20.6 (−23.3; −18) | <0.001 |
| AIS | −3.7 (−5.7; −1.8) | <0.001 | −12.5 (−15.4; −9.5) | <0.001 |
| SDS | −9.4 (−14.2; −4.5) | <0.001 | −16 (−20.9; −11.1) | <0.001 |
| SHAPS | −3.4 (−5.7; −1.2) | 0.027 | −6.2 (−8.7; −3.8) | <0.001 |
| Weight (in kg) | 0.1 (−1; 1.1) | 0.746 | −0.15 (−1.8; 1.5) | 0.629 |
| SSRI | Trazodone XR | p | |
|---|---|---|---|
| Therapeutic response (≥50% reduction in QIDS score after 12 weeks), % of patients | 64 | 83.9 | 0.088 a |
| Therapeutic response (≥50% reduction in MADRS score after 12 weeks), % of patients | 79.2 | 79.3 | 0.999 b |
| Therapeutic response (≥50% reduction in QIDS-SR score after 12 weeks), % of patients | 65 | 70 | 0.739 a |
| Remission (<6 points on QIDS-CR scale) after 12 weeks, % of patients | 64 | 83.9 | 0.088 a |
| Remission (<10 points on MADRS scale) after 12 weeks, % of patients | 70.8 | 80.6 | 0.396 a |
| Remission (<6 points on QIDS-SR scale) after 12 weeks, % of patients | 60 | 69 | 0.492 a |
| CGI-I score of 1 or 2 after 12 weeks of treatment, % of patients | 77.3 | 77.3 | >0.999 a |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siwek, M.; Gorostowicz, A.; Chrobak, A.A.; Gerlich, A.; Krupa, A.J.; Juryk, A.; Dudek, D. TED—Trazodone Efficacy in Depression: A Naturalistic Study on the Efficacy of Trazodone in an Extended-Release Formulation Compared to SSRIs in Patients with a Depressive Episode—Preliminary Report. Brain Sci. 2023, 13, 86. https://doi.org/10.3390/brainsci13010086
Siwek M, Gorostowicz A, Chrobak AA, Gerlich A, Krupa AJ, Juryk A, Dudek D. TED—Trazodone Efficacy in Depression: A Naturalistic Study on the Efficacy of Trazodone in an Extended-Release Formulation Compared to SSRIs in Patients with a Depressive Episode—Preliminary Report. Brain Sciences. 2023; 13(1):86. https://doi.org/10.3390/brainsci13010086
Chicago/Turabian StyleSiwek, Marcin, Aleksandra Gorostowicz, Adrian Andrzej Chrobak, Adrian Gerlich, Anna Julia Krupa, Andrzej Juryk, and Dominika Dudek. 2023. "TED—Trazodone Efficacy in Depression: A Naturalistic Study on the Efficacy of Trazodone in an Extended-Release Formulation Compared to SSRIs in Patients with a Depressive Episode—Preliminary Report" Brain Sciences 13, no. 1: 86. https://doi.org/10.3390/brainsci13010086