

Risk Factors for Delirium after Deep Brain Stimulation Surgery under Total Intravenous Anesthesia in Parkinson’s Disease Patients
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
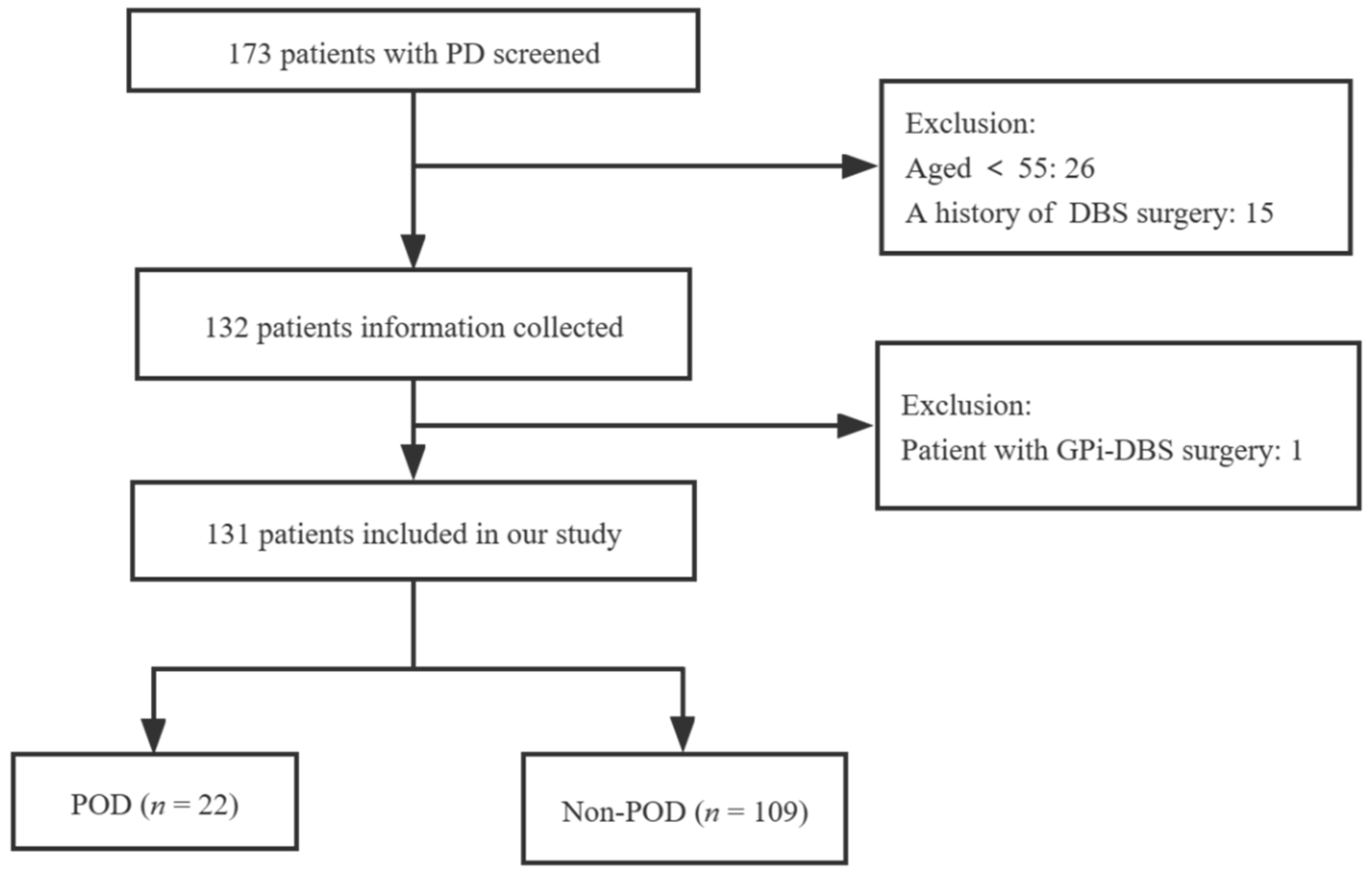
2.2. Participants
2.3. Assessment of Delirium
2.4. Surgical Procedure and Anesthesia Method
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. General Patient Information
3.2. Parkinson’s Motor Symptoms and Non-Motor Symptoms
3.3. Anesthetic and Postoperative Brain Imaging Data
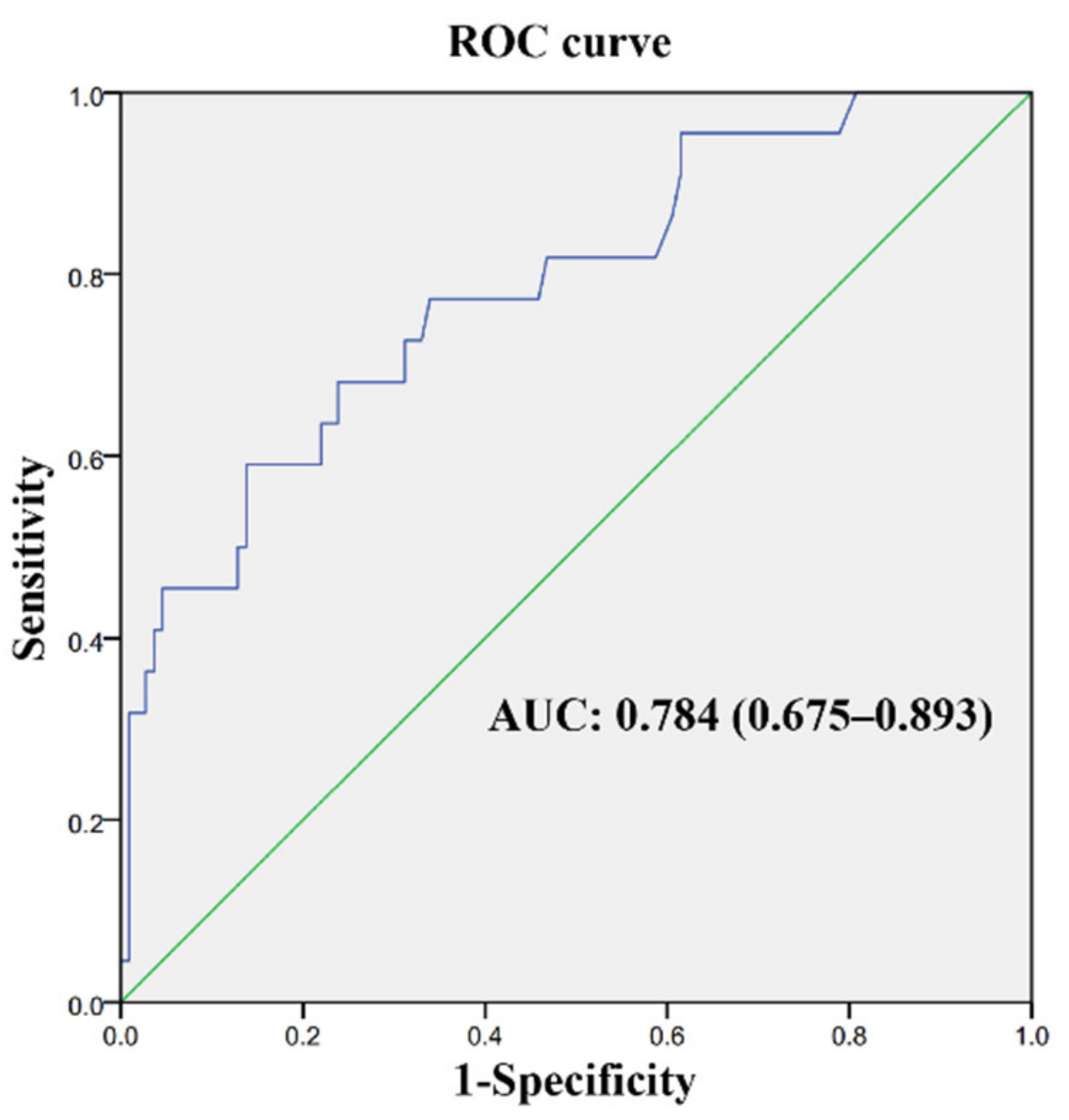
3.4. Risk Factors for Delirium after STN-DBS Surgery
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, C.; Edwards, C.; Lin, C.; Jones, E.; Yanek, L.; Esmaili, M.; Gorashi, Y.; Skelton, R.; Kaganov, D.; Curto, R.; et al. Spinal Anesthesia with Targeted Sedation based on Bispectral Index Values Compared with General Anesthesia with Masked Bispectral Index Values to Reduce Delirium: The SHARP Randomized Controlled Trial. Anesthesiology 2021, 135, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Li, J.; Yuan, L.; Wu, J.; Jiang, C.; Daniels, J.; Mehta, R.; Wang, M.; Yeung, J.; Jackson, T.; et al. Effect of Regional vs General Anesthesia on Incidence of Postoperative Delirium in Older Patients Undergoing Hip Fracture Surgery: The RAGA Randomized Trial. JAMA 2022, 327, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Lenka, A.; Mittal, S.; Lamotte, G.; Pagan, F. A Pragmatic Approach to the Perioperative Management of Parkinson’s Disease. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2021, 48, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, M.; Okun, M. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA 2020, 323, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Tani, N.; Maruo, T.; Oshino, S.; Hosomi, K.; Saitoh, Y.; Kishima, H. Risk Factors for Postoperative Delirium After Deep Brain Stimulation Surgery for Parkinson Disease. World Neurosurg. 2018, 114, e518–e523. [Google Scholar] [CrossRef]
- Zhan, L.; Wang, X.; Zhang, L. Nomogram Model for Predicting Risk of Postoperative Delirium After Deep Brain Stimulation Surgery in Patients Older Than 50 Years with Parkinson Disease. World Neurosurg. 2020, 139, e127–e135. [Google Scholar] [CrossRef]
- Carlson, J.; Neumiller, J.; Swain, L.; Mark, J.; McLeod, P.; Hirschauer, J. Postoperative delirium in Parkinson’s disease patients following deep brain stimulation surgery. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2014, 21, 1192–1195. [Google Scholar] [CrossRef]
- Migirov, A.; Chahar, P.; Maheshwari, K. Postoperative delirium and neurocognitive disorders. Curr. Opin. Crit. Care 2021, 27, 686–693. [Google Scholar] [CrossRef]
- Guidetti, M.; Marceglia, S.; Loh, A.; Harmsen, I.; Meoni, S.; Foffani, G.; Lozano, A.; Moro, E.; Volkmann, J.; Priori, A. Clinical perspectives of adaptive deep brain stimulation. Brain Stimul. 2021, 14, 1238–1247. [Google Scholar] [CrossRef]
- Li, H.; Han, S.; Feng, J. Delirium after Deep Brain Stimulation in Parkinson’s Disease. Park. Dis. 2021, 2021, 8885386. [Google Scholar] [CrossRef]
- Wilt, J.; Merner, A.; Zeigler, J.; Montpetite, M.; Kubu, C. Does Personality Change Follow Deep Brain Stimulation in Parkinson’s Disease Patients? Front. Psychol. 2021, 12, 643277. [Google Scholar] [CrossRef]
- Ishii, K.; Makita, T.; Yamashita, H.; Matsunaga, S.; Akiyama, D.; Toba, K.; Hara, K.; Sumikawa, K.; Hara, T. Total intravenous anesthesia with propofol is associated with a lower rate of postoperative delirium in comparison with sevoflurane anesthesia in elderly patients. J. Clin. Anesth. 2016, 33, 428–431. [Google Scholar] [CrossRef]
- Hamadnalla, H.; Sessler, D.I.; Troianos, C.A.; Fang, J.; Rivas, E.; Ma, C.; Mascha, E.J.; Turan, A. Optimal interval and duration of CAM-ICU assessments for delirium detection after cardiac surgery. J. Clin. Anesth. 2021, 71, 110233. [Google Scholar] [CrossRef]
- Lei, H.; Yang, C.; Zhang, M.; Qiu, Y.; Wang, J.; Xu, J.; Hu, X.; Wu, X. Optimal Contact Position of Subthalamic Nucleus Deep Brain Stimulation for Reducing Restless Legs Syndrome in Parkinson’s Disease Patients: One-Year Follow-Up with 33 Patients. Brain Sci. 2022, 12, 1645. [Google Scholar] [CrossRef]
- Segernäs, A.; Skoog, J.; Andersson, E.A.; Österberg, S.A.; Thulesius, H.; Zachrisson, H. Prediction of Postoperative Delirium After Cardiac Surgery with A Quick Test of Cognitive Speed, Mini-Mental State Examination and Hospital Anxiety and Depression Scale. Clin. Interv. Aging 2022, 17, 359–368. [Google Scholar] [CrossRef]
- Cavallieri, F.; Fraix, V.; Bove, F.; Mulas, D.; Tondelli, M.; Castrioto, A.; Krack, P.; Meoni, S.; Schmitt, E.; Lhommée, E.; et al. Predictors of Long-Term Outcome of Subthalamic Stimulation in Parkinson Disease. Ann. Neurol. 2021, 89, 587–597. [Google Scholar] [CrossRef]
- Wang, X.Q.; Zhuang, H.X.; Zhang, L.X.; Chen, X.; Niu, C.S.; Zhao, M. Nomogram for Predicting Postoperative Delirium After Deep Brain Stimulation Surgery for Parkinson’s Disease. World Neurosurg. 2019, 130, e551–e557. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, Y.; Zhang, X.; Wang, Y.; Li, J.; Li, Y. Cognitive and Psychiatric Effects of STN versus GPi Deep Brain Stimulation in Parkinson’s Disease: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2016, 11, e0156721. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, R.; Khemani, P. Treatment of Advanced Parkinson’s Disease. J. Geriatr. Psychiatry Neurol. 2022, 35, 12–23. [Google Scholar] [CrossRef]
- Oliveira, J.E.; Silva, L.; Berning, M.; Stanich, J.; Gerberi, D.; Murad, M.; Han, J.; Bellolio, F. Risk Factors for Delirium in Older Adults in the Emergency Department: A Systematic Review and Meta-Analysis. Ann. Emerg. Med. 2021, 78, 549–565. [Google Scholar] [CrossRef]
- Bramley, P.; McArthur, K.; Blayney, A.; McCullagh, I. Risk factors for postoperative delirium: An umbrella review of systematic reviews. Int. J. Surg. 2021, 93, 106063. [Google Scholar] [CrossRef]
- Visser, L.; Prent, A.; Banning, L.; van Leeuwen, B.; Zeebregts, C.; Pol, R. Risk Factors for Delirium after Vascular Surgery: A Systematic Review and Meta-Analysis. Ann. Vasc. Surg. 2021, 76, 500–513. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Wang, B.; Yin, J.; Xue, Q.; Gao, S.; Xing, L.; Wang, H.; Liu, W.; Liu, X. Risk factors for postoperative delirium after spinal surgery: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2020, 32, 1417–1434. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Ma, X.; Ye, J.; Liu, C.; Zhou, Z. Systematic review and meta-analysis of risk factor for postoperative delirium following spinal surgery. J. Orthop. Surg. Res. 2020, 15, 509. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, Y.; Yokoyama, Y.; Fukuzawa, S.; Fukata, S.; Ando, M.; Kawamura, T.; Yamada, K.; Nagino, M. Risk Factors for Postoperative Delirium in Abdominal Surgery: A Proposal of a Postoperative Delirium Risk Score in Abdominal Surgery. Dig. Surg. 2017, 34, 95–102. [Google Scholar] [CrossRef]
- Van Keulen, K.; Knol, W.; Belitser, S.V.; van der Linden, P.D.; Heerdink, E.R.; Egberts, T.C.G.; Slooter, A.J.C. Diabetes and Glucose Dysregulation and Transition to Delirium in ICU Patients. Crit. Care Med. 2018, 46, 1444–1449. [Google Scholar] [CrossRef]
- Hughes, C.G.; Patel, M.B.; Pandharipande, P.P. Pathophysiology of acute brain dysfunction: What’s the cause of all this confusion? Curr. Opin. Crit. Care 2012, 18, 518–526. [Google Scholar] [CrossRef]
- Xu, F.; Zhang, L.; Zhou, C.; Mo, J.; Shen, S.; Zhang, T.; Li, J.; Lin, L.; Wu, R.; Gan, L. Alkyl-benzofuran dimers from Eupatorium chinense with insulin-sensitizing and anti-inflammatory activities. Bioorg. Chem. 2021, 113, 105030. [Google Scholar] [CrossRef]
- Liu, M.; He, Y.; Jiang, B.; Wu, L.; Wang, J.; Yang, S.; Wang, Y. Association between metabolic syndrome and mild cognitive impairment and its age difference in a Chinese community elderly population. Clin. Endocrinol. 2015, 82, 844–853. [Google Scholar] [CrossRef]
- Aiello, E.; Grosso, M.; Caracciolo, C.; Andriulo, A.; Buscone, S.; Ottobrini, M.; Luzzatti, C. Diagnostic accuracy of noun- and verb-naming tasks in detecting cognitive impairment in Parkinson’s disease. Neurodegener. Dis. 2021, 21, 146–149. [Google Scholar] [CrossRef]
- Daiello, L.A.; Racine, A.M.; Yun Gou, R.; Marcantonio, E.R.; Xie, Z.; Kunze, L.J.; Vlassakov, K.V.; Inouye, S.K.; Jones, R.N.; Alsop, D.; et al. Postoperative Delirium and Postoperative Cognitive Dysfunction: Overlap and Divergence. Anesthesiology 2019, 131, 477–491. [Google Scholar] [CrossRef] [Green Version]
- Aarsland, D.; Batzu, L.; Halliday, G.; Geurtsen, G.; Ballard, C.; Ray Chaudhuri, K.; Weintraub, D. Parkinson disease-associated cognitive impairment. Nat. Rev. Dis. Prim. 2021, 7, 47. [Google Scholar] [CrossRef]
- Franke, C.; Ebersbach, G. Delirium in idiopathic Parkinson’s disease. Nervenarzt 2020, 91, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Olsen, A.; Feany, M. Parkinson’s disease risk genes act in glia to control neuronal α-synuclein toxicity. Neurobiol. Dis. 2021, 159, 105482. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| POD Group (n = 22) | Non-POD Group (n = 109) | p | |
|---|---|---|---|
| Age (years) | 68.27 ± 6.46 | 64.25 ± 5.65 | <0.01 |
| Male | 15 (68.2) | 56 (51.4) | 0.15 |
| BMI (kg/m2) | 24.19 ± 3.65 | 22.88 ± 3.48 | 0.11 |
| ASA (II/III) | 11/11 | 73/36 | 0.13 |
| Education level | 0.47 | ||
| Illiterate school | 2 | 12 | |
| Primary school | 5 | 17 | |
| Middle school | 12 | 52 | |
| Technical secondary school or more | 3 | 28 | |
| Length of hospital stay (days) | 9 (7–10) | 8 (7–9) | 0.18 |
| Hypertension | 7 (31.8) | 29 (26.6) | 0.62 |
| Diabetes | 5 (22.7) | 6 (5.5) | 0.03 |
| Coronary heart disease | 0 | 0 | 1 |
| Operation duration (min) | 135 (130–145) | 130 (120–140) | 0.09 |
| Family history of Parkinson’s disease | 1 (4.5) | 20 (18.3) | 0.20 |
| Disease duration (years) | 9.5 (8–12) | 9 (6–12) | 0.66 |
| VAS pain score | |||
| Postoperative 24 h | 3 (2–4) | 2 (1–3) | 0.02 |
| Postoperative 72 h | 2 (1–3) | 2 (1–2) | 0.23 |
| MMSE score | |||
| Preoperative | 23 (19–28) | 27 (26–29) | <0.01 |
| Postoperative 24 h | 18 (11–23) | 26 (23–28) | <0.0001 |
| Postoperative 72 h | 18 (13–23) | 26 (23–28) | <0.0001 |
| Postoperative 1 month | 22 (17–24) | 27 (25–28) | <0.0001 |
| Postoperative hallucination | 1 | 2 | 0.427 |
| Preoperative serum albumin (g/dl) | 44 (42–45) | 43 (42–45) | 0.69 |
| Serum Na (mmol/L) | |||
| Preoperative | 143 (142–144) | 144 (142–145) | 0.04 |
| Postoperative 24 h | 142 (140–143) | 142 (141–144) | 0.20 |
| Serum Cl (mmol/L) | |||
| Preoperative | 105 (103–106) | 106 (104–107) | 0.04 |
| Postoperative 24 h | 106 (105–108) | 106 (104–108) | 0.95 |
| Serum K (mmol/L) | |||
| Preoperative | 3.8 (3.7–4.2) | 3.9 (3.7–4.1) | 0.56 |
| Postoperative 24 h | 3.9 (3.7–4.1) | 3.9 (3.8–4.1) | 0.63 |
| Serum glucose (mmol/L) | |||
| Preoperative | 5.4 (5.3–6.3) | 5.3 (4.9–5.7) | 0.03 |
| Postoperative 24 h | 5.8 (5.5–6.6) | 5.6 (5.2–6.4) | 0.14 |
| POD Group (n = 22) | Non-POD Group (n = 109) | p | |
|---|---|---|---|
| Levodopa equivalent daily dose (mg/d) | 641.67 (550–850) | 675 (520.84–900) | 0.90 |
| Rigidity | 22 (100) | 109 (100) | 1 |
| Tremor | 20 (90.9) | 94 (86.2) | 0.81 |
| Freezing of gait | 11 (50) | 54 (49.5) | 0.81 |
| Postural reflex impairment | 20 (90.9) | 104 (95.4) | 0.74 |
| Muscle weakness | 22 (100) | 109 (100) | 1 |
| UPDRS part 1 score | 21 (19–23) | 18 (15–21) | <0.01 |
| UPDRS part 2 score | 35 (27–38) | 26 (22–31) | <0.01 |
| UPDRS part 3 (on state) score | 35 (27–51) | 25 (19–33) | <0.01 |
| UPDRS part 3 (off state) score | 65 (54–85) | 57 (51–67) | 0.01 |
| UPDRS part 4 score | 9 (6–11) | 8 (6–10) | 0.55 |
| UDysRs score | 0 (0–22) | 0 (0–25) | 0.94 |
| NMSS score | 19 (17–21) | 17 (15–19) | <0.01 |
| SSA score | 21 (21–22) | 21 (20–21) | <0.01 |
| Kubota drinking test | 20 | 94 | 0.74 |
| KPPS score | 8 (6–12) | 7 (0–12) | 0.30 |
| HAMD score | 13.5 (11–17) | 12 (8–17) | 0.10 |
| HAMA score | 10.5 (7–12) | 9 (7–13) | 0.46 |
| POD Group (n = 22) | Non-POD Group (n = 109) | p | |
|---|---|---|---|
| Drugs | |||
| Propofol (mg) | 790 (640–900) | 750 (620–850) | 0.96 |
| Sufentanil (µg) | 40 (35–40) | 40 (35–40) | 0.74 |
| Remifentanil (mg) | 1.35 (1.2–1.6) | 1.4 (1.2–1.6) | 0.87 |
| Rocuronium (mg) | 50 (50–50) | 50 (50–50) | 0.89 |
| Imaging Data | |||
| Hemorrhage | 10 (45.5) | 20 (18.3) | <0.01 |
| Edema | 12 (54.5) | 35 (32.1) | 0.04 |
| Pneumocephalus | 11 (50.0) | 59 (54.1) | 0.723 |
| OR | 95% CI | p | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Preoperative MMSE score | 0.855 | 0.768 | 0.951 | 0.004 |
| UPDRS part 3 (on state) score | 1.061 | 1.02 | 1.104 | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, W.; Chang, X.; Bo, L.; Qiu, Y.; Zhang, M.; Wang, J.; Wu, X.; Yu, X. Risk Factors for Delirium after Deep Brain Stimulation Surgery under Total Intravenous Anesthesia in Parkinson’s Disease Patients. Brain Sci. 2023, 13, 25. https://doi.org/10.3390/brainsci13010025
Lu W, Chang X, Bo L, Qiu Y, Zhang M, Wang J, Wu X, Yu X. Risk Factors for Delirium after Deep Brain Stimulation Surgery under Total Intravenous Anesthesia in Parkinson’s Disease Patients. Brain Sciences. 2023; 13(1):25. https://doi.org/10.3390/brainsci13010025
Chicago/Turabian StyleLu, Wenbin, Xinning Chang, Lulong Bo, Yiqing Qiu, Mingyang Zhang, Jiali Wang, Xi Wu, and Xiya Yu. 2023. "Risk Factors for Delirium after Deep Brain Stimulation Surgery under Total Intravenous Anesthesia in Parkinson’s Disease Patients" Brain Sciences 13, no. 1: 25. https://doi.org/10.3390/brainsci13010025