

Actigraphic Wake after Sleep Onset and Symptom Severity Correspond with Rumination in Trauma-Exposed Individuals

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Posttraumatic Stress, Depression, and Anxiety
2.2.2. Repetitive Negative Thinking
2.2.3. Sleep
2.3. Clinical and Sleep Characteristics
2.4. Statistical Analyses
3. Results
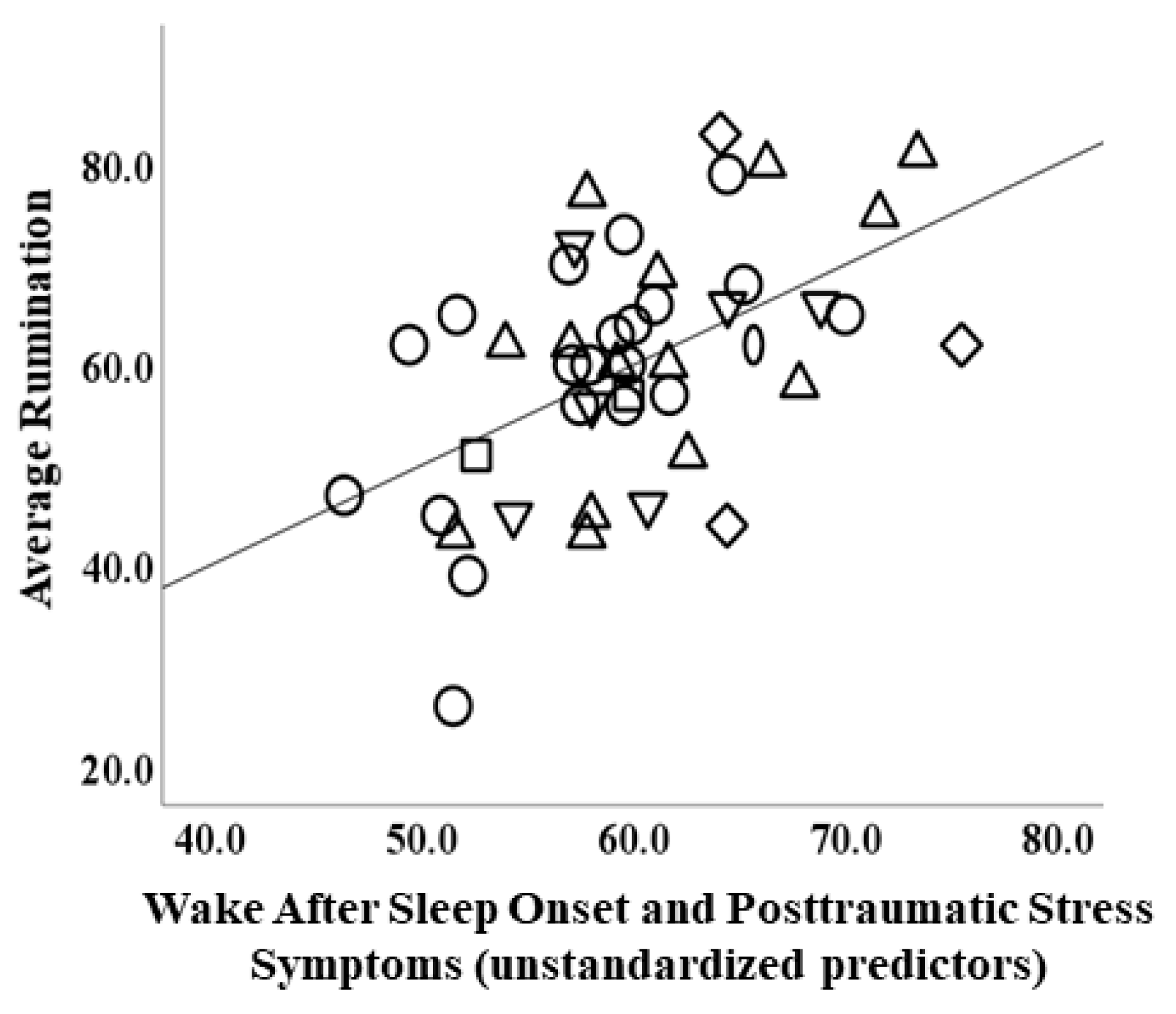
3.1. Rumination
3.2. Worry
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kilpatrick, D.G.; Resnick, H.S.; Milanak, M.E.; Miller, M.W.; Keyes, K.M.; Friedman, M.J. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. J. Trauma. Stress 2013, 26, 537–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolen-Hoeksema, S. Ruminative coping and adjustment to bereavement. In Handbook of Bereavement Research: Consequences, Coping, and Care; Stroebe, M.S., Hansson, R.O., Stroebe, W., Schut, H., Eds.; American Psychological Association: Washington, DC, USA, 2001; pp. 545–562. [Google Scholar] [CrossRef]
- Borkovec, T.; Robinson, E.; Pruzinsky, T.; DePree, J.A. Preliminary exploration of worry: Some characteristics and processes. Behav. Res. Ther. 1983, 21, 9–16. [Google Scholar] [CrossRef]
- Brady, K.T.; Killeen, T.K.; Brewerton, T.; Lucerini, S. Comorbidity of psychiatric disorders and posttraumatic stress disorder. J. Clin. Psychiatry 2000, 61, 22–32. [Google Scholar] [PubMed]
- Spinhoven, P.; Penninx, B.W.; van Hemert, A.M.; de Rooij, M.; Elzinga, B.M. Comorbidity of PTSD in anxiety and depressive disorders: Prevalence and shared risk factors. Child Abus. Negl. 2014, 38, 1320–1330. [Google Scholar] [CrossRef]
- Mennin, D.S.; Fresco, D.M. What, me worry and ruminate about DSM-5 and RDoC? The importance of targeting negative self-referential processing. Clin. Psychol. Sci. Pract. 2013, 20, 258–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEvoy, P.M.; Brans, S. Common versus unique variance across measures of worry and rumination: Predictive utility and mediational models for anxiety and depression. Cogn. Ther. Res. 2012, 37, 183–196. [Google Scholar] [CrossRef] [Green Version]
- Seligowski, A.V.; Lee, D.; Bardeen, J.R.; Orcutt, H.K. Emotion regulation and posttraumatic stress symptoms: A meta-analysis. Cogn. Behav. Ther. 2014, 44, 87–102. [Google Scholar] [CrossRef]
- Spinhoven, P.; Penninx, B.W.; Krempeniou, A.; van Hemert, A.M.; Elzinga, B. Trait rumination predicts onset of Post-Traumatic Stress Disorder through trauma-related cognitive appraisals: A 4-year longitudinal study. Behav. Res. Ther. 2015, 71, 101–109. [Google Scholar] [CrossRef]
- Topper, M.; Molenaar, D.; Emmelkamp, P.M.; Ehring, T. Are rumination and worry two sides of the same coin? A structural equation modelling approach. J. Exp. Psychopathol. 2014, 5, 363–381. [Google Scholar] [CrossRef]
- Fox, E.; Dutton, K.; Yates, A.; Georgiou, G.A.; Mouchlianitis, E. Attentional control and suppressing negative thought intrusions in pathological worry. Clin. Psychol. Sci. 2015, 3, 593–606. [Google Scholar] [CrossRef] [Green Version]
- Stout, D.M.; Shackman, A.J.; Johnson, J.S.; Larson, C.L. Worry is associated with impaired gating of threat from working memory. Emotion 2015, 15, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Whitmer, A.J.; Gotlib, I.H. An attentional scope model of rumination. Psychol. Bull. 2013, 139, 1036–1061. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Cao, S.; Shields, G.S.; Teng, Z.; Liu, Y. The relationships between rumination and core executive functions: A meta-analysis. Depress. Anxiety 2016, 34, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Dinges, D.F. A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychol. Bull. 2010, 136, 375–389. [Google Scholar] [CrossRef] [Green Version]
- Koren, D.; Arnon, I.; Lavie, P.; Klein, E. Sleep complaints as early predictors of Posttraumatic Stress Disorder: A 1-year prospective study of injured survivors of motor vehicle accidents. Am. J. Psychiatry 2002, 159, 855–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krakow, B.; Germain, A.; Warner, T.D.; Schrader, R.; Koss, M.; Hollifield, M.; Tandberg, D.; Melendrez, D.; Johnston, L. The relationship of sleep quality and posttraumatic stress to potential sleep disorders in sexual assault survivors with nightmares, insomnia, and PTSD. J. Trauma. Stress 2001, 14, 647–665. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Shapiro, C.M. Sleep disturbances and psychiatric disorders associated with posttraumatic stress disorder in the general population. Compr. Psychiatry 2000, 41, 469–478. [Google Scholar] [CrossRef] [PubMed]
- van Liempt, S.; van Zuiden, M.; Westenberg, H.; Super, A.; Vermetten, E. Impact of impaired sleep on the development of ptsd symptoms in combat veterans: A prospective longitudinal cohort study. Depress. Anxiety 2013, 30, 469–474. [Google Scholar] [CrossRef]
- Ahmadi, R.; Rahimi-Jafari, S.; Olfati, M.; Javaheripour, N.; Emamian, F.; Ghadami, M.R.; Khazaie, H.; Knight, D.C.; Tahmasian, M.; Sepehry, A.A. Insomnia and post-traumatic stress disorder: A meta-analysis on interrelated association (n = 57,618) and prevalence (n = 573,665). Neurosci. Biobehav. Rev. 2022, 141, 104850. [Google Scholar]
- Koffel, E.; Khawaja, I.S.; Germain, A. Sleep disturbances in Posttraumatic Stress Disorder: Updated review and implications for treatment. Psychiatr. Ann. 2016, 46, 173–176. [Google Scholar] [CrossRef]
- Pfaff, A.; Schlarb, A.A. Child maltreatment and sleep: Two pathways explaining the link. J. Sleep Res. 2021, 31, e13455. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, R.H.; Morgan, C.A.; Southwick, S.M. Sleep quality in treatment-seeking veterans of Operations Enduring Freedom and Iraqi Freedom: The role of cognitive coping strategies and unit cohesion. J. Psychosom. Res. 2010, 69, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Nota, J.A.; Coles, M.E. Duration and timing of sleep are associated with repetitive negative thinking. Cogn. Ther. Res. 2014, 39, 253–261. [Google Scholar] [CrossRef]
- Takano, K.; Iijima, Y.; Tanno, Y. Repetitive thought and self-reported sleep disturbance. Behav. Ther. 2012, 43, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Zoccola, P.M.; Dickerson, S.S.; Lam, S. Rumination predicts longer sleep onset latency after an acute psychosocial stressor. Psychosom. Med. 2009, 71, 771–775. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Williams, J.; Karg, R.; Spitzer, R.L. Structured Clinical Interview for DSM-5—Research Version (SCID-5 for DSM-5, Research Version; SCID-5-RV); American Psychiatric Association: Washington, DC, USA, 2015. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Carlson, E.B.; Smith, S.R.; Palmieri, P.A.; Dalenberg, C.; Ruzek, J.I.; Kimerling, R.; Burling, T.A.; Spain, D.A. Development and validation of a brief self-report measure of trauma exposure: The Trauma History Screen. Psychol. Assess. 2011, 23, 463–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weathers, F.W.; Litz, B.T.; Herman, D.; Huska, J.; Keane, T. The PTSD Checklist-Civilian Version (PCL-C); National Center for PTSD: Boston, MA, USA, 1994; p. 10. [Google Scholar]
- Conybeare, D.; Behar, E.; Solomon, A.; Newman, M.G.; Borkovec, T.D. The PTSD checklist-Civilian version: Reliability, validity, and factor structure in a nonclinical sample. J. Clin. Psychol. 2012, 68, 699–713. [Google Scholar] [CrossRef]
- Ruggiero, K.J.; Del Ben, K.; Scotti, J.; Rabalais, A.E. Psychometric properties of the PTSD checklist—Civilian version. J. Trauma. Stress 2003, 16, 495–502. [Google Scholar] [CrossRef]
- Hamilton, M. The assessment of anxiety states by rating. Psychol. Psychother. Theory Res. Pract. 1959, 32, 50–55. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S. Responses to depression and their effects on the duration of depressive episodes. J. Abnorm. Psychol. 1991, 100, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Luminet, O. Measurement of depressive rumination and associated constructs. In Depressive Rumination: Nature, Theory and Treatment; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2003; pp. 185–215. [Google Scholar] [CrossRef]
- Meyer, T.J.; Miller, M.L.; Metzger, R.L.; Borkovec, T.D. Development and validation of the Penn State Worry Questionnaire. Behav. Res. Ther. 1990, 28, 487–495. [Google Scholar] [CrossRef]
- Patel, S.R.; Weng, J.; Rueschman, M.; Dudley, K.A.; Loredo, J.S.; Mossavar-Rahmani, Y.; Ramirez, M.; Ramos, A.R.; Reid, K.; Seiger, A.N.; et al. Reproducibility of a standardized actigraphy scoring algorithm for sleep in a US Hispanic/Latino population. Sleep 2015, 38, 1497–1503. [Google Scholar] [CrossRef]
- Martin, J.L.; Hakim, A.D. Wrist actigraphy. Chest 2011, 139, 1514–1527. [Google Scholar] [CrossRef] [PubMed]
- Allison, P.D. Multiple Regression: A Primer; Pine Forge Press: Newbury Park, CA, USA, 1999. [Google Scholar]
- Weisburd, D.; Britt, C. Statistics in Criminal Justice; Springer Science+Business Media: Berlin, Germany, 2013. [Google Scholar]
- Shrivastava, D.; Jung, S.; Saadat, M.; Sirohi, R.; Crewson, K. How to interpret the results of a sleep study. J. Community Hosp. Intern. Med. Perspect. 2014, 4, 24983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szabo, Y.; Warnecke, A.J.; Newton, T.L.; Valentine, J.C. Rumination and posttraumatic stress symptoms in trauma-exposed adults: A systematic review and meta-analysis. Anxiety Stress. Coping 2017, 30, 396–414. [Google Scholar] [CrossRef]
- Cacciaglia, R.; Nees, F.; Grimm, O.; Ridder, S.; Pohlack, S.T.; Diener, S.J.; Liebscher, C.; Flor, H. Trauma exposure relates to heightened stress, altered amygdala morphology and deficient extinction learning: Implications for psychopathology. Psychoneuroendocrinology 2017, 76, 19–28. [Google Scholar] [CrossRef]
- Bei, B.; Milgrom, J.; Ericksen, J.; Trinder, J. Subjective perception of sleep, but not its objective quality, is associated with immediate postpartum mood disturbances in healthy women. Sleep 2010, 33, 531–538. [Google Scholar] [CrossRef] [Green Version]
- McCall, C.; McCall, W. Comparison of actigraphy with polysomnography and sleep logs in depressed insomniacs. J. Sleep Res. 2011, 21, 122–127. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.; Hart, C.; Wing, R.R. Discrepancies between self-reported usual sleep duration and objective measures of total sleep time in treatment-seeking overweight and obese individuals. Behav. Sleep Med. 2015, 14, 539–549. [Google Scholar] [CrossRef] [Green Version]
- Van Den Berg, J.F.; Van Rooij, F.J.A.; Vos, H.; Tulen, J.H.M.; Hofman, A.; Miedema, H.M.; Neven, A.K.; Tiemeier, H.W. Disagreement between subjective and actigraphic measures of sleep duration in a population-based study of elderly persons*. J. Sleep Res. 2008, 17, 295–302. [Google Scholar] [CrossRef]
- Van Ravesteyn, L.M.; Tulen, J.H.M.; Kamperman, A.; Raats, M.E.; Schneider, A.J.; Birnie, E.; Steegers, E.A.P.; Hoogendijk, W.J.G.; Tiemeier, H.; Berg, M.P.L.-V.D. Perceived sleep quality is worse than objective parameters of sleep in pregnant women with a mental disorder. J. Clin. Sleep Med. 2014, 10, 1137–1141. [Google Scholar] [CrossRef]
- Ruscio, A.M.; Ruscio, J.; Keane, T.M. The latent structure of posttraumatic stress disorder: A taxometric investigation of reactions to extreme stress. J. Abnorm. Psychol. 2002, 111, 290. [Google Scholar] [CrossRef] [PubMed]
- Marshall, R.D.; Olfson, M.; Hellman, F.; Blanco, C.; Guardino, M.; Struening, E.L. Comorbidity, impairment, and suicidality in subthreshold PTSD. Am. J. Psychiatry 2001, 158, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Mantua, J.; Gravel, N.; Spencer, R.M.C. Reliability of sleep measures from four personal health monitoring devices compared to research-based actigraphy and polysomnography. Sensors 2016, 16, 646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino, M.; Li, Y.; Rueschman, M.N.; Winkelman, J.W.; Ellenbogen, J.M.; Solet, J.M.; Dulin, H.; Berkman, L.F.; Buxton, O.M. Measuring sleep: Accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep 2013, 36, 1747–1755. [Google Scholar] [CrossRef] [PubMed]
- Harvey, A.G. A cognitive model of insomnia. Behav. Res. Ther. 2002, 40, 869–893. [Google Scholar] [CrossRef]
- Renna, M.E.; Fresco, D.M.; Mennin, D.S. Emotion regulation therapy and its potential role in the treatment of chronic stress-related pathology across disorders. Chronic Stress 2020, 4. [Google Scholar] [CrossRef]


{kind=link}
| Principal Diagnosis | n | % |
|---|---|---|
| Generalized anxiety disorder | 20 | 43.5 |
| Major depressive disorder | 14 | 30.4 |
| Social anxiety disorder | 6 | 13.0 |
| Posttraumatic stress disorder | 3 | 6.5 |
| Panic disorder | 2 | 4.3 |
| Persistent depressive disorder | 1 | 2.2 |
| Comorbidity | n | % |
| Social anxiety disorder | 18 | 39.1 |
| Major depressive disorder | 14 | 30.4 |
| Generalized anxiety disorder | 12 | 26.1 |
| Panic disorder | 10 | 21.7 |
| Posttraumatic stress disorder | 8 | 17.4 |
| Specific phobia | 7 | 15.2 |
| Persistent depressive disorder | 5 | 10.9 |
| Obsessive compulsive disorder | 2 | 4.3 |
| Alcohol abuse | 1 | 2.2 |
| Substance abuse | 1 | 2.2 |
| Trauma Event Type | n | % |
| Sudden death of close family or friend | 19 | 41.3 |
| Suddenly abandoned by spouse, partner, parent or family | 13 | 28.3 |
| Some other sudden event that made you feel very scared, helpless or horrified | 10 | 21.7 |
| Hurricane, flood, earthquake, tornado or fire | 10 | 21.7 |
| Forced or made to have sexual contact (adult) | 9 | 19.6 |
| Hit or kicked hard enough to injure (child) | 8 | 17.4 |
| Sudden move or loss of home and possessions | 7 | 15.2 |
| Seeing someone die suddenly or get badly hurt/killed | 6 | 13.0 |
| Really bad car, boat or airplane accident | 6 | 13.0 |
| Forced or made to have sexual contact (child) | 4 | 8.7 |
| Hit or kicked hard enough to injure (adult) | 3 | 6.5 |
| Really bad accident at work or home | 3 | 6.5 |
| Attacked with gun, knife or weapon | 2 | 4.3 |
| During military service—seeing something horrible or badly scared | 2 | 4.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, F.; Berenz, E.C.; Ajilore, O.; Langenecker, S.A.; Burgess, H.J.; Phan, K.L.; Klumpp, H. Actigraphic Wake after Sleep Onset and Symptom Severity Correspond with Rumination in Trauma-Exposed Individuals. Brain Sci. 2023, 13, 139. https://doi.org/10.3390/brainsci13010139
Chang F, Berenz EC, Ajilore O, Langenecker SA, Burgess HJ, Phan KL, Klumpp H. Actigraphic Wake after Sleep Onset and Symptom Severity Correspond with Rumination in Trauma-Exposed Individuals. Brain Sciences. 2023; 13(1):139. https://doi.org/10.3390/brainsci13010139
Chicago/Turabian StyleChang, Fini, Erin C. Berenz, Olusola Ajilore, Scott A. Langenecker, Helen J. Burgess, K. Luan Phan, and Heide Klumpp. 2023. "Actigraphic Wake after Sleep Onset and Symptom Severity Correspond with Rumination in Trauma-Exposed Individuals" Brain Sciences 13, no. 1: 139. https://doi.org/10.3390/brainsci13010139