
Physical Health in Clinical High Risk for Psychosis Individuals: A Cross-Sectional Study
 , and
, and
Abstract
:1. Introduction
Aims of the Study
2. Materials and Methods
2.1. Participants and Study Design
2.2. Assessment Instruments
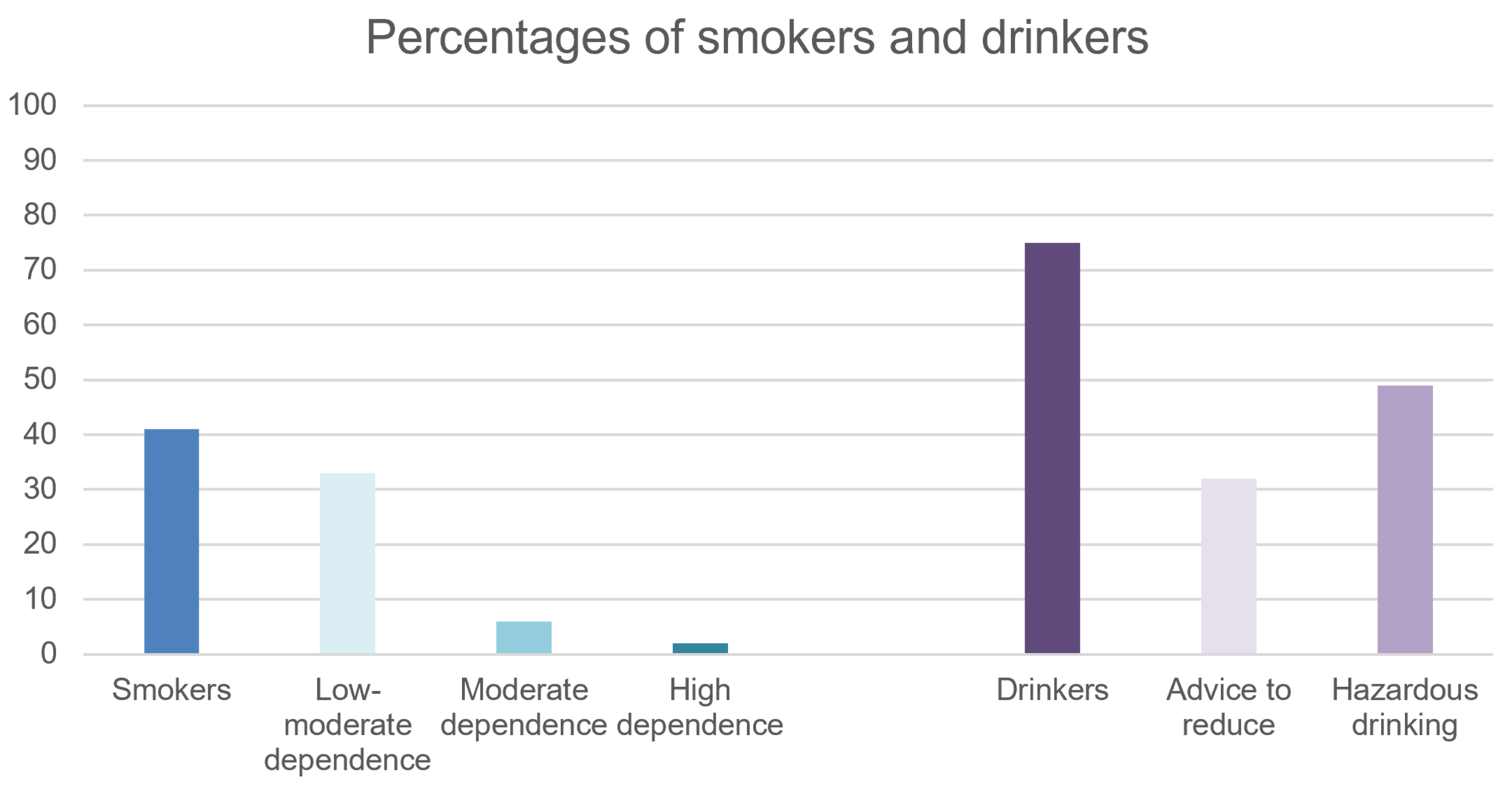
- Fagerström Test for Nicotine Dependence (FTND) [44] is a standardized instrument consisting of 6 questions exploring daily cigarette consumption, compulsive use, and dependence. The score ranges from 0 to 10 (with higher scores indicating a most severe level of dependence to nicotine). More precisely, scorings from 0 to 2 indicate a low level of dependence, from 3 to 4 low-moderate dependence, from 5 to 7 moderate dependence, and more than 8 a high level of dependence. For people that use other types of nicotine consumption other than cigarette smoking (e.g., e-cigarette, nicotine gum, or nicotine patches), we have investigated habits and reported information in adapted versions of FTND already used in the literature (i.e., equivalence of 10 vape nicotine puffs for a cigarette [45] or a re-worded test for gum users [46]).
- AUDIT (Alcohol Use Disorder Identification Test) [47] consists of 10 self-administered questions to investigate alcohol use disorder. When AUDIT-C score, which includes core questions regarding alcohol units consumed and frequency of drinking, is equal or above 4, it might indicate hazardous drinking. Regarding the AUDIT total score, a low level of risk is identified with an overall score between 0 and 7, the range from 8 to 15 is the most appropriate for simple advice focused on the reduction of drinking. Higher scores (up to 19) suggest the need for brief counselling and continuous monitoring, while a complete diagnostic evaluation for alcoholic dependence is warranted for scores 20 and over.
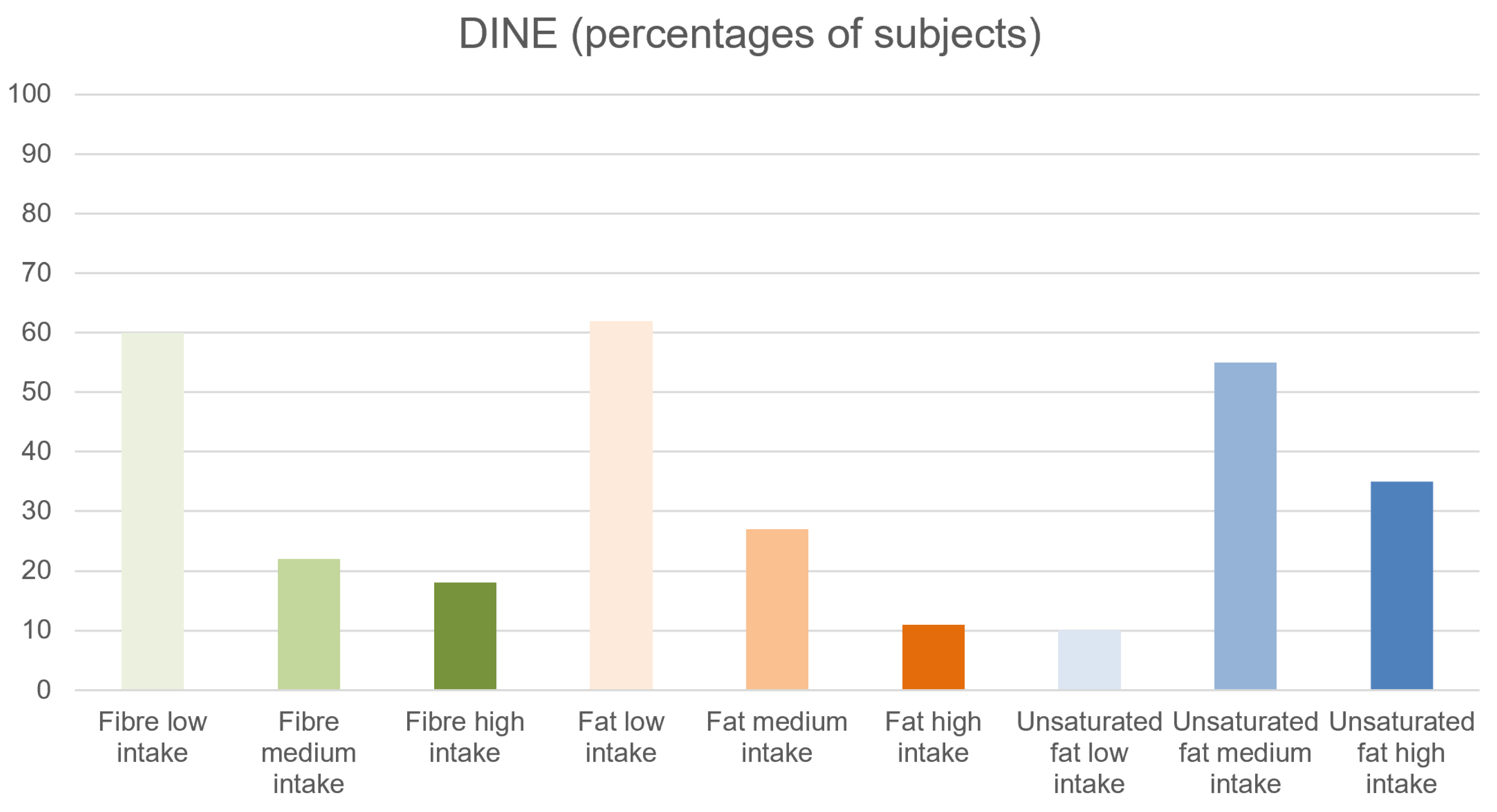
- DINE (Dietary Instrument for Nutritional Education) [48] is a structured interview investigating the intake of dietary fiber and fat (unsaturated and saturated). Scores for fibers and fat are rated into 3 different categories: low (under 30), medium (between 30 and 40), and high intake (more than 40). Scores for unsaturated fat are rated as low (less than 6), medium (6 to 9), and high (more than 9)
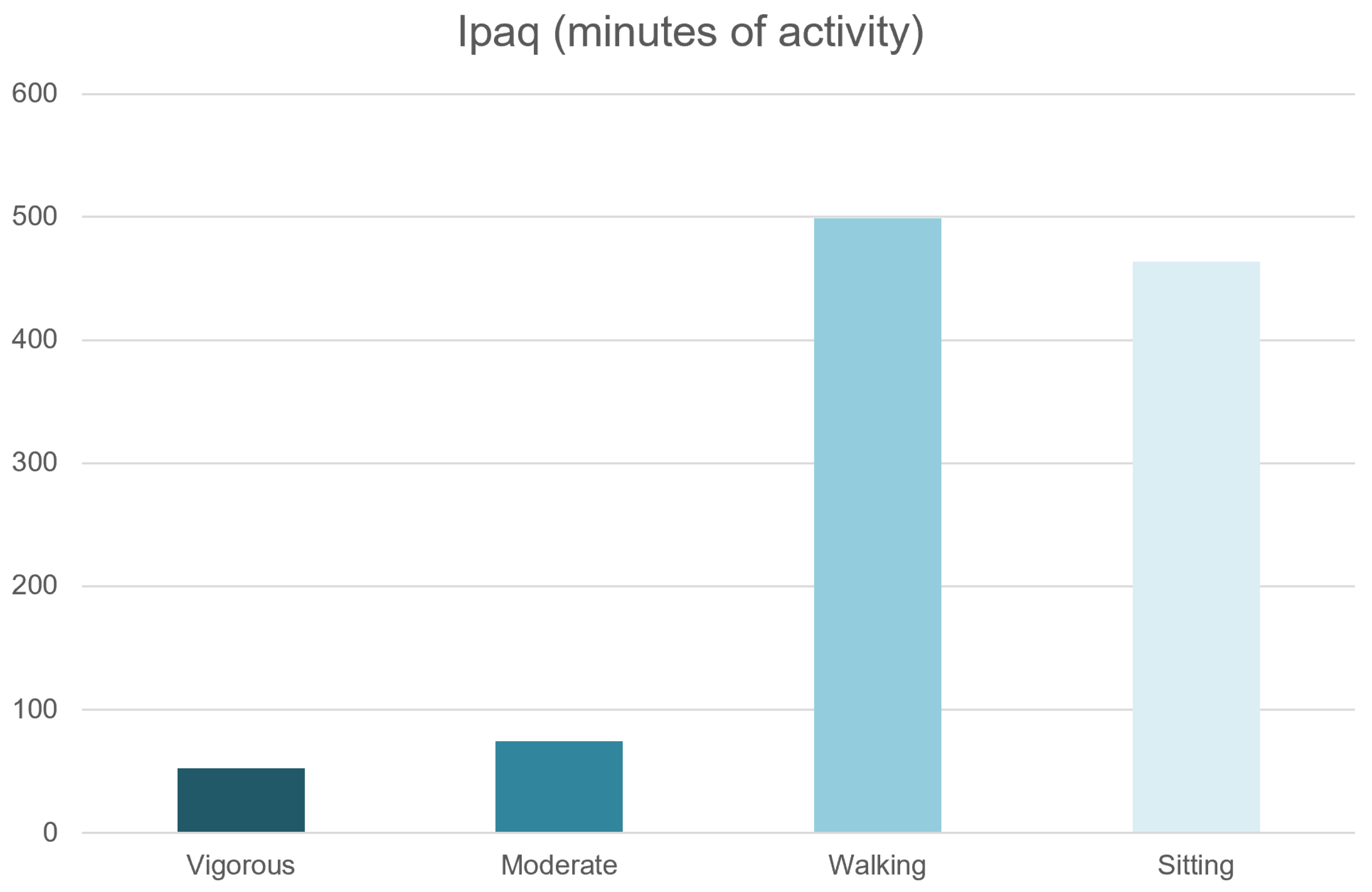
- IPAQ (International Physical Health Questionnaire) [49] rates the level of physical activity. This tool comprises 3 different categories of physical activity based on the intensity (vigorous, moderate, and walking) and quantifies the amount of time spent sitting.
2.3. Variables
- (1)
- Sociodemographic parameters: age, sex, ethnicity
- (2)
- Physical health data:
- 2.1
- Tobacco use: tobacco smoker status (yes/no), number of daily cigarettes, FTND score;
- 2.2
- Alcohol use: alcohol drinker status (yes/no), AUDIT-C and AUDIT total score;
- 2.3
- Type of diet: DINE total score, DINE fiber score, DINE fat score, DINE unsaturated fat score;
- 2.4
- Physical Activity: IPAQ total score (MET), IPAQ vigorous, moderate and walking activity (days per week; minutes per day), IPAQ sitting (minutes per week)
- 2.5
- Physical parameters: weight in kilograms, height in meters, Body Mass Index (BMI), waist circumference in centimeters, heart rate in beats per minute (bpm), respiratory rate in acts per minute (apm), systolic and diastolic pressure in mmHg.
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Physical Health Data in CHR-P Samples
3.2.1. Tobacco Use
3.2.2. Alcohol Use
3.2.3. Type of Diet
3.2.4. Physical Activity
3.2.5. Physical Parameters
3.3. Gender Differences of Physical Health Data in CHR-P Samples
- Tobacco use: differences in the number of smokers were nearly significant (p = 0.08) between male and female subjects (47% vs. 34% respectively).
- Alcohol use: differences were not significant for the number of drinkers (p = 0.60), AUDIT-C score (p = 0.63) and AUDIT total score (p = 0.63) between male and female subjects.
- Type of diet: differences between male and female subjects were non-significant for DINE total (p = 0.28), DINE fiber (p = 0.09), DINE fat (p = 0.10), DINE unsaturated fat (p = 0.69).
- Physical activity: difference between male and female subjects were significant (p < 0.001) for both days (1.80 ± 2.03 vs. 0.66 ± 1.37) and minutes-per-day of vigorous physical activity (70.20 ± 96.35 vs. 18.66 ± 39.34). There were no significant differences between male and female subjects regarding moderate activity, walking, and time spent sitting.
- Physical parameters: significative differences between male and female subjects were detected for weight (p < 0.001), height (p = 0.002), heart rate (p = 0.002), systolic pressure (p < 0.001), and diastolic pressure (p = 0.002). These differences reflect physiological differences that are also present in the general population [58].
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fusar-Poli, P.; Borgwardt, S.; Bechdolf, A.; Addington, J.; Riecher-Rossler, A.; Schultze-Lutter, F.; Keshavan, M.; Wood, S.; Ruhrmann, S.; Seidman, L.J.; et al. The psychosis high-risk state: A comprehensive state-of-the-art review. JAMA Psychiatry 2013, 70, 107–120. [Google Scholar] [CrossRef] [Green Version]
- Salazar de Pablo, G.; Radua, J.; Pereira, J.; Bonoldi, I.; Arienti, V.; Besana, F.; Soardo, L.; Cabras, A.; Fortea, L.; Catalan, A.; et al. Probability of Transition to Psychosis in Individuals at Clinical High Risk: An Updated Meta-analysis. JAMA Psychiatry 2021, 78, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Schimmelmann, B.G.; Michel, C.; Schaffner, N.; Schultze-Lutter, F. What percentage of people in the general population satisfies the current clinical at-risk criteria of psychosis? Schizophr. Res. 2011, 125, 99–100. [Google Scholar] [CrossRef] [PubMed]
- Simon, A.E.; Velthorst, E.; Nieman, D.H.; Linszen, D.; Umbricht, D.; de Haan, L. Ultra high-risk state for psychosis and non-transition: A systematic review. Schizophr. Res. 2011, 132, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Addington, J.; Cornblatt, B.A.; Cadenhead, K.S.; Cannon, T.D.; McGlashan, T.H.; Perkins, D.O.; Seidman, L.J.; Tsuang, M.T.; Walker, E.F.; Woods, S.W.; et al. At clinical high risk for psychosis: Outcome for nonconverters. Am. J. Psychiatry 2011, 168, 800–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusar-Poli, P.; Bechdolf, A.; Taylor, M.J.; Bonoldi, I.; Carpenter, W.T.; Yung, A.R.; McGuire, P. At risk for schizophrenic or affective psychoses? A meta-analysis of DSM/ICD diagnostic outcomes in individuals at high clinical risk. Schizophr. Bull. 2013, 39, 923–932. [Google Scholar] [CrossRef] [Green Version]
- Yung, A.; Nelson, B.; Yuen, H.; Spiliotacopoulos, D.; Lin, A.; Simmons, M.; Bruxner, A.; Broussard, C.; Thompson, A.; McGorry, P. Long term outcome in an ultra high risk (“prodromal”) group; Schizophrenia Bulletin. In Proceedings of the 13th International Congress on Schizophrenia Research (ICSR), Colorado Springs, Colorado, 2–6 April 2011; pp. 22–23. [Google Scholar]
- Klosterkötter, J.; Hellmich, M.; Steinmeyer, E.M.; Schultze-Lutter, F. Diagnosing schizophrenia in the initial prodromal phase. Arch. Gen. Psychiatry 2001, 58, 158–164. [Google Scholar] [CrossRef] [Green Version]
- Yung, A.R.; Yuen, H.P.; McGorry, P.D.; Phillips, L.J.; Kelly, D.; Dell’Olio, M.; Francey, S.M.; Cosgrave, E.M.; Killackey, E.; Stanford, C.; et al. Mapping the onset of psychosis: The Comprehensive Assessment of At-Risk Mental States. Aust. New Zealand J. Psychiatry 2005, 39, 964–971. [Google Scholar] [CrossRef]
- Woods, S.W.; Addington, J.; Cadenhead, K.S.; Cannon, T.D.; Cornblatt, B.A.; Heinssen, R.; Perkins, D.O.; Seidman, L.J.; Tsuang, M.T.; Walker, E.F.; et al. Validity of the prodromal risk syndrome for first psychosis: Findings from the North American Prodrome Longitudinal Study. Schizophr. Bull. 2009, 35, 894–908. [Google Scholar] [CrossRef] [Green Version]
- Yung, A.R.; Nelson, B.; Stanford, C.; Simmons, M.B.; Cosgrave, E.M.; Killackey, E.; Phillips, L.J.; Bechdolf, A.; Buckby, J.; McGorry, P.D. Validation of “prodromal” criteria to detect individuals at ultra high risk of psychosis: 2 year follow-up. Schizophr. Res. 2008, 105, 10–17. [Google Scholar] [CrossRef]
- Hutton, P.; Bowe, S.; Parker, S.; Ford, S. Prevalence of suicide risk factors in people at ultra-high risk of developing psychosis: A service audit. Early Interv. Psychiatry 2011, 5, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Seidman, L.J.; Giuliano, A.J.; Meyer, E.C.; Addington, J.; Cadenhead, K.S.; Cannon, T.D.; McGlashan, T.H.; Perkins, D.O.; Tsuang, M.T.; Walker, E.F.; et al. Neuropsychology of the prodrome to psychosis in the NAPLS consortium: Relationship to family history and conversion to psychosis. Arch. Gen. Psychiatry 2010, 67, 578–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornblatt, B.A.; Carrión, R.E.; Addington, J.; Seidman, L.; Walker, E.F.; Cannon, T.D.; Cadenhead, K.S.; McGlashan, T.H.; Perkins, D.O.; Tsuang, M.T.; et al. Risk factors for psychosis: Impaired social and role functioning. Schizophr. Bull. 2012, 38, 1247–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusar-Poli, P.; Byrne, M.; Valmaggia, L.; Day, F.; Tabraham, P.; Johns, L.; McGuire, P. Social dysfunction predicts two years clinical outcome in people at ultra high risk for psychosis. J. Psychiatr. Res. 2010, 44, 294–301. [Google Scholar] [CrossRef]
- Velthorst, E.; Nieman, D.H.; Linszen, D.; Becker, H.; de Haan, L.; Dingemans, P.M.; Birchwood, M.; Patterson, P.; Salokangas, R.K.; Heinimaa, M.; et al. Disability in people clinically at high risk of psychosis. Br. J. Psychiatry 2010, 197, 278–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bechdolf, A.; Pukrop, R.; Köhn, D.; Tschinkel, S.; Veith, V.; Schultze-Lutter, F.; Ruhrmann, S.; Geyer, C.; Pohlmann, B.; Klosterkötter, J. Subjective quality of life in subjects at risk for a first episode of psychosis: A comparison with first episode schizophrenia patients and healthy controls. Schizophr. Res. 2005, 79, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Ruhrmann, S.; Paruch, J.; Bechdolf, A.; Pukrop, R.; Wagner, M.; Berning, J.; Schultze-Lutter, F.; Janssen, B.; Gaebel, W.; Möller, H.J.; et al. Reduced subjective quality of life in persons at risk for psychosis. Acta Psychiatr. Scand. 2008, 117, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Hui, T.T.; Garvey, L.; Olasoji, M. Improving the physical health of young people with early psychosis with lifestyle interventions: Scoping review. Int. J. Ment. Health Nurs. 2021, 30, 1498–1524. [Google Scholar] [CrossRef]
- Cordes, J.; Bechdolf, A.; Engelke, C.; Kahl, K.G.; Balijepalli, C.; Lösch, C.; Klosterkötter, J.; Wagner, M.; Maier, W.; Heinz, A.; et al. Prevalence of metabolic syndrome in female and male patients at risk of psychosis. Schizophr. Res. 2017, 181, 38–42. [Google Scholar] [CrossRef]
- Carney, R.; Cotter, J.; Bradshaw, T.; Firth, J.; Yung, A.R. Cardiometabolic risk factors in young people at ultra-high risk for psychosis: A systematic review and meta-analysis. Schizophr. Res. 2016, 170, 290–300. [Google Scholar] [CrossRef]
- Sormunen, E.; Saarinen, M.M.; Salokangas, R.K.R.; Telama, R.; Hutri-Kähönen, N.; Tammelin, T.; Viikari, J.; Raitakari, O.; Hietala, J. Effects of childhood and adolescence physical activity patterns on psychosis risk—A general population cohort study. npj Schizophrenia 2017, 3, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Chan, S.K.; Lee, E.H.; Chang, W.C.; Tse, M.; Su, W.W.; Sham, P.; Hui, C.L.; Joe, G.; Chan, C.L.; et al. Aerobic exercise and yoga improve neurocognitive function in women with early psychosis. Schizophrenia 2015, 1, 15047. [Google Scholar] [CrossRef] [Green Version]
- Cotter, J.; Drake, R.J.; Bucci, S.; Firth, J.; Edge, D.; Yung, A.R. What drives poor functioning in the at-risk mental state? A systematic review. Schizophr. Res. 2014, 159, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Yung, A.R.; Cotter, J.; Wood, S.J.; McGorry, P.; Thompson, A.D.; Nelson, B.; Lin, A. Childhood maltreatment and transition to psychotic disorder independently predict long-term functioning in young people at ultra-high risk for psychosis. Psychol. Med. 2015, 45, 3453–3465. [Google Scholar] [CrossRef]
- Tsiachristas, A.; Thomas, T.; Leal, J.; Lennox, B.R. Economic impact of early intervention in psychosis services: Results from a longitudinal retrospective controlled study in England. BMJ Open 2016, 6, e012611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.J.; Langan, J.; McLean, G.; Guthrie, B.; Mercer, S.W. Schizophrenia is associated with excess multiple physical-health comorbidities but low levels of recorded cardiovascular disease in primary care: Cross-sectional study. BMJ Open 2013, 3, e002808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damiani, S.; Rutigliano, G.; Fazia, T.; Merlino, S.; Berzuini, C.; Bernardinelli, L.; Politi, P.; Fusar-Poli, P. Developing and Validating an Individualized Clinical Prediction Model to Forecast Psychotic Recurrence in Acute and Transient Psychotic Disorders: Electronic Health Record Cohort Study. Schizophr. Bull. 2021, 47, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Carney, R.; Bradshaw, T.; Yung, A.R. Monitoring of physical health in services for young people at ultra-high risk of psychosis. Early Interv. Psychiatry 2018, 12, 153–159. [Google Scholar] [CrossRef]
- Thornicroft, G. Physical health disparities and mental illness: The scandal of premature mortality. Br. J. Psychiatry 2011, 199, 441–442. [Google Scholar] [CrossRef] [Green Version]
- Damme, K.S.F.; Gupta, T.; Ristanovic, I.; Kimhy, D.; Bryan, A.D.; Mittal, V.A. Exercise Intervention in Individuals at Clinical High Risk for Psychosis: Benefits to Fitness, Symptoms, Hippocampal Volumes, and Functional Connectivity. Schizophr. Bull. 2022, 48, 1394–1405. [Google Scholar] [CrossRef]
- Lederman, O.; Rosenbaum, S.; Maloney, C.; Curtis, J.; Ward, P.B. Modifiable cardiometabolic risk factors in youth with at-risk mental states: A cross-sectional pilot study. Psychiatry Res. 2017, 257, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Perera, G.; Broadbent, M.; Callard, F.; Chang, C.K.; Downs, J.; Dutta, R.; Fernandes, A.; Hayes, R.D.; Henderson, M.; Jackson, R.; et al. Cohort profile of the South London and Maudsley NHS Foundation Trust Biomedical Research Centre (SLaM BRC) Case Register: Current status and recent enhancement of an Electronic Mental Health Record-derived data resource. BMJ Open 2016, 6, e008721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jongsma, H.E.; Gayer-Anderson, C.; Lasalvia, A.; Quattrone, D.; Mulè, A.; Szöke, A.; Selten, J.P.; Turner, C.; Arango, C.; Tarricone, I.; et al. Treated Incidence of Psychotic Disorders in the Multinational EU-GEI Study. JAMA Psychiatry 2018, 75, 36–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, R.; Soremekun, M.; Perera, G.; Broadbent, M.; Callard, F.; Denis, M.; Hotopf, M.; Thornicroft, G.; Lovestone, S. The South London and Maudsley NHS Foundation Trust Biomedical Research Centre (SLAM BRC) case register: Development and descriptive data. BMC Psychiatry 2009, 9, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusar-Poli, P.; Byrne, M.; Badger, S.; Valmaggia, L.R.; McGuire, P.K. Outreach and support in south London (OASIS), 2001-2011: Ten years of early diagnosis and treatment for young individuals at high clinical risk for psychosis. Eur. Psychiatry 2013, 28, 315–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusar-Poli, P.; Spencer, T.; De Micheli, A.; Curzi, V.; Nandha, S.; McGuire, P. Outreach and support in South-London (OASIS) 2001-2020: Twenty years of early detection, prognosis and preventive care for young people at risk of psychosis. Eur. Neuropsychopharmacol. 2020, 39, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Estradé, A.; Spencer, T.J.; Gupta, S.; Murguia-Asensio, S.; Eranti, S.; Wilding, K.; Andlauer, O.; Buhagiar, J.; Smith, M.; et al. Pan-London Network for Psychosis-Prevention (PNP). Front. Psychiatry 2019, 10, 707. [Google Scholar] [CrossRef] [Green Version]
- Fusar-Poli, P.; De Micheli, A.; Signorini, L.; Baldwin, H.; Salazar de Pablo, G.; McGuire, P. Real-world long-term outcomes in individuals at clinical risk for psychosis: The case for extending duration of care. EClinicalMedicine 2020, 28, 100578. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Schultze-Lutter, F. Predicting the onset of psychosis in patients at clinical high risk: Practical guide to probabilistic prognostic reasoning. Evid. Based Ment. Health 2016, 19, 10–15. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Palombini, E.; Davies, C.; Oliver, D.; Bonoldi, I.; Ramella-Cravaro, V.; McGuire, P. Why transition risk to psychosis is not declining at the OASIS ultra high risk service: The hidden role of stable pretest risk enrichment. Schizophr. Res. 2018, 192, 385–390. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; Schultze-Lutter, F.; Cappucciati, M.; Rutigliano, G.; Bonoldi, I.; Stahl, D.; Borgwardt, S.; Riecher-Rössler, A.; Addington, J.; Perkins, D.O.; et al. The Dark Side of the Moon: Meta-analytical Impact of Recruitment Strategies on Risk Enrichment in the Clinical High Risk State for Psychosis. Schizophr. Bull. 2016, 42, 732–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NICE. Surveillance Report 2017—Psychosis and Schizophrenia in Adults: Prevention and Management (2014) NICE Guideline CG178; National Institute for Health and Care Excellence (NICE): London, UK, 2017. [Google Scholar]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerström, K.O. The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. Br. J. Addict 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F.; Eissenberg, T. Dependence levels in users of electronic cigarettes, nicotine gums and tobacco cigarettes. Drug Alcohol Depend. 2015, 147, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Etter, J.F. Dependence on the nicotine gum in former smokers. Addict. Behav. 2009, 34, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; de la Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption--II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef]
- Little, P.; Barnett, J.; Margetts, B.; Kinmonth, A.L.; Gabbay, J.; Thompson, R.; Warm, D.; Warwick, H.; Wooton, S. The validity of dietary assessment in general practice. J. Epidemiol. Community Health 1999, 53, 165–172. [Google Scholar] [CrossRef]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A study of concurrent and construct validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef]
- Statistics on Smoking—England. 2018. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-smoking/statistics-on-smoking-england-2018 (accessed on 30 December 2022).
- Fagerström, K.; Furberg, H. A comparison of the Fagerström Test for Nicotine Dependence and smoking prevalence across countries. Addiction 2008, 103, 841–845. [Google Scholar] [CrossRef]
- Adult Drinking Habits in Great Britain: 2017—Office for National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/drugusealcoholandsmoking/bulletins/opinionsandlifestylesurveyadultdrinkinghabitsingreatbritain/2017 (accessed on 30 December 2022).
- Holmes, J.; Beard, E.; Brown, J.; Brennan, A.; Meier, P.S.; Michie, S.; Stevely, A.K.; Webster, L.; Buykx, P.F. Effects on alcohol consumption of announcing and implementing revised UK low-risk drinking guidelines: Findings from an interrupted time series analysis. J. Epidemiol. Community Health 2020, 74, 942–949. [Google Scholar] [CrossRef]
- Physical Activity—Public Health Data from the Office for Health Improvement and Disparities, UK. 2015. Available online: https://fingertips.phe.org.uk/profile/physical-activity (accessed on 30 December 2022).
- Adult’s Average BMI—Health Survey for England 2019. Available online: http://healthsurvey.hscic.gov.uk/data-visualisation/data-visualisation/explore-the-trends/weight/adult/bmi.aspx#:~:text=There%20has%20been%20a%20general,(kg%2Fm2) (accessed on 30 December 2022).
- Department of Epidemiology and Public Health. Mean Waist Circumference of Adult’s in England in 2019, by Gender and Age; Department of Epidemiology and Public Health: London, UK, 2019. [Google Scholar]
- Prabhavathi, K.; Selvi, K.T.; Poornima, K.N.; Sarvanan, A. Role of biological sex in normal cardiac function and in its disease outcome—A review. J. Clin. Diagn. Res. 2014, 8, Be01-04. [Google Scholar] [CrossRef] [PubMed]
- Hartz, S.M.; Pato, C.N.; Medeiros, H.; Cavazos-Rehg, P.; Sobell, J.L.; Knowles, J.A.; Bierut, L.J.; Pato, M.T. Comorbidity of severe psychotic disorders with measures of substance use. JAMA Psychiatry 2014, 71, 248–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Leon, J.; Diaz, F.J. A meta-analysis of worldwide studies demonstrates an association between schizophrenia and tobacco smoking behaviors. Schizophr. Res. 2005, 76, 135–157. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.; McCreadie, R.G. Smoking habits, current symptoms, and premorbid characteristics of schizophrenic patients in Nithsdale, Scotland. Am. J. Psychiatry 1999, 156, 1751–1757. [Google Scholar] [CrossRef] [PubMed]
- Beratis, S.; Katrivanou, A.; Gourzis, P. Factors affecting smoking in schizophrenia. Compr. Psychiatry 2001, 42, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Weiser, M.; Reichenberg, A.; Rabinowitz, J.; Kaplan, Z.; Caspi, A.; Yasvizky, R.; Mark, M.; Knobler, H.Y.; Nahon, D.; Davidson, M. Self-reported drug abuse in male adolescents with behavioral disturbances, and follow-up for future schizophrenia. Biol. Psychiatry 2003, 54, 655–660. [Google Scholar] [CrossRef]
- Catalan, A.; Salazar de Pablo, G.; Aymerich, C.; Damiani, S.; Sordi, V.; Radua, J.; Oliver, D.; McGuire, P.; Giuliano, A.J.; Stone, W.S.; et al. Neurocognitive Functioning in Individuals at Clinical High Risk for Psychosis: A Systematic Review and Meta-analysis. JAMA Psychiatry 2021, 78, 859. [Google Scholar] [CrossRef]
- De Micheli, A.; Provenzani, U.; Solmi, M.; Van Lawick Van Pabst, A.; Youssef, E.; McGuire, P.; Fusar-Poli, P. Prevalence of tobacco smoking in CHR-P: Systematic review and meta-analysis of the evidence. Schizophr. Res. 2022; under review. [Google Scholar]
- Fusar-Poli, P.; Salazar de Pablo, G.; Correll, C.U.; Meyer-Lindenberg, A.; Millan, M.J.; Borgwardt, S.; Galderisi, S.; Bechdolf, A.; Pfennig, A.; Kessing, L.V.; et al. Prevention of Psychosis: Advances in Detection, Prognosis, and Intervention. JAMA Psychiatry 2020, 77, 755–765. [Google Scholar] [CrossRef]
- Gogos, A.; Skokou, M.; Ferentinou, E.; Gourzis, P. Nicotine consumption during the prodromal phase of schizophrenia—A review of the literature. Neuropsychiatr. Dis. Treat. 2019, 15, 2943–2958. [Google Scholar] [CrossRef] [Green Version]
- van der Heijden, H.S.; Schirmbeck, F.; McGuire, P.; Valmaggia, L.R.; Kempton, M.J.; van der Gaag, M.; Nelson, B.; Riecher-Rossler, A.; Bressan, R.; Barrantes-Vidal, N.; et al. Association between tobacco use and symptomatology in individuals at ultra-high risk to develop a psychosis: A longitudinal study. Schizophr. Res. 2021, 236, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hou, C.L.; Ma, X.R.; Zang, Y.; Jia, F.J.; Lai, K.Y.C.; Ungvari, G.S.; Ng, C.H.; Cai, M.Y.; Xiang, Y.T. Nicotine dependence in community-dwelling Chinese patients with schizophrenia. Gen. Psychiatr. 2019, 32, e100014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engels, R.C.; Knibbe, R.A.; Drop, M.J. Inconsistencies in adolescents’ self-reports of initiation of alcohol and tobacco use. Addict. Behav. 1997, 22, 613–623. [Google Scholar] [CrossRef]
- Carney, R.; Yung, A.R.; Amminger, G.P.; Bradshaw, T.; Glozier, N.; Hermens, D.F.; Hickie, I.B.; Killackey, E.; McGorry, P.; Pantelis, C.; et al. Substance use in youth at risk for psychosis. Schizophr. Res. 2017, 181, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Auther, A.M.; Cadenhead, K.S.; Carrion, R.E.; Addington, J.; Bearden, C.E.; Cannon, T.D.; McGlashan, T.H.; Perkins, D.O.; Seidman, L.; Tsuang, M.; et al. Alcohol confounds relationship between cannabis misuse and psychosis conversion in a high-risk sample. Acta Psychiatr. Scand. 2015, 132, 60–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bozymski, K.M.; Whitten, J.A.; Blair, M.E.; Overley, A.M.; Ott, C.A. Monitoring and Treating Metabolic Abnormalities in Patients with Early Psychosis Initiated on Antipsychotic Medications. Community Ment. Health J 2018, 54, 717–724. [Google Scholar] [CrossRef]
- NHS UK: Physical Activity Guidelines for Adults Aged 19 to 64 (Page Last Reviewed: 4 August 2021). Available online: https://www.nhs.uk/live-well/exercise/exercise-guidelines/physical-activity-guidelines-for-adults-aged-19-to-64/ (accessed on 30 December 2022).




{kind=link}
{kind=link}
{kind=link}
| N | Mean | Sd | ||
|---|---|---|---|---|
| Age (years) | 194 | 23.70 | 5.12 | |
| N | Count | % | ||
| Gender | 194 | |||
| Females | 90 | 46 | ||
| Males | 104 | 54 | ||
| Ethnicity | 174 | |||
| White | 72 | 41 | ||
| Asian | 4 | 2 | ||
| Black African | 16 | 9 | ||
| Black Caribbean | 5 | 3 | ||
| Black British | 37 | 21 | ||
| Other | 40 | 23 |
| Total | Males | Females | Difference M/F | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Count | % | N | Count | % | N | Count | % | Fisher’s Exact Test | |
| Tobacco smokers | 194 | 80 | 41 | 104 | 49 | 47 | 90 | 31 | 34 | p = 0.08 |
| Alcohol drinkers | 194 | 139 | 75 | 104 | 71 | 68 | 90 | 68 | 76 | p = 0.58 |
| N | Mean | SD | N | Mean | SD | N | Mean | SD | Student’s t test | |
| Daily cigarettes | 77 | 8.47 | 7.86 | 48 | 9.69 | 8.97 | 29 | 6.98 | 5.65 | t = 1.46; p = 0.15 |
| FTND score | 77 | 2.51 | 2.54 | 48 | 2.68 | 2.55 | 29 | 2.27 | 2.51 | t = 0.70; p = 0.49 |
| Audit-C score | 139 | 4.94 | 2.93 | 71 | 5.39 | 3.08 | 68 | 4.47 | 2.70 | t = 1.87; p = 0.63 |
| Audit total score | 139 | 7.88 | 6.63 | 71 | 8.90 | 6.99 | 68 | 6.81 | 6.10 | t = 1.87; p = 0.63 |
| DINE fibre score | 187 | 28.05 | 14.02 | 99 | 29.60 | 15.28 | 88 | 26.07 | 12.32 | t = 1.72; p = 0.09 |
| DINE saturated fat score | 187 | 27.22 | 11.57 | 99 | 28.57 | 11.25 | 88 | 25.83 | 11.83 | t = 1.62; p = 0.10 |
| DINE unsaturated fat score | 187 | 8.68 | 2.39 | 99 | 8.61 | 2.27 | 88 | 8.75 | 2.54 | t = −0.40; p = 0.69 |
| IPAQ vigorous activity (dpw) | 160 | 1.21 | 1.78 | 98 | 1.80 | 2.03 | 86 | 0.66 | 1.37 | t = 4.38; p < 0.001 * |
| IPAQ vigorous activity (mpd) | 160 | 43.06 | 72.44 | 98 | 70.20 | 96.35 | 86 | 18.66 | 39.34 | t = 4.63; p < 0.001 * |
| IPAQ moderate activity (dpw) | 160 | 1.73 | 2.01 | 99 | 2.11 | 2.12 | 85 | 1.55 | 1.99 | t = 1.85; p = 0.66 |
| IPAQ moderate activity (mpd) | 160 | 43.06 | 72.45 | 97 | 82.37 | 144.77 | 84 | 45.42 | 83.65 | t = 2.06; p = 0.41 |
| IPAQ walking (dpw) | 160 | 5.25 | 2.16 | 97 | 5.13 | 2.24 | 85 | 5.42 | 2.01 | t = −0.91; p = 0.36 |
| IPAQ walking (mpd) | 160 | 94.47 | 115.35 | 94 | 94.41 | 127.13 | 83 | 107.23 | 123.11 | t = −0.68; p = 0.50 |
| IPAQ sitting (mpw) | 160 | 463.80 | 278.40 | 91 | 446.40 | 282.60 | 75 | 484.20 | 260.40 | t = −0.88; p = 0.38 |
| Total | Males | Females | Difference M/F | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | N | Mean | SD | N | Mean | SD | Student’s t Test | |
| Weight (Kg) | 184 | 71.53 | 16.04 | 102 | 74.54 | 16.56 | 82 | 67.74 | 14.72 | t = 2.91; p < 0.001 * |
| Height (m) | 184 | 1.72 | 0.10 | 103 | 1.78 | 0.08 | 81 | 1.64 | 0.06 | t = 12.75; p < 0.001 * |
| Body Mass Index | 182 | 24.45 | 4.50 | 102 | 23.86 | 3.82 | 80 | 25.20 | 5.19 | t = −2.02; p = 0.45 |
| Waist circumference (cm) | 144 | 82.29 | 13.04 | 83 | 83.00 | 11.73 | 61 | 81.33 | 14.68 | t = 0.76; p = 0.45 |
| Heart rate (beats per minute) | 185 | 69.42 | 11.57 | 103 | 67.33 | 12.19 | 81 | 72.31 | 10.00 | t = 2.97; p = 0.002 * |
| Respiratory rate (acts per minute) | 165 | 17.93 | 5.32 | 93 | 17.22 | 4.95 | 71 | 18.96 | 5.65 | t = 2.10; p = 0.37 |
| Systolic pressure (mmHg) | 178 | 115.81 | 12.00 | 98 | 120.20 | 10.76 | 79 | 110.34 | 11.33 | t = 5.92; p < 0.001 * |
| Diastolic pressure (mmHg) | 178 | 72.24 | 9.32 | 98 | 74.08 | 9.52 | 79 | 70.09 | 8.61 | t = 2.89; p = 0.002 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Provenzani, U.; De Micheli, A.; Damiani, S.; Oliver, D.; Brondino, N.; Fusar-Poli, P. Physical Health in Clinical High Risk for Psychosis Individuals: A Cross-Sectional Study. Brain Sci. 2023, 13, 128. https://doi.org/10.3390/brainsci13010128
Provenzani U, De Micheli A, Damiani S, Oliver D, Brondino N, Fusar-Poli P. Physical Health in Clinical High Risk for Psychosis Individuals: A Cross-Sectional Study. Brain Sciences. 2023; 13(1):128. https://doi.org/10.3390/brainsci13010128
Chicago/Turabian StyleProvenzani, Umberto, Andrea De Micheli, Stefano Damiani, Dominic Oliver, Natascia Brondino, and Paolo Fusar-Poli. 2023. "Physical Health in Clinical High Risk for Psychosis Individuals: A Cross-Sectional Study" Brain Sciences 13, no. 1: 128. https://doi.org/10.3390/brainsci13010128