
First Trimester Ultrasound Detection of Fetal Central Nervous System Anomalies
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
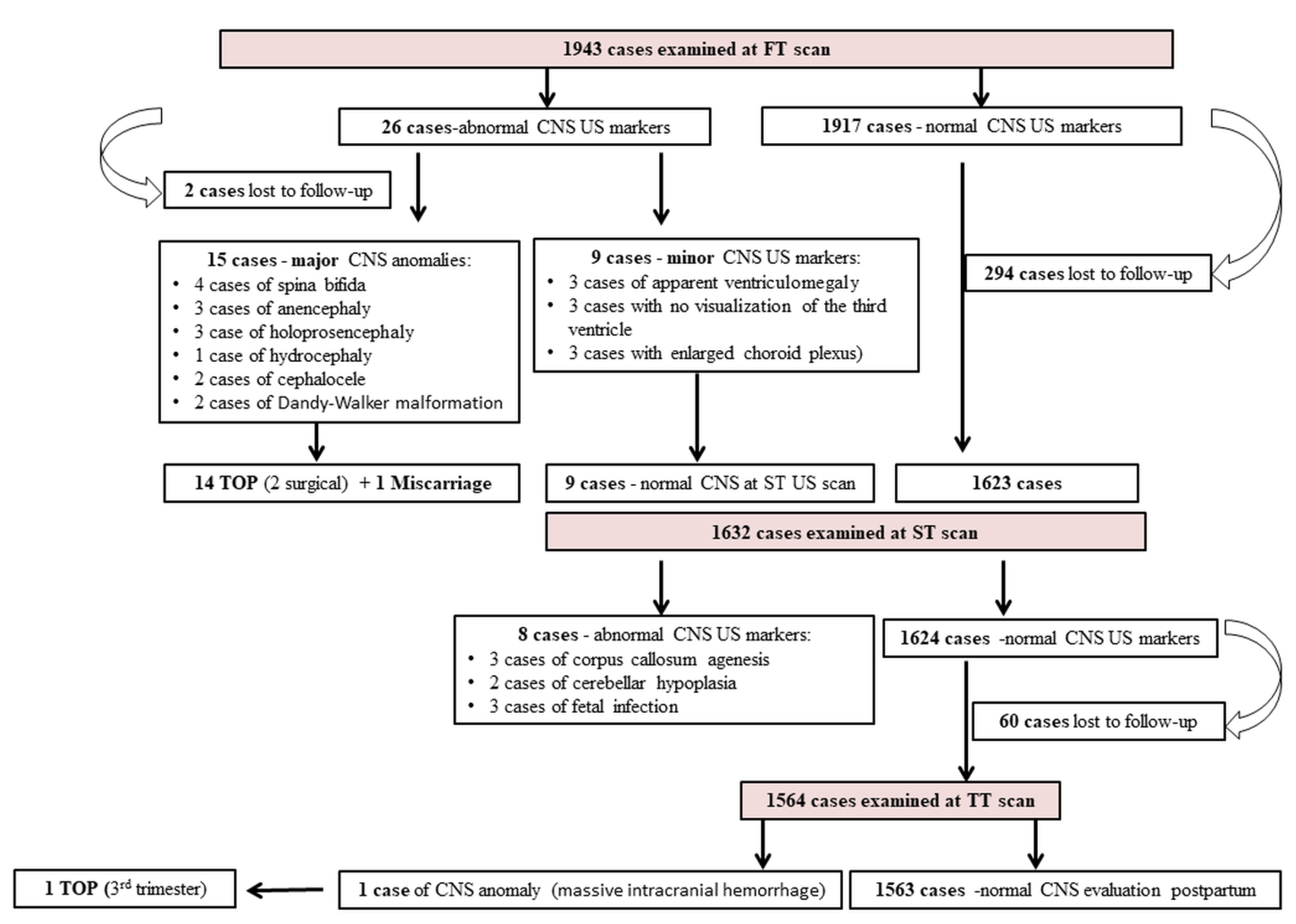
3. Results
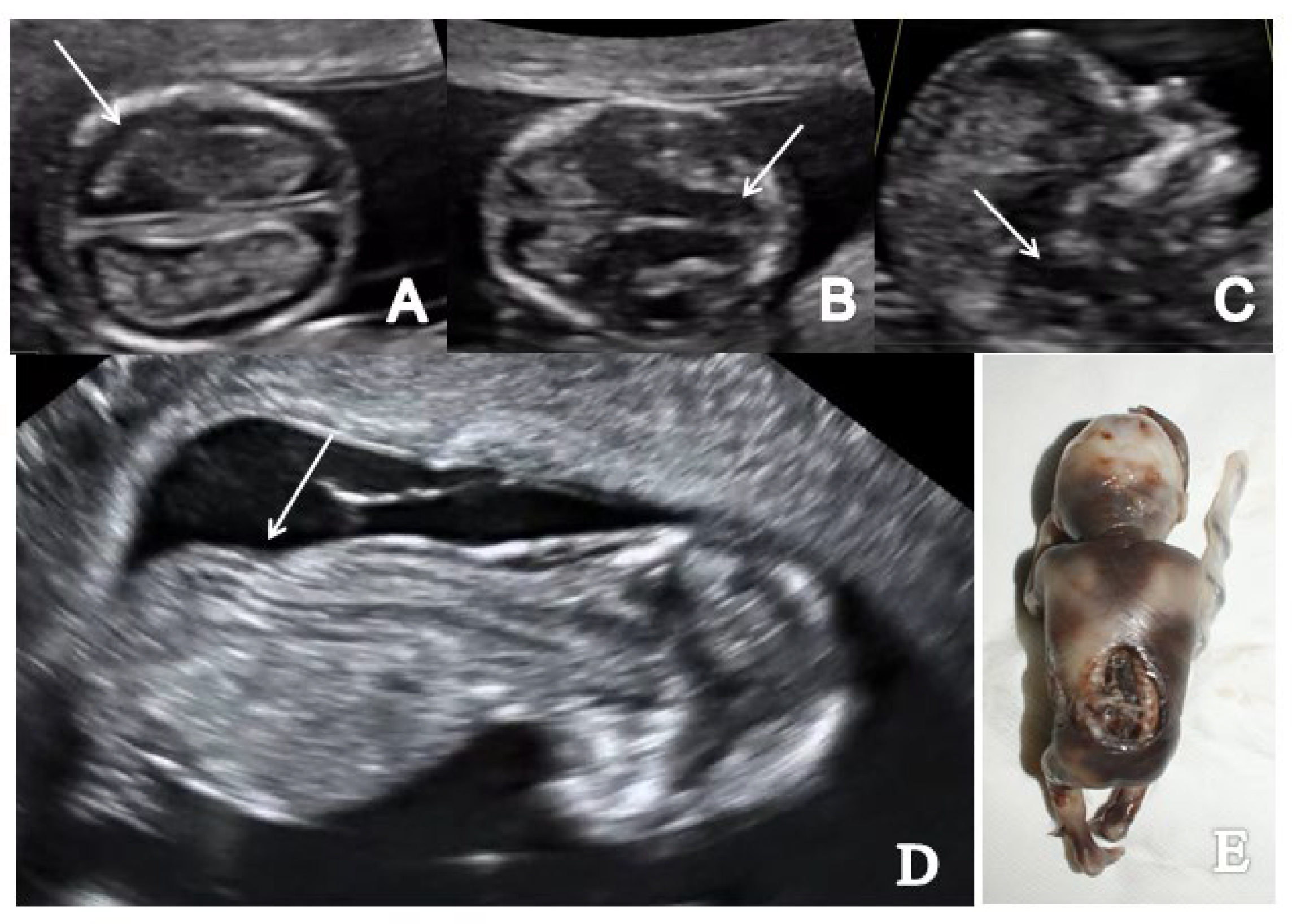
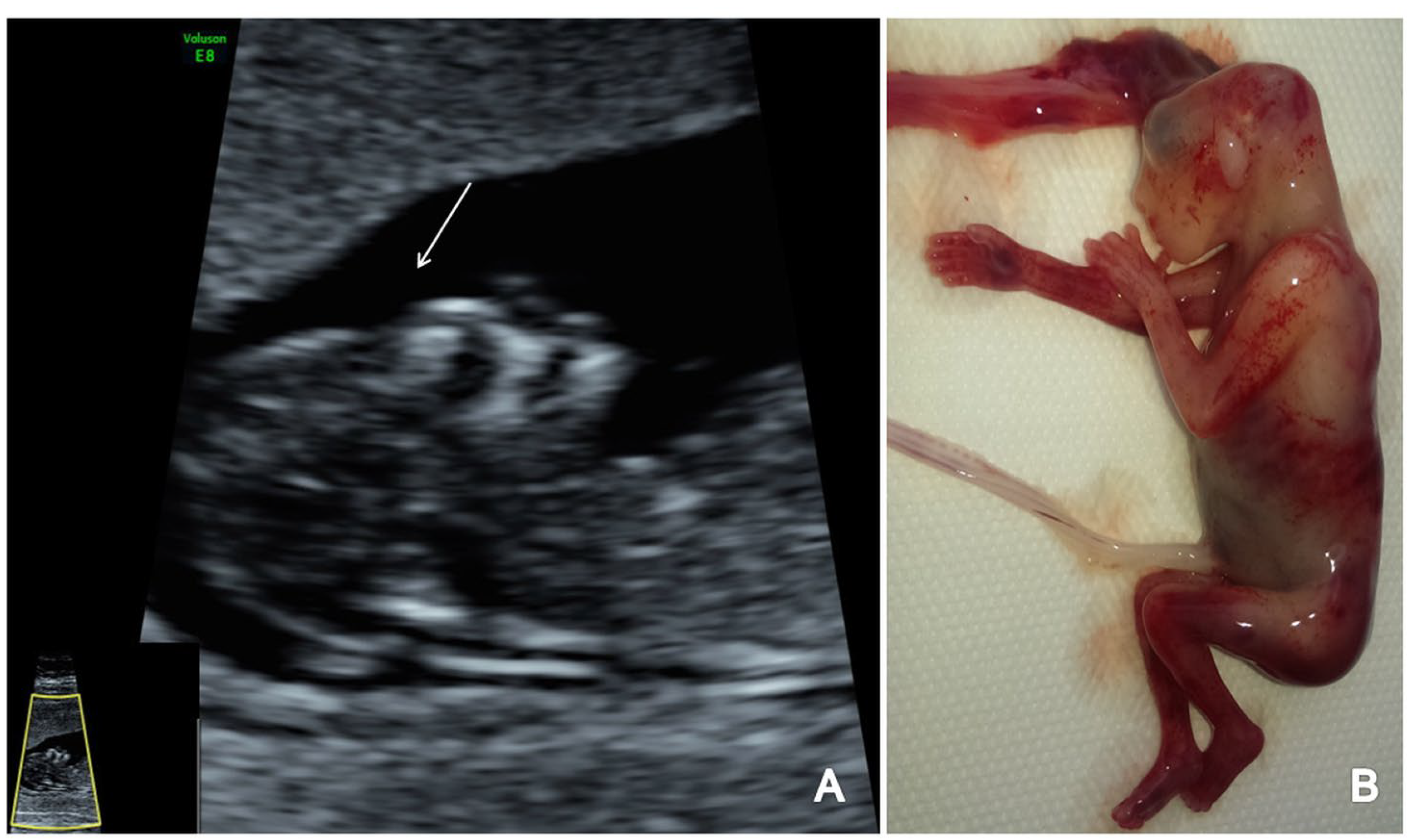
3.1. Spina Bifida
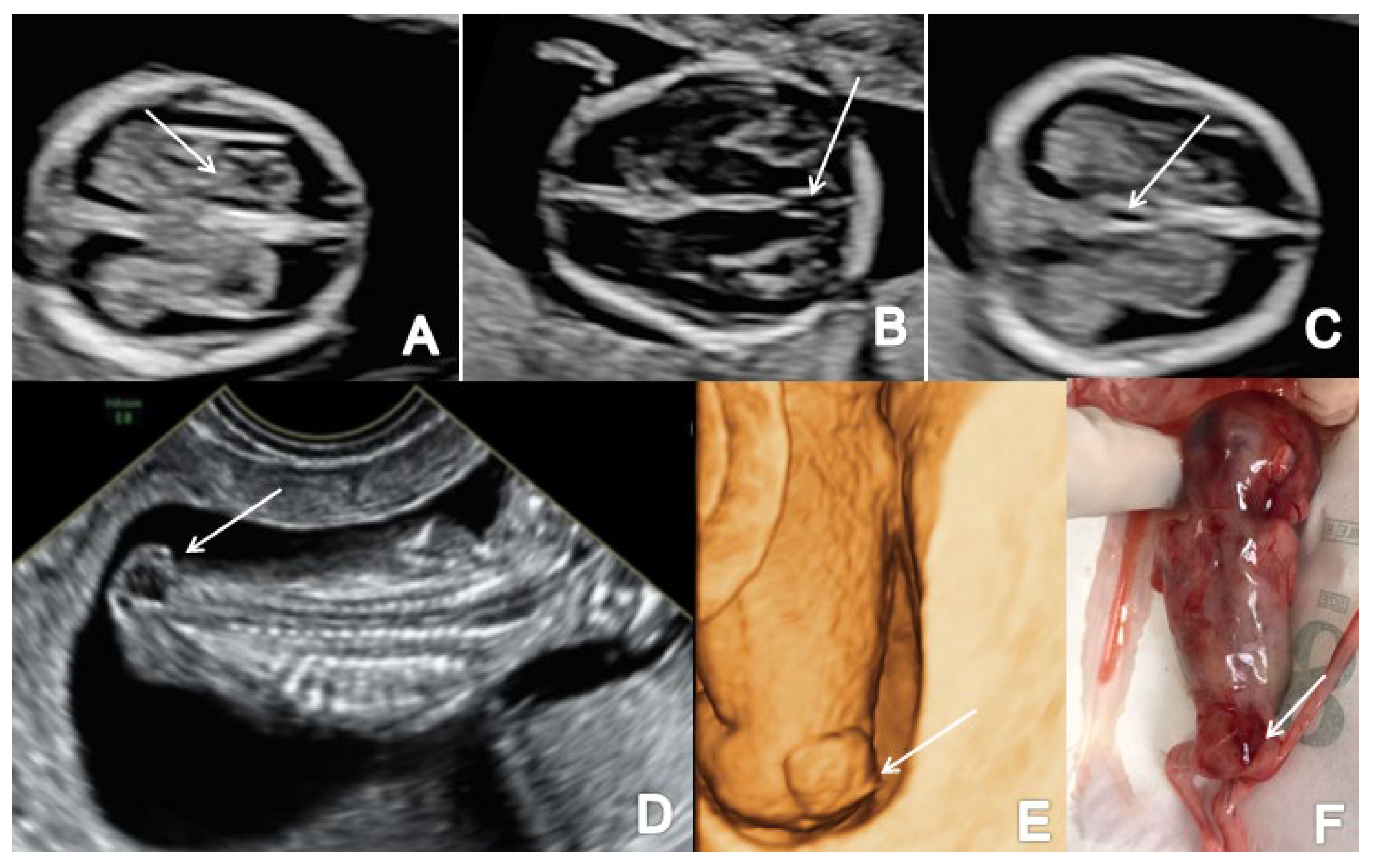
3.2. Cephalocele
3.3. Dandy-Walker Malformation
3.4. Acrania, Exencephaly, Anencephaly
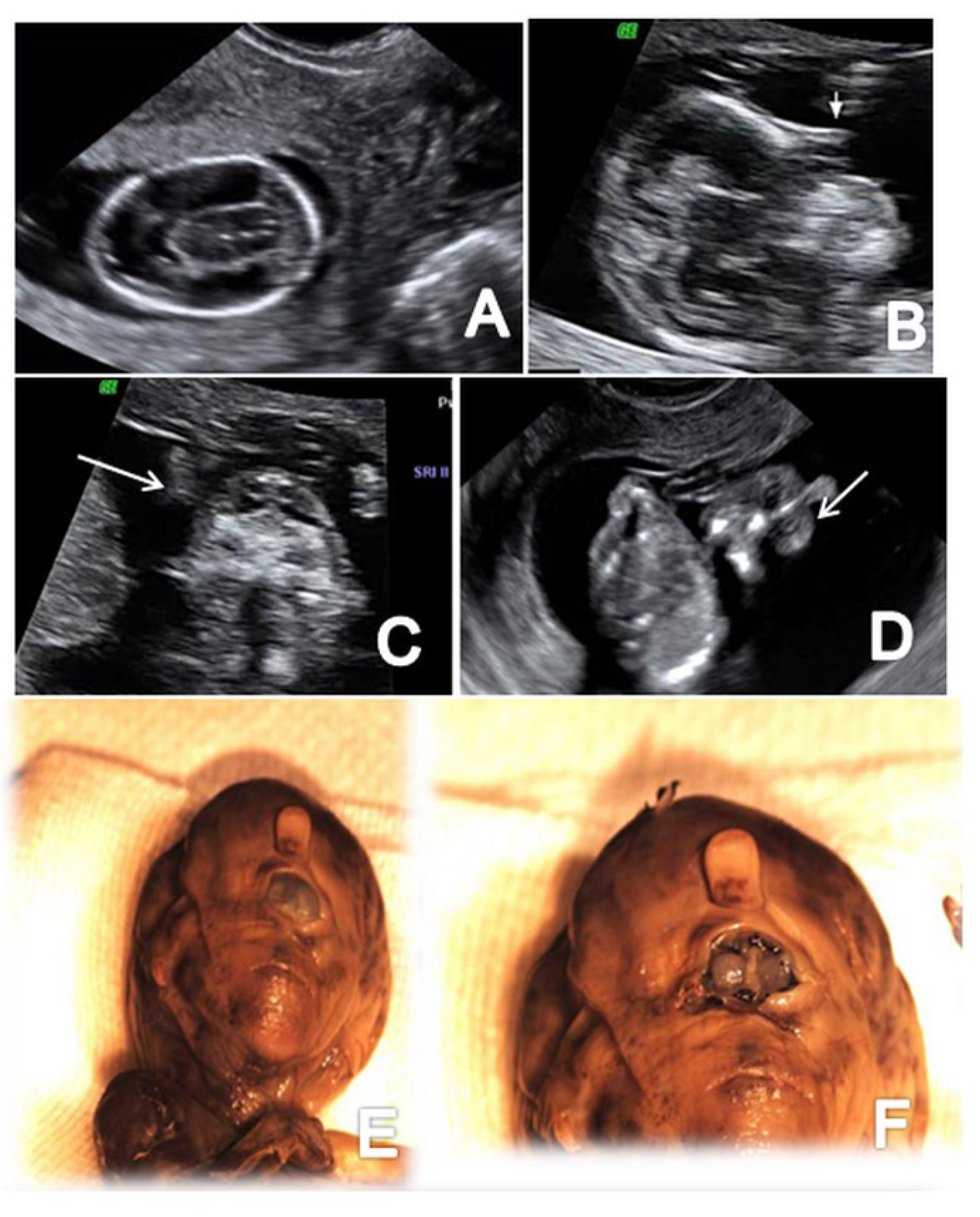
3.5. Holoprosencephaly
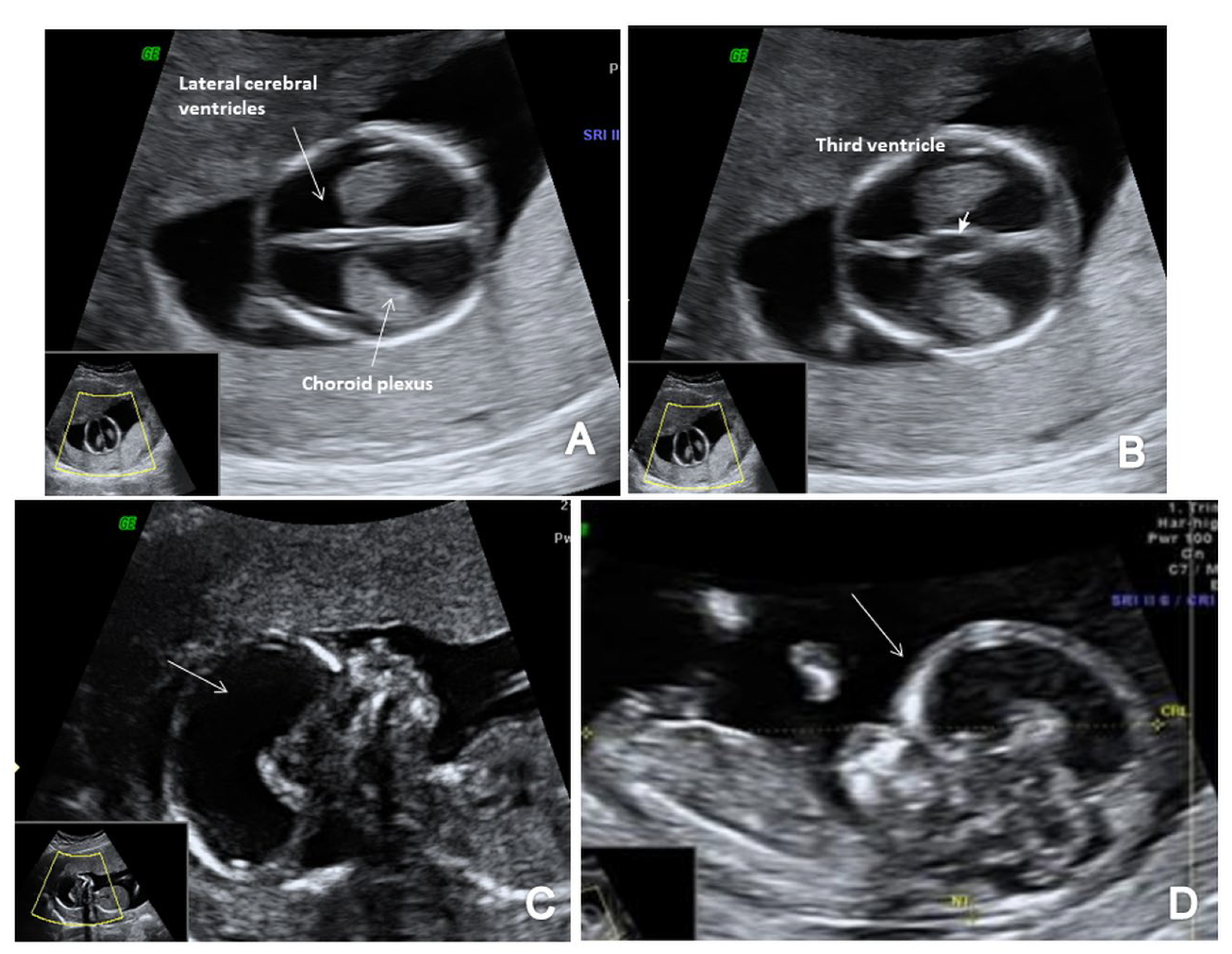
3.6. Ventriculomegaly/Hydrocephaly
4. Discussion
4.1. Spina Bifida
4.2. Open Spina Bifida
4.3. Closed Spina Bifida
4.4. Cephalocele
4.5. Dandy-Walker Malformation
4.6. Acrania, Exencephaly, Anencephaly
4.7. Holoprosencephaly
4.8. Ventriculomegaly/Hydrocephaly
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iliescu, D.G.; Comanescu, C. CNS Abnormalities at 11–14 Weeks. Neonatal Pediatr. Med. 2017, 3, 141. [Google Scholar] [CrossRef] [Green Version]
- Nicolades, K.H. Turning the pyramid of prenatal care. Fetal Diagn. Ther. 2011, 29, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Gheorman, L.; Iliescu, D.; Ceauşu, I.; Paulescu, D.; Pleşea, I.E.; Gheorman, V. Importance of early complex evaluation in high-risk pregnancy associated to diabetes mellitus. Case presentation and review of the literature. Rom. J. Morphol. Embryol. 2011, 52, 1127–1132. [Google Scholar] [PubMed]
- Engels, A.C.; Joyeux, L.; Brantner, C.; De Keersmaecker, B.; De Catte, L.; Baud, D.; Deprest, J.; Van Mieghem, T. Sonographic detection of central nervous system defects in the first trimester of pregnancy. Prenat. Diagn. 2016, 36, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Cara, M.L.; Streatam, I.; Buga, A.M.; Iliescu, D.G. Developmental brain asymmetry. The good and the bad sides. Symmetry 2022, 14, 128. [Google Scholar] [CrossRef]
- Blaas, H.-G.; Eik-Nes, S.H. Sonoembryology and early prenatal diagnosis of neural anomalies. Prenat. Diagn. 2009, 29, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Pilu, G.; Hobbins, J.C. Sonography of fetal cerebrospinal anomalies. Prenat. Diagn. 2002, 22, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Salomon, L.J.; Alfirevic, Z.; Bilardo, C.M.; Chalouhi, G.E.; Ghi, T.; Kagan, K.O.; Lau, T.K.; Papageorghiou, A.T.; Raine-Fenning, N.J.; Stirnemann, J.; et al. ISUOG Practice Guidelines: Performance of first-trimester fetal ultrasound scan. Ultrasound Obstet. Gynecol. 2013, 41, 102–113. [Google Scholar]
- Malinger, G.; Paladini, D.; Haratz, K.K.; Monteagudo, A.; Pilu, G.; Timor-Tritsch, I.E. ISUOG Practice Guidelines (updated): Sonographic examination of the fetal central nervous system. Part 1: Performance of screening examination and indications for targeted neurosonography. Ultrasound Obstet. Gynecol. 2020, 56, 476–484. [Google Scholar] [CrossRef]
- Souka, A.P.; Nicolaides, K.H. Diagnosis of fetal abnormalities at the 10–14-week scan. Ultrasound Obstet Gynecol. 1997, 10, 429–442. [Google Scholar] [CrossRef]
- Paladini, D.; Malinger, G.; Birnbaum, R.; Monteagudo, A.; Pilu, G.; Salomon, L.J.; Timor-Tritsch, I.E. ISUOG Practice Guidelines (updated): Sonographic examination of the fetal central nervous system. Part 2: Performance of targeted neurosonography. Ultrasound Obstet. Gynecol. 2021, 57, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Davies, V.; Gledhill, J.; McFadyen, A.; Whitlow, B.; Economides, D. Psychological outcome in women undergoing termination of pregnancy for ultrasound-detected fetal anomaly in the first and second trimesters: A pilot study. Ultrasound Obstet. Gynecol. 2005, 25, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Chaoui, R.; Nicolaides, K.H. Detecting open spina bifida at the 11–13-week scan by assessing intracranial translucency and the posterior brain region: Mid-sagittal or axial plane? Ultrasound Obstet. Gynecol. 2011, 38, 609–612. [Google Scholar] [CrossRef] [PubMed]
- Ushakov, F.; Sacco, A.; Andreeva, E.; Tudorache, S.; Everett, T.; David, A.L.; Pandya, P.P. Crash sign: New first-trimester sonographic marker of spina bifida. Ultrasound Obstet. Gynecol. 2019, 54, 740–745. [Google Scholar] [CrossRef]
- Lachmann, R.; Chaoui, R.; Moratalla, J. Posterior brain in fetuses with open spina bifida at 11 to 13 weeks. Prenat. Diagn. 2011, 31, 103–106. [Google Scholar] [CrossRef]
- Lachmann, R.; Picciarelli, G.; Moratalla, J.; Greene, N.; Nicolaides, K.H. Frontomaxillary facial angle in fetuses with spina bifida at 11–13 weeks’ gestation. Ultrasound Obstet. Gynecol. 2010, 36, 268–271. [Google Scholar] [CrossRef]
- Salomon, L.J.; Alfirevic, Z.; Berghella, V. Practice guidelines for performance of the routine mid-trimester fetal ultrasound scan. Ultrasound Obstet. Gynecol. 2011, 37, 116–126. [Google Scholar] [CrossRef]
- Ungureanu, D.R.; Zorila, L.G.; Capitanescu, R.G. First trimester cerebral appearance in the presence of closed spina bifida with myelomeningocele, part of the OEIS complex. BMJ Case Rep. CP 2020, 13, e235395. [Google Scholar] [CrossRef]
- Yankova, M. Detection of fetal defects in first trimester by ultrasound examination-abilities and limitations. Int. J. Gynecol. Obstet. Neonatal Care 2016, 3, 41–46. [Google Scholar] [CrossRef]
- Iliescu, D.; Tudorache, S.; Comanescu, A.; Antsaklis, P.; Cotarcea, S.; Novac, L.; Cernea, N.; Antsaklis, A. Improved detection rate of structural abnormalities in the first trimester using an extended examination protocol. Ultrasound Obstet. Gynecol. 2013, 42, 300–309. [Google Scholar] [CrossRef]
- Grande, M.; Arigita, M.; Borobio, V.; Jimenez, J.M.; Fernandez, S.; Borrell, A. First-trimester detection of structural abnormalities and the role of aneuploidy markers. Ultrasound Obstet. Gynecol. 2012, 39, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, D.G.; Tudorache, S.; Comanescu, A.; Novac, L.; Antsaklis, P.; Cernea, N. Reability of first trimester structural sonografic extended evaluation. Ultrasound Obstet. Gynecol. 2012, 40, 188–189. [Google Scholar] [CrossRef]
- Blundell, J.E.; Baker, J.L.; Boyland, E.; Blaak, E.; Charzewska, J.; de Henauw, S.; Frühbeck, G.; Gonzalez-Gross, M.; Hebebrand, J.; Holm, L.; et al. Variations in the prevalence of obesity among european countries, and a consideration of possible causes. Obes. Facts 2017, 10, 25–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iliescu, D.; Tudorache, Ş.; Comanescu, A.; Căpitănescu, R.; Manolea, M.; Novac, M.; Cernea, N.; Novac, L. Feasbility of neurosonogram adjusted with recently described markers at the 11–13+6 week scan. In Advance in Perinatal Medicine; Conference Proceedings Citation Index; Web of Science® Database: Bucharest, Romania, 2010; pp. 143–148. ISBN 978-88-6521-027-7. [Google Scholar]
- Syngelaki, A.; Chelemen, T.; Dagklis, T.; Allan, L.; Nicolaides, K.H. Challenges in the diagnosis of fetal non-chromosomal abnormalities at 11–13 weeks. Prenat. Diagn. 2011, 31, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Nagy, R.D.; Ruican, D.; Zorilă, G.-L.; Istrate-Ofiţeru, A.-M.; Badiu, A.M.; Iliescu, D.G. Feasibility of fetal portal venous system ultrasound assessment at the FT anomaly scan. Diagnostics 2022, 12, 361. [Google Scholar] [CrossRef]
- Martinez-Ten, P.; Illescas, T.; Adiego, B.; Estevez, M.; Bermejo, C.; Wong, A.E.; Sepulveda, W. Non-visualization of choroid plexus of fourth ventricle as first-trimester predictor of posterior fossa anomalies and chromosomal defects. Ultrasound Obstet. Gynecol. 2018, 51, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Beke, A.; Papp, C.; Tóth-Pál, E. Trisomies and other chromosome abnormalities detected after positive sonographic findings. J. Reprod. Med. 2005, 50, 675–691. [Google Scholar]
- Mei, J.Y.; Afshar, Y.; Platt, L.D. First-Trimester ultrasound. Obstet. Gynecol. Clin. N. Am. 2019, 46, 829–852. [Google Scholar] [CrossRef]
- Şorop-Florea, M.; Ciurea, R.N.; Ioana, M.; Stepan, A.E.; Stoica, G.A.; Tănase, F.; Comănescu, M.C.; Novac, M.B.; Drăgan, I.; Pătru, C.L.; et al. The importance of perinatal autopsy. Review of the literature and series of cases. Rom. J. Morphol. Embryol. 2017, 58, 323–337. [Google Scholar]
- Ruican, D.; Petrescu, A.M.; Ungureanu, A.L.; Marinaş, M.C.; Pirici, D.; Istrate-Ofiţeru, A.M.; Roşu, G.C.; Badiu, A.M.; Simionescu, C.E.; Şerbănescu, M.-S.; et al. Virtual autopsy and confirmation of normal fetal heart anatomy in the first trimester using three-dimensional (3D) reconstruction of histological sections. Rom. J. Morphol. Embryol. 2021, 62, 101–108. [Google Scholar] [CrossRef]
- Boyd, P.A.; Wellesley, D.G.; De Walle, H.E.; Tenconi, R.; GarciaMinaur, S.; Zandwijken, G.R.; Stoll, C.; Clementi, M. Evaluation of the prenatal diagnosis of neural tube defects by fetal ultrasonographic examination in different centres across Europe. J. Med. Screen. 2000, 7, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Ghi, T.; Pilu, G.; Falco, P. Prenatal diagnosis of open and closed spina bifida. Ultrasound Obstet. Gynecol. 2006, 28, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Tortori-Donati, P.; Rossi, A.; Cama, A. Spinal dysraphism: A review of neuroradiological features with embryological correlations and proposal for a new classification. Neuroradiology 2000, 42, 471–491. [Google Scholar] [CrossRef]
- Copp, A.J.; Adzick, N.S.; Chitty, L.S.; Fletcher, J.M.; Holmbeck, G.N.; Shaw, G.M. Spina bifida. Nat. Rev. Dis. Prim. 2015, 1, 15007. [Google Scholar] [CrossRef] [Green Version]
- Watson, W.J.; Chescheir, N.C.; Katz, V.L.; Seeds, J.W. The role of ultrasound in evaluation of patients with elevated maternal serum alpha-fetoprotein: A review. Obstet. Gynecol. 1991, 78, 123–128. [Google Scholar] [PubMed]
- Flake, A. Percutaneous minimal-access fetoscopic surgery for myelomeningocele—Not so minimal! Ultrasound Obstet. Gynecol. 2014, 44, 499–500. [Google Scholar] [CrossRef] [PubMed]
- Erickson, J.D. The International Clearinghouse for Birth Defects Monitoring Systems: Past, present and future. Int. J. Risk Saf. Med. 1991, 2, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, Z.; Siegler, E.; Bronshtein, M. The early diagnosis of neural tube defects. Prenat. Diagn. 1993, 13, 863–871. [Google Scholar] [CrossRef]
- Blaas, H.-G.; Eik-Nes, S.H.; Isaksen, C.V. The detection of spina bifida before 10 gestational weeks using two- and three-dimensional ultrasound. Ultrasound Obstet. Gynecol. 2000, 16, 25–29. [Google Scholar] [CrossRef]
- Sebire, N.J.; Noble, P.L.; Thorpe-Beeston, J.G.; Snijders, R.J.; Nicolaides, K.H. Presence of the ‘lemon’sign in fetuses with spina bifida at the 10–14-week scan. Ultrasound Obstet. Gynecol. 1997, 10, 403–405. [Google Scholar] [CrossRef]
- Sepulveda, W.; Wong, A.E.; Fauchon, D.E. Fetal spinal anomalies in a first trimester sonographic screening program for aneuploidy. Prenat. Diagn. 2011, 31, 107–114. [Google Scholar] [CrossRef]
- Mangione, R.; Dhombres, F.; Lelong, N.; Amat, S.; Atoub, F.; Friszer, S.; Khoshnood, B.; Jouannic, J.-M. Screening for fetal spina bifida at the 11–13-week scan using three anatomical features of the posterior brain. Ultrasound Obstet. Gynecol. 2013, 42, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, T.; Ushakov, F.; Montenegro, N.; Gielchinsky, Y.; Nicolaides, K.H. Cerebral ventricular system in fetuses with open spina bifida at 11–13 weeks’ gestation. Ultrasound Obstet Gynecol. 2012, 39, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Zhao, S.; Yang, X.; Feng, Q.; Zhang, X.; Yang, F.; Chen, X. First-trimester cranial ultrasound markers of open spina bifida. J. Ultrasound Med. 2021, 40, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Coates, A.; Papageorghiou, A.; Bhide, A.; Thilaganathan, B. Biparietal diameter at 11–13 weeks’ gestation in fetuses with open spina bifida. Ultrasound Obstet. Gynecol. 2013, 42, 409–415. [Google Scholar] [CrossRef]
- Simon, E.G.; Arthuis, C.J.; Haddad, G.; Bertrand, P.; Perrotin, F. Biparietal/transverse abdominal diameter ratio ≤ 1: Potential marker for open spina bifida at 11–13-week scan. Ultrasound Obstet. Gynecol. 2005, 45, 267–272. [Google Scholar] [CrossRef]
- Manegold-Brauer, G.; Oseledchyk, A.; Floeck, A.; Berg, C.; Gembruch, U.; Geipel, A. Approach to the sonographic evaluation of fetal ventriculomegaly at 11 to 14 weeks gestation. BMC Pregnancy Childbirth 2016, 16, 3. [Google Scholar] [CrossRef] [Green Version]
- Orlandi, E.; Rossi, C.; Perino, A.; Cucinella, G.; Orlandi, F. Prospective sonographic detection of spina bifida at 11–14 weeks and systematic literature review. J. Matern. Fetal Neonatal Med. 2016, 29, 2363–2367. [Google Scholar] [CrossRef]
- Graham, P. Spina Bifida Occulta. Orthop. Nurs. 2021, 40, 259–261. [Google Scholar] [CrossRef]
- Chaoui, R.; Benoit, B.; Mitkowska-Wozniak, H.; Heling, K.S.; Nicolaides, K.H. Assessment of intracranial translucency (IT) in the detection of spina bifida at the 11–13-week scan. Ultrasound Obstet. Gynecol. 2009, 34, 249–252. [Google Scholar] [CrossRef]
- Liao, Y.; Wen, H.; Luo, G.; Ouyang, S.; Bi, J.; Yuan, Y.; Luo, D.; Huang, Y.; Zhang, K.; Tian, X.; et al. Fetal open and closed spina bifida on a routine scan at 11 weeks to 13 weeks 6 days. J. Ultrasound Med. 2021, 40, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Maruotti, G.M.; Saccone, G.; D’Antonio, F. Diagnostic accuracy of intracranial translucency in detecting spina bifida: A systematic review and meta-analysis. Prenat. Diagn. 2016, 36, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Fong, K.W.; Toi, A.; Okun, N. Retrospective review of diagnostic performance of intracranial translucency in detection of open spina bifida at the 11–13-week scan. Ultrasound Obstet. Gynecol. 2011, 38, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, D.; Comănescu, A.; Antsaklis, P.; Tudorache, S.; Ghiluşi, M.; Comănescu, V.; Paulescu, D.; Ceauşu, I.; Antsaklis, A.; Novac, L.; et al. Neuroimaging parameters in early open spina bifida detection. Further benefit in first trimester screening? Rom. J. Morphol. Embryol. 2011, 52, 809–817. [Google Scholar]
- Kappou, D.; Papastefanou, I.; Pilalis, A.; Kavalakis, I.; Kassanos, D.; Souka, A.P. Towards detecting open spina bifida in the first trimester: The examination of the posterior brain. Fetal Diagn. Ther. 2015, 37, 294–300. [Google Scholar] [CrossRef]
- Herman, A.; Maymon, R.; Dreazen, E.; Caspi, E.; Bukovsky, I.; Weinraub, Z. Nuchal translucency audit: A novel image-scoring method. Ultrasound Obstet. Gynecol. 1998, 12, 398–403. [Google Scholar] [CrossRef]
- Kose, S.; Altunyurt, S.; Keskinoglu, P. A prospective study on fetal posterior cranial fossa assessment for early detection of open spina bifida at 11–13 weeks. Congenit. Anom. 2018, 58, 4–9. [Google Scholar] [CrossRef]
- Garcia-Posada, R.; Eixarch, E.; Sanz, M.; Puerto, B.; Figueras, F.; Borrell, A. Cisterna magna width at 11–13 weeks in the detection of posterior fossa anomalies. Ultrasound Obstet. Gynecol. 2013, 41, 515–520. [Google Scholar] [CrossRef]
- Chen, F.C.; Gerhardt, J.; Entezami, M. Detection of spina bifida by first trimester screening—Results of the prospective multicenter Berlin ITstudy. Ultraschall Med. 2017, 38, 151–157. [Google Scholar] [CrossRef]
- Kulkarni, A.V.; Pierre-Kahn, A.; Zerah, M. Conservative management of asymptomatic spinal lipomas of the conus. Neurosurgery 2004, 54, 868–873, discussion 873–875. [Google Scholar] [CrossRef]
- Main, D.M.; Mennuti, M.T. Neural tube defects: Issues in prenatal diagnosis and counselling. Obstet. Gynecol. 1986, 67, 1–16. [Google Scholar] [PubMed]
- Sepulveda, W.; Wong, A.E.; Andreeva, E. Sonographic spectrum of first-trimester fetal cephalocele: Review of 35 cases. Ultrasound Obstet. Gynecol. 2015, 46, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Cedergren, M.; Selbing, A. Detection of fetal structural abnormalities by an 11-14-week ultrasound dating scan in an unselected Swedish population. Acta Obstet. Gynecol. Scand. 2006, 85, 912–915. [Google Scholar] [CrossRef] [PubMed]
- Egle, D.; Strobl, I.; Weiskopf-Schwendinger, V. Appearance of the fetal posterior fossa at 11 + 3 to 13 + 6 gestational weeks on transabdominal ultrasound examination. Ultrasound Obstet. Gynecol. 2011, 38, 620–624. [Google Scholar] [CrossRef] [PubMed]
- Papastefanou, I.; Souka, A.P.; Pilalis, A.; Panagopoulos, P.; Kassanos, D. Fetal intracranial translucency and cisterna magna at 11 to 14 weeks: Reference ranges and correlation with chromosomal abnormalities. Prenat. Diagn. 2011, 31, 1189–1192. [Google Scholar] [CrossRef] [Green Version]
- Guibaud, L.; Larroque, A.; Ville, D. Prenatal diagnosis of ‘isolated’ Dandy-Walker malformation: Imaging findings and prenatal counselling. Prenat. Diagn. 2012, 32, 185–193. [Google Scholar] [CrossRef]
- Timor-Tritsch, I.E.; Monteagudo, A.; Pilu, G.; Malinger, G.; Buyukkurt, S. Anomalies of the cerebellum. In Ultrasonography of the Prenatal Brain, 3rd ed.; McGraw-Hill: New York, NY, USA, 2012; pp. 283–302. [Google Scholar]
- D’Antonio, F.; Khalil, A.; Garel, C. Systematic review and meta-analysis of isolated posterior fossa malformations on prenatal ultrasound imaging (part 1): Nomenclature, diagnostic accuracy and associated anomalies. Ultrasound Obstet. Gynecol. 2016, 47, 690–697. [Google Scholar] [CrossRef]
- Society for Maternal-Fetal Medicine (SMFM); Monteagudo, A. Dandy-Walker Malformation. Am. J. Obstet. Gynecol. 2020, 223, B38–B41. [Google Scholar] [CrossRef]
- Chatzipapas, I.K.; Whitlow, B.J.; Economides, D.L. The ‘Mickey Mouse’ sign and the diagnosis of anencephaly in early pregnancy. Ultrasound Obstet. Gynecol. 1999, 13, 196–199. [Google Scholar] [CrossRef]
- Obeidi, N.; Russell, N.; Higgins, J.R.; O’Donoghue, K. The natural history of anencephaly. Prenat. Diagn. 2010, 30, 357–360. [Google Scholar] [CrossRef]
- Chen, C.-P. Chromosomal abnormalities associated with neural tube defects (I): Full aneuploidy. Taiwan J. Obstet. Gynecol. 2007, 46, 325–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, H.S.; Lam, Y.H.; Tang, M.H.; Cheung, L.W.; Ng, L.K.; Yan, K.W. First-trimester ultrasound diagnosis of holoprosencephaly: Three case reports. Ultrasound Obstet. Gynecol. 1999, 13, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, W.; Wong, A.E. First trimester screening for holoprosencephaly with choroid plexus morphology (‘butterfly’ sign) and biparietal diameter. Prenat. Diagn. 2013, 33, 1233–1237. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, W.; Wong, A.E.; Andreeva, E. Biparietal diameterto-crown-rump length disproportion in first-trimester fetuses with holoprosencephaly. J. Ultrasound Med. 2014, 33, 1165–1169. [Google Scholar] [CrossRef]
- Paladini, D.; Volpe, P. Ultrasound of Congenital Fetal Anomalies: Differential Diagnosis and Prognostic Indicators, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar] [CrossRef]
- Kagan, K.O.; Staboulidou, I.; Syngelaki, A. The 11–13-week scan: Diagnosis and outcome of holoprosencephaly, exomphalos and megacystis. Ultrasound Obstet. Gynecol. 2010, 36, 10–14. [Google Scholar] [CrossRef]
- Kim, M.S.; Jeanty, P.; Turner, C.; Benoit, B. Three-dimensional sonographic evaluation of embryonic brain development. J. Ultrasound Med. 2008, 27, 119–124. [Google Scholar] [CrossRef]
- Timor-Tritsch, I.E.; Monteagudo, A.; Santos, R. Three-dimensional inversion rendering in the first- and early second-trimester fetal brain: Its use in holoprosencephaly. Ultrasound Obstet. Gynecol. 2008, 32, 744–750. [Google Scholar] [CrossRef]
- D’Ottavio, G.; Mandruzzato, G.; Meir, Y.J.; Rustico, M.A.; Fischer-Tamaro, L.; Conoscenti, G.; Natale, R. Comparisons of first and second trimester screening for fetal anomalies. Ann. N. Y. Acad. Sci. 1998, 847, 200–209. [Google Scholar] [CrossRef]
- Loureiro, T.; Ushakov, F.; Maiz, N.; Montenegro, N.; Nicolaides, K.H. Lateral ventricles in fetuses with aneuploidies at 11–13 weeks’ gestation. Ultrasound Obstet. Gynecol. 2012, 40, 282–287. [Google Scholar] [CrossRef]
- Gaglioti, P.; Oberto, M.; Todros, T. The significance of fetal ventriculomegaly: Etiology, short- and long-term outcomes. Prenat. Diagn. 2009, 29, 381–388. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
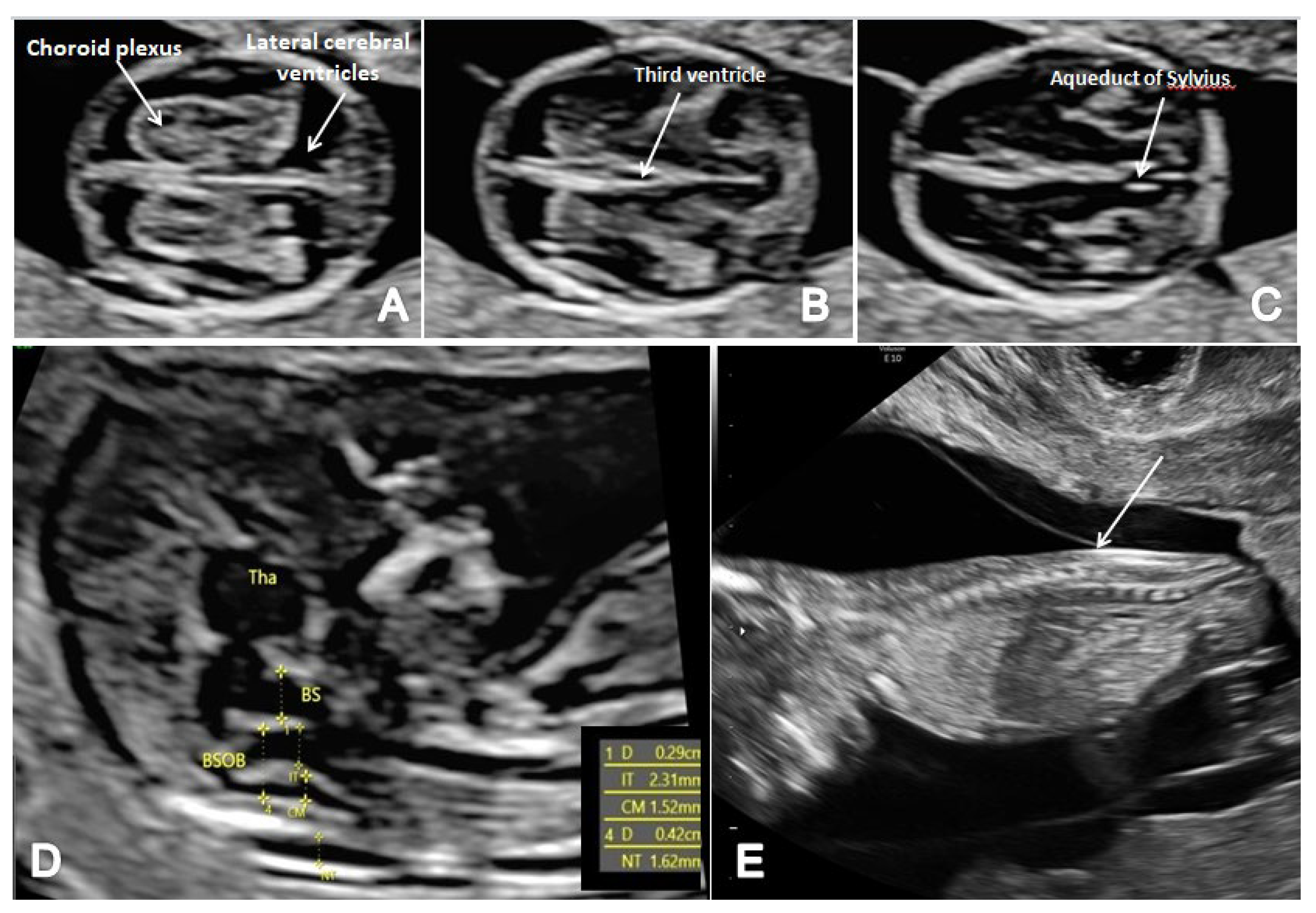
| Identification of all CNS Features by TAUS | Associated Unfavorable Conditions Requiring a Reschedule/TVUS Examination 137/1943 Cases (7.05%) | CNS Features That Were Not Properly Identified at the Initial TAUS and Required TVUS or Re-Evaluation | |||||
|---|---|---|---|---|---|---|---|
| Abnormal group (major CNS anomalies + minor CNS US markers group) | 22/26 cases (84.6%) | Fibroids 4 cases (2.9%) BMI > 24 32 cases (23.3%) unfavorable fetal position 11 cases (8%) retroverted uterus 11 cases (8%) Abdominal scar 23 cases (16.7%) Fibroids and abdominal scar 6 cases (4.3%) Unfavorable fetal position and increased BMI20 cases (14.5%) Increased BMI and abdominal scar 22 cases (16%) | The lateral ventricles and the choroid plexus | The third ventricle | The aqueduct of Sylvius | The fourth ventricle/Cisterna Magna/BS/BSOB | Spine and underlying skin |
| 2/4 cases (50%) | 2/4 cases (50%) | 1/4 cases (25%) | 3/4 cases (75%) | 1/4 cases (25%) | |||
| Normal group | 1784/1917 cases (93%) | 13/133 cases (9.7%) | 37/133 cases (27.8%) | 52/133 cases (39%) | 71/133 cases (53.3%) | 88/133 cases (66.1%) | |
| No. | GA | Ultrasound Findings Respecting the Scanning Protocol | Diagnosis | Karyotype | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| The Lateral Ventricles and the Choroid Plexus | The Third Ventricle | The Aqueduct of Sylvius | The Fourth Ventricle | Cisterna Magna | BS/BSOB | The Spine | |||||
| 1. | 12 w + 3 d | + | + | + | + | + | + | + | Open Spina Bifida | 46XY | 1st trimester TOP |
| 2. | 12 w + 5 d | − | + | + | + | + | + | + | Open Spina Bifida | Trisomy 18 | 1st trimester TOP (surgical) |
| 3. | 13 w + 2 d | − | − | − | − | − | − | + | Open Spina Bifida | 46XX | 1st trimester TOP |
| 4. | 13 w + 1 d | − | − | − | − | − | − | + | Closed Spina Bifida | 46XX | Early 2st trimester TOP |
| 5 | 12 w + 0 d | + | + | + | + | + | + | − | Anencephaly | unknown | Miscarriage |
| 6. | 12 w + 1 d | + | + | + | + | + | + | − | Anencephaly | unknown | 1st trimester TOP |
| 7. | 12 w + 4 d | + | + | + | + | + | + | − | Anencephaly | 46XX | 1st trimester TOP |
| 8. | 12 w + 3 d | + | + | + | + | + | + | − | Holoprosencephaly | unknown | 1st trimester TOP (surgical) |
| 9. | 12 w + 5 d | + | + | + | + | + | + | − | Holoprosencephaly | unknown | 1st trimester TOP |
| 10. | 13 w + 1 d | + | + | − | + | + | + | − | Holoprosencephaly | Trisomy 18 | 1st trimester TOP |
| 11. | 13 w + 5 d | + | + | + | + | + | + | − | Hydrocephaly | Trisomy 21 | Early 2st trimester TOP |
| 12. | 13 w + 4 d | − | + | + | − | + | − | − | Cephalocele | Trisomy 21 | 1st trimester TOP |
| 13. | 13 w + 6 d | − | + | + | − | + | − | − | Cephalocele | unknown | 1st trimester TOP |
| 14 | 12 w + 6 d | − | − | − | + | + | + | − | Dandy-Walker malformation | unknown | 1st trimester TOP |
| 15 | 13 w + 1 d | − | − | − | + | + | + | − | Dandy-Walker malformation | Trisomy 18 | 2st trimester TOP |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ungureanu, D.R.; Drăgușin, R.C.; Căpitănescu, R.G.; Zorilă, L.; Ofițeru, A.M.I.; Marinaș, C.; Pătru, C.L.; Comănescu, A.C.; Comănescu, M.C.; Sîrbu, O.C.; et al. First Trimester Ultrasound Detection of Fetal Central Nervous System Anomalies. Brain Sci. 2023, 13, 118. https://doi.org/10.3390/brainsci13010118
Ungureanu DR, Drăgușin RC, Căpitănescu RG, Zorilă L, Ofițeru AMI, Marinaș C, Pătru CL, Comănescu AC, Comănescu MC, Sîrbu OC, et al. First Trimester Ultrasound Detection of Fetal Central Nervous System Anomalies. Brain Sciences. 2023; 13(1):118. https://doi.org/10.3390/brainsci13010118
Chicago/Turabian StyleUngureanu, Delia Roxana, Roxana Cristina Drăgușin, Răzvan Grigoraș Căpitănescu, Lucian Zorilă, Anca Maria Istrate Ofițeru, Cristian Marinaș, Ciprian Laurențiu Pătru, Alexandru Cristian Comănescu, Maria Cristina Comănescu, Ovidiu Costinel Sîrbu, and et al. 2023. "First Trimester Ultrasound Detection of Fetal Central Nervous System Anomalies" Brain Sciences 13, no. 1: 118. https://doi.org/10.3390/brainsci13010118