

Acute Visual Impairment in a Patient with Parkinson’s Disease after Successful Bilateral Subthalamic Nucleus Deep Brain Stimulation with Low-Dose Levodopa: A Case Report

Abstract
:1. Background
2. Case Presentation
3. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PD | Parkinson disease |
| DBS | deep brain stimulation |
| STN | subthalamic nucleus |
| UPDRS | Unified Parkinson’s Disease Rating Scale |
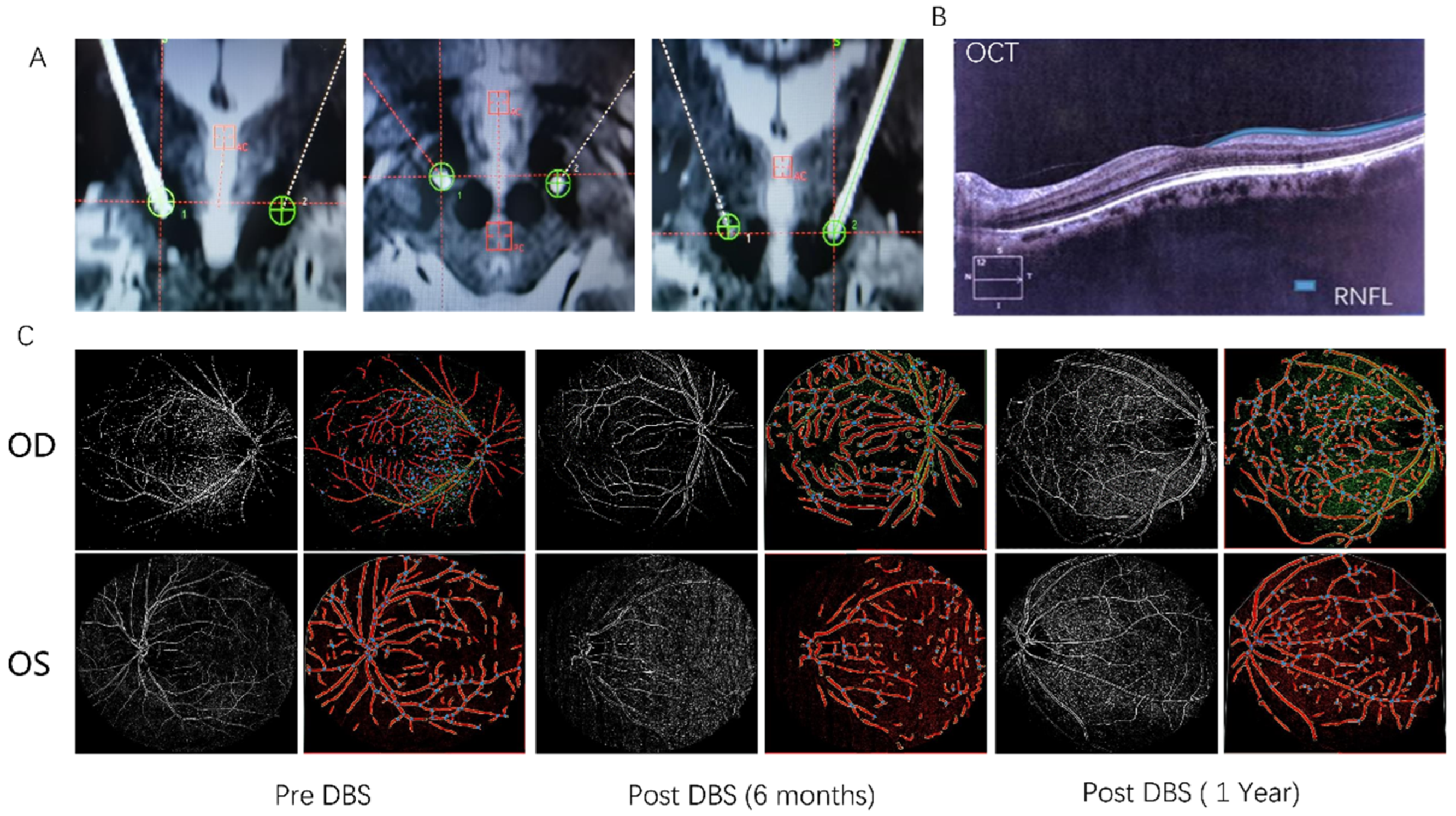
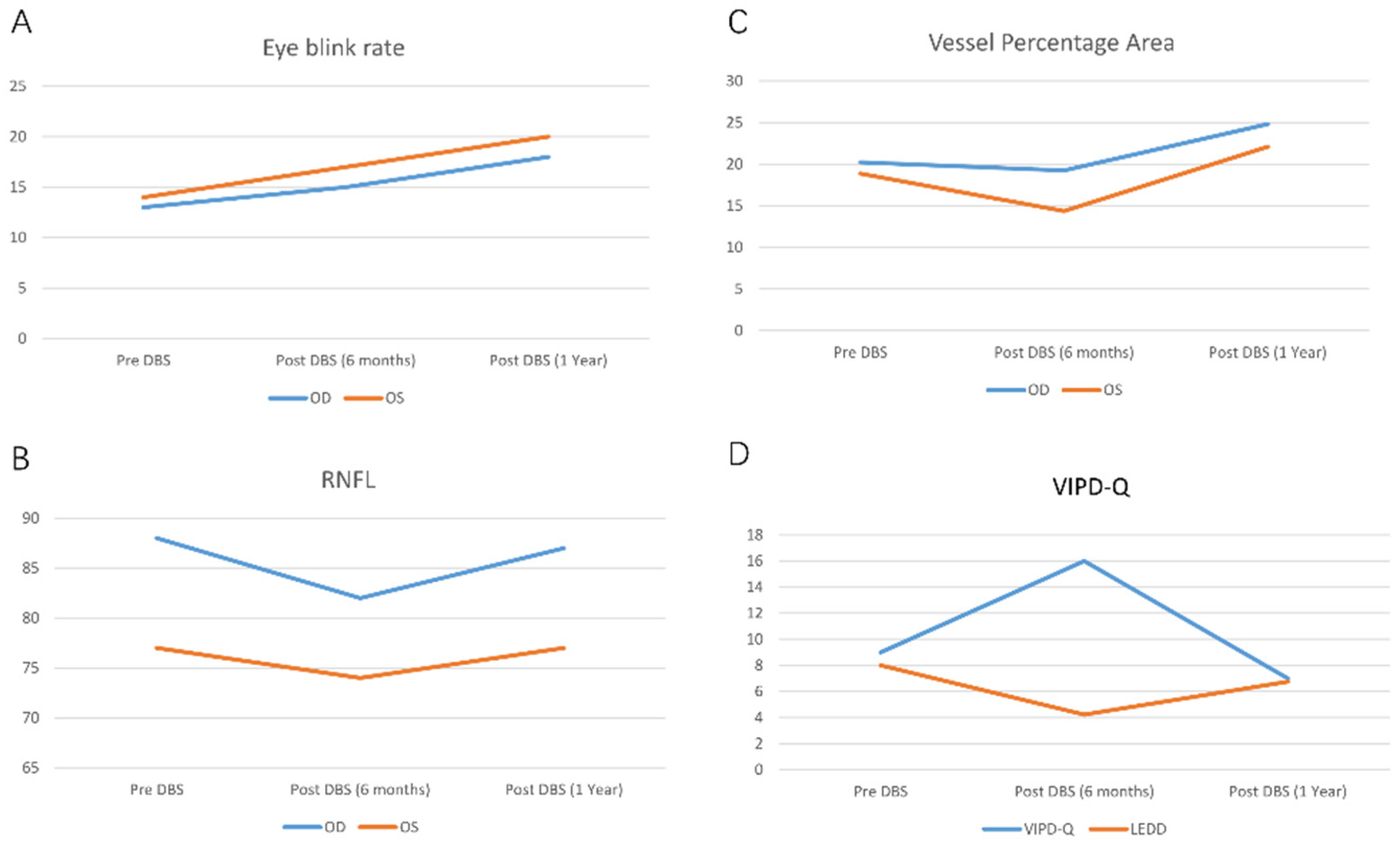
| RNFL | retinal nerve fiber layer |
| VIPD-Q | Visual Impairment in Parkinson’s Disease Questionnaire |
| VPA | vessel percentage area |
References
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA 2020, 323, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Hamedani, A.; Abraham, D.; Maguire, M.; Willis, A. Visual Impairment Is More Common in Parkinson′s Disease and Is a Risk Factor for Poor Health Outcomes. Mov. Disord. 2020, 35, 1542–1549. [Google Scholar] [CrossRef] [PubMed]
- Ekker, M.S.; Janssen, S.; Seppi, K.; Poewe, W.; de Vries, N.M.; Theelen, T.; Nonnekes, J.; Bloem, B.R. Ocular and visual disorders in Parkinson′s disease: Common but frequently overlooked. Park. Relat. Disord. 2017, 40, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokushige, S.I.; Matsuda, S.I.; Oyama, G.; Shimo, Y.; Umemura, A.; Sasaki, T.; Inomata-Terada, S.; Yugeta, A.; Hamada, M.; Ugawa, Y.; et al. Effect of subthalamic nucleus deep brain stimulation on visual scanning. Clin. Neurophysiol. 2018, 129, 2421–2432. [Google Scholar] [CrossRef] [PubMed]
- Aung, M.H.; Park, H.N.; Han, M.K.; Obertone, T.S.; Abey, J.; Aseem, F.; Thule, P.M.; Iuvone, P.M.; Pardue, M.T. Dopamine deficiency contributes to early visual dysfunction in a rodent model of type 1 diabetes. J. Neurosci. 2014, 34, 726–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krauss, J.K.; Lipsman, N.; Aziz, T.; Boutet, A.; Brown, P.; Chang, J.W.; Davidson, B.; Grill, W.M.; Hariz, M.I.; Horn, A.; et al. Technology of deep brain stimulation: Current status and future directions. Nat. Rev. Neurol. 2021, 17, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Borm, C.; Visser, F.; Werkmann, M.; de Graaf, D.; Putz, D.; Seppi, K.; Poewe, W.; Vlaar, A.; Hoyng, C.; Bloem, B.; et al. Seeing ophthalmologic problems in Parkinson disease: Results of a visual impairment questionnaire. Neurology 2020, 94, e1539–e1547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wladis, E.J.; Aakalu, V.K.; Sobel, R.K.; McCulley, T.J.; Foster, J.A.; Tao, J.P.; Freitag, S.K.; Yen, M.T. Interventions for Indirect Traumatic Optic Neuropathy: A Report by the American Academy of Ophthalmology. Ophthalmology 2021, 128, 928–937. [Google Scholar] [CrossRef]
- Razeghinejad, M.R.; Nowroozzadeh, M.H.; Eghbal, M.H. Levodopa and Other Pharmacologic Interventions in Ischemic and Traumatic Optic Neuropathies and Amblyopia. Clin. Neuropharmacol. 2016, 39, 40–48. [Google Scholar] [CrossRef]
- Diederich, N.; Pieri, V.; Hipp, G.; Rufra, O.; Blyth, S.; Vaillant, M. Discriminative power of different nonmotor signs in early Parkinson′s disease. A case-control study. Mov. Disord. 2010, 25, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.; Boyd, B.; Christensen, C.; Javid, C.; McKay, B.; Fagan, T.; Snyder, R. Levodopa Positively Affects Neovascular Age-Related Macular Degeneration. Am. J. Med. 2021, 134, 122–128.e3. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Scott, J.; Griffiths, H.; Self, J.; Lotery, A. Oral levodopa rescues retinal morphology and visual function in a murine model of human albinism. Pigment. Cell Melanoma Res. 2019, 32, 657–671. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pre-DBS | Post-DBS (1 Month) | Post-DBS (6 Months) | Post-DBS (1 Year) | ||
|---|---|---|---|---|---|
| Eye-blink rate | OD | 13 | 14 (on stimulation); 13 (off stimulation) | 15 (on stimulation); 11 (off stimulation) | 18 (on stimulation); 12 (off stimulation) |
| OS | 14 | 13 (on stimulation); 13 (off stimulation) | 17 (on stimulation); 12 (off stimulation) | 20 (on stimulation); 13 (off stimulation) | |
| RNFL | OD | 88 | 88 | 82 | 87 |
| OS | 77 | 77 | 74 | 77 | |
| VPA | OD | 20.22 | 20.12 | 19.25 | 24.82 |
| OS | 18.87 | 18.86 | 14.37 | 22.1 | |
| VIPD-Q | - | 9 | 9 | 16 | 7 |
| LEDD | - | 800 | 800 | 422.5 | 675 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, C.; Sun, J.; Li, Z.; Liu, N.; Li, C. Acute Visual Impairment in a Patient with Parkinson’s Disease after Successful Bilateral Subthalamic Nucleus Deep Brain Stimulation with Low-Dose Levodopa: A Case Report. Brain Sci. 2023, 13, 103. https://doi.org/10.3390/brainsci13010103
Zhang C, Sun J, Li Z, Liu N, Li C. Acute Visual Impairment in a Patient with Parkinson’s Disease after Successful Bilateral Subthalamic Nucleus Deep Brain Stimulation with Low-Dose Levodopa: A Case Report. Brain Sciences. 2023; 13(1):103. https://doi.org/10.3390/brainsci13010103
Chicago/Turabian StyleZhang, Chao, Jinxing Sun, Zhenke Li, Na Liu, and Chao Li. 2023. "Acute Visual Impairment in a Patient with Parkinson’s Disease after Successful Bilateral Subthalamic Nucleus Deep Brain Stimulation with Low-Dose Levodopa: A Case Report" Brain Sciences 13, no. 1: 103. https://doi.org/10.3390/brainsci13010103