
Effects of High Cervical Spinal Cord Stimulation on Gait Disturbance and Dysarthropneumophonia in Parkinson’s Disease and Parkinson Variant of Multiple System Atrophy: A Case Series
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcome Measurements
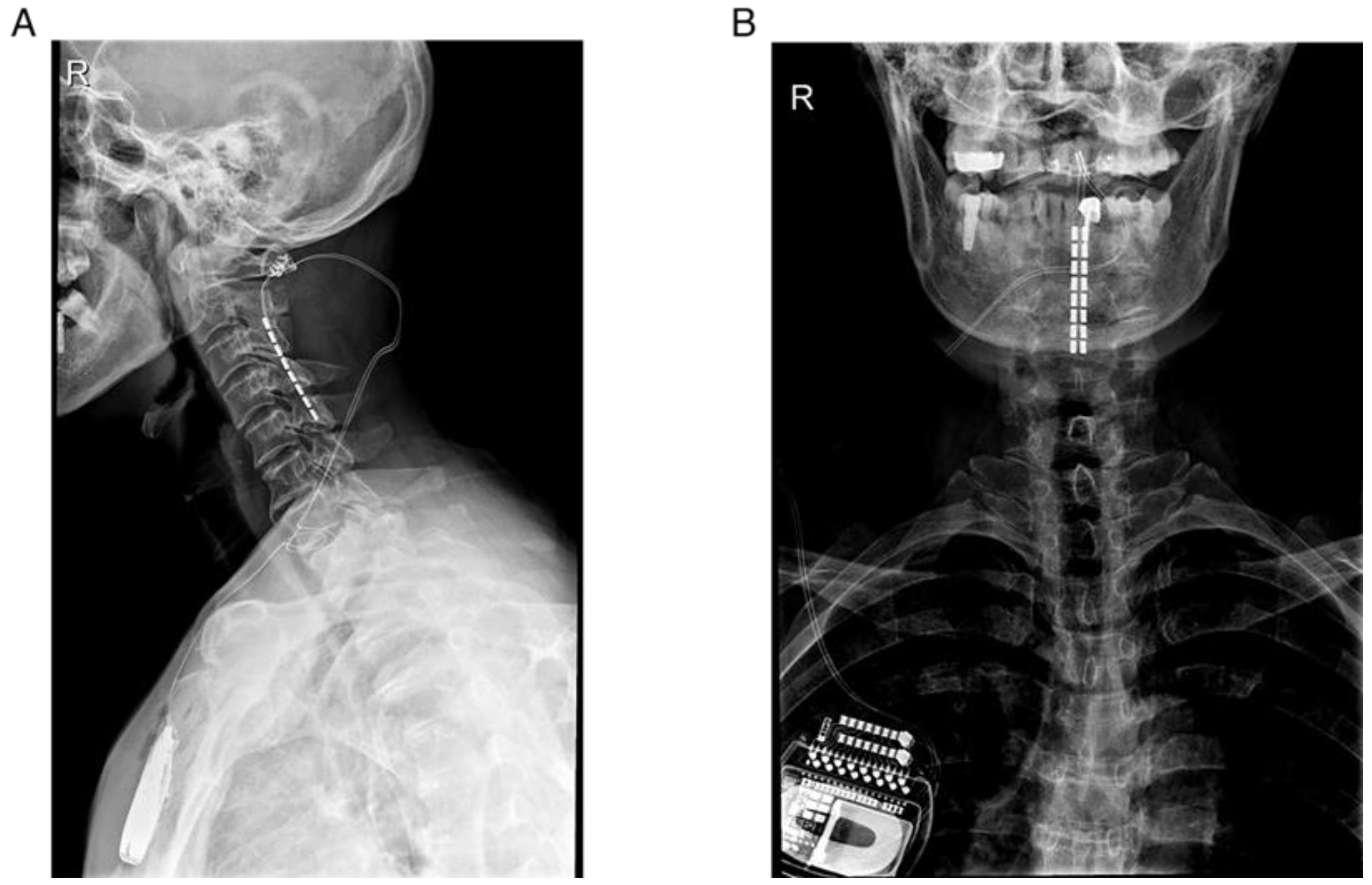
2.3. Surgical Procedure
2.4. Statistical Analyses
3. Results
3.1. Demographic Data and Stimulation Parameters
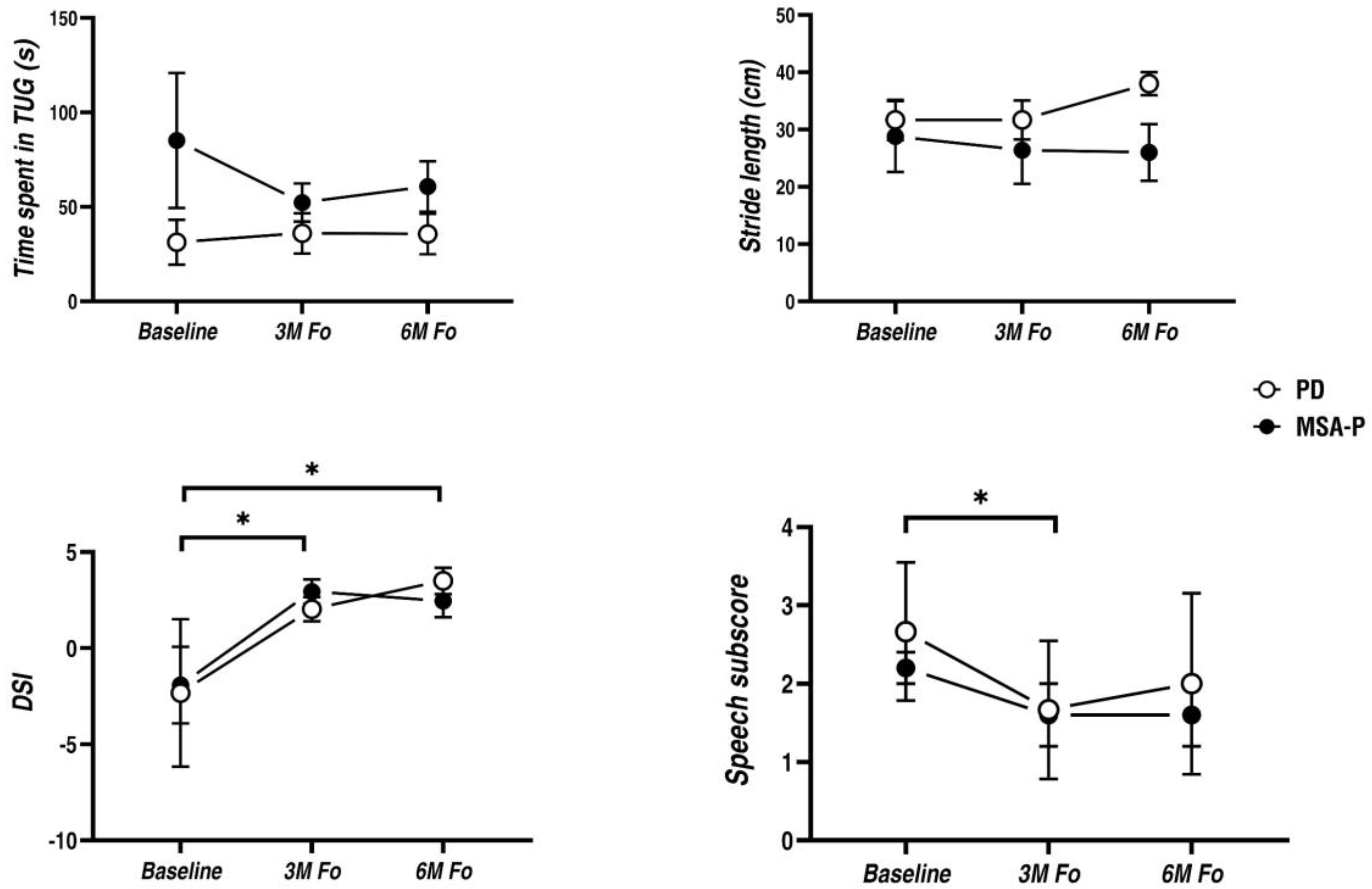
3.2. Main Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saxena, M.; Behari, M.; Kumaran, S.S.; Goyal, V.; Narang, V. Assessing Speech Dysfunction Using BOLD and Acoustic Analysis in Parkinsonism. Parkinsonism Relat. Disord. 2014, 20, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Skodda, S. Aspects of Speech Rate and Regularity in Parkinson’s Disease. J. Neurol. Sci. 2011, 310, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Huh, Y.E.; Park, J.; Suh, M.K.; Lee, S.E.; Kim, J.; Jeong, Y.; Kim, H.-T.; Cho, J.W. Differences in Early Speech Patterns between Parkinson Variant of Multiple System Atrophy and Parkinson’s Disease. Brain Lang. 2015, 147, 14–20. [Google Scholar] [CrossRef]
- Shealy, C.N.; Mortimer, J.T.; Reswick, J.B. Electrical Inhibition of Pain by Stimulation of the Dorsal Columns: Preliminary Clinical Report. Anesth. Analg. 1967, 46, 489–491. [Google Scholar] [CrossRef]
- Samotus, O.; Parrent, A.; Jog, M. Spinal Cord Stimulation Therapy for Gait Dysfunction in Advanced Parkinson’s Disease Patients. Mov. Disord. 2018, 33, 783–792. [Google Scholar] [CrossRef]
- Prasad, S.; Aguirre-Padilla, D.H.; Poon, Y.; Kalsi-Ryan, S.; Lozano, A.M.; Fasano, A. Spinal Cord Stimulation for Very Advanced Parkinson’s Disease: A 1-Year Prospective Trial. Mov. Disord. 2020, 35, 1082–1083. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, R.; Petersson, P.; Siesser, W.B.; Caron, M.G.; Nicolelis, M.A.L. Spinal Cord Stimulation Restores Locomotion in Animal Models of Parkinson’s Disease. Science 2009, 323, 1578–1582. [Google Scholar] [CrossRef] [PubMed]
- Santana, M.B.; Halje, P.; Simplício, H.; Richter, U.; Freire, M.A.M.; Petersson, P.; Fuentes, R.; Nicolelis, M.A.L. Spinal Cord Stimulation Alleviates Motor Deficits in a Primate Model of Parkinson Disease. Neuron 2014, 84, 716–722. [Google Scholar] [CrossRef]
- Deer, T.R.; Skaribas, I.M.; Haider, N.; Salmon, J.; Kim, C.; Nelson, C.; Tracy, J.; Espinet, A.; Lininger, T.E.; Tiso, R.; et al. Effectiveness of Cervical Spinal Cord Stimulation for the Management of Chronic Pain. Neuromodulation Technol. Neural Interface 2014, 17, 265–271. [Google Scholar] [CrossRef]
- Mazzone, P.; Viselli, F.; Ferraina, S.; Giamundo, M.; Marano, M.; Paoloni, M.; Masedu, F.; Capozzo, A.; Scarnati, E. High Cervical Spinal Cord Stimulation: A One Year Follow-Up Study on Motor and Non-Motor Functions in Parkinson’s Disease. Brain Sci. 2019, 9, 78. [Google Scholar] [CrossRef] [Green Version]
- Thevathasan, W.; Mazzone, P.; Jha, A.; Djamshidian, A.; Dileone, M.; di Lazzaro, V.; Brown, P. Spinal cord stimulation failed to relieve akinesia or restore locomotion in parkinson disease. Neurology 2010, 74, 1325–1327. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.; Amer, S.; Alwaki, A.; Elborno, A. A Patient with Parkinson’s Disease Benefits from Spinal Cord Stimulation. J. Clin. Neurosci. 2013, 20, 1155–1156. [Google Scholar] [CrossRef] [PubMed]
- Defazio, G.; Fabbrini, G.; Erro, R.; Albanese, A.; Barone, P.; Zibetti, M.; Esposito, M.; Pellicciari, R.; Avanzino, L.; Bono, F.; et al. Does Acute Peripheral Trauma Contribute to Idiopathic Adult-Onset Dystonia? Parkinsonism Relat. Disord. 2020, 71, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Turner, G.S.; Tjaden, K.; Weismer, G. The Influence of Speaking Rate on Vowel Space and Speech Intelligibility for Individuals with Amyotrophic Lateral Sclerosis. J. Speech Lang. Hear. Res. 1995, 38, 1001–1013. [Google Scholar] [CrossRef]
- Wuyts, F.L.; de Bodt, M.S.; Molenberghs, G.; Remacle, M.; Heylen, L.; Millet, B.; van Lierde, K.; Raes, J.; van de Heyning, P.H. The Dysphonia Severity Index: An Objective Measure of Vocal Quality Based on a Multiparameter Approach. J. Speech Lang. Hear. Res. 2000, 43, 796–809. [Google Scholar] [CrossRef]
- Fénelon, G.; Goujon, C.; Gurruchaga, J.-M.; Cesaro, P.; Jarraya, B.; Palfi, S.; Lefaucheur, J.-P. Spinal Cord Stimulation for Chronic Pain Improved Motor Function in a Patient with Parkinson’s Disease. Parkinsonism Relat. Disord. 2012, 18, 213–214. [Google Scholar] [CrossRef]
- Soltani, F.; Lalkhen, A. Improvement of parkinsonian symptoms with spinal cord stimulation: Consequence or coincidence? J. Neurol Neurosurg. Psychiatry 2013, 84, e2.74. [Google Scholar] [CrossRef]
- Landi, A.; Trezza, A.; Pirillo, D.; Vimercati, A.; Antonini, A.; Sganzerla, E. pietro Spinal Cord Stimulation for the Treatment of Sensory Symptoms in Advanced Parkinson’s Disease. Neuromodulation Technol. Neural Interface 2013, 16, 276–279. [Google Scholar] [CrossRef]
- Thiriez, C.; Gurruchaga, J.-M.; Goujon, C.; Fénelon, G.; Palfi, S. Spinal Stimulation for Movement Disorders. Neurotherapeutics 2014, 11, 543–552. [Google Scholar] [CrossRef]
- Cai, Y.; Reddy, R.D.; Varshney, V.; Chakravarthy, K.V. Spinal Cord Stimulation in Parkinson’s Disease: A Review of the Preclinical and Clinical Data and Future Prospects. Bioelectron Med. 2020, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Waltz, J.M.; Andreesen, W.H.; Hunt, D.P. Spinal Cord Stimulation and Motor Disorders. Pacing Clin. Electrophysiol. 1987, 10, 180–204. [Google Scholar] [CrossRef]
- Hakkesteegt, M.M.; Wieringa, M.H.; Brocaar, M.P.; Mulder, P.G.H.; Feenstra, L. The Interobserver and Test-Retest Variability of the Dysphonia Severity Index. Folia Phoniatr. Logop. 2008, 60, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Zhuge, P.; You, H.; Wang, H.; Zhang, Y.; Du, H. An Analysis of the Effects of Voice Therapy on Patients with Early Vocal Fold Polyps. J. Voice 2016, 30, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Pinto, S.; Ozsancak, C.; Tripoliti, E.; Thobois, S.; Limousin-Dowsey, P.; Auzou, P. Treatments for Dysarthria in Parkinson’s Disease. Lancet Neurol. 2004, 3, 547–556. [Google Scholar] [CrossRef]
- de Andrade, E.M.; Ghilardi, M.G.; Cury, R.G.; Barbosa, E.R.; Fuentes, R.; Teixeira, M.J.; Fonoff, E.T. Spinal Cord Stimulation for Parkinson’s Disease: A Systematic Review. Neurosurg. Rev. 2016, 39, 27–35. [Google Scholar] [CrossRef]
- Wang, B.J.; Carter, F.L.; Altman, K.W. Relationship between Dysarthria and Oral-Oropharyngeal Dysphagia: The Present Evidence. Ear Nose Throat J. 2020, 014556132095164. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient | Age (Year) | Gender | LEDD (mg) | Diagnosis | Disease Duration (Year) | DBS | Lead Location | Follow Up Period (mo) |
|---|---|---|---|---|---|---|---|---|
| No.1 | 53 | M | 1164.25 | PD | 13 | Yes | C2–C5 | 6 |
| No.2 | 75 | M | 550 | PD | 7 | No | C2–C5 | 6 |
| No.3 | 63 | M | 900 | PD | 4 | No | C2–C5 | 6 |
| No.4 | 60 | F | 600 | MSA-P | 6 | No | C2–C5 | 6 |
| No.5 | 61 | F | 500 | MSA-P | 6 | No | C2–C5 | 6 |
| No.6 | 58 | F | 575 | MSA-P | 4 | Yes | C2–C5 | 6 |
| No.7 | 54 | M | 300 | MSA-P | 1 | No | C2–C5 | 7 |
| No.8 | 67 | F | (-) | MSA-P | 3 | No | C2–C5 | 7 |
| Patient | Diagnosis | 3M Fo | 6M Fo | ||||
|---|---|---|---|---|---|---|---|
| Frequency (Hz) | Pulse Width (μs) # | Amplitude (V) # | Frequency (Hz) | Pulse Width (μs) # | Amplitude (V) # | ||
| No.1 | PD | 20 | 120 | 1.60 | 20 | 150 | 1 |
| No.2 | PD | 35 | 280 | 2 | 40 | 280 | 2.5 |
| No.3 | PD | 30 | 240 | 2 | 30 | 135 | 2 |
| No.4 | MSA-P | 15 | 220 | 0.45 | 15 | 120 | 0.6 |
| No.5 | MSA-P | 25 | 210 | 1.15 | 45 | 210 | 1.5 |
| No.6 | MSA-P | 45 | 310 | 0.8 | 35 | 180 | 0.55 |
| No.7 | MSA-P | 20 | 240 | 1.8 | 30 | 260 | 3.8 |
| No.8 | MSA-P | 25 | 240 | 0.8 | 25 | 240 | 1.5 |
| Baseline | 3M Fo | 6M Fo | p Value (3M Fo vs. Baseline) | p Value (6M Fo vs. Baseline) | ||
|---|---|---|---|---|---|---|
| MDS UPDRS-III | ||||||
| Total | PD | 44 (5) | 39 (3) | 37 (1) | 0.268 | 0.121 |
| MSA-P | 44 (16) | 44 (14) | 44 (18) | |||
| Rigidity subscore | PD | 8 (5) | 5 (2) | 2 (2) | 0.134 | 0.129 |
| MSA-P | 9 (4) | 8 (4) | 9 (3) | |||
| Bradykinesia subscore | PD | 21 (1) | 22 (1) | 21 (2) | 0.154 | 0.756 |
| MSA-P | 21 (14) | 23 (12) | 21 (14) | |||
| Axial subscore | PD | 13 (3) | 12 (1) | 12 (4) | 0.133 | 0.476 |
| MSA-P | 14 (4) | 13 (4) | 14 (4) | |||
| PDQ-8 | ||||||
| Total | PD | 10 (2) | 5 (4) | 9 (7) | <0.05 | 0.397 |
| MSA-P | 14 (2) | 10 (3) | 12 (2) | |||
| Baseline | 3M Fo | 6M Fo | p Value (3m Fo vs. Baseline) | p Value (6m Fo vs. Baseline) | ||
|---|---|---|---|---|---|---|
| Articulation | ||||||
| f0 (%) | PD | 152 (14) | 148 (32) | 148 (30) | 0.401 | 0.123 |
| MSA-P | 171 (37) | 189 (53) | 226 (82) | |||
| Intensity (dB) | PD | 67 (14) | 78 (4) | 81 (1) | <0.01 | <0.05 |
| MSA-P | 68 (5) | 77 (6) | 76 (4) | |||
| Phonation | ||||||
| Jitter (%) | PD | 2.9 (3.8) | 0.3 (0.1) | 0.2 (0.1) | <0.05 | <0.05 |
| MSA-P | 3.6 (2.9) | 0.3 (0.1) | 0.2 (0.2) | |||
| Shimmer (%) | PD | 17.2 (6.7) | 11.9 (2.5) | 12.1 (3.6) | 0.073 | <0.05 |
| MSA-P | 22.8 (15.6) | 9.5 (3.1) | 7.4 (3.0) | |||
| HNR (dB) | PD | 4.6 (3.6) | 9.0 (1.9) | 11.0 (2.3) | 0.236 | <0.05 |
| MSA-P | 11.5 (4.4) | 11.5 (5.1) | 16.8 (5.3) | |||
| Resonance | ||||||
| VSA (Hz2) | PD | 72,608 (29,029) | 282,290 (147,647) | 80,814 (59,988) | 0.069 | 0.401 |
| MSA-P | 111,526 (161,014) | 175,379 (87,519) | 156,835 (79,689) | |||
| Respiration | ||||||
| MPT (s) | PD | 8.8 (5.3) | 8.9 (3.4) | 13.0 (8.0) | 0.582 | 0.401 |
| MSA-P | 7.9 (3.9) | 6.8 (3.9) | 8.7 (7.4) | |||
| Prosody | ||||||
| SD f0 (%) | PD | 2.3 (3.0) | 1.2 (0.8) | 2.0 (2.7) | <0.05 | 0.069 |
| MSA-P | 19.5 (11.0) | 1.3 (1.0) | 4.6 (8.1) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Zhu, R.; Pan, Y.; Huang, P.; Tan, Y.; Fang, B.; Liu, J.; Li, D. Effects of High Cervical Spinal Cord Stimulation on Gait Disturbance and Dysarthropneumophonia in Parkinson’s Disease and Parkinson Variant of Multiple System Atrophy: A Case Series. Brain Sci. 2022, 12, 1222. https://doi.org/10.3390/brainsci12091222
Wang L, Zhu R, Pan Y, Huang P, Tan Y, Fang B, Liu J, Li D. Effects of High Cervical Spinal Cord Stimulation on Gait Disturbance and Dysarthropneumophonia in Parkinson’s Disease and Parkinson Variant of Multiple System Atrophy: A Case Series. Brain Sciences. 2022; 12(9):1222. https://doi.org/10.3390/brainsci12091222
Chicago/Turabian StyleWang, Linbin, Rui Zhu, Yixin Pan, Peng Huang, Yuyan Tan, Boyan Fang, Jun Liu, and Dianyou Li. 2022. "Effects of High Cervical Spinal Cord Stimulation on Gait Disturbance and Dysarthropneumophonia in Parkinson’s Disease and Parkinson Variant of Multiple System Atrophy: A Case Series" Brain Sciences 12, no. 9: 1222. https://doi.org/10.3390/brainsci12091222