
What Do We Know about Social and Non-Social Factors Influencing the Pathway from Cognitive Health to Dementia? A Systematic Review of Reviews
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Methods
2.2. Eligibility Criteria
2.3. Data Extraction and Synthesis
2.4. Quality Assessment
3. Results
3.1. Literature Search and Study Selection
3.2. Included SRs and MAs Characteristics
3.3. Quality Assessment Results
3.4. Categorization of the Obtained Data
3.4.1. Somatic Diseases and Biological Factors
3.4.2. Lifestyle
3.4.3. Social
3.4.4. Psychiatric & Psychological
3.4.5. Socioeconomic
3.4.6. Environmental
3.4.7. Demographic
3.5. Types of Relationships (Negative or Positive) between Factors and Cognitive Function
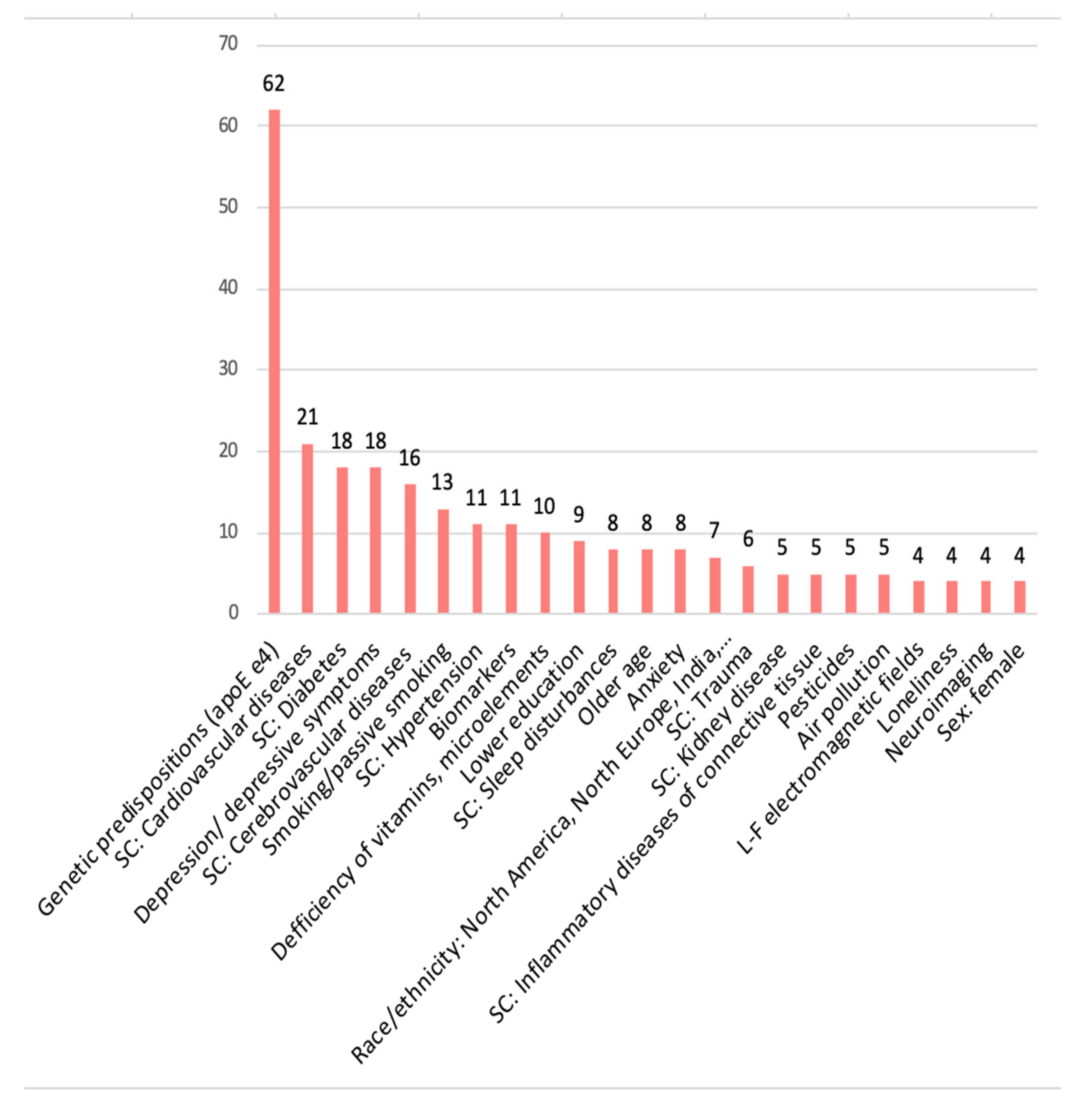
3.5.1. Negative Relationship (‘Risk Factors’)
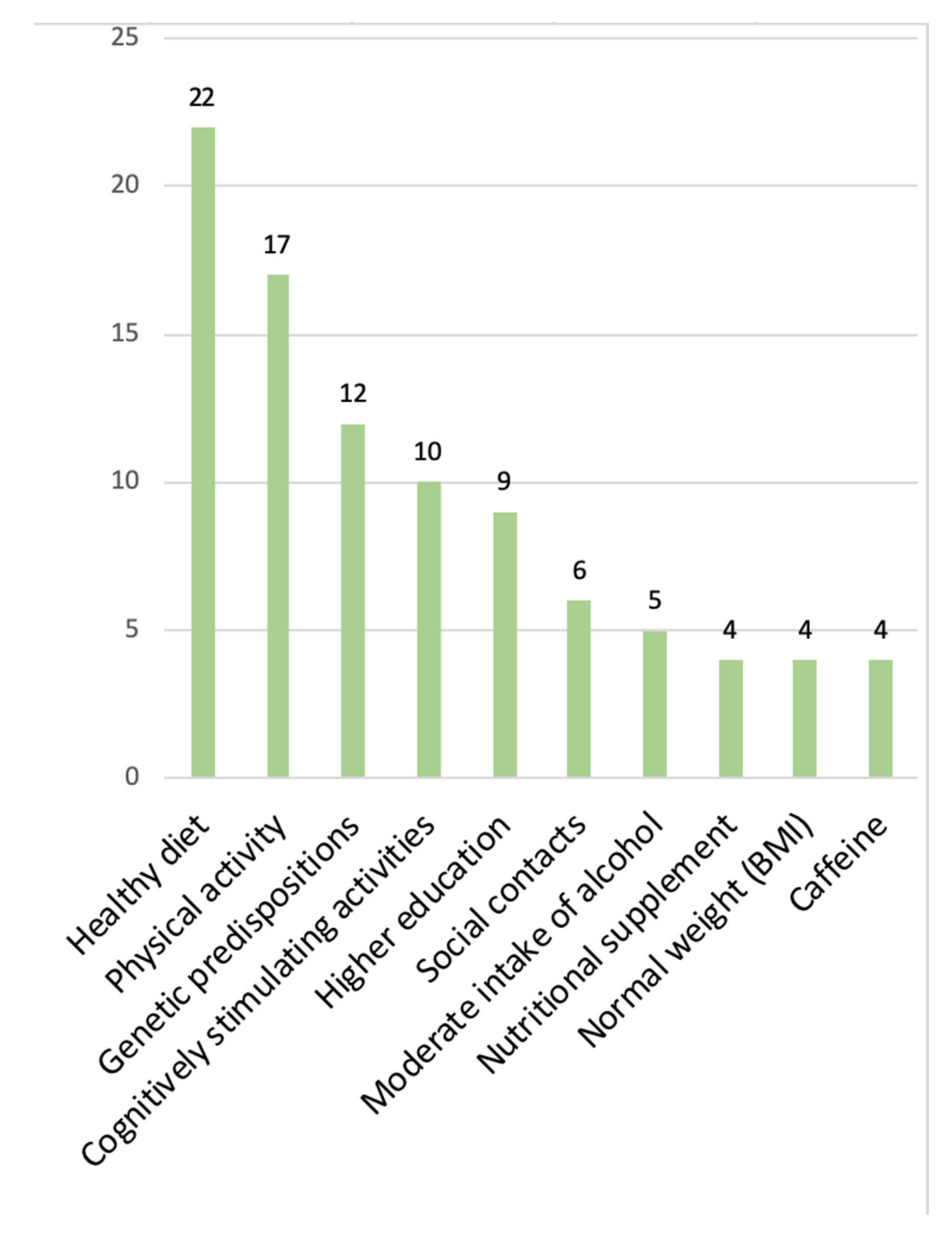
3.5.2. Positive Relationship (‘Protective Factors’)
3.5.3. Inconsistent Results (‘Unclear Association’)
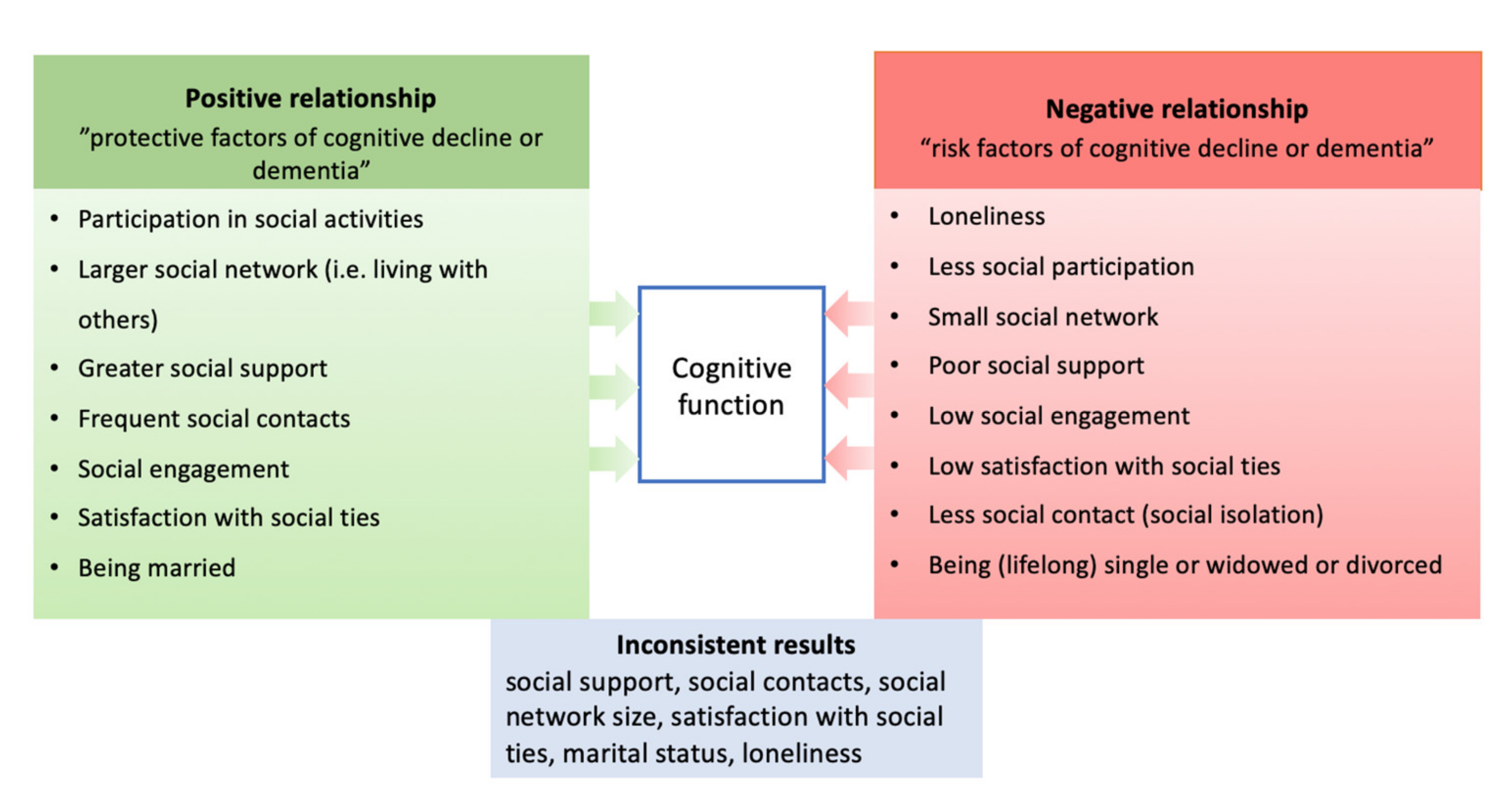
3.6. Inconsistent Results on Social Factors and Their Relationship with Cognitive Functioning in the Context of Dementia Development
3.6.1. Reports on Cognitive Health
3.6.2. Reports on Cognitive Decline, Dementia, and AD
4. Discussion
4.1. Findings on Social Factors in the Context of Other Research
4.2. Research Gaps and Implications for Future Studies
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bihaqi, S.W.; Schumacher, A.; Maloney, B.; Lahiri, D.K.; Zawia, N.H. Do Epigenetic Pathways Initiate Late Onset Alzheimer Disease (LOAD): Towards a New Paradigm. Curr. Alzheimer Res. 2012, 9, 574–588. [Google Scholar] [CrossRef]
- Fenoglio, C.; Scarpini, E.; Serpente, M.; Galimberti, D. Role of Genetics and Epigenetics in the Pathogenesis of Alzheimer’s Disease and Frontotemporal Dementia. J. Alzheimer’s Dis. 2018, 62, 913–932. [Google Scholar] [CrossRef] [PubMed]
- Licher, S.; Ahmad, S.; Karamujić-Čomić, H.; Voortman, T.; Leening, M.J.G.; Ikram, M.A.; Ikram, M.K. Genetic Predisposition, Modifiable-Risk-Factor Profile and Long-Term Dementia Risk in the General Population. Nat. Med. 2019, 25, 1364–1369. [Google Scholar] [CrossRef] [PubMed]
- Bellou, V.; Belbasis, L.; Tzoulaki, I.; Middleton, L.T.; Ioannidis, J.P.A.; Evangelou, E. Systematic Evaluation of the Associations between Environmental Risk Factors and Dementia: An Umbrella Review of Systematic Reviews and Meta-Analyses. Alzheimers. Dement. 2017, 13, 406–418. [Google Scholar] [CrossRef] [PubMed]
- Killin, L.O.J.; Starr, J.M.; Shiue, I.J.; Russ, T.C. Environmental Risk Factors for Dementia: A Systematic Review. BMC Geriatr. 2016, 16, 175. [Google Scholar] [CrossRef]
- Hussenoeder, F.S. Riedel-Heller Primary Prevention of Dementia: From Modifiable Risk Factors to a Public Brain Health Agenda? Soc. Psychiatry Psychiatr. Epidemiol. Int. J. Res. Soc. Genet. Epidemiol. Ment. Health Serv. 2018, 53, 1289–1301. [Google Scholar] [CrossRef]
- Marioni, R.E.; Proust-Lima, C.; Amieva, H.; Brayne, C.; Matthews, F.E.; Dartigues, J.F.; Jacqmin-Gadda, H. Social Activity, Cognitive Decline and Dementia Risk: A 20-Year Prospective Cohort Study Chronic Disease Epidemiology. BMC Public Health 2015, 15, 1–8. [Google Scholar] [CrossRef]
- Anstey, K.J.; Ee, N.; Eramudugolla, R.; Jagger, C.; Peters, R. A Systematic Review of Meta-Analyses That Evaluate Risk Factors for Dementia to Evaluate the Quantity, Quality, and Global Representativeness of Evidence. J. Alzheimer’s Dis. 2019, 70, S165–S186. [Google Scholar] [CrossRef]
- Peters, R.; Booth, A.; Rockwood, K.; Peters, J.; D’Este, C.; Anstey, K.J. Combining Modifiable Risk Factors and Risk of Dementia: A Systematic Review and Meta-Analysis. BMJ Open 2019, 9, 1–22. [Google Scholar] [CrossRef]
- Clare, L.; Wu, Y.T.; Teale, J.C.; MacLeod, C.; Matthews, F.; Brayne, C.; Woods, B. Potentially Modifiable Lifestyle Factors, Cognitive Reserve, and Cognitive Function in Later Life: A Cross-Sectional Study. PLoS Med. 2017, 14, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Evans, I.E.M.; Llewellyn, D.J.; Matthews, F.; Woods, B.; Brayne, C.; Clare, L. P4-185: Social Isolation, Cognitive Reserve, and Cognition in Older People With Mental Health Problems. Alzheimer’s Dement. 2018, 14, P1509–P1510. [Google Scholar] [CrossRef]
- Ihle, A.; Oris, M.; Sauter, J.; Rimmele, U.; Kliegel, M. Cognitive Reserve and Social Capital Accrued in Early and Midlife Moderate the Relation of Psychological Stress to Cognitive Performance in Old Age. Dement. Geriatr. Cogn. Disord. 2018, 45, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Fleck, J.I.; Arnold, M.; Dykstra, B.; Casario, K.; Douglas, E.; Morris, O. Distinct Functional Connectivity Patterns Are Associated With Social and Cognitive Lifestyle Factors: Pathways to Cognitive Reserve. Front. Aging Neurosci. 2019, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Penninkilampi, R.; Casey, A.N.; Singh, M.F.; Brodaty, H. The Association between Social Engagement, Loneliness, and Risk of Dementia: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2018, 66, 1619–1633. [Google Scholar] [CrossRef]
- Stern, Y. What Is Cognitive Reserve? Theory and Research Application of the Reserve Concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Fratiglioni, L.; Marseglia, A.; Dekhtyar, S. Ageing without Dementia: Can Stimulating Psychosocial and Lifestyle Experiences Make a Difference? Lancet Neurol. 2020, 19, 533–543. [Google Scholar] [CrossRef]
- Valenzuela, M.J.; Sachdev, P. Brain Reserve and Dementia: A Systematic Review. Psychol. Med. 2006, 36, 441–454. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; André Knottnerus, J.; Green, L.; Van Der Horst, H.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; Van Der Meer, J.W.M.; et al. How Should We Define Health? BMJ 2011, 343, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Dröes, R.M.; Chattat, R.; Diaz, A.; Gove, D.; Graff, M.; Murphy, K.; Verbeek, H.; Vernooij-Dassen, M.; Clare, L.; Johannessen, A.; et al. Social Health and Dementia: A European Consensus on the Operationalization of the Concept and Directions for Research and Practice. Aging Ment. Health 2017, 21, 4–17. [Google Scholar] [CrossRef]
- Plassman, B.L.; Williams, J.W.J.; Burke, J.R.; Holsinger, T.; Benjamin, S. Systematic Review: Factors Associated with Risk for and Possible Prevention of Cognitive Decline in Later Life. Ann. Intern. Med. 2010, 153, 182–193. [Google Scholar] [CrossRef] [Green Version]
- Hunt, H.; Pollock, A.; Campbell, P.; Estcourt, L.; Brunton, G. An Introduction to Overviews of Reviews: Planning a Relevant Research Question and Objective for an Overview. Syst. Rev. 2018, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Vonville, H. Excel Workbook for Screening Titles and Abstracts; UTHealth School of Public Health Library: Houston, TX, USA, 2015. [Google Scholar]
- Fleiss, J.L. Measuring Nominal Scale Agreement among Many Raters. Psychol. Bull. 1971, 76, 378–382. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing Systematic Reviews: Methodological Development, Conduct and Reporting of an Umbrella Review Approach. Int. J. Evid. Based. Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef]
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A Measurement Tool to Assess the Methodological Quality of Systematic Reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef]
- Kelly, M.E.; Duff, H.; Kelly, S.; McHugh Power, J.E.; Brennan, S.; Lawlor, B.A.; Loughrey, D.G. The Impact Ofsocial Activities, Social Networks, Social Support and Social Relationships on the Cognitive Functioning of Healthy Older Adults: A Systematic Review SR. Syst. Rev. 2017, 6, 259. [Google Scholar] [CrossRef]
- Wu, Z.; Phyo, A.Z.Z.; Al-harbi, T.; Woods, R.L.; Ryan, J. Distinct Cognitive Trajectories in Late Life and Associated Predictors and Outcomes: A Systematic Review. J. Alzheimer’s Dis. Rep. 2020, 4, 459–478. [Google Scholar] [CrossRef]
- Boss, L.; Kang, D.-H.; Branson, S. Loneliness and Cognitive Function in the Older Adult: A Systematic Review. Int. Psychogeriatrics 2015, 27, 541–553. [Google Scholar] [CrossRef]
- Besser, L.M.; McDonald, N.C.; Song, Y.; Kukull, W.A.; Rodriguez, D.A. Neighborhood Environment and Cognition in Older Adults: A Systematic Review. Am. J. Prev. Med. 2017, 53, 241–251. [Google Scholar] [CrossRef]
- Kuiper, J.S.; Zuidersma, M.; Oude Voshaar, R.C.; Zuidema, S.U.; van den Heuvel, E.R.; Stolk, R.P.; Smidt, N. Social Relationships and Risk of Dementia: A Systematic Review and Meta-Analysis of Longitudinal Cohort Studies. Ageing Res. Rev. 2015, 22, 39–57. [Google Scholar] [CrossRef]
- Kuiper, J.S.; Zuidersma, M.; Zuidema, S.U.; Burgerhof, J.G.M.; Stolk, R.P.; Oude Voshaar, R.C.; Smidt, N. Social Relationships and Cognitive Decline: A Systematic Review and Meta-Analysis of Longitudinal Cohort Studies. Int. J. Epidemiol. 2016, 45, 1169–1206. [Google Scholar] [CrossRef] [PubMed]
- Lekoubou, A.; Echouffo-Tcheugui, J.B.; Kengne, A.P. Epidemiology of Neurodegenerative Diseases in Sub-Saharan Africa: A Systematic Review. BMC Public Health 2014, 14, 653. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, L.Y.; Marzo, A.; Mu~noz-Ruiz, M.; Ikram, M.A.; Kivipelto, M.; Ruefenacht, D.; Venneri, A.; Soininen, H.; Wanke, I.; Ventikos, Y.A.; et al. Modifiable Lifestyle Factors in Dementia: A Systematic Review of Longitudinal Observational Cohort Studies. J. Alzheimer’s Dis. 2014, 42, 119–135. [Google Scholar] [CrossRef]
- Lafortune, L.; Martin, S.; Kelly, S.; Kuhn, I.; Remes, O.; Cowan, A.; Brayne, C. Behavioural Risk Factors in Mid-Life Associated with Successful Ageing, Disability, Dementia and Frailty in Later Life: A Rapid Systematic Review. PLoS ONE 2016, 11, e0144405. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; John, A.; Stott, J.; Charlesworth, G. Living Alone and Risk of Dementia: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2020, 62, 101122. [Google Scholar] [CrossRef]
- McGrattan, A.M.; Zhu, Y.; Richardson, C.D.; Mohan, D.; Soh, Y.C.; Sajjad, A.; Van Aller, C.; Chen, S.; Paddick, S.M.; Prina, M.; et al. Prevalence and Risk of Mild Cognitive Impairment in Low and Middle-Income Countries: A Systematic Review. J. Alzheimer’s Dis. 2021, 79, 743–762. [Google Scholar] [CrossRef]
- Hersi, M.; Irvine, B.; Gupta, P.; Gomes, J.; Birkett, N.; Krewski, D. Risk Factors Associated with the Onset and Progression of Alzheimer’s Disease: A Systematic Review of the Evidence. Neurotoxicology 2017, 61, 143–187. [Google Scholar] [CrossRef]
- Sommerlad, A.; Ruegger, J.; Singh-Manoux, A.; Lewis, G.; Livingston, G. Marriage and Risk of Dementia: Systematic Review and Meta-Analysis of Observational Studies. J. Neurol. Neurosurg. Psychiatry 2017, 89, 231–238. [Google Scholar] [CrossRef]
- Walker, J.D.; Spiro, G.; Loewen, K.; Jacklin, K. Alzheimer’s Disease and Related Dementia in Indigenous Populations: A Systematic Review of Risk Factors. J. Alzheimer’s Dis. 2020, 78, 1439–1451. [Google Scholar] [CrossRef]
- Tang, E.Y.H.; Harrison, S.L.; Errington, L.; Gordon, M.F.; Visser, P.J.; Novak, G.; Dufouil, C.; Brayne, C.; Robinson, L.; Launer, L.J.; et al. Current Developments in Dementia Risk Prediction Modelling: An Updated Systematic Review. PLoS ONE 2015, 10, e0136181. [Google Scholar] [CrossRef] [Green Version]
- Qiu, C.; De Ronchi, D.; Fratiglioni, L. The Epidemiology of the Dementias: An Update. Curr. Opin. Psychiatry 2007, 20, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Qiu, C.; Xu, W.; Fratiglioni, L. Vascular and Psychosocial Factors in Alzheimer’s Disease: Epidemiological Evidence toward Intervention. J. Alzheimer’s Dis. 2010, 20, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Rakesh, G.; Szabo, S.; Alexopoulos, G.S.; Zannas, A.S. Strategies for Dementia Prevention: Latest Evidence and Implications. Ther. Adv. Chronic Dis. 2017, 8, 121–136. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.B.; Becofsky, K.; Anderson, L.A.; Bryant, L.L.; Hunter, H.; Ivey, S.L.; Belza, B.; Logsdon, R.G.; Brannon, S.; Ann, E. Public Perceptions about Risk and Protective Factors for Cognitive Health and Impairment: A Review of the Literature. Int. Psychogeriatr. 2015, 27, 1263–1275. [Google Scholar] [CrossRef]
- Gaugler, J.E.; Bain, L.J.; Mitchell, L.; Finlay, J.; Fazio, S.; Jutkowitz, E.; Banerjee, S.; Butrum, K.; Gaugler, J.; Gitlin, L.; et al. Reconsidering Frameworks of Alzheimer’s Dementia When Assessing Psychosocial Outcomes. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2019, 5, 388–397. [Google Scholar] [CrossRef]
- Vernooij-Dassen, M.; Moniz-Cook, E.; Verhey, F.; Chattat, R.; Woods, B.; Meiland, F.; Franco, M.; Holmerova, I.; Orrell, M.; de Vugt, M. Bridging the Divide between Biomedical and Psychosocial Approaches in Dementia Research: The 2019 INTERDEM Manifesto. Aging Ment. Health 2019, 25, 206–212. [Google Scholar] [CrossRef]
- Chapko, D.; McCormack, R.; Black, C.; Staff, R.; Murray, A. Life-Course Determinants of Cognitive Reserve (CR) in Cognitive Aging and Dementia—A Systematic Literature Review. Aging Ment. Health 2017, 22, 915–926. [Google Scholar] [CrossRef]
- Meng, X.; D’Arcy, C. Education and Dementia in the Context of the Cognitive Reserve Hypothesis: A Systematic Review with Meta-Analyses and Qualitative Analyses. PLoS ONE 2012, 7, e38268. [Google Scholar] [CrossRef]
- Fleck, J.I.; Kuti, J.; Mercurio, J.; Mullen, S.; Austin, K.; Pereira, O. The Impact of Age and Cognitive Reserve on Resting-State Brain Connectivity. Front. Aging Neurosci. 2017, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Study | % | n |
|---|---|---|
| Systematic review (SR) | 41.1 | 129 |
| Meta-analysis (MA) | 22.6 | 71 |
| Systematic review and Meta-analysis | 36.3 | 114 |
| Publication Year | ||
| 2009 | 4.1 | 13 |
| 2010 | 3.5 | 11 |
| 2011 | 4.8 | 15 |
| 2012 | 7.3 | 23 |
| 2013 | 9.5 | 30 |
| 2014 | 7.6 | 24 |
| 2015 | 8.9 | 28 |
| 2016 | 13.4 | 42 |
| 2017 | 18.2 | 57 |
| 2018 | 13.1 | 41 |
| 2019 | 8.3 | 26 |
| 2020 | 1.0 | 3 |
| 2021 | 0.3 | 1 |
| Country (by first author) | ||
| European countries (UK) | 35.8 | 112 (41) |
| China | 28.3 | 89 |
| USA | 12.7 | 40 |
| Australia | 7.3 | 23 |
| Canada | 5.7 | 18 |
| Asia (various) | 5.4 | 17 |
| South America | 3.8 | 12 |
| Africa | 1.0 | 3 |
| Age of participants | ||
| Young adulthood and mid-life (<65) | 0.9 | 3 |
| Mid-life and late-life (≥40) | 45.2 | 142 |
| Late-life (≥65) | 23.6 | 74 |
| All ages (≥18) | 13.7 | 43 |
| No data | 16.6 | 52 |
| Cognitive outcome variables (n = 462) | % | n = 462 |
| Cognitively Healthy (CH) [incl. Cognitive Reserve (CR)] | 10.4 | 48 (2) |
| Subjective Cognitive Impairment (SCI) | 0.6 | 3 |
| Cognitive impairment/Cognitive decline (CI/CD) | 24.0 | 111 |
| Mild Cognitive Impairment (MCI) | 10.4 | 48 |
| Dementia (any type) (D) [incl. AD] | 54.6 (34.6) | 252 (160) |
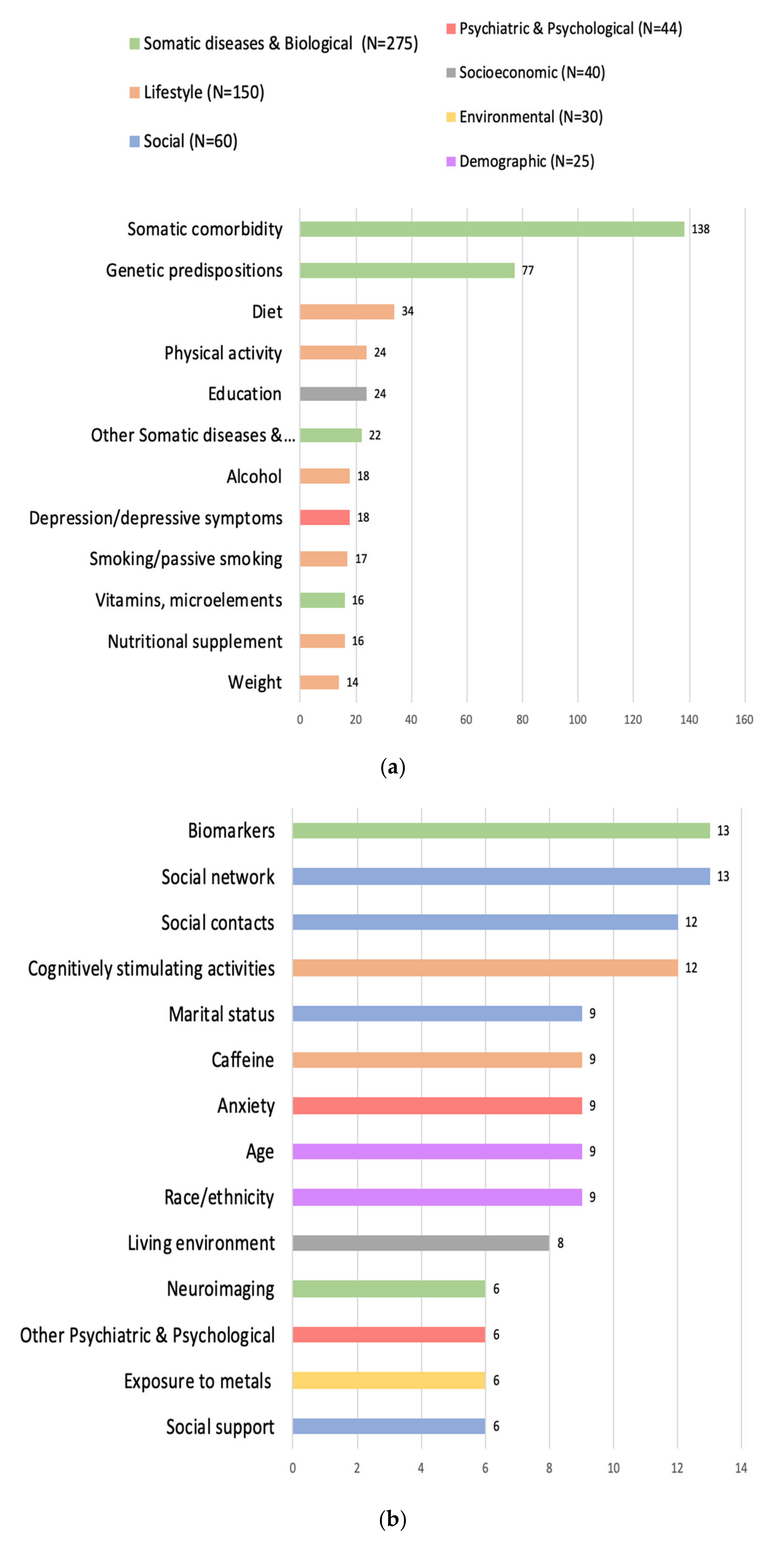
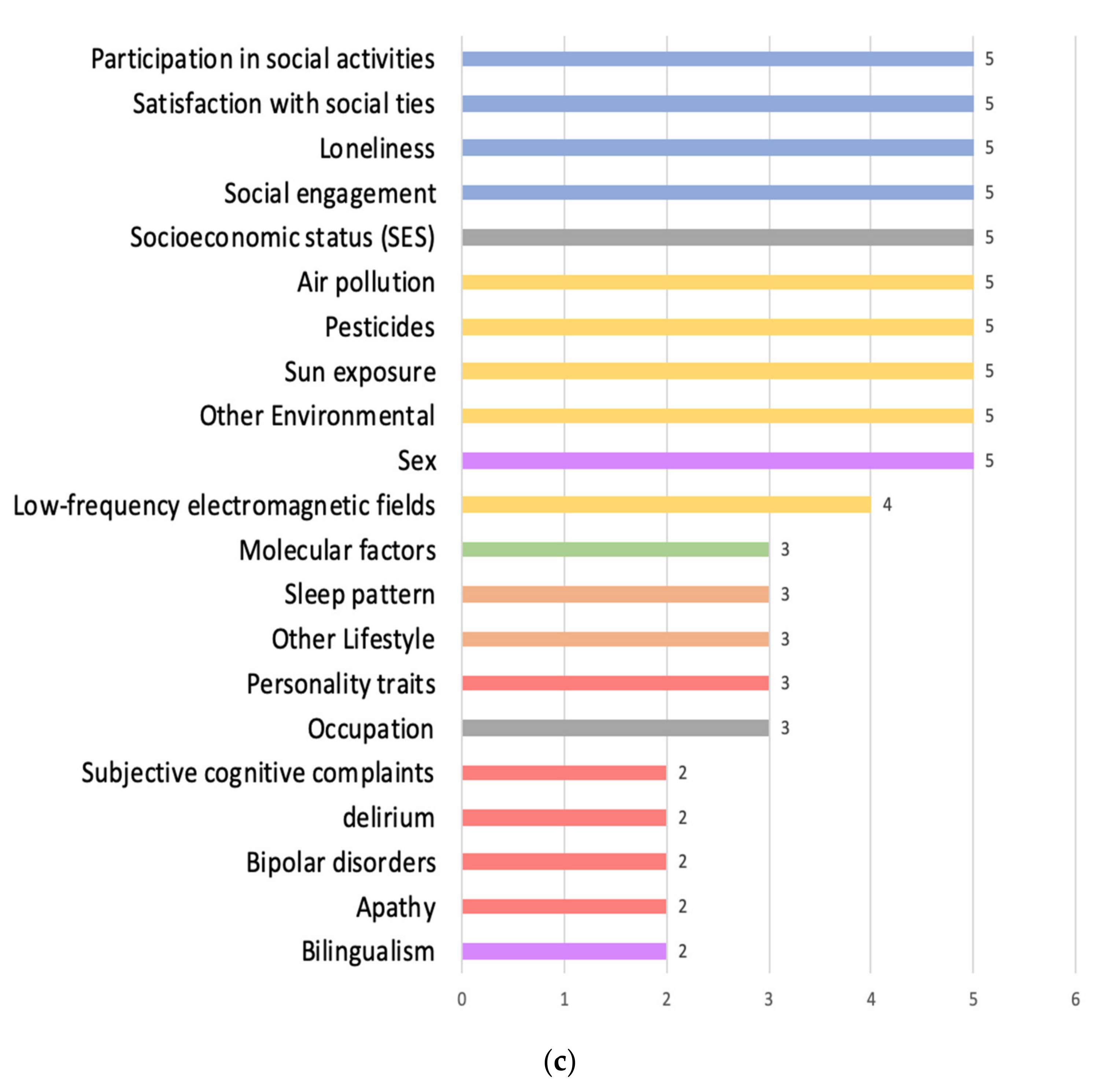
| Category | Subcategory | Frequency of Reporting the Factors |
|---|---|---|
| Demographic (n = 25) | Age | 9 |
| Race/ethnicity | 9 | |
| Sex | 5 | |
| Bilingualism | 2 | |
| Environmental (n = 30) | Exposure to metals | 6 |
| Air pollution | 5 | |
| Pesticides | 5 | |
| Sun exposure | 5 | |
| Other Environmental | 4 | |
| Low-frequency electromagnetic fields | 4 | |
| Socioeconomic (n = 40) | Education | 24 |
| Living environment | 8 | |
| Socioeconomic status (SES) | 5 | |
| Occupation | 3 | |
| Psychiatric & Psychological (n = 44) | Depression/depressive symptoms | 18 |
| Anxiety | 9 | |
| Other Psychiatric & Psychological | 6 | |
| Personality traits | 3 | |
| Subjective cognitive complaints | 2 | |
| Delirium | 2 | |
| Bipolar disorders | 2 | |
| Apathy | 2 | |
| Social (n = 60) | Social network | 13 |
| Social contacts/isolation | 12 | |
| Marital status | 9 | |
| Social support | 6 | |
| Participation in social activities | 5 | |
| Satisfaction with social ties | 5 | |
| Loneliness | 5 | |
| Social engagement | 5 | |
| Lifestyle (n = 150) | Diet | 34 |
| Physical activity | 24 | |
| Alcohol | 18 | |
| (passive) Smoking | 17 | |
| Nutritional supplement | 16 | |
| Weight | 14 | |
| Cognitively stimulating activities | 12 | |
| Caffeine | 9 | |
| Sleep pattern | 3 | |
| Other lifestyle | 3 | |
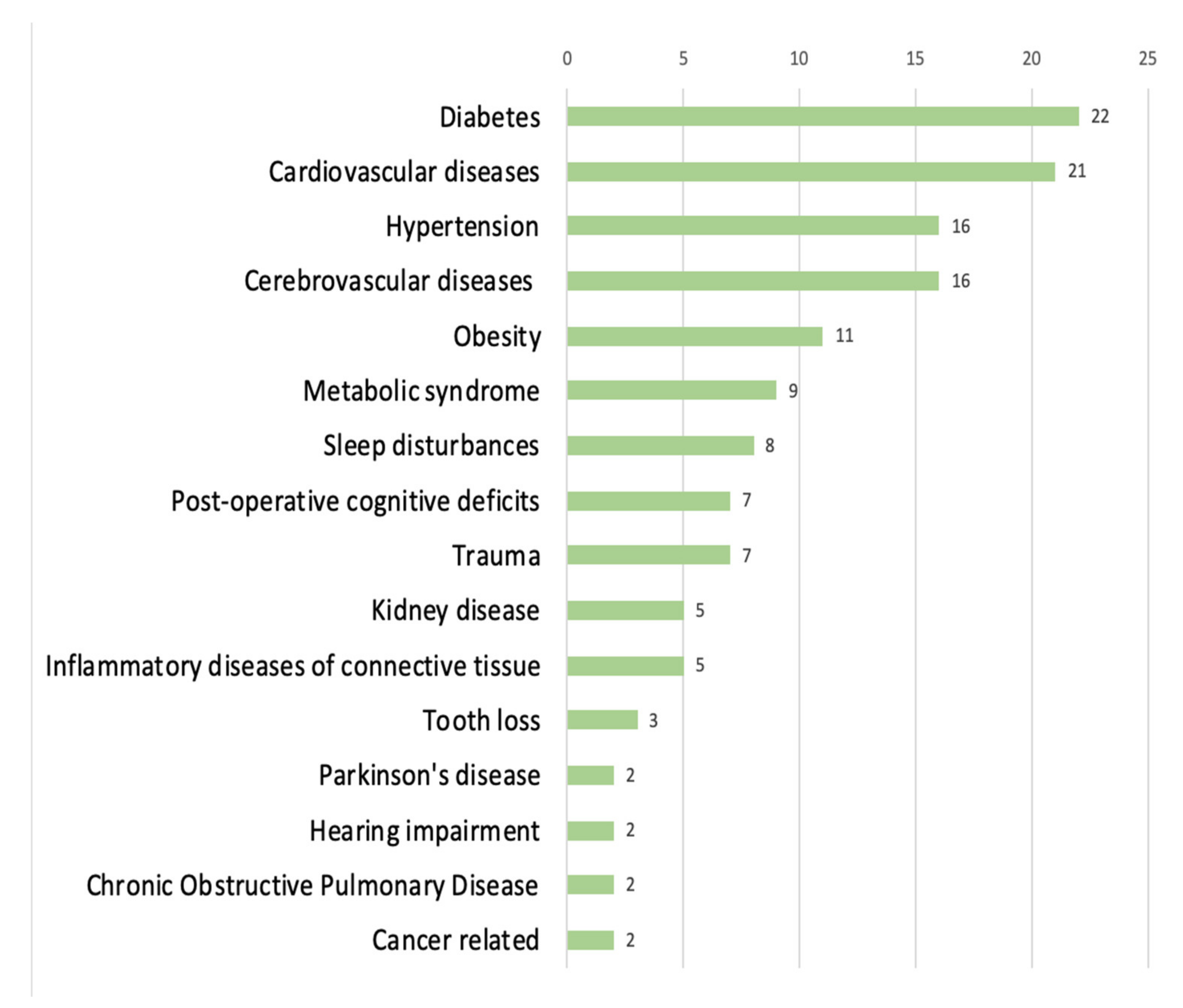
| Somatic diseases & Biological (n = 275) | Somatic Comorbidity | 138 |
| Genetic predispositions | 77 | |
| Other somatic diseases & biological | 22 | |
| Vitamins, microelements | 16 | |
| Biomarkers | 13 | |
| Neuroimaging | 6 | |
| Molecular factors | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenart-Bugla, M.; Łuc, M.; Pawłowski, M.; Szcześniak, D.; Seifert, I.; Wiegelmann, H.; Gerhardus, A.; Wolf-Ostermann, K.; Rouwette, E.A.J.A.; Ikram, M.A.; et al. What Do We Know about Social and Non-Social Factors Influencing the Pathway from Cognitive Health to Dementia? A Systematic Review of Reviews. Brain Sci. 2022, 12, 1214. https://doi.org/10.3390/brainsci12091214
Lenart-Bugla M, Łuc M, Pawłowski M, Szcześniak D, Seifert I, Wiegelmann H, Gerhardus A, Wolf-Ostermann K, Rouwette EAJA, Ikram MA, et al. What Do We Know about Social and Non-Social Factors Influencing the Pathway from Cognitive Health to Dementia? A Systematic Review of Reviews. Brain Sciences. 2022; 12(9):1214. https://doi.org/10.3390/brainsci12091214
Chicago/Turabian StyleLenart-Bugla, Marta, Mateusz Łuc, Marcin Pawłowski, Dorota Szcześniak, Imke Seifert, Henrik Wiegelmann, Ansgar Gerhardus, Karin Wolf-Ostermann, Etiënne A. J. A. Rouwette, M. Arfan Ikram, and et al. 2022. "What Do We Know about Social and Non-Social Factors Influencing the Pathway from Cognitive Health to Dementia? A Systematic Review of Reviews" Brain Sciences 12, no. 9: 1214. https://doi.org/10.3390/brainsci12091214