
Factors Associated with Fear of Falling in Individuals with Different Types of Mild Cognitive Impairment

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
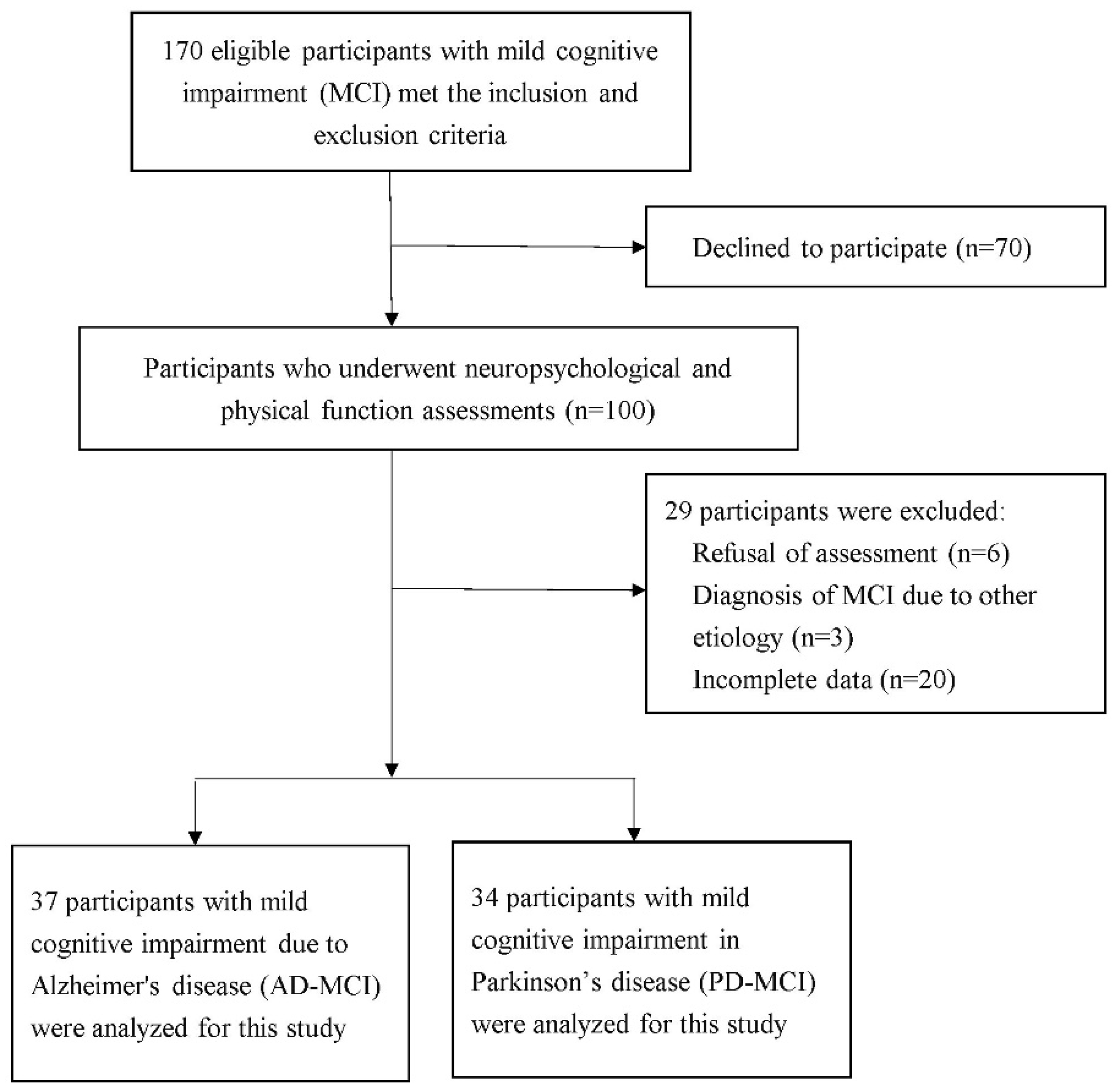
2.1. Participants and Study Design
2.2. Defining the MCI Etiologies
2.3. Assessment of Fear of Falling
2.4. Outcome Measures
2.5. Statistics
3. Results
3.1. Baseline Demographic Data and Comparisons between AD-MCI and PD-MCI
3.2. Factors Determining FOF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katz, R.; Shah, P. The patient who falls: Challenges for families, clinicians, and communities. JAMA 2010, 303, 273–274. [Google Scholar] [CrossRef] [PubMed]
- Borges Sde, M.; Radanovic, M.; Forlenza, O.V. Fear of falling and falls in older adults with mild cognitive impairment and Alzheimer’s disease. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2015, 22, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Gazibara, T.; Kurtagic, I.; Kisic-Tepavcevic, D.; Nurkovic, S.; Kovacevic, N.; Gazibara, T.; Pekmezovic, T. Falls, risk factors and fear of falling among persons older than 65 years of age. Psychogeriatrics 2017, 17, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Hoang, O.T.; Jullamate, P.; Piphatvanitcha, N.; Rosenberg, E. Factors related to fear of falling among community-dwelling older adults. J. Clin. Nurs. 2017, 26, 68–76. [Google Scholar] [CrossRef]
- Holtzer, R.; Friedman, R.; Lipton, R.B.; Katz, M.; Xue, X.; Verghese, J. The relationship between specific cognitive functions and falls in aging. Neuropsychology 2007, 21, 540–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch. Neurol. 2001, 58, 1985–1992. [Google Scholar] [CrossRef]
- Allali, G.; Launay, C.P.; Blumen, H.M.; Callisaya, M.L.; De Cock, A.M.; Kressig, R.W.; Srikanth, V.; Steinmetz, J.P.; Verghese, J.; Beauchet, O. Falls, Cognitive Impairment, and Gait Performance: Results from the GOOD Initiative. J. Am. Med. Dir. Assoc. 2017, 18, 335–340. [Google Scholar] [CrossRef] [Green Version]
- Scheffer, A.C.; Schuurmans, M.J.; van Dijk, N.; van der Hooft, T.; de Rooij, S.E. Fear of falling: Measurement strategy, prevalence, risk factors and consequences among older persons. Age Ageing 2008, 37, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.O.; Nordberg, A.; Bäckman, L.; Albert, M.; Almkvist, O.; et al. Mild cognitive impairment--beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [Green Version]
- Litvan, I.; Goldman, J.G.; Tröster, A.I.; Schmand, B.A.; Weintraub, D.; Petersen, R.C.; Mollenhauer, B.; Adler, C.H.; Marder, K.; Williams-Gray, C.H.; et al. Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: Movement Disorder Society Task Force guidelines. Mov. Disord. 2012, 27, 349–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palavra, N.C.; Naismith, S.L.; Lewis, S.J. Mild cognitive impairment in Parkinson’s disease: A review of current concepts. Neurol. Res. Int. 2013, 2013, 576091. [Google Scholar] [CrossRef] [PubMed]
- O’Bryant, S.E.; Lacritz, L.H.; Hall, J.; Waring, S.C.; Chan, W.; Khodr, Z.G.; Massman, P.J.; Hobson, V.; Cullum, C.M. Validation of the New Interpretive Guidelines for the Clinical Dementia Rating Scale Sum of Boxes Score in the National Alzheimer’s Coordinating Center Database. Arch. Neurol. 2010, 67, 746–749. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-F.; Chwo, M.-J.; Wen, C.-H.; Yang, C.-C. A Three Month Follow-up Study of Hemorrhagic Stroke Patients Receiving Rehabilitation Therapy as Assessed by the Barthel Index. Taiwan J. Fam. Med. 2007, 17, 250–263. [Google Scholar]
- Chuang, Y.-F.; Sung, H.-C.; Lin, L.-P. Health Status and Health Resource Utilization among Older People in Rural Mining Area. Tzu Chi Nurs. J. 2005, 4, 34–41. [Google Scholar]
- Gibb, W.R.; Lees, A.J. The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1988, 51, 745–752. [Google Scholar] [CrossRef] [Green Version]
- Powell, L.E.; Myers, A.M. The Activities-specific Balance Confidence (ABC) Scale. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1995, 50, M28–M34. [Google Scholar] [CrossRef]
- Talley, K.M.; Wyman, J.F.; Gross, C.R. Psychometric properties of the activities-specific balance confidence scale and the survey of activities and fear of falling in older women. J. Am. Geriatr. Soc. 2008, 56, 328–333. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Tsolaki, M.; Chantzi, H.; Kazis, A. Mini Mental State Examination (MMSE): A validation study in Greece. Am. J. Alzheimer’s Dis. Other Dement. 2000, 15, 342–345. [Google Scholar] [CrossRef]
- Arnett, J.A.; Labovitz, S.S. Effect of physical layout in performance of the Trail Making Test. Psychol. Assess. 1995, 7, 220–221. [Google Scholar] [CrossRef]
- Brucki, S.M.; Rocha, M.S. Category fluency test: Effects of age, gender and education on total scores, clustering and switching in Brazilian Portuguese-speaking subjects. Braz. J. Med. Biol. Res. 2004, 37, 1771–1777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, J.T. Measures of short-term memory: A historical review. Cortex 2007, 43, 635–650. [Google Scholar] [CrossRef]
- Chang, C.C.; Kramer, J.H.; Lin, K.N.; Chang, W.N.; Wang, Y.L.; Huang, C.W.; Lin, Y.T.; Chen, C.; Wang, P.N. Validating the Chinese version of the Verbal Learning Test for screening Alzheimer’s disease. J. Int. Neuropsychol. Soc. 2010, 16, 244–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calamia, M.; Markon, K.; Denburg, N.L.; Tranel, D. Developing a short form of Benton’s Judgment of Line Orientation Test: An item response theory approach. Clin. Neuropsychol. 2011, 25, 670–684. [Google Scholar] [CrossRef] [Green Version]
- del Toro, C.M.; Bislick, L.P.; Comer, M.; Velozo, C.; Romero, S.; Gonzalez Rothi, L.J.; Kendall, D.L. Development of a short form of the Boston naming test for individuals with aphasia. J. Speech Lang. Hear. Res. 2011, 54, 1089–1100. [Google Scholar] [CrossRef]
- Liu, C.Y.; Wang, S.J.; Teng, E.L.; Fuh, J.L.; Lin, C.C.; Lin, K.N.; Chen, H.M.; Lin, C.H.; Wang, P.N.; Yang, Y.Y.; et al. Depressive disorders among older residents in a Chinese rural community. Psychol. Med. 1997, 27, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- De Ridder, R.; Lebleu, J.; Willems, T.; De Blaiser, C.; Detrembleur, C.; Roosen, P. Concurrent Validity of a Commercial Wireless Trunk Triaxial Accelerometer System for Gait Analysis. J. Sport Rehabil. 2019, 28, jsr.2018-0295. [Google Scholar] [CrossRef] [Green Version]
- Tavares, G.M.S.; Pacheco, B.P.; Gottlieb, M.G.V.; Müller, D.V.K.; Santos, G.M. Interaction between cognitive status, fear of falling, and balance in elderly persons. Clinics 2020, 75, e1612. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.-T.; Wang, W.-S. Comparison of three established measures of fear of falling in community-dwelling older adults: Psychometric testing. Int. J. Nurs. Stud. 2009, 46, 1313–1319. [Google Scholar] [CrossRef]
- Henry, J.D.; Thompson, C.; Ruffman, T.; Leslie, F.; Withall, A.; Sachdev, P.; Brodaty, H. Threat perception in mild cognitive impairment and early dementia. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2009, 64, 603–607. [Google Scholar] [CrossRef] [Green Version]
- Shirooka, H.; Nishiguchi, S.; Fukutani, N.; Tashiro, Y.; Nozaki, Y.; Hirata, H.; Yamaguchi, M.; Tasaka, S.; Matsushita, T.; Matsubara, K.; et al. Cognitive impairment is associated with the absence of fear of falling in community-dwelling frail older adults. Geriatr. Gerontol. Int. 2017, 17, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Muir, S.W.; Gopaul, K.; Montero Odasso, M.M. The role of cognitive impairment in fall risk among older adults: A systematic review and meta-analysis. Age Ageing 2012, 41, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Sakurai, R.; Suzuki, H.; Ogawa, S.; Kawai, H.; Yoshida, H.; Hirano, H.; Ihara, K.; Obuchi, S.; Fujiwara, Y. Fear of falling, but not gait impairment, predicts subjective memory complaints in cognitively intact older adults. Geriatr. Gerontol. Int. 2017, 17, 1125–1131. [Google Scholar] [CrossRef]
- Peeters, G.; Leahy, S.; Kennelly, S.; Kenny, R.A. Is Fear of Falling Associated with Decline in Global Cognitive Functioning in Older Adults: Findings from the Irish Longitudinal Study on Ageing. J. Am. Med. Dir. Assoc. 2018, 19, 248–254.e3. [Google Scholar] [CrossRef]
- Noh, H.M.; Roh, Y.K.; Song, H.J.; Park, Y.S. Severe Fear of Falling Is Associated with Cognitive Decline in Older Adults: A 3-Year Prospective Study. J. Am. Med. Dir. Assoc. 2019, 20, 1540–1547. [Google Scholar] [CrossRef] [PubMed]
- Quattropani, M.C.; Sardella, A.; Morgante, F.; Ricciardi, L.; Alibrandi, A.; Lenzo, V.; Catalano, A.; Squadrito, G.; Basile, G. Impact of cognitive Reserve and Premorbid IQ on Cognitive and Functional Status in Older Outpatients. Brain Sci. 2021, 11, 824. [Google Scholar] [CrossRef] [PubMed]
- Woollacott, M.; Shumway-Cook, A. Attention and the control of posture and gait: A review of an emerging area of research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef]
- Lindholm, B.; Hagell, P.; Hansson, O.; Nilsson, M.H. Factors associated with fear of falling in people with Parkinson’s disease. BMC Neurol. 2014, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Haertner, L.; Elshehabi, M.; Zaunbrecher, L.; Pham, M.H.; Maetzler, C.; van Uem, J.M.T.; Hobert, M.A.; Hucker, S.; Nussbaum, S.; Berg, D.; et al. Effect of Fear of Falling on Turning Performance in Parkinson’s Disease in the Lab and at Home. Front. Aging Neurosci. 2018, 10, 78. [Google Scholar] [CrossRef] [PubMed]
- Uemura, K.; Shimada, H.; Makizako, H.; Doi, T.; Tsutsumimoto, K.; Yoshida, D.; Anan, Y.; Ito, T.; Lee, S.; Park, H.; et al. Effects of mild and global cognitive impairment on the prevalence of fear of falling in community-dwelling older adults. Maturitas 2014, 78, 62–66. [Google Scholar] [CrossRef]
- Cheng, F.Y.; Yang, Y.R.; Wang, C.J.; Wu, Y.R.; Cheng, S.J.; Wang, H.C.; Wang, R.Y. Factors influencing turning and its relationship with falls in individuals with Parkinson’s disease. PLoS ONE 2014, 9, e93572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nutt, J.G.; Bloem, B.R.; Giladi, N.; Hallett, M.; Horak, F.B.; Nieuwboer, A. Freezing of gait: Moving forward on a mysterious clinical phenomenon. Lancet Neurol. 2011, 10, 734–744. [Google Scholar] [CrossRef]
- Visser, J.E.; Voermans, N.C.; Oude Nijhuis, L.B.; van der Eijk, M.; Nijk, R.; Munneke, M.; Bloem, B.R. Quantification of trunk rotations during turning and walking in Parkinson’s disease. Clin. Neurophysiol. 2007, 118, 1602–1606. [Google Scholar] [CrossRef]
- Parry, S.W.; Bamford, C.; Deary, V.; Finch, T.L.; Gray, J.; MacDonald, C.; McMeekin, P.; Sabin, N.J.; Steen, I.N.; Whitney, S.L.; et al. Cognitive-behavioural therapy-based intervention to reduce fear of falling in older people: Therapy development and randomised controlled trial—The Strategies for Increasing Independence, Confidence and Energy (STRIDE) study. Health Technol. Assess 2016, 20, 1–206. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Delbaere, K.; Zijlstra, G.A.; Carpenter, H.; Iliffe, S.; Masud, T.; Skelton, D.; Morris, R.; Kendrick, D. Exercise for reducing fear of falling in older people living in the community: Cochrane systematic review and meta-analysis. Age Ageing 2016, 45, 345–352. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Total (n = 71) | AD-MCI (N = 37) | PD-MCI (N = 34) | p-Value |
|---|---|---|---|---|
| Gender (male/female) | 38/33 | 20/17 | 18/16 | 0.936 |
| Age (years) | 70.46 ± 9.64 | 72.41 ± 8.84 | 68.35 ± 10.16 | 0.077 |
| Education (years) | 7.85 ± 3.95 | 7.03 ± 4.11 | 8.74 ± 3.61 | 0.068 |
| Onset duration (years) | 1.83 ± 1.80 | 2.11 ± 1.91 | 1.53 ± 1.54 | 0.167 |
| Falls history (n) | 28 | 11 | 17 | 0.081 |
| BMI | 23.93 ± 3.42 | 23.86 ± 3.6 | 24.00 ± 3.27 | 0.861 |
| Barthel Index | 98.21 ± 7.42 | 99.59 ± 1.82 | 96.67 ± 10.51 | 0.124 |
| IADL | 21.54 ± 4.76 | 22.27 ± 4.37 | 20.73 ± 5.11 | 0.178 |
| Hypertension (n) | 42 | 26 | 16 | 0.047 |
| Diabetes mellitus (n) | 20 | 12 | 8 | 0.405 |
| Cardiovascular disease (n) | 25 | 19 | 6 | 0.003 |
| Global cognitive function | ||||
| MMSE | 25.32 ± 3.57 | 24.65 ± 4.10 | 26.06 ± 2.79 | 0.096 |
| Episodic memory | ||||
| CVLT-SF | 18.79 ± 5.40 | 18.70 ± 5.36 | 18.88 ± 5.51 | 0.890 |
| Visuospatial performance | ||||
| Judgment of line orientation | 13.51 ± 3.56 | 13.25 ± 3.23 | 13.79 ± 3.91 | 0.534 |
| Attention and working memory | ||||
| Forward digits | 7.24 ± 1.53 | 7.43 ± 1.56 | 7.03 ± 1.49 | 0.269 |
| Backward digits | 3.97 ± 1.52 | 4.03 ± 1.67 | 3.91 ± 1.38 | 0.753 |
| Executive function | ||||
| Category fluency test | 12.45 ± 3.79 | 12.57 ± 3.87 | 12.32 ± 3.76 | 0.789 |
| Trail making test A (s) | 25.60 ± 15.57 | 24.51 ± 15.22 | 26.81 ± 16.09 | 0.542 |
| Trail making test B (s) | 67.00 ± 36.49 | 63.67 ± 36.67 | 70.65 ± 36.50 | 0.431 |
| Language | ||||
| Boston naming test | 22.39 ± 5.24 | 21.78 ± 5.48 | 23.06 ± 4.97 | 0.309 |
| Depression | ||||
| GDS-15 | 3.07 ± 3.34 | 2.76 ± 3.11 | 3.42 ± 3.60 | 0.408 |
| Anxiety | ||||
| GAD-7 | 2.43 ± 3.67 | 2.00 ± 3.66 | 2.91 ± 3.68 | 0.304 |
| Fear of falling | ||||
| ABC scale | 82.40 ± 22.60 | 90.28 ± 16.10 | 73.58 ± 25.62 | 0.002 |
| Balance and gait performance | ||||
| Tinetti gait | 14.91 ± 2.52 | 15.62 ± 1.21 | 14.12 ± 3.30 | 0.018 |
| Tinetti balance | 11.44 ± 1.52 | 11.86 ± 0.67 | 10.97 ± 2.01 | 0.019 |
| Straight walking performance | ||||
| Gait speed (m/s) | 0.84 ± 0.22 | 0.87 ± 0.22 | 0.82 ± 0.21 | 0.302 |
| Stride length (cm) | 63.01 ± 19.39 | 63.36 ± 17.38 | 62.63 ± 21.57 | 0.876 |
| Cadence (steps/min) | 97.86 ± 14.18 | 97.60 ± 11.39 | 98.13 ± 16.81 | 0.878 |
| TUG subtasks | ||||
| Sit-to-stand (s) | 1.83 ± 0.57 | 1.74 ± 0.58 | 1.91 ± 0.55 | 0.209 |
| Turn-to-walk (s) | 2.65 ± 1.34 | 2.23 ± 0.80 | 3.11 ± 1.64 | 0.007 |
| Turn-to-sit (s) | 2.50 ± 1.53 | 2.09 ± 0.93 | 2.96 ± 1.91 | 0.022 |
| Stand-to-sit (s) | 2.45 ± 0.89 | 2.40 ± 0.83 | 2.51 ± 0.97 | 0.593 |
| Group | AD-MCI Group (N = 37) | PD-MCI Group (N = 34) | |||
|---|---|---|---|---|---|
| ABC Score | ABC Score | ||||
| Domain | Outcome Measures | r | p-Value | r | p-Value |
| Cognition | MMSE | 0.431 * | 0.008 | 0.244 | 0.165 |
| CVLT-SF | 0.315 | 0.058 | 0.221 | 0.209 | |
| Judgment of line orientation | 0.217 | 0.203 | 0.011 | 0.952 | |
| Forward digits | 0.516 * | 0.001 | 0.297 | 0.088 | |
| Backward digits | 0.414 * | 0.012 | 0.117 | 0.510 | |
| Category fluency test | 0.155 | 0.360 | 0.279 | 0.109 | |
| Trail making test A | −0.290 | 0.082 | −0.319 | 0.070 | |
| Trail making test B | −0.409 * | 0.013 | −0.221 | 0.217 | |
| Boston naming test | 0.234 | 0.164 | 0.252 | 0.150 | |
| Depression | GDS-15 | −0.250 | 0.136 | −0.056 | 0.754 |
| Anxiety | GAD-7 | −0.218 | 0.195 | −0.173 | 0.329 |
| Group | AD-MCI Group (N = 37) | PD-MCI Group (N = 34) | |||
|---|---|---|---|---|---|
| ABC Score | ABC Score | ||||
| Domain | Outcome Measures | r | p-Value | r | p-Value |
| Gait performance | Speed (m/s) | 0.507 * | 0.002 | 0.385 * | 0.027 |
| Stride Length | 0.439 * | 0.007 | 0.321 | 0.065 | |
| Cadence step | 0.349 * | 0.037 | 0.119 | 0.503 | |
| Tinetti assessment scale | Tinetti Posture | 0.482 * | 0.003 | 0.165 | 0.352 |
| Tinetti Gait | 0.336 * | 0.042 | 0.317 | 0.068 | |
| TUG subtasks | Turn-to-walk | −0.316 | 0.056 | −0.663 ** | <0.001 |
| Turn-to-sit | −0.302 | 0.069 | −0.464 * | 0.006 | |
| Sit-to-stand | −0.292 | 0.079 | −0.503 * | 0.002 | |
| Stand-to-sit | −0.138 | 0.415 | −0.229 | 0.192 | |
| AD-MCI Group | PD-MCI Group | ||||
|---|---|---|---|---|---|
| Variable | β | Coefficient | Variable | β | Coefficient |
| Age | −0.338 | −0.344 | Age | −0.113 | −0.015 |
| Sex | −0.198 | −0.224 | Sex | −0.089 | −0.132 |
| Fall history | −0.056 | −0.063 | Fall history | −0.191 | −0.277 |
| Education level | 0.168 | 0.192 | Education level | 0.113 | 0.167 |
| Hypertension | −0.037 | −0.042 | Hypertension | 0.019 | 0.028 |
| Diabetes mellitus | 0.001 | 0.001 | Diabetes mellitus | 0.197 | 0.291 |
| Cardiovascular disease | −0.286 | −0.328 | Cardiovascular disease | −0.020 | −0.029 |
| MMSE | 0.176 | 0.188 | Speed | 0.068 | 0.080 |
| Forward digits | 0.497 | Turn-to-walk | −0.735 | ||
| Backward digits | 0.049 | 0.047 | Turn-to-sit | −0.021 | −0.014 |
| Trail making test B | −0.115 | −0.127 | Sit-to-stand | −0.136 | −0.173 |
| Speed | 0.268 | 0.297 | R square | 0.541 | |
| Stride Length | 0.389 | 0.443 | Adjusted R square | 0.525 | |
| Cadence step | −0.047 | −0.052 | p value | <0.001 | |
| Tinetti Posture | 0.071 | 0.081 | |||
| R square | 0.247 | ||||
| Adjusted R square | 0.223 | ||||
| p value | 0.003 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, P.-H.; Yang, Y.-Y.; Liao, Y.-Y.; Cheng, S.-J.; Wang, P.-N.; Cheng, F.-Y. Factors Associated with Fear of Falling in Individuals with Different Types of Mild Cognitive Impairment. Brain Sci. 2022, 12, 990. https://doi.org/10.3390/brainsci12080990
Chen P-H, Yang Y-Y, Liao Y-Y, Cheng S-J, Wang P-N, Cheng F-Y. Factors Associated with Fear of Falling in Individuals with Different Types of Mild Cognitive Impairment. Brain Sciences. 2022; 12(8):990. https://doi.org/10.3390/brainsci12080990
Chicago/Turabian StyleChen, Pei-Hao, Ya-Yuan Yang, Ying-Yi Liao, Shih-Jung Cheng, Pei-Ning Wang, and Fang-Yu Cheng. 2022. "Factors Associated with Fear of Falling in Individuals with Different Types of Mild Cognitive Impairment" Brain Sciences 12, no. 8: 990. https://doi.org/10.3390/brainsci12080990