
Application of Network Analysis to Uncover Variables Contributing to Functional Recovery after Stroke

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Statistical Analysis
2.3.1. Estimating Networks
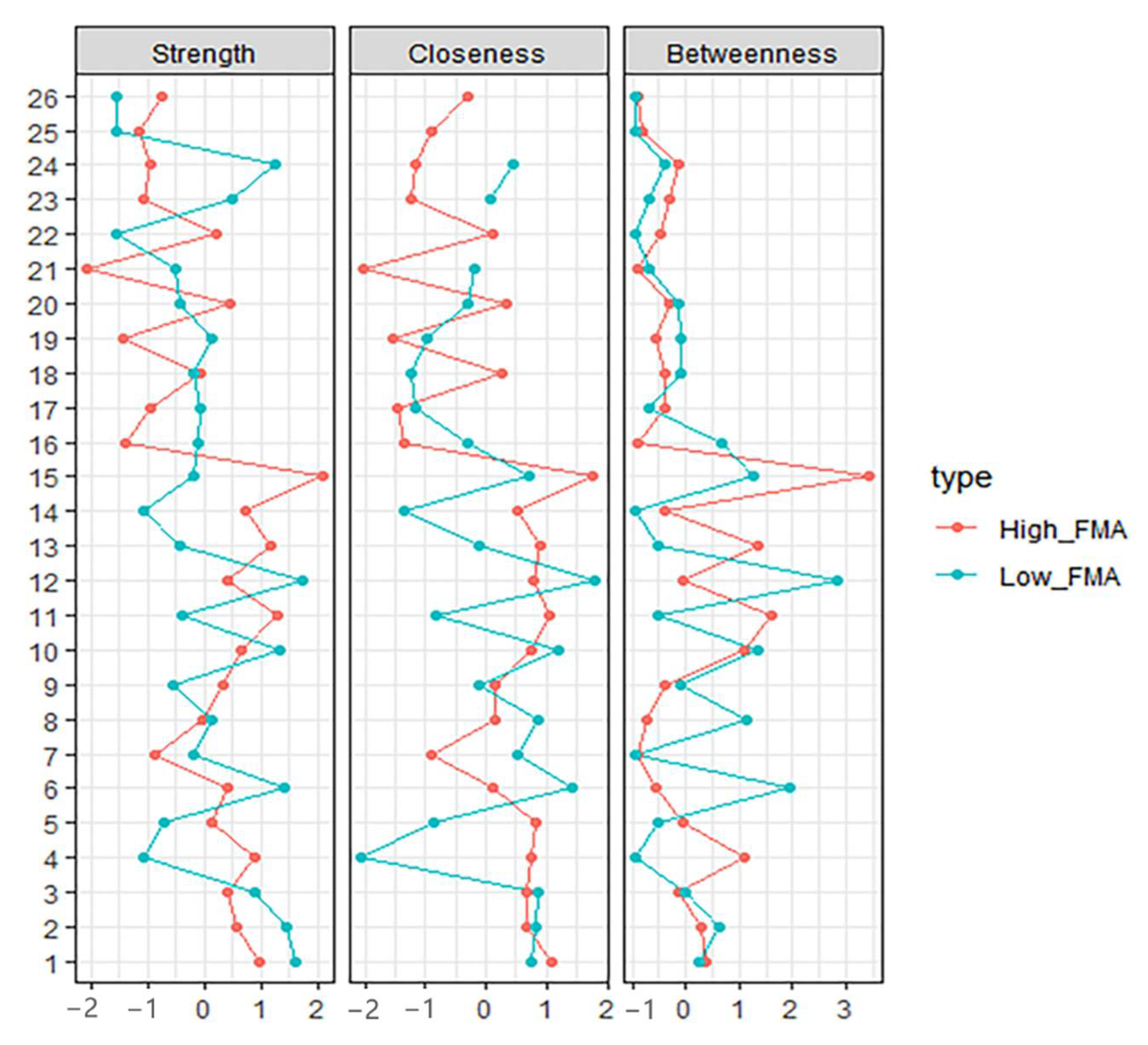
2.3.2. Computing Centrality Indices
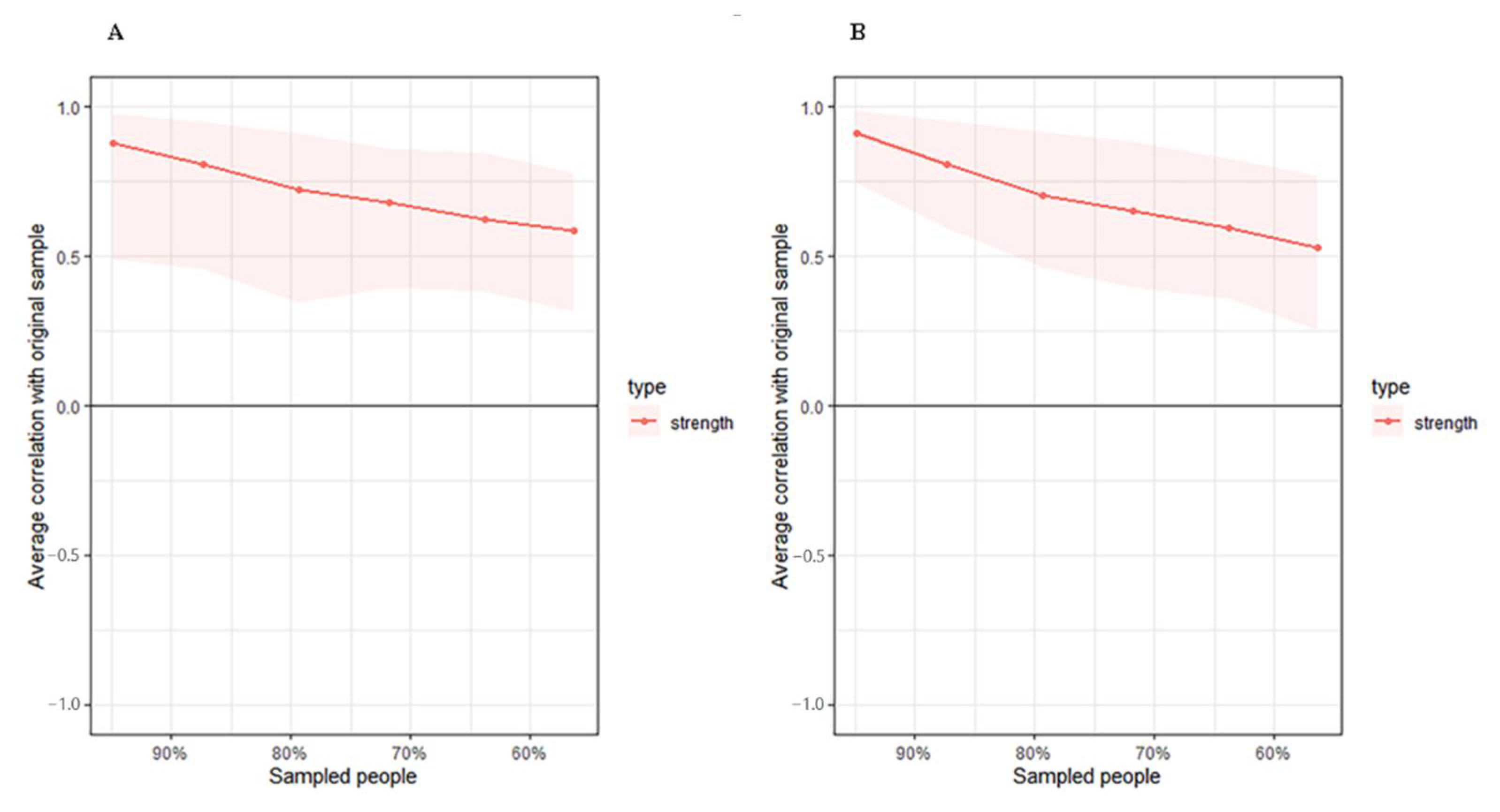
2.3.3. Accuracy Test
2.3.4. Network Comparison
3. Results
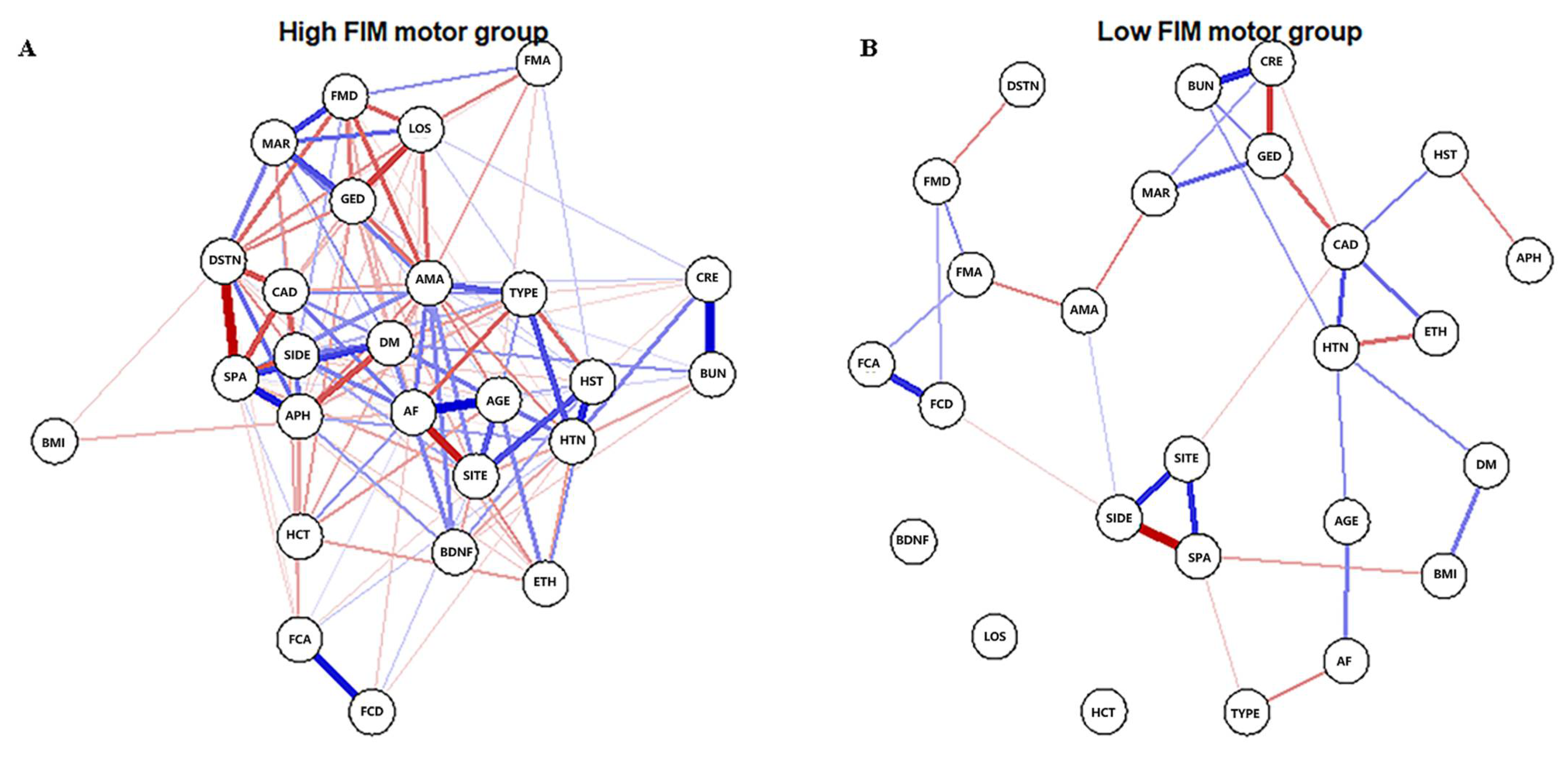
3.1. High-FIM Network
3.2. Low-FIM Network
3.3. Network Comparison
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-Adjusted Life Years (DALYs) for 291 Diseases and Injuries in 21 Regions, 1990–2010: A Systematic Analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Ali, S.F.; Siddiqui, K.; Ay, H.; Silverman, S.; Singhal, A.; Viswanathan, A.; Rost, N.; Lev, M.; Schwamm, L.H. Baseline Predictors of Poor Outcome in Patients Too Good to Treat With Intravenous Thrombolysis. Stroke 2016, 47, 2986–2992. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.; Middleton, S.; Wilson, P.H.; Johnstone, S.J. Predicting Functional Outcomes after Stroke: An Observational Study of Acute Single-Channel EEG. Top. Stroke Rehabil. 2020, 27, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yuan, Z.; Ji, J.; Li, H.; Xue, F. Network or Regression-Based Methods for Disease Discrimination: A Comparison Study. BMC Med. Res. Methodol. 2016, 16, 100. [Google Scholar] [CrossRef]
- Zhou, X.; Zhang, Z.; Liang, X. Regulatory Network Analysis to Reveal Important MiRNAs and Genes in Non-Small Cell Lung Cancer. Cell J. 2020, 21, 459–466. [Google Scholar] [CrossRef]
- Bortolon, C.; Raffard, S. [Network analyses: Are we moving toward a new conceptualization and treatment of mental disorder?]. L’encephale 2019, 45, 433–440. [Google Scholar] [CrossRef]
- Strauss, G.P.; Esfahlani, F.Z.; Kirkpatrick, B.; Allen, D.N.; Gold, J.M.; Visser, K.F.; Sayama, H. Network Analysis Reveals Which Negative Symptom Domains Are Most Central in Schizophrenia vs. Bipolar Disorder. Schizophr. Bull. 2019, 45, 1319–1330. [Google Scholar] [CrossRef]
- Bryant, R.A.; Creamer, M.; O’Donnell, M.; Forbes, D.; McFarlane, A.C.; Silove, D.; Hadzi-Pavlovic, D. Acute and Chronic Posttraumatic Stress Symptoms in the Emergence of Posttraumatic Stress Disorder: A Network Analysis. JAMA Psychiatry 2017, 74, 135–142. [Google Scholar] [CrossRef]
- Ortega Díaz, A.; Gutiérrez, E.C. Competing Actors in the Climate Change Arena in Mexico: A Network Analysis. J. Environ. Manag. 2018, 215, 239–247. [Google Scholar] [CrossRef]
- DuBois, R.H.; Rodgers, R.F.; Franko, D.L.; Eddy, K.T.; Thomas, J.J. A Network Analysis Investigation of the Cognitive-Behavioral Theory of Eating Disorders. Behav. Res. Ther. 2017, 97, 213–221. [Google Scholar] [CrossRef]
- Dalege, J.; Borsboom, D.; van Harreveld, F.; van der Maas, H.L.J. Network Analysis on Attitudes: A Brief Tutorial. Soc. Psychol. Personal. Sci. 2017, 8, 528–537. [Google Scholar] [CrossRef]
- Hartung, T.J.; Fried, E.I.; Mehnert, A.; Hinz, A.; Vehling, S. Frequency and Network Analysis of Depressive Symptoms in Patients with Cancer Compared to the General Population. J. Affect. Disord. 2019, 256, 295–301. [Google Scholar] [CrossRef]
- Luo, W.; Liu, T.; Li, S.; Wen, H.; Zhou, F.; Zafonte, R.; Luo, X.; Xu, M.; Black-Schaffer, R.; Wood, L.J.; et al. The Serum BDNF Level Offers Minimum Predictive Value for Motor Function Recovery After Stroke. Transl. Stroke Res. 2019, 10, 342–351. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating Psychological Networks and Their Accuracy: A Tutorial Paper. Behav. Res. Methods 2018, 50, 195–212. [Google Scholar] [CrossRef]
- Robinaugh, D.J.; Millner, A.J.; McNally, R.J. Identifying Highly Influential Nodes in the Complicated Grief Network. J. Abnorm. Psychol. 2016, 125, 747–757. [Google Scholar] [CrossRef]
- Hevey, D. Network Analysis: A Brief Overview and Tutorial. Health Psychol. Behav. Med. 2018, 6, 301–328. [Google Scholar] [CrossRef]
- van Borkulo, C.D.; van Bork, R.; Boschloo, L.; Kossakowski, J.J.; Tio, P.; Schoevers, R.A.; Borsboom, D.; Waldorp, L.J. Comparing Network Structures on Three Aspects: A Permutation Test. Psychol. Methods 2022. [Google Scholar] [CrossRef]
- Spritzer, S.D.; Kinney, C.L.; Condie, J.; Wellik, K.E.; Hoffman-Snyder, C.R.; Wingerchuk, D.M.; Demaerschalk, B.M. Amantadine for Patients with Severe Traumatic Brain Injury: A Critically Appraised Topic. Neurologist 2015, 19, 61–64. [Google Scholar] [CrossRef]
- Ghate, P.S.; Bhanage, A.; Sarkar, H.; Katkar, A. Efficacy of Amantadine in Improving Cognitive Dysfunction in Adults with Severe Traumatic Brain Injury in Indian Population: A Pilot Study. Asian J. Neurosurg. 2018, 13, 647–650. [Google Scholar] [CrossRef]
- Giacino, J.T.; Whyte, J.; Bagiella, E.; Kalmar, K.; Childs, N.; Khademi, A.; Eifert, B.; Long, D.; Katz, D.I.; Cho, S.; et al. Placebo-Controlled Trial of Amantadine for Severe Traumatic Brain Injury. N. Engl. J. Med. 2012, 366, 819–826. [Google Scholar] [CrossRef]
- Lehnerer, S.M.; Scheibe, F.; Buchert, R.; Kliesch, S.; Meisel, A. Awakening with Amantadine from a Persistent Vegetative State after Subarachnoid Haemorrhage. BMJ Case Rep. 2017, 2017, bcr-2017-220305. [Google Scholar] [CrossRef] [PubMed]
- Khasanova, D.R.; Saĭkhunov, M.V.; Kitaeva, E.A.; Khafiz’ianova, R.K.; Islaamov, R.R.; Demin, T.V. [Amantadine sulfate (PK-Merz) in the treatment of ischemic stroke: A clinical-experimental study]. Zhurnal Nevrol. I Psikhiatrii Im. SS Korsakova 2009, 109, 37–43. [Google Scholar]
- Kim, J.-H.; Lee, H.-W.; Hwang, J.; Kim, J.; Lee, M.-J.; Han, H.-S.; Lee, W.-H.; Suk, K. Microglia-Inhibiting Activity of Parkinson’s Disease Drug Amantadine. Neurobiol. Aging 2012, 33, 2145–2159. [Google Scholar] [CrossRef]
- Suwa, M.; Kishimoto, H.; Nofuji, Y.; Nakano, H.; Sasaki, H.; Radak, Z.; Kumagai, S. Serum Brain-Derived Neurotrophic Factor Level Is Increased and Associated with Obesity in Newly Diagnosed Female Patients with Type 2 Diabetes Mellitus. Metabolism 2006, 55, 852–857. [Google Scholar] [CrossRef]
- Boyuk, B.; Degirmencioglu, S.; Atalay, H.; Guzel, S.; Acar, A.; Celebi, A.; Ekizoglu, I.; Simsek, C. Relationship between Levels of Brain-Derived Neurotrophic Factor and Metabolic Parameters in Patients with Type 2 Diabetes Mellitus. J. Diabetes Res. 2014, 2014, 978143. [Google Scholar] [CrossRef]
- Fujinami, A.; Ohta, K.; Obayashi, H.; Fukui, M.; Hasegawa, G.; Nakamura, N.; Kozai, H.; Imai, S.; Ohta, M. Serum Brain-Derived Neurotrophic Factor in Patients with Type 2 Diabetes Mellitus: Relationship to Glucose Metabolism and Biomarkers of Insulin Resistance. Clin. Biochem. 2008, 41, 812–817. [Google Scholar] [CrossRef]
- Lambert, G.W.; Schlaich, M.P.; Esler, M.D. Brain Derived Neurotrophic Factor (BDNF) Release from the Human Brain in Patients with Type 2 Diabetes--Possible Influence of Venous Anatomy and Comorbid Major Depressive Disorder. Diabetologia 2007, 50, 2027–2028. [Google Scholar] [CrossRef]
- Pivac, N.; Kim, B.; Nedić, G.; Joo, Y.H.; Kozarić-Kovacić, D.; Hong, J.P.; Muck-Seler, D. Ethnic Differences in Brain-Derived Neurotrophic Factor Val66Met Polymorphism in Croatian and Korean Healthy Participants. Croat. Med. J. 2009, 50, 43–48. [Google Scholar] [CrossRef]
- Boyne, P.; Meyrose, C.; Westover, J.; Whitesel, D.; Hatter, K.; Reisman, D.S.; Cunningham, D.; Carl, D.; Jansen, C.; Khoury, J.C.; et al. Exercise Intensity Affects Acute Neurotrophic and Neurophysiological Responses Poststroke. J. Appl. Physiol. 2019, 126, 431–443. [Google Scholar] [CrossRef]
- Stranahan, A.M.; Lee, K.; Martin, B.; Maudsley, S.; Golden, E.; Cutler, R.G.; Mattson, M.P. Voluntary Exercise and Caloric Restriction Enhance Hippocampal Dendritic Spine Density and BDNF Levels in Diabetic Mice. Hippocampus 2009, 19, 951–961. [Google Scholar] [CrossRef] [PubMed]
- Duan, W.; Guo, Z.; Jiang, H.; Ware, M.; Mattson, M.P. Reversal of Behavioral and Metabolic Abnormalities, and Insulin Resistance Syndrome, by Dietary Restriction in Mice Deficient in Brain-Derived Neurotrophic Factor. Endocrinology 2003, 144, 2446–2453. [Google Scholar] [CrossRef]
- Unger, T.J.; Calderon, G.A.; Bradley, L.C.; Sena-Esteves, M.; Rios, M. Selective Deletion of Bdnf in the Ventromedial and Dorsomedial Hypothalamus of Adult Mice Results in Hyperphagic Behavior and Obesity. J. Neurosci. 2007, 27, 14265–14274. [Google Scholar] [CrossRef] [PubMed]
- Bus, B.A.A.; Molendijk, M.L.; Penninx, B.J.W.H.; Buitelaar, J.K.; Kenis, G.; Prickaerts, J.; Elzinga, B.M.; Voshaar, R.C.O. Determinants of Serum Brain-Derived Neurotrophic Factor. Psychoneuroendocrinology 2011, 36, 228–239. [Google Scholar] [CrossRef] [PubMed]
- Kowiański, P.; Lietzau, G.; Czuba, E.; Waśkow, M.; Steliga, A.; Moryś, J. BDNF: A Key Factor with Multipotent Impact on Brain Signaling and Synaptic Plasticity. Cell. Mol. Neurobiol. 2018, 38, 579–593. [Google Scholar] [CrossRef]
- Chang, K.-C.; Tseng, M.-C.; Weng, H.-H.; Lin, Y.-H.; Liou, C.-W.; Tan, T.-Y. Prediction of Length of Stay of First-Ever Ischemic Stroke. Stroke 2002, 33, 2670–2674. [Google Scholar] [CrossRef]
- Svendsen, M.L.; Ehlers, L.H.; Andersen, G.; Johnsen, S.P. Quality of Care and Length of Hospital Stay among Patients with Stroke. Med. Care 2009, 47, 575–582. [Google Scholar] [CrossRef]
- Cha, E.; Kim, S.-Y.; Lee, H.; Kim, D.; Lee, J.; Sohn, M.; LEE, S.-G.; Oh, G.-J.; Lee, Y.-S.; Joo, M.C.; et al. Prevalence Rate of Spasticity at 3 Months after Stroke in Korea: The Korean Stroke Cohort for Functioning and Rehabilitation (KOSCO) Study. Brain Neurorehabil. 2016, 9, e6. [Google Scholar] [CrossRef]
- Lundström, E.; Terént, A.; Borg, J. Prevalence of Disabling Spasticity 1 Year after First-Ever Stroke. Eur. J. Neurol. 2008, 15, 533–539. [Google Scholar] [CrossRef]
- Ryu, J.S.; Lee, J.W.; Lee, S.I.; Chun, M.H. Factors Predictive of Spasticity and Their Effects on Motor Recovery and Functional Outcomes in Stroke Patients. Top. Stroke Rehabil. 2010, 17, 380–388. [Google Scholar] [CrossRef]
- Li, S. Spasticity, Motor Recovery, and Neural Plasticity after Stroke. Front. Neurol. 2017, 8, 120. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.S.; Ruiz, J.; Hawkins, K.; Wicker, E. The Impact of Mobility Limitations on Health Outcomes among Older Adults. Geriatr. Nurs. 2018, 39, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Borsboom, D.; Cramer, A.O.J. Network Analysis: An Integrative Approach to the Structure of Psychopathology. Annu. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef] [PubMed]
- Beard, C.; Millner, A.J.; Forgeard, M.J.C.; Fried, E.I.; Hsu, K.J.; Treadway, M.T.; Leonard, C.V.; Kertz, S.J.; Björgvinsson, T. Network Analysis of Depression and Anxiety Symptom Relationships in a Psychiatric Sample. Psychol. Med. 2016, 46, 3359–3369. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S. Brief Report on Estimating Regularized Gaussian Networks from Continuous and Ordinal Data. arXiv 2017, arXiv:1606.05771v2. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| ID | Variable | Abbreviation |
|---|---|---|
| 1 | Spasticity (non-spastic vs spastic) | SPA |
| 2 | Stroke side (right side vs left side vs both sides) | SIDE |
| 3 | Stroke site (supratentorial vs infratentorial vs both sites) | SITE |
| 4 | Discharge destination (home vs skilled nursing facility vs acute hospital) | DSTN |
| 5 | Stroke type (ischemic stroke vs hemorrhage stroke) | TYPE |
| 6 | Gender | GED |
| 7 | Ethnicity (Hispanic vs non-Hispanic) | ETH |
| 8 | Marriage (married vs unmarried) | MAR |
| 9 | Prior stroke history | HST |
| 10 | Hypertension | HTN |
| 11 | Atrial fibrillation (AF) | AF |
| 12 | Coronary artery disease (CAD) | CAD |
| 13 | Diabetes mellitus (DM) | DM |
| 14 | Aphasia | APH |
| 15 | Amantadine | AMA |
| 16 | FIM motor subscores on admission (FMA) | FMA |
| 17 | FIM cognitive subscores on admission (FCA) | FCA |
| 18 | FIM motor subscores at discharge (FMD) | FMD |
| 19 | FIM cognitive subscores at discharge (FCD) | FCD |
| 20 | Age | AGE |
| 21 | Body mass index (BMI) | BMI |
| 22 | Length of stay (LOS) | LOS |
| 23 | Blood urea nitrogen (BUN) | BUN |
| 24 | Creatinine | CRE |
| 25 | Hematocrit (HCT) | HCT |
| 26 | brain-derived neurotrophic factor (BDNF) | BDNF |
| ID | Variables | High Motor Function | Low Motor Function | ||||
|---|---|---|---|---|---|---|---|
| Betweenness | Closeness | Strength | Betweenness | Closeness | Strength | ||
| 1 | Spasticity | 0.36 | 1.07 | 0.98 | 0.26 | 0.75 | 1.60 |
| 2 | Stroke side | 0.28 | 0.65 | −0.58 | 0.62 | 0.83 | 1.44 |
| 3 | Stroke site | −0.14 | 0.68 | 0.40 | −0.02 | 0.87 | 0.89 |
| 4 | Destination | 1.11 | 0.75 | 0.88 | −0.93 | −2.05 | −1.06 |
| 5 | Stroke type | −0.06 | 0.84 | 0.15 | −0.54 | −0.87 | −0.69 |
| 6 | Gender | −0.56 | 0.10 | 0.41 | 1.93 | 1.43 | 1.40 |
| 7 | Ethnicity | −0.98 | −0.91 | −0.86 | −0.93 | 0.51 | −0.18 |
| 8 | Marriage | −0.72 | 0.17 | −0.03 | 1.14 | 0.86 | 0.13 |
| 9 | Stroke history | −0.39 | 0.13 | 0.31 | −0.10 | −0.10 | −0.54 |
| 10 | Hypertension | 1.11 | 0.76 | 0.66 | 1.33 | 1.20 | 1.35 |
| 11 | AF | 1.61 | 1.05 | 1.29 | −0.50 | −0.81 | −0.38 |
| 12 | CAD | −0.06 | 0.78 | 0.42 | 2.85 § | 1.81 § | 1.74 § |
| 13 | Diabetes | 1.36 | 0.89 | 1.18 | −0.50 | −0.12 | −0.42 |
| 14 | Aphasia | −0.39 | 0.54 | 0.71 | −0.93 | −1.35 | −1.05 |
| 15 | Amantadine | 3.44 § | 1.75 § | 2.07 § | 1.25 | 0.70 | −0.18 |
| 16 | FMA | −0.98 | −1.36 | −1.39 | 0.66 | −0.31 | −0.10 |
| 17 | FCA | −0.39 | −1.46 | −0.96 | −0.69 | −1.18 | −0.07 |
| 18 | FMD | −0.39 | 0.28 | −0.05 | −0.10 | −1.23 | −0.20 |
| 19 | FCD | −0.56 | −1.54 | −1.42 | −0.10 | −0.97 | 0.13 |
| 20 | Age | −0.31 | 0.34 | 0.44 | −0.14 | −0.31 | −0.42 |
| 21 | BMI | −0.89 | −2.01 | −2.06 | −0.69 | −0.18 | −0.51 |
| 22 | LOS | −0.47 | 0.10 | 0.22 | −0.93 | NA † | −1.53 |
| 23 | BUN | −0.31 | −1.25 | −1.08 | −0.69 | 0.08 | 0.48 |
| 24 | Creatinine | −0.14 | −1.16 | −0.95 | −0.38 | 0.44 | 1.25 |
| 25 | HCT | −0.81 | −0.89 | −1.13 | −0.93 | NA † | −1.53 |
| 26 | BDNF | −0.89 | −0.29 | −0.76 | −0.93 | NA † | −1.53 |
| Correlation Represented by the Edge of Two Variables | p Value |
|---|---|
| FMA-Marriage | <0.001 |
| FMD-LOS | <0.001 |
| FMD-Gender | <0.001 |
| Marriage-LOS | 0.001 |
| Gender-LOS | 0.003 |
| Amantadine-LOS | 0.011 |
| Age-HCT | 0.015 |
| Destination-AF | 0.023 |
| Spasticity-Aphasia | 0.027 |
| Stroke Site-Age | 0.027 |
| Spasticity-Destination | 0.028 |
| Amantadine-FMD | 0.031 |
| Stroke Site-Stroke History | 0.033 |
| Stroke History-Hypertension | 0.033 |
| Spasticity-Stroke Site | 0.034 |
| Destination-Aphasia | 0.035 |
| AF-Age | 0.04 |
| Destination-LOS | 0.04 |
| AF-HCT | 0.042 |
| Marriage-Amantadine | 0.044 |
| DM-Aphasia | 0.045 |
| Stroke Type-Hypertension | 0.046 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xi, X.; Li, Q.; Wood, L.J.; Bose, E.; Zeng, X.; Wang, J.; Luo, X.; Wang, Q.M. Application of Network Analysis to Uncover Variables Contributing to Functional Recovery after Stroke. Brain Sci. 2022, 12, 1065. https://doi.org/10.3390/brainsci12081065
Xi X, Li Q, Wood LJ, Bose E, Zeng X, Wang J, Luo X, Wang QM. Application of Network Analysis to Uncover Variables Contributing to Functional Recovery after Stroke. Brain Sciences. 2022; 12(8):1065. https://doi.org/10.3390/brainsci12081065
Chicago/Turabian StyleXi, Xiao, Qianfeng Li, Lisa J. Wood, Eliezer Bose, Xi Zeng, Jun Wang, Xun Luo, and Qing Mei Wang. 2022. "Application of Network Analysis to Uncover Variables Contributing to Functional Recovery after Stroke" Brain Sciences 12, no. 8: 1065. https://doi.org/10.3390/brainsci12081065