
Psychosocial Interventions for Attention Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis by the CADDRA Guidelines Work GROUP



Abstract
:1. Introduction
1.1. Etiologies of ADHD
1.2. Pharmacological Treatment of ADHD
1.3. Psychosocial Interventions for ADHD
1.4. Present Study
2. Methods
2.1. Eligibility Criteria
2.2. Information Source
2.3. Search Strategy
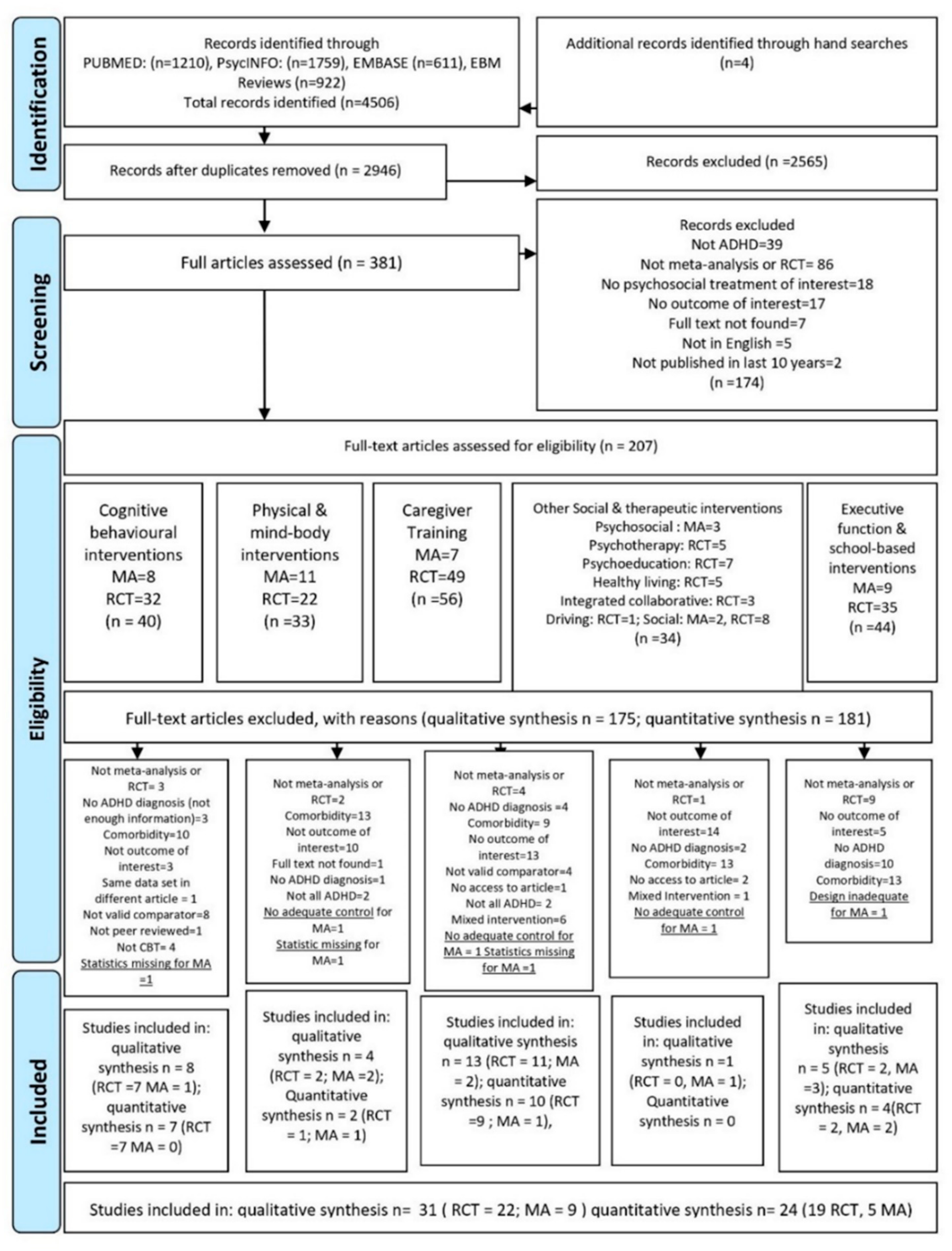
2.4. Selection Process
- Cognitive-behavioral therapy;
- Caregiver (parent) training;
- Metacognitive or school based (i.e., teacher training) interventions;
- Physical exercise or mind–body interventions;
- Other psychosocial interventions
2.5. Data Items
2.6. Study Risk of Bias
2.7. Effect Measures
2.8. Synthesis Methods
2.9. Risk of Bias across Studies
2.10. Certainty and Recommendation
3. Results
3.1. Study Characteristics and Qualitative Summary
3.2. Individual Study Bias
3.3. Three-Level Meta-Analyses Results
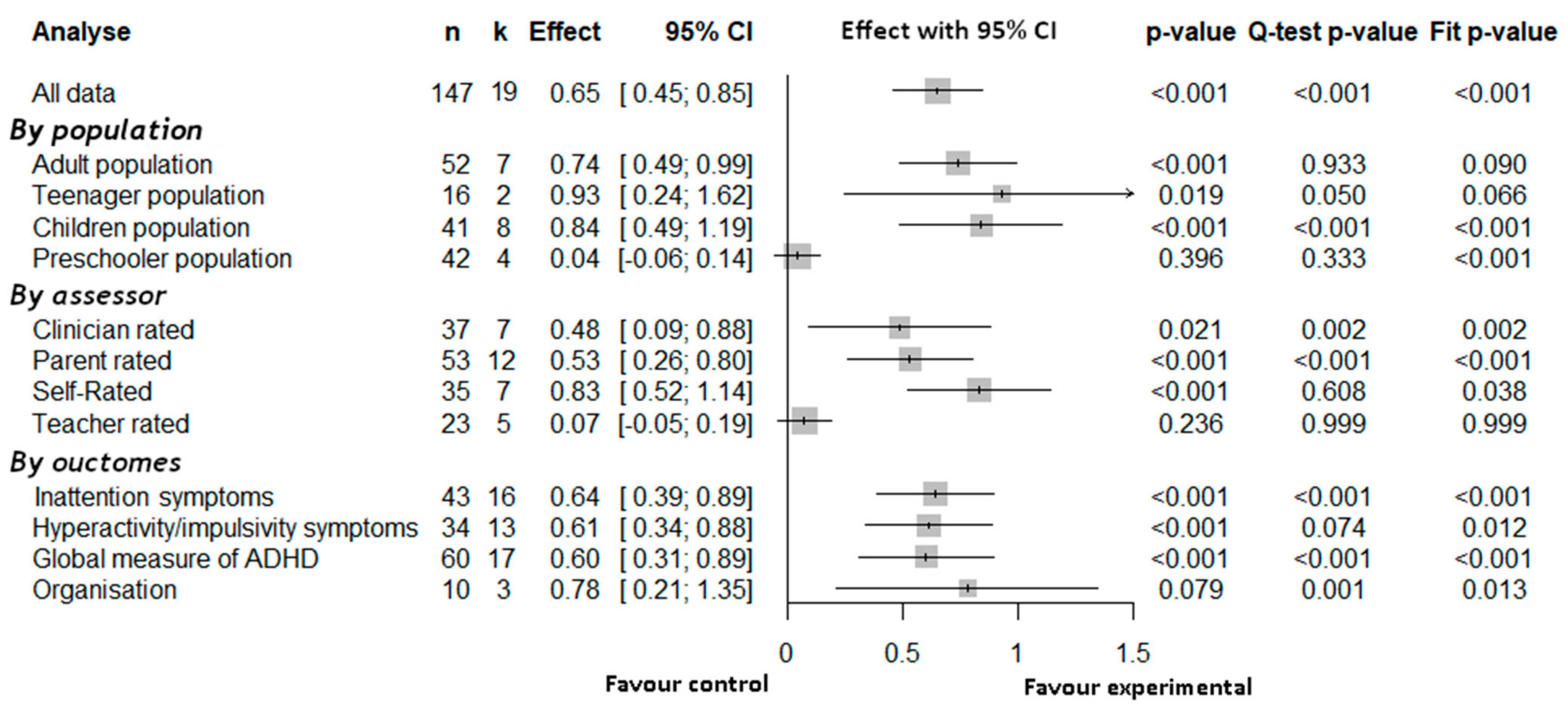
3.3.1. Overall Three-Level Meta-Analyses Results
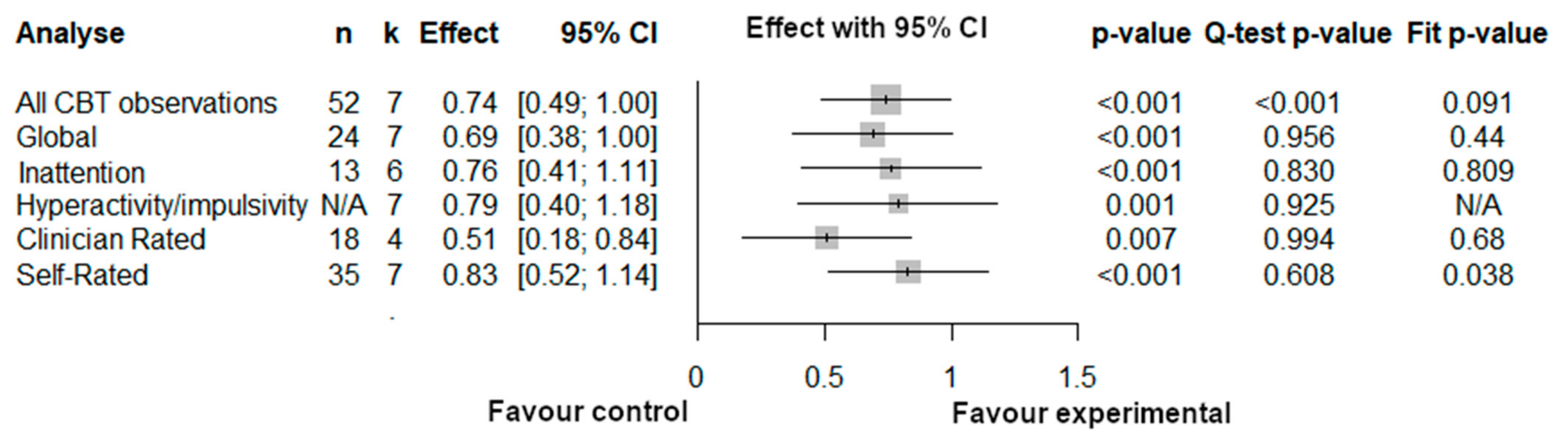
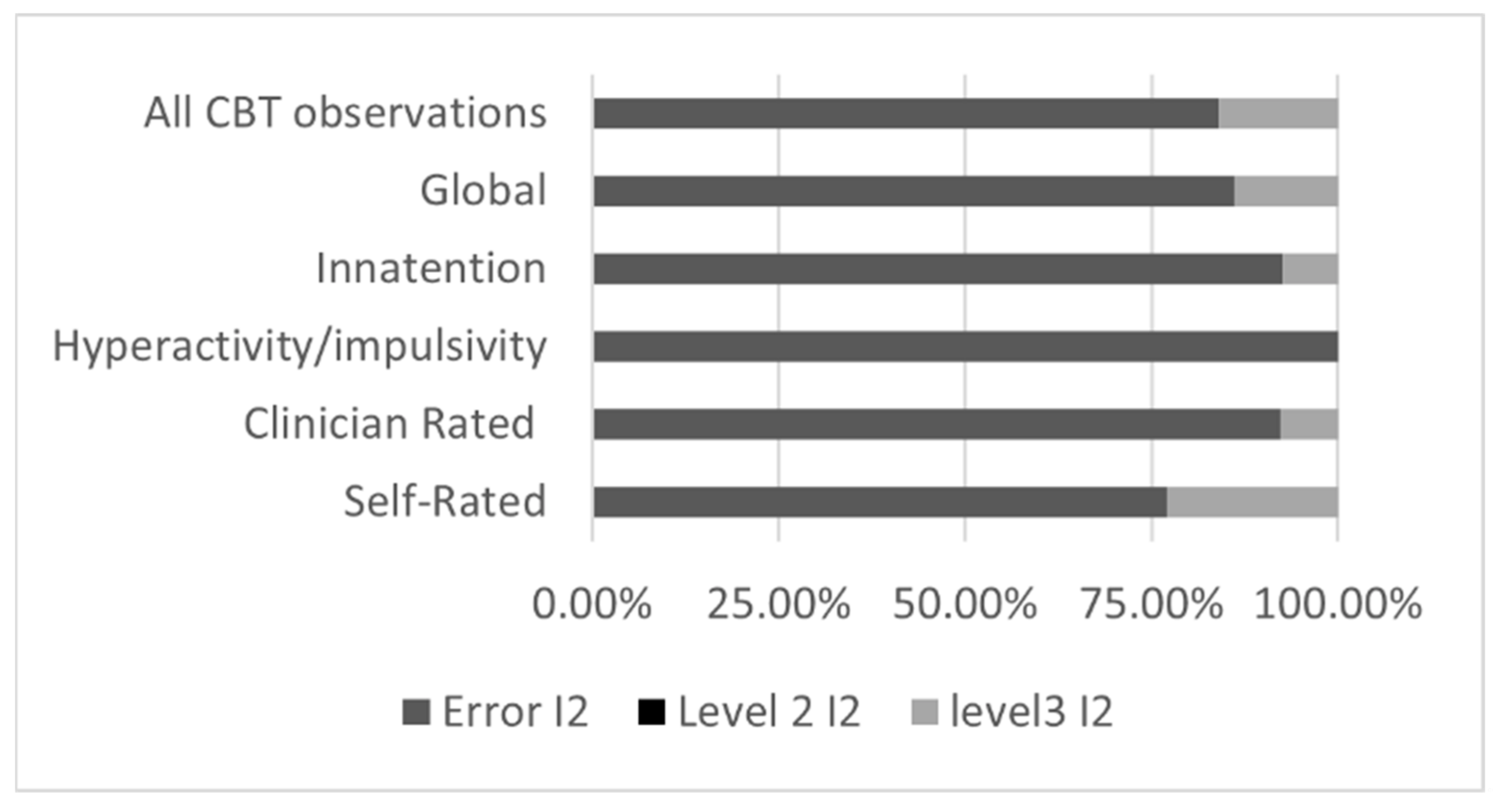
3.3.2. Three-Level Meta-Analyses Results for Cognitive Behavioral Therapy
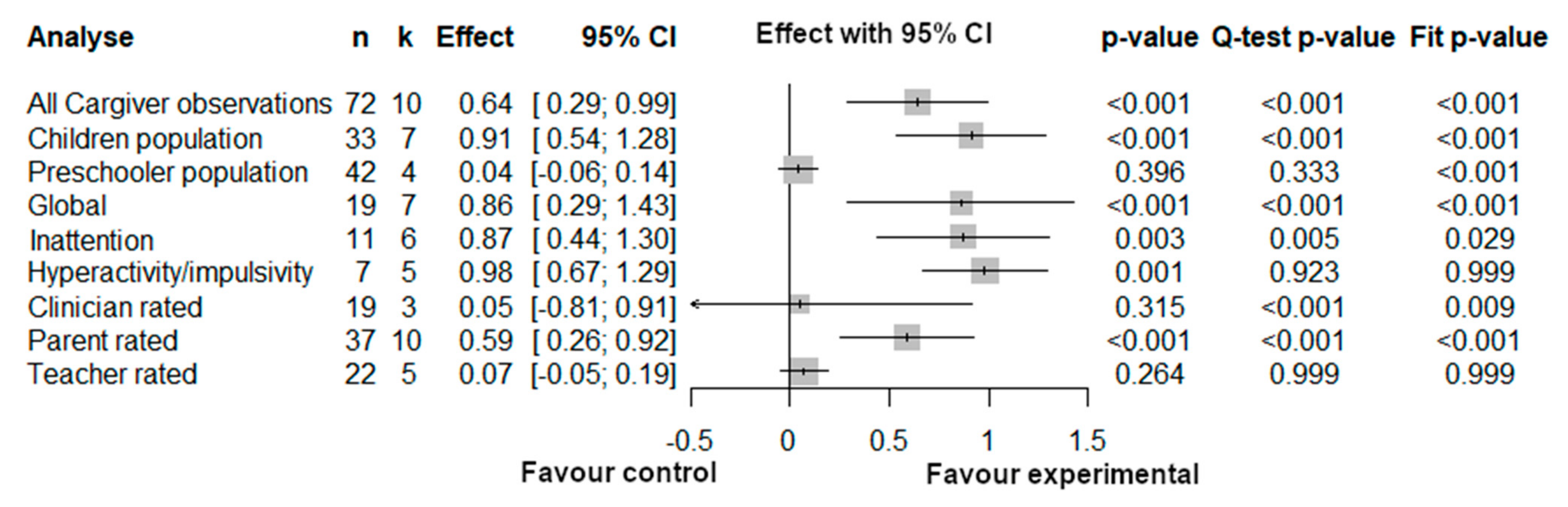
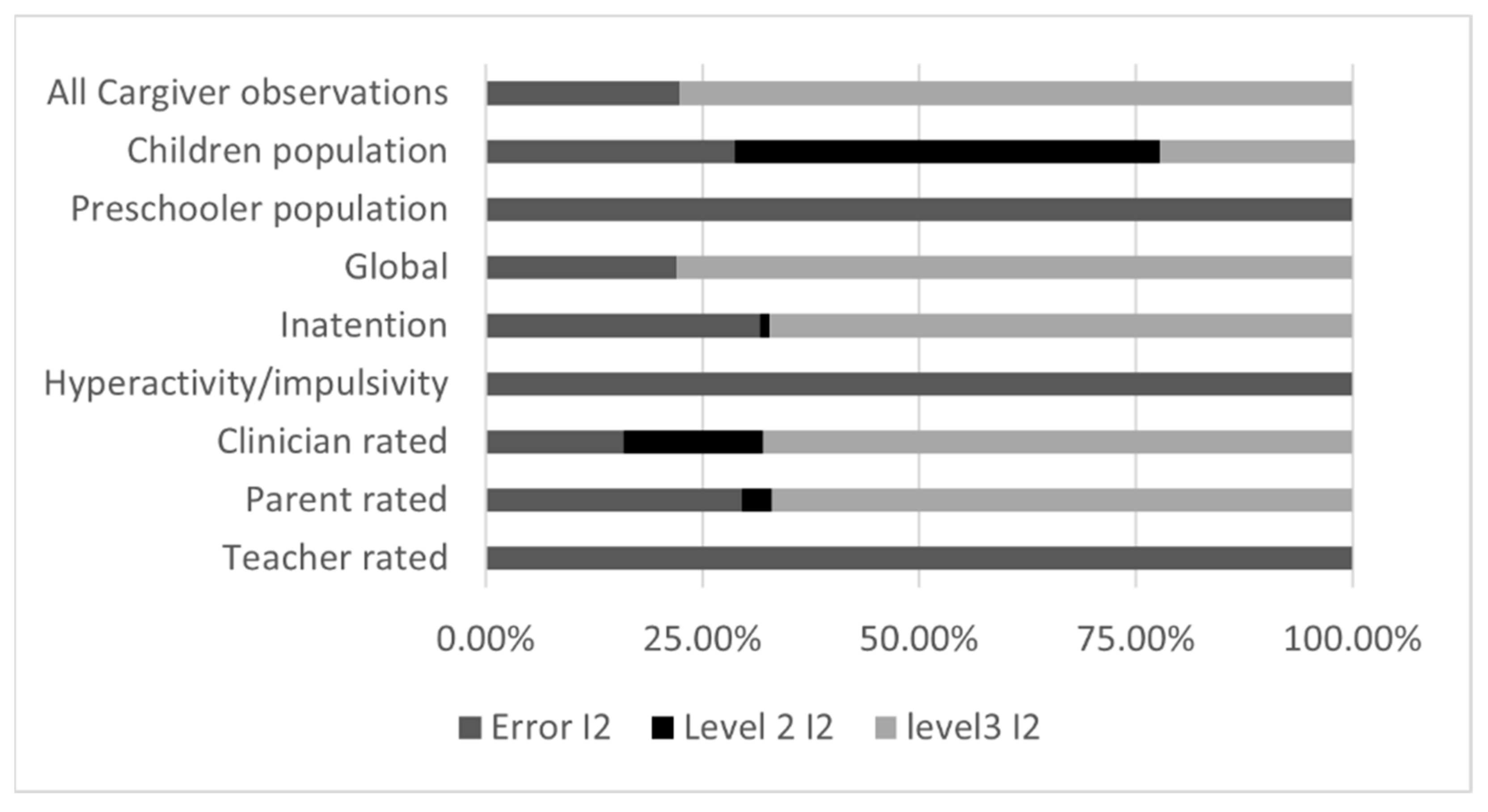
3.3.3. Three-Level Meta-Analyses Results for Caregiver Intervention
3.3.4. Three-Level Meta-Analyses Results for School Based and Executive Intervention
3.4. Attrition and Adverse Effects
3.5. Meta-Regression
3.6. Publication Bias
3.7. Four-Levels Meta-Analysis
3.8. Certainty of Assessment and Recommendation
4. Discussion
4.1. Psychosocial Intervention for ADHD: Which One and for Whom?
- We recommend Cognitive Behavioral Therapy for reducing global, inattention and hyperactivity/impulsivity symptoms of ADHD for adults. Our confidence in the efficacity of this intervention is moderate;
- We recommend caregiver interventions for reducing inattention and hyperactivity/impulsivity symptoms of ADHD of school age children. Our confidence in the efficacity of this intervention is low;
- We recommend caregiver interventions for reducing inattention and hyperactivity/impulsivity symptoms of ADHD of school age children. Our confidence in the efficacity of this intervention is very low;
- We recommend School based or Executive interventions for reducing inattention and hyperactivity/impulsivity symptoms of ADHD of school age children. Our confidence in the efficacity of this intervention is very low;
- We do not recommend caregiver interventions for reducing inattention and hyperactivity/impulsivity symptoms of ADHD of preschoolers. Our confidence in the lack of efficacity of this intervention is low;
- No recommendation can be formulated for other interventions, populations, and outcomes (e.g., disorganization symptoms)
4.2. Limitations of the Present Review
4.3. Future Research
- Implement robust randomization procedures, including proper concealment of the allocation sequence [137];
- Assure that all assessment personnel and participants are blinded. While a double blind paradigm may be difficult to implement in the context of psychosocial intervention, it is possible to design active control group that mimics some aspect of the intervention group, thus creating a credible alternative to the active intervention. This design is referred to as “dual blind” and has been used in other psychosocial research, such as mindfulness-based intervention [138];
- Preregister the study protocol, so that reporting bias may be correctly assessed [139].
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; DSM-5 Diagnostic Classification; American Psychiatric Association, American Psychiatric Publishing Inc.: Washington, DC, USA, 2013; Volume 10. [Google Scholar]
- World Health Organization. Internațional Classification of Diseases; 11th Revision; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Willcutt, E.G.; Nigg, J.T.; Pennington, B.F.; Solanto, M.V.; Rohde, L.A.; Tannock, R.; Loo, S.K.; Carlson, C.L.; McBurnett, K.; Lahey, B.B. Validity of DSM-IV Attention Deficit/Hyperactivity Disorder Symptom Dimensions and Subtypes. J. Abnorm. Psychol. 2012, 121, 991–1010. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Yang, H.-J.; Chen, V.C.-H.; Lee, W.-T.; Teng, M.-J.; Lin, C.-H.; Gossop, M. Meta-analysis of Quality of Life in Children and Adolescents with ADHD: By Both Parent Proxy-report and Child Self-report Using PedsQL™. Res. Dev. Disabil. 2016, 51, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Lansford, J.; Dodge, K.; Pettit, G.; Bates, J. A Public Health Perspective on School Dropout and Adult Outcomes: A Prospective Study of Risk and Protective Factors From Age 5 to 27 Years. J. Adolesc. Health 2016, 58, 652–658. [Google Scholar] [CrossRef]
- Breslau, J.; Miller, E.; Chung, W.-J.J.; Schweitzer, J.B. Childhood and Adolescent Onset Psychiatric Disorders, Substance Sse, and Failure to Graduate High School on Time. J. Psychiatr. Res. 2011, 45, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Fleming, M.; Fitton, C.A.; Steiner, M.F.; McLay, J.S.; Clark, D.; King, A.; Lindsay, R.; Mackay, D.F.; Pell, J.P. Educational and Health Outcomes of Children Treated for Attention-Deficit/Hyperactivity Disorder. JAMA Pediatr. 2017, 171, e170691. [Google Scholar] [CrossRef]
- Beheshti, A.; Chavanon, M.-L.; Christiansen, H. Emotion Dysregulation in Adults with Attention Deficit Hyperactivity Disorder: A Meta-analysis. BMC Psychiatry 2020, 20, 120. [Google Scholar] [CrossRef] [PubMed]
- Strine, T.W.; Lesesne, C.A.; Okoro, C.A.; McGuire, L.C.; Chapman, D.P.; Balluz, L.S.; Mokdad, A.H. Peer Reviewed: Emotional and Behavioral Difficulties and Impairments in Everyday Functioning Among Children with a History of Attention-Deficit/Hyperactivity Disorder. Prev. Chronic Dis. 2006, 3, A52. [Google Scholar]
- Ros, R.; Graziano, P.A. Social Functioning in Children with or at Risk for Attention Deficit/Hyperactivity Disorder: A Meta-analytic Review. J. Clin. Child Adolesc. Psychol. 2018, 47, 213–235. [Google Scholar] [CrossRef] [PubMed]
- Turcotte Benedict, F.; Vivier, P.M.; Gjelsvik, A. Mental Health and Bullying in the United States among Children Aged 6 to 17 Years. J. Interpers. Violence 2015, 30, 782–795. [Google Scholar] [CrossRef]
- Mohr-Jensen, C.; Bisgaard, C.M.; Boldsen, S.K.; Steinhausen, H.-C. Attention-Deficit/Hyperactivity Disorder in Childhood and Adolescence and the Risk of Crime in Young Adulthood in a Danish Nationwide Study. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 443–452. [Google Scholar] [CrossRef]
- Liang, S.H.-Y.; Yang, Y.-H.; Kuo, T.-Y.; Liao, Y.-T.; Lin, T.-C.; Lee, Y.; McIntyre, R.S.; Kelsen, B.A.; Wang, T.-N.; Chen, V.C.-H. Suicide Risk Reduction In Youths with Attention-Deficit/Hyperactivity Disorder Prescribed Methylphenidate: A Taiwan Nationwide Population-Based Cohort Study. Res. Dev. Disabil. 2018, 72, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Banaschewski, T.; Coghill, D.; Zheng, Y.; Biederman, J.; Bellgrove, M.A.; Newcorn, J.H.; Gignac, M.; Al Saud, N.M.; Manor, I.; et al. The World Federation of ADHD International Consensus Statement: 208 Evidence-Based Conclusions About the Disorder. Neurosci. Biobehav. Rev. 2021, 128, 789–818. [Google Scholar] [CrossRef] [PubMed]
- Spencer, T.J.; Biederman, J.; Mick, E. Attention-Deficit/Hyperactivity Disorder: Diagnosis, Lifespan, Comorbidities, and Neurobiology. J. Pediatric Psychol. 2007, 32, 631–642. [Google Scholar] [CrossRef]
- Fayyad, J.; Sampson, N.A.; Hwang, I.; Adamowski, T.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Andrade, L.H.; Borges, G.; de Girolamo, G.; Florescu, S.; et al. The Descriptive Epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. ADHD Atten. Deficit Hyperact. Disord. 2017, 9, 47–65. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Biederman, J.; Mick, E. The Age-Dependent Decline of Attention Deficit Hyperactivity Disorder: A Meta-Analysis of Follow-Up Studies. Psychol. Med. 2006, 36, 159–165. [Google Scholar] [CrossRef]
- Voort, J.L.V.; He, J.-P.; Jameson, N.D.; Merikangas, K.R. Impact of the DSM-5 Attention-Deficit/Hyperactivity Disorder Age-of-Onset Criterion in the US Adolescent Population. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Matte, B.; Anselmi, L.; Salum, G.A.; Kieling, C.; Gonçalves, H.; Menezes, A.; Grevet, E.H.; Rohde, L.A. ADHD in DSM-5: A Field Trial in a Large, Representative Sample of 18- to 19-Year-Old Adults. Psychol. Med. 2015, 45, 361–373. [Google Scholar] [CrossRef]
- Børglum, A.; Neale, B.; Franke, B. Unfolding the genetic basis of adhd. Eur. Neuropsychopharmacol. 2019, 29, S722. [Google Scholar] [CrossRef]
- Demontis, D.; Walters, R.K.; Martin, J.; Mattheisen, M.; Als, T.D.; Agerbo, E.; Baldursson, G.; Belliveau, R.; Bybjerg-Grauholm, J.; Bækvad-Hansen, M.; et al. Discovery of the First Genome-Wide Significant Risk Loci for Attention Deficit/Hyperactivity Disorder. Nat. Genet. 2019, 51, 63–75. [Google Scholar] [CrossRef]
- Faraone, S.; Asherson, P.; Banaschewski, T.; Biederman, J.; Buitelaar, J.; Ramos-Quiroga, J.A.; Rohde, L.A.; Sonuga-Barke, E.J.S.; Tannock, R.; Franke, B. Attention Deficit/Hyperactivity Disorder. Nat. Rev. Dis. Primers 2015, 1, 15020. [Google Scholar] [CrossRef]
- Faraone, S.V.; Larsson, H. Genetics of Attention Deficit Hyperactivity Disorder. Mol. Psychiatry 2019, 24, 562–575. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Mick, E. Molecular Genetics of Attention Deficit Hyperactivity Disorder. Psychiatr. Clin. N. Am. 2010, 33, 159–180. [Google Scholar] [CrossRef]
- Boedhoe, P.S.; Van Rooij, D.; Hoogman, M.; Twisk, J.W.; Schmaal, L.; Abe, Y.; Alonso, P.; van Rooij, D.; Ameis, S.H.; Anikin, A.; et al. Subcortical Brain Volume, Regional Cortical Thickness, and Cortical Surface Area Across Disorders: Findings from the ENIGMA ADHD, ASD, and OCD Working Groups. Am. J. Psychiatry 2020, 177, 834–843. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Hu, X.; Ouyang, L.; He, N.; Liao, Y.; Liu, Q.; Zhou, M.; Wu, M.; Huang, X.; Gong, Q. A Systematic Review and Meta-Analysis of Tract-Based Spatial Statistics Studies Regarding Attention-Deficit/Hyperactivity Disorder. Neurosci. Biobehav. Rev. 2016, 68, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Kelly, C.; Chabernaud, C.; Proal, E.; Di Martino, A.; Milham, M.P.; Castellanos, F.X. Toward Systems Neuroscience of ADHD: A Meta-Analysis of 55 fMRI Studies. Am. J. Psychiatry 2012, 169, 1038–1055. [Google Scholar] [CrossRef] [PubMed]
- Curatolo, P.; D’Agati, E.; Moavero, R. The Neurobiological Basis of ADHD. Ital. J. Pediatr. 2010, 36, 79. [Google Scholar] [CrossRef]
- Hoogman, M.; Bralten, J.; Hibar, D.P.; Mennes, M.; Zwiers, M.P.; Schweren, L.S.; van Hulzen, K.J.E.; Medland, S.E.; Shumskaya, E.; Jahanshad, N.; et al. Subcortical Brain Volume Differences in Participants with Attention Deficit Hyperactivity Disorder in Children and Adults: A Cross-Sectional Mega-Analysis. Lancet Psychiatry 2017, 4, 310–319. [Google Scholar] [CrossRef]
- Hoogman, M.; Muetzel, R.; Guimaraes, J.P.; Shumskaya, E.; Mennes, M.; Zwiers, M.P.; Jahanshad, N.; Sudre, G.; Wolfers, T.; Earl, E.A. Brain Imaging of the Cortex in ADHD: A coordinated analysis of large-scale clinical and population-based samples. Am. J. Psychiatry 2019, 176, 531–542. [Google Scholar] [CrossRef]
- Lukito, S.; Norman, L.; Carlisi, C.; Radua, J.; Hart, H.; Simonoff, E.; Rubia, K. Comparative Meta-Analyses of Brain Structural and Functional Abnormalities During Cognitive Control in Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder. Psychol. Med. 2020, 50, 894–919. [Google Scholar] [CrossRef]
- Norman, L.J.; Carlisi, C.; Lukito, S.; Hart, H.; Mataix-Cols, D.; Radua, J.; Rubia, K. Structural and Functional Brain Abnormalities In Attention-Deficit/Hyperactivity Disorder and Obsessive-Compulsive Disorder: A Comparative Meta-Analysis. JAMA Psychiatry 2016, 73, 815–825. [Google Scholar] [CrossRef]
- Rubia, K. Cognitive Neuroscience of Attention Deficit Hyperactivity Disorder (ADHD) and its Clinical Translation. Front. Hum. Neurosci. 2018, 12, 100. [Google Scholar] [CrossRef] [PubMed]
- Fenollar-Cortés, J.; Navarro-Soria, I.; González-Gómez, C.; García-Sevilla, J. Detección de Perfiles Cognitivos Mediante WISC-IV en Niños Diagnosticados de TDAH: ¿Existen Diferencias Entre Subtipos? Rev. Psicodidáctica, 2015; 20, 157–176. [Google Scholar]
- Patros, C.H.; Tarle, S.J.; Alderson, R.M.; Lea, S.E.; Arrington, E.F. Planning Deficits in Children with Attention-Deficit/Hyperactivity Disorder (ADHD): A Meta-Analytic Review of Tower Task Performance. Neuropsychology 2019, 33, 425. [Google Scholar] [CrossRef] [PubMed]
- Pievsky, M.A.; McGrath, R.E. The Neurocognitive Profile of Attention-Deficit/Hyperactivity Disorder: A Review of Meta-Analyses. Arch. Clin. Neuropsychol. 2018, 33, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Schoechlin, C.; Engel, R.R. Neuropsychological Performance in Adult Attention-Deficit Hyperactivity Disorder: Meta-Analysis of Empirical Data. Arch. Clin. Neuropsychol. 2005, 20, 727–744. [Google Scholar] [CrossRef] [PubMed]
- Hyman, S.E. The Diagnosis of Mental Disorders: The Problem of Reification. Annu. Rev. Clin. Psychol. 2010, 6, 155–179. [Google Scholar] [CrossRef]
- Te Meerman, S.; Batstra, L.; Grietens, H.; Frances, A. ADHD: A Critical Update for Educational Professionals. Int. J. Qual. Stud. Health Well-Being 2017, 12 (Suppl. 1), 1298267. [Google Scholar] [CrossRef]
- Froehlich, T.E.; Anixt, J.S.; Loe, I.M.; Chirdkiatgumchai, V.; Kuan, L.; Gilman, R.C. Update on Environmental Risk Factors for Attention-Deficit/Hyperactivity Disorder. Curr. Psychiatry Rep. 2011, 13, 333–344. [Google Scholar] [CrossRef]
- Harold, G.T.; Leve, L.D.; Barrett, D.; Elam, K.; Neiderhiser, J.M.; Natsuaki, M.N.; Shaw, D.S.; Reiss, D.; Thapar, A. Biological and Rearing Mother Influences on Child ADHD Symptoms: Revisiting The Developmental Interface Between Nature And Nurture. J. Child Psychol. Psychiatry 2013, 54, 1038–1046. [Google Scholar] [CrossRef]
- Castells, X.; Ramos-Quiroga, J.; Bosch, R.; Nogueira, M.; Casas, M. Amphetamines for Attention Deficit Hyperactivity Disorder (ADHD) in Adults. Cochrane Database Syst. Rev. 2011, 6, CD007813. [Google Scholar] [CrossRef]
- Cortese, S.; Adamo, N.; Del Giovane, C.; Mohr-Jensen, C.; Hayes, A.J.; Carucci, S.; Atkinson, L.Z.; Tessari, L.; Banaschewski, T.; Coghill, D.; et al. Comparative Efficacy and Tolerability of Medications for Attention-Deficit Hyperactivity Disorder in Children, Adolescents, and Adults: A Systematic Review and Network Meta-Analysis. Lancet Psychiatry 2018, 5, 727–738. [Google Scholar] [CrossRef]
- Maneeton, N.; Maneeton, B.; Woottiluk, P.; Suttajit, S.; Likhitsathian, S.; Charnsil, C.; Srisurapanont, M. Comparative Efficacy, Acceptability, and Tolerability of Dexmethylphenidate Versus Placebo in Child and Adolescent ADHD: A Meta-Analysis of Randomized Controlled Trials. Neuropsychiatr. Dis. Treat. 2015, 11, 2943. [Google Scholar] [CrossRef]
- Coughlin, C.G.; Cohen, S.C.; Mulqueen, J.M.; Ferracioli-Oda, E.; Stuckelman, Z.D.; Bloch, M.H. Meta-Analysis: Reduced Risk of Anxiety with Psychostimulant Treatment in Children with Attention-Deficit/Hyperactivity Disorder. J. Child Adolesc. Psychopharmacol. 2015, 25, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.; Correll, C.U. Efficacy and Safety of Atomoxetine in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder: Results from a Comprehensive Meta-Analysis and Metaregression. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Jangmo, A.; Stålhandske, A.; Chang, Z.; Chen, Q.; Almqvist, C.; Feldman, I.; Bulik, C.M.; Lichtenstein, P.; D’Onofrio, B.; Kuja-Halkola, R.; et al. Attention-Deficit/Hyperactivity Disorder, School Performance, and Effect of Medication. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Keilow, M.; Holm, A.; Fallesen, P. Medical treatment of Attention Deficit/Hyperactivity Disorder (ADHD) and children’s academic performance. PLoS ONE 2018, 13, e0207905. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Sjölander, A.; Cederlöf, M.; D’Onofrio, B.M.; Almqvist, C.; Larsson, H.; Lichtenstein, P. Association Between Medication Use and Performance on Higher Education Entrance Tests in Individuals With Attention-Deficit/Hyperactivity Disorder. JAMA Psychiatry 2017, 74, 815. [Google Scholar] [CrossRef] [PubMed]
- Tsujii, N.; Okada, T.; Usami, M.; Kuwabara, H.; Fujita, J.; Negoro, H.; Kawamura, M.; Lida, J.; Saito, T. Effect of Continuing and Discontinuing Medications on Quality of Life After Symptomatic Remission in Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis. J. Clin. Psychiatry 2020, 81, 11514. [Google Scholar] [CrossRef] [PubMed]
- Chang, Z.; D’Onofrio, B.M.; Quinn, P.D.; Lichtenstein, P.; Larsson, H. Medication for Attention-Deficit/Hyperactivity Disorder and Risk for Depression: A Nationwide Longitudinal Cohort Study. Biol. Psychiatry 2016, 80, 916–922. [Google Scholar] [CrossRef]
- Chen, Q.; Sjölander, A.; Runeson, B.; D’Onofrio, B.M.; Lichtenstein, P.; Larsson, H. Drug Treatment for Attention-Deficit/Hyperactivity Disorder and Suicidal Behaviour: Register Based Study. BMJ 2014, 348, g3769. [Google Scholar] [CrossRef]
- Hua, M.-H.; Huang, K.-L.; Hsu, J.-W.; Bai, Y.-M.; Su, T.-P.; Tsai, S.-J.; Li, C.-H.; Lin, W.-C.; Chen, T.-J.; Chen, M.-H. Early Pregnancy Risk among Adolescents with ADHD: A Nationwide Longitudinal Study. J. Atten. Disord. 2021, 25, 1199–1206. [Google Scholar] [CrossRef]
- Chang, Z.; Lichtenstein, P.; Halldner, L.; D’Onofrio, B.; Serlachius, E.; Fazel, S.; Langstrom, N.; Larsson, H. Stimulant ADHD Medication and Risk for Substance Abuse. J. Child Psychol. Psychiatry 2014, 55, 878–885. [Google Scholar] [CrossRef]
- Chen, V.C.-H.; Yang, Y.-H.; Liao, Y.-T.; Kuo, T.-Y.; Liang, H.-Y.; Huang, K.-Y.; Huangm, Y.-C.; Lee, Y.; McIntyre, R.S.; Lin, T.-C. The Association Between Methylphenidate Treatment and the Risk For Fracture Among Young ADHD Patients: A Nationwide Population-Based Study in Taiwan. PLoS ONE 2017, 12, e0173762. [Google Scholar]
- Ghirardi, L.; Chen, Q.; Chang, Z.; Kuja-Halkola, R.; Skoglund, C.; Quinn, P.D.; D’Onofrio, B.M.; Larsson, H. Use of Medication for Attention-Deficit/Hyperactivity Disorder and Risk of Unintentional Injuries in Children and Adolescents with Co-Occurring Neurodevelopmental Disorders. J. Child Psychol. Psychiatry 2020, 61, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Man, K.K.; Chan, E.W.; Coghill, D.; Douglas, I.; Ip, P.; Leung, L.-P.; Tsui, M.S.H.; Wong, W.H.S.; Wong, I.C. Methylphenidate and the Risk of Trauma. Pediatrics 2015, 135, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Chang, Z.; Lichtenstein, P.; D’Onofrio, B.M.; Sjölander, A.; Larsson, H. Serious Transport Accidents in Adults with Attention-Deficit/Hyperactivity Disorder and the Effect of Medication: A Population-Based Study. JAMA Psychiatry 2014, 71, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Chang, Z.; Quinn, P.D.; Hur, K.; Gibbons, R.D.; Sjölander, A.; Larsson, H.; D’Onofrio, B.M. Association Between Medication Use for Attention-Deficit/Hyperactivity Disorder and Risk of Motor Vehicle Crashes. JAMA Psychiatry 2017, 74, 597–603. [Google Scholar] [CrossRef]
- Chen, V.C.-H.; Chan, H.-L.; Wu, S.-I.; Lu, M.-L.; Dewey, M.E.; Stewart, R.; Lee, C.T.-C. Methylphenidate and Mortality in Children with Attention-Deficit Hyperactivity Disorder: Population-Based Cohort Study. Br. J. Psychiatry 2020, 220, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Partridge, B.; Lucke, J.; Hall, W. Public Attitudes Towards the Acceptability of Using Drugs to Treat Depression and ADHD. Aust. N. Z. J. Psychiatry 2012, 46, 958–965. [Google Scholar] [CrossRef] [PubMed]
- Dosreis, S.; Zito, J.M.; Safer, D.J.; Soeken, K.L.; Mitchell, J.W., Jr.; Ellwood, L.C. Parental Perceptions and Satisfaction with Stimulant Medication for Attention-Deficit Hyperactivity Disorder. J. Dev. Behav. Pediatr. 2003, 24, 155–162. [Google Scholar] [CrossRef]
- Stroh, J.; Frankenberger, W.; Cornell-Swanson, L.V.; Wood, C.; Pahl, S. The Use of Stimulant Medication and Behavioral Interventions for the Treatment of Attention Deficit Hyperactivity Disorder: A Survey of Parents’ Knowledge, Attitudes, and Experiences. J. Child Fam. Stud. 2008, 17, 385–401. [Google Scholar] [CrossRef]
- Curtis, D.F.; Pisecco, S.; Hamilton, R.J.; Moore, D.W. Teacher Perceptions of Classroom Interventions for Children with ADHD: A Cross-Cultural Comparison of Teachers in the United States and New Zealand. Sch. Psychol. Q. 2006, 21, 171. [Google Scholar] [CrossRef]
- Frisch, L.; Moser, S.E.; Hawley, F.; Johnston, J.; Romereim, M. Kansas School Nurses’ Knowledge and Opinions About ADHD Stimulant Medication Therapy. J. Sch. Health 2003, 73, 127–128. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, R.; McCaffery, K.J.; Aslani, P. Factors Influencing Parental Decision Making About Stimulant Treatment for Attention-Deficit/Hyperactivity Disorder. J. Child Adolesc. Psychopharmacol. 2013, 23, 163–178. [Google Scholar] [CrossRef]
- Wang, L.-J.; Lee, S.-Y.; Yuan, S.-S.; Yang, C.-J.; Yang, K.-C.; Lee, T.-L.; Shyu, Y.-C. Impact of Negative Media Publicity on Attention-Deficit/Hyperactivity Disorder Medication in Taiwan. Pharmacoepidemiol. Drug Saf. 2016, 25, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.A.; Samuel, S.; Patel, D.R. Pharmacologic Management of Attention Deficit Hyperactivity Disorder in Children and Adolescents: A Review for Practitioners. Transl. Pediatr. 2018, 7, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Solmi, M.; Fornaro, M.; Ostinelli, E.G.; Zangani, C.; Croatto, G.; Monaco, F.; Kirinitski, D.; Fusar-Poli, P.; Correll, C.U. Safety of 80 Antidepressants, Antipsychotics, Anti-Attention-Deficit/Hyperactivity Medications and Mood Stabilizers in Children and Adolescents with Psychiatric Disorders: A Large Scale Systematic Meta-Review of 78 Adverse Effects. World Psychiatry 2020, 19, 214–232. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Biederman, J.; Morley, C.P.; Spencer, T.J. Effect of Stimulants on Height and Weight: A Review of the Literature. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 994–1009. [Google Scholar] [CrossRef]
- Shrestha, M.; Lautenschleger, J.; Soares, N. Non-pharmacologic management of attention-deficit/hyperactivity disorder in children and adolescents: A review. Transl. Pediatr. 2020, 9 (Suppl. 1), S114. [Google Scholar] [CrossRef]
- Borrell-Carrio, F. The Biopsychosocial Model 25 Years Later: Principles, Practice, and Scientific Inquiry. Ann. Fam. Med. 2004, 2, 576–582. [Google Scholar] [CrossRef]
- Farre, A.; Rapley, T. The New Old (and Old New) Medical Model: Four Decades Navigating the Biomedical and Psychosocial Understandings of Health and Illness. Healthcare 2017, 5, 88. [Google Scholar] [CrossRef]
- Inerney, S. Introducing the Biopsychosocial Model for Good Medicine and Good Doctors. BMJ 2018, 324, 1533. [Google Scholar]
- Ninot, G. Non-Pharmacological Interventions: An Essential Answer to Current Demographic, Health, and Environmental Transitions; Springer Nature: Berlin/Heidelberg, Germany, 2021; ISBN 9783030609702. [Google Scholar]
- Goldet, G.; Howick, J. Understanding GRADE: An Introduction. J. Evid. -Based Med. 2013, 6, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Parry, G.D.; Crawford, M.J.; Duggan, C. Iatrogenic harm from psychological therapies–time to move on. Br. J. Psychiatry 2016, 208, 210–212. [Google Scholar] [CrossRef]
- Rhule, D.M. Take care to do no harm: Harmful interventions for youth problem behavior. Prof. Psychol. Res. Pract. 2005, 36, 618. [Google Scholar] [CrossRef]
- Russell, G.; Ford, T.; Rosenberg, R.; Kelly, S. The Association of Attention Deficit Hyperactivity Disorder with Socioeconomic Disadvantage: Alternative Explanations and Evidence. J. Child Psychol. Psychiatry 2014, 55, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Gnanavel, S.; Sharma, P.; Kaushal, P.; Hussain, S. Attention Deficit Hyperactivity Disorder and Comorbidity: A Review of Literature. World J. Clin. Cases 2019, 7, 2420. [Google Scholar] [CrossRef] [PubMed]
- Schunemann, H.; GRADE Handbook for Grading Quality of Evidence and Strength of Recommendation. Version 3.2. 2008. Available online: https://www.cc-ims.net/gradepro (accessed on 19 April 2020).
- Lüdecke, D.; David, B.W. Package ‘esc’; R Package Version 0.5, 1; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Van den Noortgate, W.; López-López, J.A.; Marín-Martínez, F.; Sánchez-Meca, J. Three-Level Meta-Analysis of Dependent Effect Sizes. Behav. Res. Methods 2013, 45, 576–594. [Google Scholar] [CrossRef] [PubMed]
- Cheung, M.W.-L. A Guide to Conducting a Meta-Analysis with Non-Independent Effect Sizes. Neuropsychol. Rev. 2019, 29, 387–396. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Assink, M.; Wibbelink, C.J. Fitting Three-Level Meta-Analytic Models in R: A Step-by-Step Tutorial. Quant. Methods Psychol. 2016, 12, 154–174. [Google Scholar] [CrossRef]
- Bowden, J.; Tierney, J.F.; Copas, A.J.; Burdett, S. Quantifying, Displaying and Accounting for Heterogeneity in the Meta-Analysis of RCTs Using Standard and Generalised Qstatistics. BMC Med. Res. Methodol. 2011, 11, 41. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Habeck, C.W.; Schultz, A.K. Community-level impacts of white-tailed deer on understorey plants in North American forests: A meta-analysis. AoB Plants 2015, 7, plv119. [Google Scholar] [CrossRef]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading Quality of Evidence and Strength of Recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Corbisiero, S.; Bitto, H.; Newark, P.; Abt-Mörstedt, B.; Elsässer, M.; Buchli-Kammermann, J.; Künne, S.; Nyberg, E.; Hofecker-Fallahpour, M.; Stieglitz, R.D. A Comparison of Cognitive-Behavioral Therapy and Pharmacotherapy vs. Pharmacotherapy Alone in Adults With Attention-Deficit/Hyperactivity Disorder (ADHD)-A Randomized Controlled Trial. Front. Psychiatry 2018, 9, 571. [Google Scholar] [CrossRef]
- Emilsson, B.; Gudjonsson, G.; Sigurdsson, J.F.; Baldursson, G.; Einarsson, E.; Olafsdottir, H.; Young, S. Cognitive behaviour therapy in medication-treated adults with ADHD and persistent Symptoms: A randomized controlled trial. BMC Psychiatry 2011, 11, 116. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Xu, G.; Zhu, Y. A Randomized controlled trial of mindfulness-based cognitive therapy for college students with ADHD. J. Atten. Disord. 2016, 22, 388–399. [Google Scholar] [CrossRef]
- Pettersson, R.; Söderström, S.; Edlund-Söderström, K.; Nilsson, K. Internet-based cognitive behavioral therapy for adults with ADHD in outpatient psychiatric care. J. Atten. Disord. 2016, 21, 508–521. [Google Scholar] [CrossRef]
- Safren, S.A.; Sprich, S.; Mimiaga, M.J.; Surman, C.; Knouse, L.; Groves, M.; Otto, M. Cognitive behavioral therapy vs relaxation with educational support for medication-treated adults with ADHD and persistent symptoms. JAMA 2010, 304, 875–880. [Google Scholar] [CrossRef]
- Schoenberg, P.L.; Hepark, S.; Kan, C.C.; Barendregt, H.P.; Buitelaar, J.K.; Speckens, A.E. Effects of mindfulness-based cognitive therapy on neurophysiological correlates of performance monitoring in adult attention-deficit/hyperactivity disorder. Clin. Neurophysiol. 2014, 125, 1407–1416. [Google Scholar] [CrossRef]
- Solanto, M.V.; Marks, D.J.; Wasserstein, J.; Mitchell, K.; Abikoff, H.; Alvir, J.M.J.; Kofman, M.D. Efficacy of meta-cognitive therapy for adult ADHD. Am. J. Psychiatry 2010, 167, 958–968. [Google Scholar] [CrossRef]
- Kang, K.D.; Choi, J.W.; Kang, S.G.; Han, D.H. Sports Therapy for attention, cognitions and sociality. Laryngo-Rhino-Otologie 2011, 32, 953–959. [Google Scholar] [CrossRef]
- Meßler, C.F.; Holmberg, H.-C.; Sperlich, B. Multimodal therapy involving high-intensity interval training improves the physical fitness, motor skills, social behavior, and quality of life of boys with ADHD: A randomized controlled study. J. Atten. Disord. 2016, 22, 806–812. [Google Scholar] [CrossRef]
- Abikoff, H.B.; Thompson, M.; Laver-Bradbury, C.; Long, N.; Forehand, R.; Brotman, L.M.; Klein, R.G.; Reiss, P.; Huo, L.; Sonuga-Barke, E. Parent training for preschool ADHD: A randomized controlled trial of specialized and generic programs. J. Child Psychol. Psychiatry 2014, 56, 618–631. [Google Scholar] [CrossRef]
- Yang, L.; Bai, G.-N.; Wang, Y.-F.; Niu, W.-Y. Effectiveness of a focused, brief psychoeducation program for parents of ADHD children: Improvement of medication adherence and symptoms. Neuropsychiatr. Dis. Treat. 2015, 11, 2721–2735. [Google Scholar] [CrossRef]
- Behbahani, M.; Zargar, F.; Assarian, F.; Akbari, H. Effects of Mindful Parenting Training on Clinical Symptoms in Children with Attention Deficit Hyperactivity Disorder and Parenting Stress: Randomized Controlled Trial. Iran. J. Med. Sci. 2018, 43, 596–604. [Google Scholar] [CrossRef]
- Haack, L.M.; Villodas, M.; McBurnett, K.; Hinshaw, S.; Pfiffner, L.J. Parenting as a Mechanism of Change in Psychosocial Treatment for Youth with ADHD, Predominantly Inattentive Presentation. J. Abnorm. Child Psychol. 2016, 45, 841–855. [Google Scholar] [CrossRef]
- Herbert, S.D.; Harvey, E.A.; Roberts, J.L.; Wichowski, K.; Lugo-Candelas, C.I. A Randomized Controlled Trial of a Parent Training and Emotion Socialization Program for Families of Hyperactive Preschool-Aged Children. Behav. Ther. 2013, 44, 302–316. [Google Scholar] [CrossRef]
- Lange, A.-M.; Daley, D.; Frydenberg, M.; Houmann, T.; Kristensen, L.J.; Rask, C.; Sonuga-Barke, E.; Søndergaard-Baden, S.; Udupi, A.; Thomsen, P.H. Parent Training for Preschool ADHD in Routine, Specialist Care: A Randomized Controlled Trial. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 593–602. [Google Scholar] [CrossRef]
- Hosainzadeh Maleki, Z.; Mashhadi, A.; Soltanifar, A.; Moharreri, F.; Ghanaei Ghamanabad, A. Barkley’s Parent Training Program, Working Memory Training and their Combination for Children with ADHD: Attention Deficit Hyperactivity Disorder. Iran. J. Psychiatry 2014, 9, 47–54. [Google Scholar]
- Pfiffner, L.J.; Hinshaw, S.P.; Owens, E.; Zalecki, C.; Kaiser, N.M.; Villodas, M.; McBurnett, K. A two-site randomized clinical trial of integrated psychosocial treatment for ADHD-inattentive type. J. Consult. Clin. Psychol. 2014, 82, 1115–1127. [Google Scholar] [CrossRef] [PubMed]
- Shafiee-Kandjani, A.R.; Noorazar, G.; Shahrokhi, H.; Nazari, M.A.; Farhang, S. Effect of Parent Management Training on Attention, Response Prevention, Impulsivity and Vigilance of Boys with Attention Deficient/Hyperactive Disorder. Iran. J. Psychiatry Behav. Sci. 2017, 11. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.J.S.; Barton, J.; Daley, D.; Hutchings, J.; Maishman, T.; Raftery, J.; Stanton, L.; Laver-Bradbury, C.; Chorozoglou, M.; Coghill, D.; et al. A comparison of the clinical effectiveness and cost of specialised individually delivered parent training for preschool attention-deficit/hyperactivity disorder and a generic, group-based programme: A multi-centre, randomised controlled trial of the New Forest Parenting Programme versus Incredible Years. Eur. Child Adolesc. Psychiatry 2017, 27, 797–809. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, Ö.; Gonka, Ö.; Aynur, A.P. The effects of the triple P-positive parenting programme on parenting, family functioning and symptoms of attention-deficit/hyperactivity disorder. A randomized controlled trial. Psychiatry Clin. Psychopharmacol. 2018, 29, 665–673. [Google Scholar] [CrossRef]
- Corkum, P.; Elik, N.; Blotnicky-Gallant, P.A.C.; McGonnell, M.; McGrath, P. Web-Based Intervention for Teachers of Elementary Students With ADHD: Randomized Controlled Trial. J. Atten. Disord. 2015, 23, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Schultz, B.K.; Evans, S.W.; Langberg, J.M.; Schoemann, A. Outcomes for adolescents who comply with long-term psychosocial treatment for ADHD. J. Consult. Clin. Psychol. 2017, 85, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Dittner, A.J.; Hodsoll, J.; Rimes, K.A.; Russell, A.J.; Chalder, T. Cognitive-behavioural therapy for adult attention-deficit hyperactivity disorder: A proof of concept randomised controlled trial. Acta Psychiatr. Scand. 2017, 137, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Solanto, M.V.; Surman, C.B.; Alvir, J. The efficacy of cognitive-behavioral therapy for older adults with ADHD: A randomized controlled trial. Atten. Defic. Hyperact. Disord. 2018, 10, 223–235. [Google Scholar] [CrossRef] [PubMed]
- Cerrillo-Urbina, A.J.; García-Hermoso, A.; Sánchez-López, M.; Pardo-Guijarro, M.J.; Santos Gómez, J.L.; Martínez-Vizcaíno, V. The effects of physical exercise in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis of randomized control trials. Child: Care Health Develop. 2015, 41, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Zang, Y. Impact of physical exercise on children with attention deficit hyperactivity disorders: Evidence through a meta-analysis. Medicine 2019, 98, e17980. [Google Scholar] [CrossRef] [PubMed]
- Mulqueen, J.M.; Bartley, C.A.; Bloch, M.H. Meta-Analysis: Parental Interventions for Preschool ADHD. J. Atten. Disord. 2015, 19, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Rimestad, M.L.; Lambek, R.; Zacher Christiansen, H.; Hougaard, E. Short- and Long-Term Effects of Parent Training for Preschool Children With or at Risk of ADHD: A Systematic Review and Meta-Analysis. J. Atten. Disord. 2019, 23, 423–434. [Google Scholar] [CrossRef] [PubMed]
- DuPaul, G.J. Promoting success across school years for children with Attention-Deficit/Hyperactivity Disorder: Collaborative school-home intervention. J. Am. Acad. Child. Adolesc. Psychiatry. 2018, 57, 231–232. [Google Scholar] [CrossRef] [PubMed]
- Bikic, A.; Reichow, B.; McCauley, S.A.; Ibrahim, K.; Sukhodolsky, D.G. Meta-Analysis of Organizational Skills Interventions for Children and Adolescents with Attention-Deficit/Hyperactivity Disorder. Clin. Psychol. Rev. 2017, 52, 108–123. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.W.; Schultz, B.K.; DeMars, C.E.; Davis, H. Effectiveness of the Challenging Horizons After-School Program for Young Adolescents With ADHD. Behav. Ther. 2011, 42, 462–474. [Google Scholar] [CrossRef]
- Dziak, J.J.; Coffman, D.L.; Lanza, S.T.; Li, R.; Jermiin, L.S. Sensitivity and specificity of information criteria. Brief. Bioinform. 2020, 21, 553–565. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide; Chapman and Hall/CRC: Boca Raton, FL, USA, 2021; ISBN 9780367610074. [Google Scholar]
- Gaastra, G.F.; Groen, Y.; Tucha, L.; Tucha, O. The Effects of Classroom Interventions on Off-Task and Disruptive Classroom Behavior in Children with Symptoms of Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Review. PLoS ONE 2016, 11, e0148841. [Google Scholar] [CrossRef]
- Hodgson, K.; Hutchinson, A.D.; Denson, L. Nonpharmacological Treatments for ADHD: A Meta-Analytic Review. J Atten Disord. 2014, 18, 275–282. [Google Scholar] [CrossRef]
- Rimestad, M.L.; O’Toole, M.S.; Hougaard, E. Mediators of Change in a Parent Training Program for Early ADHD Difficulties: The Role of Parental Strategies, Parental Self-Efficacy, and Therapeutic Alliance. J Atten Disord. 2020, 24, 1966–1976. [Google Scholar] [CrossRef]
- Achenbach, T.M.; McConaughy, S.H.; Howell, C.T. Child/Adolescent Behavioral and Emotional Problems: Implications of Cross-Informant Correlations for Situational Specificity. Psychol. Bull. 1987, 101, 213. [Google Scholar] [CrossRef]
- Biederman, J.; Faraone, S.V.; Milberger, S.; Doyle, A. Diagnoses of Attention-Deficit Hyperactivity Disorder from Parent Reports Predict Diagnoses Based on Teacher Reports. J. Am. Acad. Child Adolesc. Psychiatry 1993, 32, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Antrop, I.; Roeyers, H.; Oosterlaan, J.; Van Oost, P. Agreement Between Parent and Teacher Ratings of Disruptive Behavior Disorders in Children with Clinically Diagnosed ADHD. J. Psychopathol. Behav. Assess. 2002, 24, 67–73. [Google Scholar] [CrossRef]
- Malhi, P.; Singhi, P.; Sidhu, M. Impact of Parent and Teacher Toncordance on Diagnosing Attention Deficit Hyperactivity Disorder and its Sub-Sypes. Indian J. Pediatr. 2008, 75, 223–228. [Google Scholar] [CrossRef]
- Lavigne, J.V.; Dulcan, M.K.; LeBailly, S.A.; Binns, H.J. Can Parent Reports Serve as a Proxy for Teacher Ratings in Medication Management of Attention-Deficit Hyperactivity Disorder? J. Dev. Behav. Pediatr. 2012, 33, 336–342. [Google Scholar] [CrossRef] [PubMed]
- DuPaul, G.J.; Fu, Q.; Anastopoulos, A.D.; Reid, R.; Power, T.J. ADHD Parent and Teacher Symptom Ratings: Differential Item Functioning Across Gender, Age, Race, and Ethnicity. J. Abnorm. Child Psychol. 2020, 48, 679–691. [Google Scholar] [CrossRef]
- Hartman, C.A.; Rhee, S.H.; Willcutt, E.G.; Pennington, B.F. Modeling Rater Disagreement for ADHD: Are Parents or Teachers Biased? J. Abnorm. Child Psychol. 2007, 35, 536–542. [Google Scholar] [CrossRef]
- Jungersen, C.M.; Lonigan, C.J. Do Parent and Teacher Ratings of ADHD Reflect the Same Constructs? A Measurement Invariance Analysis. J. Psychopathol. Behav. Assess. 2021, 43, 778–792. [Google Scholar] [CrossRef]
- Takeda, T.; Nissley-Tsiopinis, J.; Nanda, S.; Eiraldi, R. Factors Associated with Discrepancy in Parent–Teacher Reporting of Symptoms of ADHD in a Large Clinic-Referred Sample of Children. J. Atten. Disord. 2020, 24, 1605–1615. [Google Scholar] [CrossRef]
- Doig, G.S.; Simpson, F. Randomization and Allocation Concealment: A Practical Guide for Researchers. J. Crit. Care 2005, 20, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Davidson, R.J.; Kaszniak, A.W. Conceptual and Methodological Issues in Research on Mindfulness and Meditation. Am. Psychol. 2015, 70, 581. [Google Scholar] [CrossRef]
- Munafò, M.R.; Nosek, B.A.; Bishop, D.V.; Button, K.S.; Chambers, C.D.; Percie du Sert, N.; Simonson, U.; Wagenmakers, E.-J.; Ware, J.J.; Ioannidis, J. A Manifesto for Reproducible Science. Nat. Hum. Behav. 2017, 1, 0021. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | n2 | Intervention | Population (Age Range If Provided) | Mean Age (% Male) | Comparator | % (Exp, Ctrl) on RX 3 | Follow Up (Weeks) | ADHD Scales | GRADE Rating (Limitation Domain or Other Reason If Downgraded) |
|---|---|---|---|---|---|---|---|---|---|---|
| CBT | ||||||||||
| Corbisiero [92] | 2018 | 35–41 | 10–12 weeks individual CBT | Adults (18–49) | 32.05 (60%) | TAU | 100%, 100% | 39 | WRAADDS (C), CAARS (S:S; O:L) ADHD-SR (S) | 3 (Blinding) |
| 2018 | 39–46 | 16 weeks individual CBT | Adults (18–65) | 35.9 (69%) | TAU | 63%, 87% | 42 | CSS (S;O), CGI-I (S,C 4) | 3 (Blinding) | |
| Emilsson [93] | 2011 | 21–35 | 15 session group/individual CBT (R&R2ADHD) | Adults | 33.9 (37%) | TAU | 100%, 100% | 12 | K-SADS-PL (C), CGI-S (C), BCS (S), RATE-S(S) | 3 (Blinding) |
| Gu [94] | 2018 | 54 | 6 weeks Individual MCBT | Adults (19–24) | 20.3 (55%) | Waitlist | 72%, 77% | 12 | CAARS (S:S) | 2 (Allocation concealment, control group, blinding) |
| Pettersson [95] | 2017 | 28–32 5 | 10 weeks internet individual and group therapy (In focus) | Adults | 34.7 (33%) | Waitlist | 43%, 50% | None | CSS (S) | 3 (control group, blinding) |
| Safren [96] | 2010 | 67–84 | 12 sessions (15 weeks) of individual CBT | Adults (18–65) | 43.2 (56%) | Relaxation training and emotional support | 100%, 100% | 26 and 52 | CCS (S), ADHD-RS-IV (S), CGI-S (C) | 4 |
| Schonberg [97] | 2013 | 44 | 12 weeks Group MCBT | Adults (19–53) | 37.0 (48%) | Waitlist | 48%, 62% | None | CAARS(S:S) | 2 (Allocation Concealment, blinding, inactive control group, no ITT) |
| Solanto [98] | 2010 | 81 | Meta-cognitive therapy | Adults (18–65) | 41.7 (34%) | Group support | Not reported | None | AISRS-IN (C), CAARS (O:L); BAS (S) ON-TOP (S) | 2 (Allocation concealment, blinding, no ITT) |
| Physical and Mind body intervention | ||||||||||
| Kang [99] | 2011 | 28 | 6 weeks (12 90 sessions) of sport therapy | Children | 8.5 (100%) | Education on behavior control | 100%, 100% | None | K-ARS (P,T) | 2 (allocation concealment, blinding) |
| Meßler [100] * | 2018 | 28 | 3 weeks HIIT training (3 sessions/w of 4 × 4 min intervals) | Children (8 to 13) | 11 (100%) | weeks of low intensity physical activity (1 90 min session/week | 36%, 29% | None | FBB-HKS (P) SBB-HKS (S) DISYPS-II (?) | 2 (allocation concealment, blinding) |
| Caregiver | ||||||||||
| Abikoff [101] | 2015 | 101 | New Forest Parenting Program (8 × 60–90 min individual sessions) | Preschooler (3–4) | 73% | Waitlist | 0%, 0% | None | CPRS-R (P), CTRS-R (T) DuPaul ADHD-RS-IV (C) | 4 * Example of dual blind |
| Bai [102] | 2017 | 89 | 3 months of medication adherence program, individual and group, online and in person | Children/adolescent (6–16) | 9.5 (80%) | General clinical counselling | 1%, 1% | None | ADHD-RS-IV (P) | 4 |
| Behbahani [103] | 2018 | 48–52 | Mindful Parenting programme (8 weeks) | Children (7–12 | ? (66%) | Waitlist | 100%, 100% | 8 | SNAP- IV (P) | 2 (allocation concealment, blinding, passive control group, no ITT) |
| Haack [104] | 2017 | 128 | 10–13 weeks Parent Focused Training | Children (7–11) | 8.6 (58%) | TAU | 9%, 2% | 21–30 | CSI (P;T) COSS (T;P) | 3 (Allocation concealment, blinding) |
| Herbert [105] | 2013 | 31 | The Parenting Your Hyperactive Preschooler program (14 × 90 min session) | Preschooler (34–76 mo) | 4.6 (74%) | Waitlist | 18%, 7% | None | DBRS (P) | 3(blinding, passive control group) |
| Lange [106] | 2018 | 129–148 | New Forest Parenting Program (8 × 60–90 min individual sessions) | Preschooler/children (3–7) | ? (73%) | TAU | 0%, 0% | 36 | ADHD-RS-IV (P) | 4 |
| Maleki * [107] | 2014 | 36 | Barkley Parent Training program | Children (6–12) | ? * (?) | Working memory training | 100%, 100%6 | SNAP-IV (P) CLCL (P) | 3 (allocation concealment, blinding) | |
| Pfiffner [108] | 2014 | 90–122 | 12 weeks Parent focused training | Children (7–11) inattentive type only | 8.6 (58%) | TAU | 15%, 14% | 12 weeks | CSI (T;P), COSS (T;P), CGI-I (T;P), CGI-S (T) | 2 (allocation concealment, blinding) |
| Shafiee-Kandjani [109] | 2017 | 25–32 | New Forest Parenting Program 8 × 60–90 min individual sessions) | Children (6–12 years) | 7.1 (100%) | TAU | ?? | 4 | CPRS (P) | 4 |
| Sonuga-Barke [110] | 2018 | 173–175 | New Forest Parenting Program (12 individual sessions) and Incredible years (12 group sessions) | Preschooler (2 y 9 mo–4 years 6 mo) | 3.55 (68%) | TAU | 0%,0% | 26 | SNAP-IV (P,T) DOA (C) | 4 |
| Yusuf [111] | 2019 | 48 | Triple P program (8 weeks, 5 × 120 m session + 3 × 15–30 m phone session) | Children (7–12) | 10.25 (79%) | Waitlist | 100%, 100% | None | DuPaul ADHD-RS-IV (C), GCI-S (C) | 2 (allocation concealment, blinding, passive control group) |
| School Based and Executive | ||||||||||
| Corkum [112] | 2019 | 58 | 6 weeks Online teacher training | Children (grade 1 to 6) | 8.2 (88%) | Waitlist | 85%, 76% | 6 | CPRS-3 (P) CPRS-3 (T) IRS (P,T) | 3 (Blinding, passive control group) |
| Schultz [113] | 2017 | 88–216 | Challenge Horizon Program (1 year after school training, 2 × 75 min/week) | Adolescents (Grade 6 to 8) | 12.15 (72%) | Community Care | 49%, 47% | 28 | COSS (P) DBRS (P) | 3 (blinding) |
| First Author | Year | Number of Studies | Total n | Design of Included Studies | Type of Intervention | Population | Average Study Quality 1 | Evidence of Publication Bias |
|---|---|---|---|---|---|---|---|---|
| Bikic [121] | 2017 | 12 | 1054 | RCT | Executive training | Children and adolescents | Low (high risk of bias) | Not reported |
| Cerrillo-Urbina [116] | 2015 | 8 | 249 | RCT | Physical exercise | Children and adolescents | Low | No |
| Gaastra [125] | 2016 | 24 | Not reported | Whitin-study design | School based intervention | Children | Moderate to high | Yes |
| Hodgson [126] * | 2014 | 4 | 206 | Unclear | Behavioral training, school based, executive training, parent training | Preschoolers to adolescents | Not reported | Not reported |
| Mulqueen [118] | 2015 | 8 | 399 | RCT | Parent training | Preschoolers | Not reported | No |
| Rimestad [127] | 2011 | 16 | 1003 | RCT | Parent training | Preschoolers | Moderate | No |
| Zang * [117] | 2019 | 14 | 574 | RCT, case-control | Physical exercise | Children and adolescents | Moderate | Yes |
| All | Parent | Teacher | |
|---|---|---|---|
| Observations | 69 | 42 | 27 |
| Studies | 49 | 35 | 24 |
| Meta-analyses | 5 | 5 | 3 |
| Effect Size | 0.604 | 0.524 | 0.610 |
| Standard Error | 0.148 | 0.066 | 0.38 |
| p-value | 0.001 | 0.001 | 0.12 |
| Qp-value | 0 | 0.001 | 0.00 |
| Fitvslvl3 | 0.002 | 0.0327 | 0.01 |
| Fitlvl4 | 0.0001 | 0.0001 | 0.00 |
| Error I2 | 10.03% | 39.90% | 3.57% |
| Level 2 I2 | 12.71% | 0.00% | 0.00% |
| Level 3 I2 | 63.51% | 61.10% | 55.56% |
| Level 4 I2 | 13.75% | 0.00% | 40.86% |
| Number of Studies | Total n | Quality of Evidence (GRADE) | Pooled Effect Size (95% CI) | Recommendation | |
|---|---|---|---|---|---|
| Overall | 20 1 | 1673 | ⊕⊕⊝⊝ WEAK (unreported or inadequate allocation concealment, inadequate blinding, lack of ITT analyses evidence of publication bias) | 0.66 (0.50; 0.82) | Probably do it |
| Cognitive behavioral therapy | 8 | 417 | ⊕⊕⊕⊝ MODERATE (unreported or inadequate allocation concealment, inadequate blinding) | 0.74 (0.50; 0.98) | Do it |
| Mind–body intervention and physical exercise | 1 2 | 56 | ⊕⊝⊝⊝ Very Weak (Insufficient data) | N/A | No recommendation |
| Caregiver intervention | 10 3 | 962 | ⊕⊝⊝⊝ Very Weak (unreported or inadequate allocation concealment, inadequate blinding, lack of ITT analyses in presence of attrition, variability in effect by population and by outcome assessor, publication bias) | 0.64 (0.37–0.91) | Probably do it |
| School-based intervention | 2 [118] 4 | 274 | ⊕⊝⊝⊝ Very Weak (Insufficient data, allocation concealment, inadequate blinding, lack of ITT analyses) | 0.52 (0.30; 0.74) | Probably do it |
| Adults (note: only based on CBT) | 8 [121] | 56 | ⊕⊕⊕⊝ MODERATE (unreported or inadequate allocation concealment, inadequate blinding) | 0.74 (0.50; 0.98) | Do it |
| Adolescents | 2 | 305 | ⊕⊝⊝⊝ Very Weak (Insufficient data) | Not enough study for analyses | No recommendation |
| Children | 15 [125] | 998 | ⊕⊕⊝⊝ WEAK (unreported or inadequate allocation concealment, inadequate blinding, lack of ITT analyses in presence of attrition, high between-study heterogeneity) | 0.73 (0.49; 0.97) | Probably do it |
| Preschoolers | 5 [119] | 455 | ⊕⊕⊝⊝ WEAK (unreported or inadequate allocation concealment, inadequate blinding, lack of ITT analyses in presence of attrition) | 0.32 (−0.01; 0.63) | Probably don’t do it |
| Studies | Total n | Quality of Evidence (GRADE) | Pooled Effect Size (95% CI) | Recommendation | |
|---|---|---|---|---|---|
| Adults | 8 | 417 | ⊕⊕⊕⊝ MODERATE (unreported or inadequate allocation concealment, inadequate blinding) | 0.74 (0.50; 0.98) | Do It |
| Adolescents | 0 | ? No data | N/A | No recommendation | |
| Children | 0 | ? No data | N/A | No recommendation | |
| Preschoolers | 0 | ? No data | N/A | No recommendation |
| Studies | Total n | Quality of Evidence (GRADE) | Pooled Effect Size (95% CI) | Recommendation | |
|---|---|---|---|---|---|
| Adults | 0 | 0 | ? No data | N/A | No recommendation |
| Adolescents | 0 | 0 | ? No data | No recommendation | |
| Children | 1 (+1 quali) | 56 | ⊕⊝⊝⊝ Very Weak (Insufficient data, allocation concealment, blinding) | No recommendation | |
| Preschoolers | 0 | 0 | ? No data | No recommendation |
| Nb of Studies | Total n | Quality of Evidence (GRADE) | Pooled Effect Size (95% CI) | Recommendation | |
|---|---|---|---|---|---|
| Adolescents | 1 | 89 | ⊕⊝⊝⊝ Very Weak (Insufficient data) | N/A | No recommendation |
| Children | 7 | 907 | ⊕⊝⊝⊝ Very Weak (unreported or inadequate allocation concealment, inadequate blinding, lack of ITT analyses in presence of attrition, variability in effect by outcome assessor, publication bias) | 0.91 (0.54–1.28) | Probably do it |
| Preschoolers | 4 | 455 | ⊕⊕⊝⊝ WEAK (unreported or inadequate allocation concealment, inadequate blinding, lack of ITT analyses in presence of attrition) | 0.04 (0.06; 0.14) | Probably don’t do it |
| k (j) | Total n | Quality of Evidence (GRADE) | Pooled Effect Size (95% CI) | Recommendation | |
|---|---|---|---|---|---|
| Adults | 0 | 0 | ? No data | No recommendation | |
| Adolescents | 1 | 216 | ⊕⊝⊝⊝ Very Weak (Insufficient data) | N/A | No recommendation |
| Children | 1 | 58 | ⊕⊝⊝⊝ Very Weak (Insufficient data) | N/A | No recommendation |
| Preschoolers | 0 | 0 | ? No data | No recommendation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tourjman, V.; Louis-Nascan, G.; Ahmed, G.; DuBow, A.; Côté, H.; Daly, N.; Daoud, G.; Espinet, S.; Flood, J.; Gagnier-Marandola, E.; et al. Psychosocial Interventions for Attention Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis by the CADDRA Guidelines Work GROUP. Brain Sci. 2022, 12, 1023. https://doi.org/10.3390/brainsci12081023
Tourjman V, Louis-Nascan G, Ahmed G, DuBow A, Côté H, Daly N, Daoud G, Espinet S, Flood J, Gagnier-Marandola E, et al. Psychosocial Interventions for Attention Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis by the CADDRA Guidelines Work GROUP. Brain Sciences. 2022; 12(8):1023. https://doi.org/10.3390/brainsci12081023
Chicago/Turabian StyleTourjman, Valerie, Gill Louis-Nascan, Ghalib Ahmed, Anaïs DuBow, Hubert Côté, Nadia Daly, George Daoud, Stacey Espinet, Joan Flood, Emilie Gagnier-Marandola, and et al. 2022. "Psychosocial Interventions for Attention Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis by the CADDRA Guidelines Work GROUP" Brain Sciences 12, no. 8: 1023. https://doi.org/10.3390/brainsci12081023