
Type 2 Diabetes Mellitus with Tight Glucose Control and Poor Pre-Injury Stair Climbing Capacity May Predict Postoperative Delirium: A Secondary Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
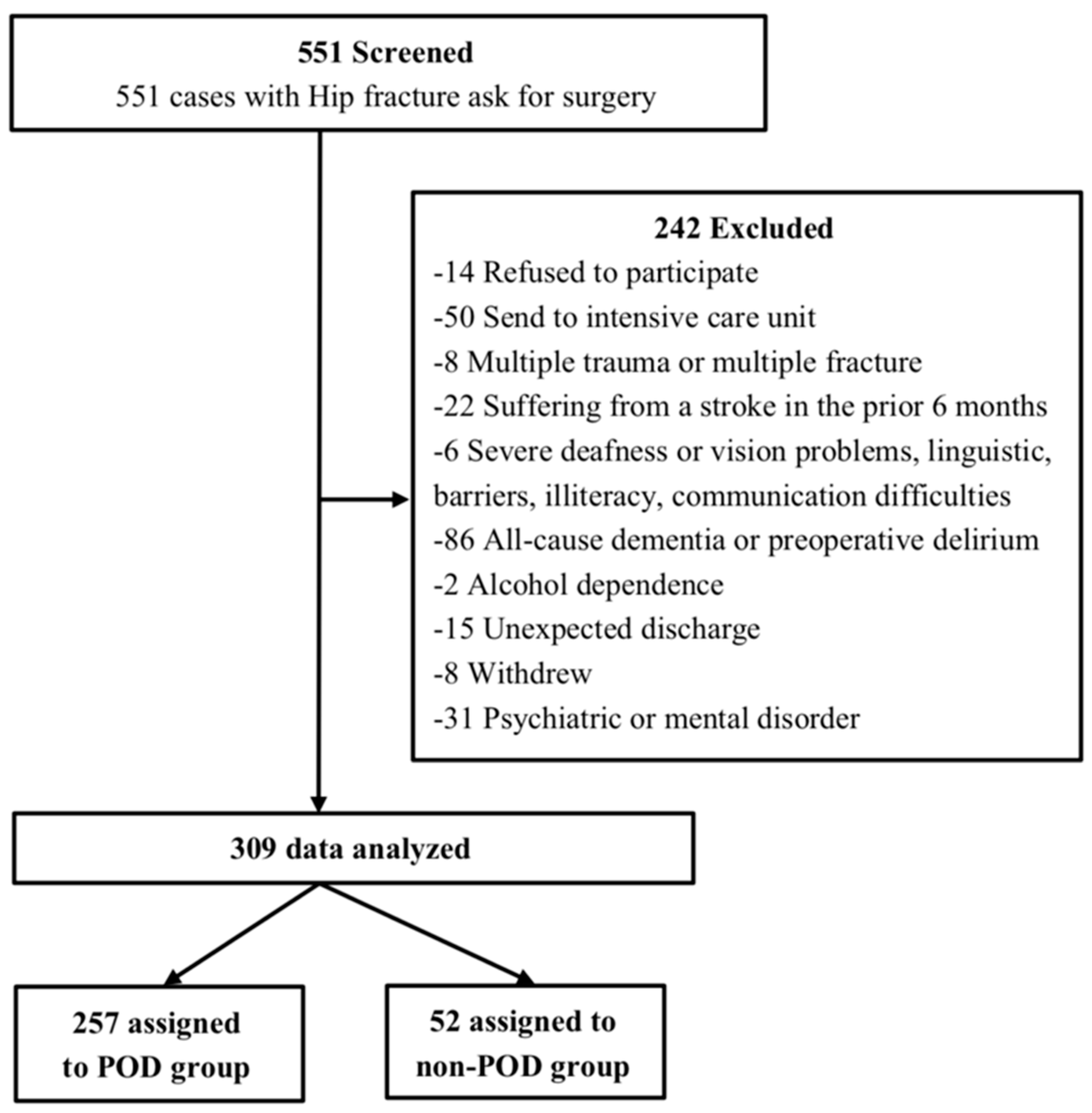
2.2. Participants and Features
2.3. Preoperative Interview
2.4. Glycemic Control Factors
2.5. Assessment of Pre-Injury Physical Performance
2.6. Anesthesia and Analgesia
2.7. Postoperative Assessment
2.8. Statistical Analysis
3. Results
3.1. Baseline Features
3.2. Glycemic Control Factors
3.3. Pre-Injury Physical Performance
3.4. Univariate Logistic Regression Analysis
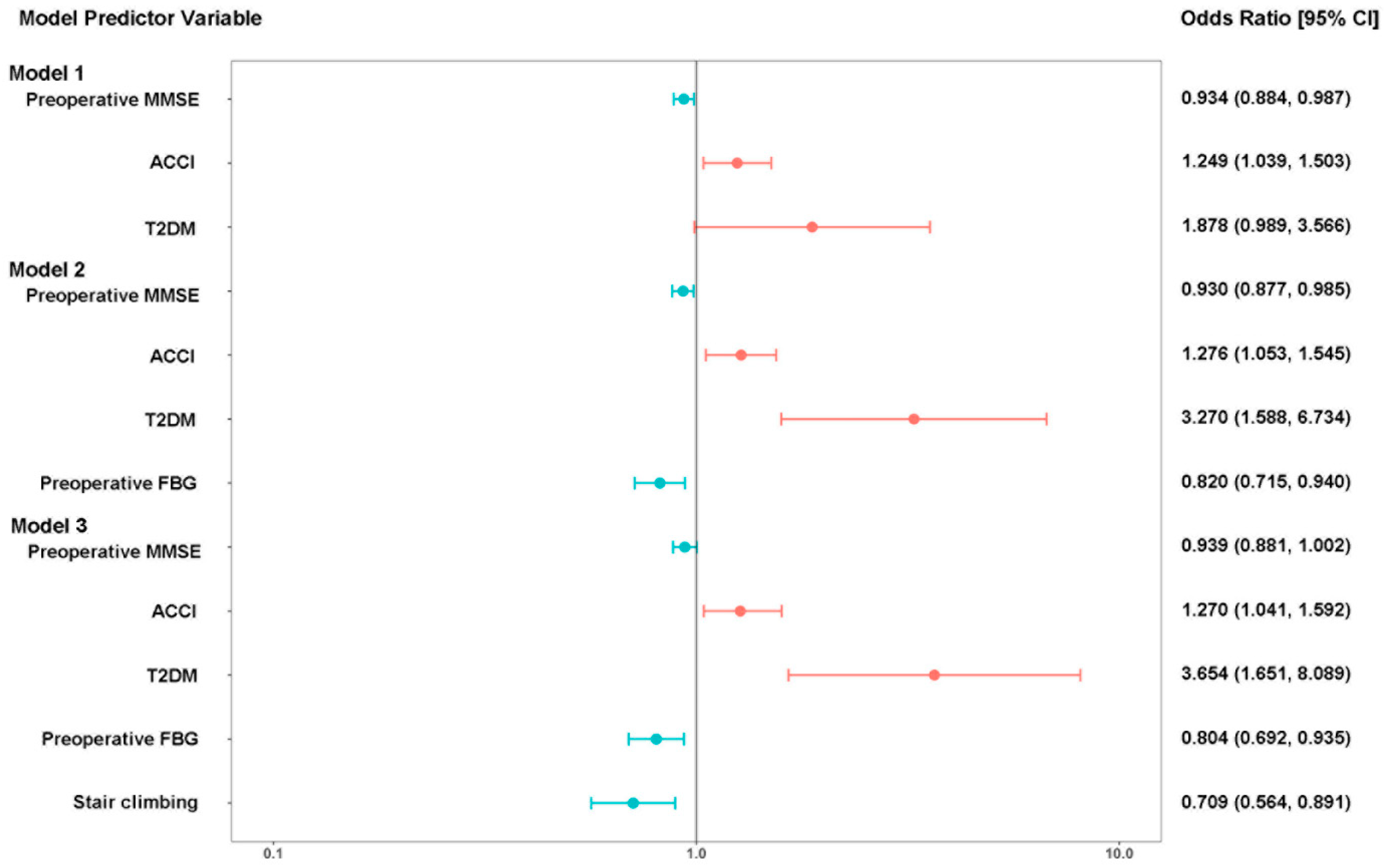
3.5. Multivariable Logistic Regression Analysis
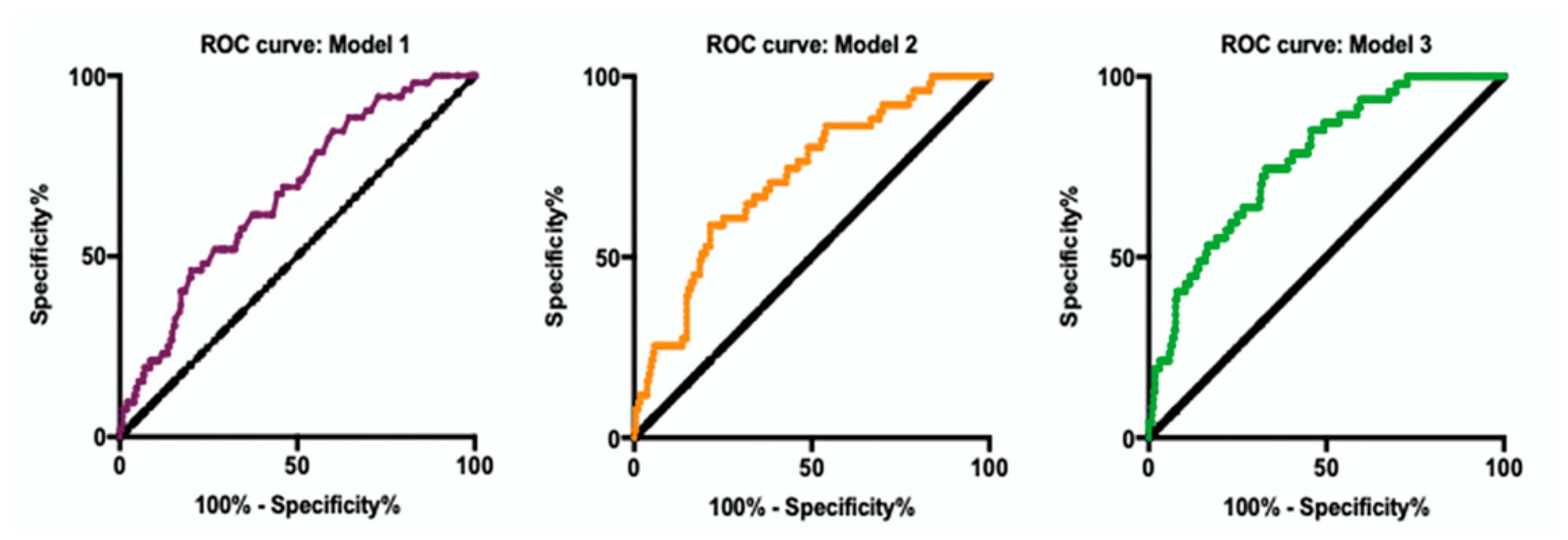
3.6. Prediction Model for POD
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Poeran, J.; Cozowicz, C.; Zubizarreta, N.; Weinstein, S.M.; Deiner, S.G.; Leipzig, R.M.; Friedman, J.I.; Liu, J.; Mazumdar, M.; Memtsoudis, S.G. Modifiable factors associated with postoperative delirium after hip fracture repair: An age-stratified retrospective cohort study. Eur. J. Anaesthesiol. 2020, 37, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Zywiel, M.G.; Hurley, R.T.; Perruccio, A.V.; Hancock-Howard, R.L.; Coyte, P.C.; Rampersaud, Y.R. Health economic implications of perioperative delirium in older patients after surgery for a fragility hip fracture. J. Bone Joint Surg. Am. 2015, 97, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.Y.; Mei, X.C.; Li, C.; Chen, Y.P.; Zheng, H.L.; Wu, Y.J.; Zheng, H.; Liu, L.; Marcantonio, E.R.; Xie, Z.C.; et al. Postoperative Delirium Is Associated with Long-term Decline in Activities of Daily Living. Anesthesiology 2019, 131, 492–500. [Google Scholar] [CrossRef] [Green Version]
- Sprung, J.; Roberts, R.O.; Weingarten, T.N.; Nunes Cavalcante, A.; Knopman, D.S.; Petersen, R.C.; Hanson, A.C.; Schroeder, D.R.; Warner, D.O. Postoperative delirium in elderly patients is associated with subsequent cognitive impairment. Br. J. Anaesth. 2017, 119, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Flikweert, E.R.; Wendt, K.W.; Diercks, R.L.; Izaks, G.J.; Landsheer, D.; Stevens, M.; Reininga, I.H.F. Complications after hip fracture surgery: Are they preventable? Eur. J. Trauma Emerg. Surg. 2018, 44, 573–580. [Google Scholar] [CrossRef]
- Yang, Q.; Wang, J.; Huang, X.; Xu, Y.; Zhang, Y. Incidence and risk factors associated with postoperative delirium following primary elective total hip arthroplasty: A retrospective nationwide inpatient sample database study. BMC Psychiatry 2020, 20, 343. [Google Scholar] [CrossRef]
- Jin, Z.; Hu, J.; Ma, D. Postoperative delirium: Perioperative assessment, risk reduction, and management. Br. J. Anaesth. 2020, 125, 492–504. [Google Scholar] [CrossRef]
- Chu, Z.; Wu, Y.; Dai, X.; Zhang, C.; He, Q. The risk factors of postoperative delirium in general anesthesia patients with hip fracture: Attention needed. Medicine 2021, 100, e26156. [Google Scholar] [CrossRef]
- Lin, Y.J.; Lin, L.Y.; Peng, Y.C.; Zhang, H.R.; Chen, L.W.; Huang, X.Z.; Chen, Q. Association between glucose variability and postoperative delirium in acute aortic dissection patients: An observational study. J. Cardiothorac. Surg. 2021, 16, 82. [Google Scholar] [CrossRef]
- Kotfis, K.; Szylinska, A.; Listewnik, M.; Brykczynski, M.; Ely, E.W.; Rotter, I. Diabetes and elevated preoperative HbA1c level as risk factors for postoperative delirium after cardiac surgery: An observational cohort study. Neuropsychiatr. Dis. Treat. 2019, 15, 511–521. [Google Scholar] [CrossRef] [Green Version]
- van Keulen, K.; Knol, W.; Belitser, S.V.; Zaal, I.J.; van der Linden, P.D.; Heerdink, E.R.; Egberts, T.C.G.; Slooter, A.J.C. Glucose variability during delirium in diabetic and non-diabetic intensive care unit patients: A prospective cohort study. PLoS ONE 2018, 13, e0205637. [Google Scholar] [CrossRef]
- Roberts, G.; Sires, J.; Chen, A.; Thynne, T.; Sullivan, C.; Quinn, S.; Chen, W.S.; Meyer, E. A comparison of the stress hyperglycemia ratio, glycemic gap, and glucose to assess the impact of stress-induced hyperglycemia on ischemic stroke outcome. J. Diabetes 2021, 13, 1034–1042. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.J.; Liao, W.I.; Wang, J.C.; Tsai, C.L.; Lee, J.T.; Peng, G.S.; Lee, C.H.; Hsu, C.W.; Tsai, S.H. Usefulness of glycated hemoglobin A1c-based adjusted glycemic variables in diabetic patients presenting with acute ischemic stroke. Am. J. Emerg. Med. 2017, 35, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Laurila, J.V.; Laakkonen, M.L.; Tilvis, R.S.; Pitkala, K.H. Predisposing and precipitating factors for delirium in a frail geriatric population. J. Psychosom. Res. 2008, 65, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Bickel, H.; Gradinger, R.; Kochs, E.; Forstl, H. High risk of cognitive and functional decline after postoperative delirium. A three-year prospective study. Dement. Geriatr. Cogn. Disord. 2008, 26, 26–31. [Google Scholar] [CrossRef]
- Gual, N.; Garcia-Salmones, M.; Britez, L.; Crespo, N.; Udina, C.; Perez, L.M.; Inzitari, M. The role of physical exercise and rehabilitation in delirium. Eur. Geriatr. Med. 2020, 11, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Y.; Li, Z.Q.; Yang, N.; Han, Y.Z.; Ji, X.J.; Han, D.Y.; Wang, X.X.; Li, Y.; Liu, T.T.; Yuan, F.; et al. Exosome alpha-Synuclein Release in Plasma May be Associated With Postoperative Delirium in Hip Fracture Patients. Front. Aging Neurosci. 2020, 12, 67. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Liu, Y.; Yuan, Y.; Jia, X.; Zhang, W.; Wang, G.; Jia, Y.; Wang, X.; Liu, L.; Li, W.; et al. Effects of general versus subarachnoid anaesthesia on circadian melatonin rhythm and postoperative delirium in elderly patients undergoing hip fracture surgery: A prospective cohort clinical trial. EBioMedicine 2021, 70, 103490. [Google Scholar] [CrossRef]
- Yuan, Y.; Song, Y.A.; Wang, G.; Jia, Y.Y.; Zhou, Y.; Mi, X.N.; Jia, X.X.; Wang, X.X.; Liu, C.; Li, Y.; et al. Effects of general versus regional anaesthesia on circadian melatonin rhythm and its association with postoperative delirium in elderly patients undergoing hip fracture surgery: Study protocol for a prospective cohort clinical trial. BMJ Open 2021, 11, e043720. [Google Scholar] [CrossRef]
- Ringdal, G.I.; Ringdal, K.; Juliebo, V.; Wyller, T.B.; Hjermstad, M.J.; Loge, J.H. Using the Mini-Mental State Examination to Screen for Delirium in Elderly Patients with Hip Fracture. Dement. Geriatr. Cogn. 2011, 32, 394–400. [Google Scholar] [CrossRef]
- Liu, M.; Yue, Y.H.; He, Y. Association between chronic obstructive pulmonary disease and activity of daily living among oldest-old in China: Based on Chinese Longitudinal Health Longevity Survey. Int. J. Chronic. Obstr. 2019, 14, 1959–1966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuhaus, V.; King, J.; Hageman, M.G.; Ring, D.C. Charlson comorbidity indices and in-hospital deaths in patients with hip fractures. Clin. Orthop. Relat. Res. 2013, 471, 1712–1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, D.J.; Goyal, A.; Bansal, P.; Garmon, E.H. American Society of Anesthesiologists Classification. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Chamberlain, J.J.; Rhinehart, A.S.; Shaefer, C.F., Jr.; Neuman, A. Diagnosis and Management of Diabetes: Synopsis of the 2016 American Diabetes Association Standards of Medical Care in Diabetes. Ann. Intern. Med. 2016, 164, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, S.; Boulton, A.J.; Dyck, P.J.; Freeman, R.; Horowitz, M.; Kempler, P.; Lauria, G.; Malik, R.A.; Spallone, V.; Vinik, A.; et al. Diabetic neuropathies: Update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 2010, 33, 2285–2293. [Google Scholar] [CrossRef] [Green Version]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, F.G.; Hiatt, W.R.; Jonsson, B.; Lacroix, P.; et al. Measurement and interpretation of the ankle-brachial index: A scientific statement from the American Heart Association. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef] [Green Version]
- Assoc, A.D. Glycemic Targets: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41, S55–S64. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Yang, X.; Meng, K.; Zeng, Z.; Ma, B.; Liu, X.; Qi, B.; Cui, S.; Cao, P.; Yang, Y. Stress-induced hyperglycemia after hip fracture and the increased risk of acute myocardial infarction in nondiabetic patients. Diabetes Care 2013, 36, 3328–3332. [Google Scholar] [CrossRef] [Green Version]
- Liao, W.I.; Wang, J.C.; Lin, C.S.; Yang, C.J.; Hsu, C.C.; Chu, S.J.; Chu, C.M.; Tsai, S.H. Elevated Glycemic Gap Predicts Acute Respiratory Failure and In-hospital Mortality in Acute Heart Failure Patients with Diabetes. Sci. Rep. 2019, 9, 6279. [Google Scholar] [CrossRef] [Green Version]
- Hsing, S.C.; Lin, C.; Chen, J.T.; Chen, Y.H.; Fang, W.H. Glycemic Gap as a Useful Surrogate Marker for Glucose Variability and Progression of Diabetic Retinopathy. J. Pers Med. 2021, 11, 799. [Google Scholar] [CrossRef]
- Liao, W.I.; Lin, C.S.; Lee, C.H.; Wu, Y.C.; Chang, W.C.; Hsu, C.W.; Wang, J.C.; Tsai, S.H. An Elevated Glycemic Gap is Associated with Adverse Outcomes in Diabetic Patients with Acute Myocardial Infarction. Sci. Rep. 2016, 6, 27770. [Google Scholar] [CrossRef]
- Leung, J.; Leung, V.; Leung, C.M.; Pan, P.C. Clinical utility and validation of two instruments (the Confusion Assessment Method Algorithm and the Chinese version of Nursing Delirium Screening Scale) to detect delirium in geriatric inpatients. Gen. Hosp. Psychiatry 2008, 30, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.Y.; Wu, Y.J.; Li, C.; Fu, S.K.; Li, G.D.; Zhu, Y.B.; Swain, C.A.; Marcantonio, E.R.; Xie, Z.C.; Shen, Y. Using the Chinese version of Memorial Delirium Assessment Scale to describe postoperative delirium after hip surgery. Front. Aging Neurosci. 2014, 6, 297. [Google Scholar] [CrossRef] [PubMed]
- Sieber, F.E.; Neufeld, K.J.; Gottschalk, A.; Bigelow, G.E.; Oh, E.S.; Rosenberg, P.B.; Mears, S.C.; Stewart, K.J.; Ouanes, J.P.; Jaberi, M.; et al. Effect of Depth of Sedation in Older Patients Undergoing Hip Fracture Repair on Postoperative Delirium: The STRIDE Randomized Clinical Trial. JAMA Surg. 2018, 153, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Haynes, M.S.; Alder, K.D.; Toombs, C.; Amakiri, I.C.; Rubin, L.E.; Grauer, J.N. Predictors and Sequelae of Postoperative Delirium in a Geriatric Patient Population With Hip Fracture. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2021, 5, e20.00221. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.G.; Qin, Y.F.; Wan, X.; Song, L.C.; Li, Z.J.; Li, H. Incidence and risk factors of postoperative delirium in the elderly patients with hip fracture. J. Orthop. Surg. Res. 2018, 13, 186. [Google Scholar] [CrossRef] [Green Version]
- Subramaniam, B.; Lerner, A.; Novack, V.; Khabbaz, K.; Paryente-Wiesmann, M.; Hess, P.; Talmor, D. Increased glycemic variability in patients with elevated preoperative HbA1C predicts adverse outcomes following coronary artery bypass grafting surgery. Anesth. Analg. 2014, 118, 277–287. [Google Scholar] [CrossRef]
- Viderman, D.; Brotfain, E.; Bilotta, F.; Zhumadilov, A. Risk Factors and Mechanisms of Postoperative Delirium After Intracranial Neurosurgical Procedures. Asian J. Anesthesiol. 2020, 58, 5–13. [Google Scholar] [CrossRef]
- van Keulen, K.; Knol, W.; Belitser, S.V.; van der Linden, P.D.; Heerdink, E.R.; Egberts, T.C.G.; Slooter, A.J.C. Diabetes and Glucose Dysregulation and Transition to Delirium in ICU Patients. Crit Care Med. 2018, 46, 1444–1449. [Google Scholar] [CrossRef]
- Scheen, A.J. Central nervous system: A conductor orchestrating metabolic regulations harmed by both hyperglycaemia and hypoglycaemia. Diabetes Metab. 2010, 36, S31–S38. [Google Scholar] [CrossRef]
- Languren, G.; Montiel, T.; Julio-Amilpas, A.; Massieu, L. Neuronal damage and cognitive impairment associated with hypoglycemia: An integrated view. Neurochem. Int. 2013, 63, 331–343. [Google Scholar] [CrossRef]
- Krinsley, J.S.; Meyfroidt, G.; van den Berghe, G.; Egi, M.; Bellomo, R. The impact of premorbid diabetic status on the relationship between the three domains of glycemic control and mortality in critically ill patients. Curr. Opin. Clin. Nutr. 2012, 15, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Whitmer, R.A.; Karter, A.J.; Yaffe, K.; Quesenberry, C.P.; Selby, J.V. Hypoglycemic Episodes and Risk of Dementia in Older Patients With Type 2 Diabetes Mellitus. JAMA-J. Am. Med. Assoc. 2009, 301, 1565–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stollery, B.; Christian, L. Glucose improves object-location binding in visual-spatial working memory. Psychopharmacology 2016, 233, 529–547. [Google Scholar] [CrossRef] [Green Version]
- Saager, L.; Duncan, A.E.; Yared, J.P.; Hesler, B.D.; You, J.; Deogaonkar, A.; Sessler, D.I.; Kurz, A. Intraoperative Tight Glucose Control Using Hyperinsulinemic Normoglycemia Increases Delirium after Cardiac Surgery. Anesthesiology 2015, 122, 1214–1223. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.; Browndyke, J.; Mathew, J.P. Intraoperative Glycemic Control to Prevent Delirium after Cardiac Surgery Steering a Course between Scylla and Charybdis. Anesthesiology 2015, 122, 1186–1188. [Google Scholar] [CrossRef] [Green Version]
- Sinclair, A.; Dunning, T.; Rodriguez-Manas, L. Diabetes in older people: New insights and remaining challenges. Lancet Diabetes Endocrinol. 2015, 3, 275–285. [Google Scholar] [CrossRef]
- Geijselaers, S.L.C.; Sep, S.J.S.; Stehouwer, C.D.A.; Biessels, G.J. Glucose regulation, cognition, and brain MRI in type 2 diabetes: A systematic review. Lancet Diabetes Endocrinol. 2015, 3, 75–89. [Google Scholar] [CrossRef]
- Rau, C.S.; Wu, S.C.; Chen, Y.C.; Chien, P.C.; Hsieh, H.Y.; Kuo, P.J.; Hsieh, C.H. Mortality Rate Associated with Admission Hyperglycemia in Traumatic Femoral Fracture Patients Is Greater Than Non-Diabetic Normoglycemic Patients but Not Diabetic Normoglycemic Patients. Int. J. Environ. Res. Public Health 2018, 15, 28. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.Y.; Chou, R.H.; Kuo, C.S.; Chao, T.F.; Wu, C.H.; Tsai, Y.L.; Lu, Y.W.; Kuo, M.R.; Huang, P.H.; Lin, S.J. The paradox of the glycemic gap: Does relative hypoglycemia exist in critically ill patients? Clin. Nutr. 2021, 40, 4654–4661. [Google Scholar] [CrossRef]
- Jensen, A.V.; Egelund, G.B.; Andersen, S.B.; Petersen, P.T.; Benfield, T.; Witzenrath, M.; Rohde, G.; Ravn, P.; Faurholt-Jepsen, D.; Dreher, M.; et al. The Glycemic Gap and 90-Day Mortality in Community-acquired Pneumonia A Prospective Cohort Study. Ann. Am. Thorac. Soc. 2019, 16, 1518–1526. [Google Scholar] [CrossRef]
- Lee, M.; Lim, J.S.; Kim, Y.; Lee, J.H.; Kim, C.H.; Lee, S.H.; Jang, M.U.; Oh, M.S.; Lee, B.C.; Yu, K.H. Effects of Glycemic Gap on Post-Stroke Cognitive Impairment in Acute Ischemic Stroke Patients. Brain Sci. 2021, 11, 612. [Google Scholar] [CrossRef] [PubMed]
- Duaso, E.; Formiga, F.; Marimon, P.; Sandiumenge, M.; Salgado, M.T.; Murga, V.; Gamboa, A.; Rodriguez, C.; Castella, J.; Escalante, E.; et al. Advantages of care for patients with hip fractures in the acute geriatric unit: Hip study Anoia. Geriatr. Gerontol. Int. 2018, 18, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, M.; Izawa, K.P.; Satomi-Kobayashi, S.; Kitamura, A.; Tsuboi, Y.; Komaki, K.; Ono, R.; Sakai, Y.; Tanaka, H.; Okita, Y. Preoperative exercise capacity is associated with the prevalence of postoperative delirium in elective cardiac surgery. Aging Clin. Exp. Res. 2018, 30, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Oshima, H.; Shimizu, M.; Kobayashi, K.; Matsui, S.; Nishida, Y.; Usui, A. Preoperative 6-Minute Walk Distance Is Associated With Postoperative Cognitive Dysfunction. Ann. Thorac. Surg. 2018, 106, 505–512. [Google Scholar] [CrossRef] [PubMed]
- de Asteasu, M.L.S. Effect of Exercise Intervention on Functional Decline in Very Elderly Patients During Acute Hospitalization: A Randomized Clinical Trial (vol 179, pg 28, 2018). JAMA Intern. Med. 2019, 179, 127. [Google Scholar] [CrossRef] [Green Version]
- Buchman, A.S.; Yu, L.; Wilson, R.S.; Lim, A.; Dawe, R.J.; Gaiteri, C.; Leurgans, S.E.; Schneider, J.A.; Bennett, D.A. Physical activity, common brain pathologies, and cognition in community-dwelling older adults. Neurology 2019, 92, e811–e822. [Google Scholar] [CrossRef]
- Zhao, G.; Ford, E.S.; Li, C.; Balluz, L.S. Physical activity in U.S. older adults with diabetes mellitus: Prevalence and correlates of meeting physical activity recommendations. J. Am. Geriatr. Soc. 2011, 59, 132–137. [Google Scholar] [CrossRef]
- Healy, G.N.; Winkler, E.A.; Owen, N.; Anuradha, S.; Dunstan, D.W. Replacing sitting time with standing or stepping: Associations with cardio-metabolic risk biomarkers. Eur. Heart J. 2015, 36, 2643–2649. [Google Scholar] [CrossRef] [Green Version]
- Boujibar, F.; Gillibert, A.; Gravier, F.E.; Gillot, T.; Bonnevie, T.; Cuvelier, A.; Baste, J.M. Performance at stair-climbing test is associated with postoperative complications after lung resection: A systematic review and meta-analysis. Thorax 2020, 75, 791–797. [Google Scholar] [CrossRef]
- Susano, M.J.; Grasfield, R.H.; Friese, M.; Rosner, B.; Crosby, G.; Bader, A.M.; Kang, J.D.; Smith, T.R.; Lu, Y.; Groff, M.W.; et al. Brief Preoperative Screening for Frailty and Cognitive Impairment Predicts Delirium after Spine Surgery. Anesthesiology 2020, 133, 1184–1191. [Google Scholar] [CrossRef]
- Liu, H.; Jiao, J.; Zhu, C.; Zhu, M.; Wen, X.; Jin, J.; Wang, H.; Lv, D.; Zhao, S.; Wu, X.; et al. Potential associated factors of functional disability in Chinese older inpatients: A multicenter cross-sectional study. BMC Geriatr. 2020, 20, 319. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Non-POD (n = 257) | POD (n = 52) | p |
|---|---|---|---|
| Baseline features | |||
| Male (%) | 68 (26.46%) | 16 (30.77%) | 0.524 |
| Age (years) | 79 (73, 83) | 81 (75, 85) | 0.146 |
| BMI (kg m−2) | 23.44 (21.12, 26.20) | 23.67 (22.09, 26.19) | 0.524 |
| History of smoking (%) | 49 (19.07%) | 11 (21.15%) | 0.729 |
| History of alcohol (%) | 23 (8.95%) | 7 (13.46%) | 0.316 |
| Education (years) | 9 (4, 12) | 9 (6, 12) | 0.628 |
| Preoperative MMSE (points) | 26 (23, 28) | 25.5 (21, 28) | 0.065 |
| Preoperative MMSE < 24 | 172 (66.9%) | 30 (57.7%) | 0.202 |
| ADL (points) | 6 (6, 6) | 6 (4, 6) | 0.237 |
| ACCI (points) | 3 (2, 4) | 4 (3, 5) | 0.003 |
| ASA classification (%) | 0.667 | ||
| I | 4 (1.65%) | 0 (0%) | |
| II | 177 (68.78%) | 34 (65.38%) | |
| III | 76 (29.57%) | 18 (34.62%) | |
| Baseline laboratory | |||
| Hemoglobin (mg L−1) | 122 (110, 131) | 120 (105, 126) | 0.195 |
| Albumin (g L−1) | 41.4 (39.4, 43.4) | 40.9 (39.0, 42.1) | 0.063 |
| Abnormal K+ (%) | 26 (10.12%) | 7 (13.46%) | 0.470 |
| Abnormal Na+ (%) | 28 (10.89%) | 3 (5.77%) | 0.287 |
| Abnormal Cl− (%) | 57 (22.18%) | 9 (17.31%) | 0.502 |
| Abnormal Ca2+ (%) | 129 (59.19%) | 29 (55.77%) | 0.423 |
| Medical history | |||
| T2DM | 69 (26.85%) | 23 (44.23%) | 0.012 |
| Hypertension (%) | 146 (56.81%) | 36 (69.23%) | 0.097 |
| Coronary heart disease (%) | 58 (22.57%) | 13 (25.00%) | 0.704 |
| Kidney failure (%) | 9 (3.50%) | 3 (5.77%) | 0.705 |
| Stroke history (%) | 46 (17.90%) | 11 (21.15%) | 0.608 |
| Cardiac interventional therapy (%) | 6 (2.33%) | 4 (7.69%) | 0.118 |
| Variable | Non-POD (n = 257) | POD (n = 52) | p |
|---|---|---|---|
| Time from injury to operation (hours) | 95 (70, 123) | 81 (59, 145) | 0.499 |
| Anesthesia method (%) | 0.001 | ||
| SA | 124 (48.25%) | 20 (38.46%) | |
| GA | 99 (38.52%) | 32 (61.54%) | |
| SA + GA | 34 (13.23%) | 0 (0%) | |
| Surgery type (%) | 0.020 | ||
| Intramedullary needle | 132 (51.36%) | 25 (48.08%) | |
| THA | 30 (11.67%) | 11 (21.15%) | |
| Hemiarthroplasty | 64 (24.90%) | 16 (30.77%) | |
| Hollow screw fixation | 31 (12.06%) | 0 (0%) | |
| Anesthesia time (minutes) | 90 (75, 110) | 90 (79, 116) | 0.454 |
| Surgery time (minutes) | 60 (40, 80) | 60 (38, 90) | 0.822 |
| Variable | Non-POD (n = 257) | POD (n = 52) | p |
|---|---|---|---|
| Postoperative complications (%) | 117 (45.53%) | 27 (51.92%) | 0.399 |
| Hypoxemia (%) | 30 (11.67%) | 5 (9.62%) | 0.669 |
| Hypokalemia (%) | 14 (5.45%) | 6 (11.54%) | 0.187 |
| Pulmonary infection (%) | 11 (4.28%) | 8 (15.38%) | 0.006 |
| Deep venous thrombosis (%) | 17 (6.61%) | 2 (3.85%) | 0.659 |
| Respiratory failure (%) | 16 (6.23%) | 2 (3.85%) | 0.731 |
| Urinary infection (%) | 11 (4.28%) | 4 (7.69%) | 0.49 |
| Hypoproteinemia (%) | 10 (3.89%) | 3 (5.77%) | 0.813 |
| Hospitalization time (days) | 2 (2, 3) | 3 (2, 5) | <0.001 |
| Variable | Non-POD (n = 257) | POD (n = 52) | p |
|---|---|---|---|
| Preoperative FBG (mmol L−1) | 7.9 (6.6, 10.1) | 7.5 (6.65, 8.9) | 0.156 |
| HbA1c (%) | 5.8 (5.4, 6.5) | 6.0 (5.5, 6.7) | 0.313 |
| GG (mg dL−1) | 37.9 (10.5, 71.32) | 28.5 (8.96, 58.27) | 0.245 |
| Patient without T2DM a | 188 (73.15%) | 29 (55.77%) | |
| Preoperative FBG (mmol L−1) a | 7.4 (6.8, 8.8) | 7.1 (5.9, 7.9) | 0.084 |
| HbA1c (%) a | 5.6 (5.3, 5.9) | 5.7 (5.32, 6.0) | 0.746 |
| GG (mg dL−1) a | 22.7 (8.8, 41.2) | 14.4 (6.66, 28.6) | 0.112 |
| SIH (%) a | 90 (47.87%) | 14 (48.28%) | 0.834 |
| Patient with T2DM | 69 (26.85%) | 23 (44.23%) | |
| Preoperative FBG (mmol L−1) b | 10.6 (8.7, 13.6) | 8.4 (7.5, 10.1) | 0.015 |
| HbA1c (%) b | 6.9 (6.3, 8.0) | 6.7 (6.0, 7.5) | 0.285 |
| GG (mg dL−1) b | 37.9 (10.5, 71.3) | 28.5 (9.0, 58.3) | 0.245 |
| Insulin administration (%) b | 19 (27.54%) | 5 (21.74%) | 0.677 |
| Hypoglycemia (%) b | 5 (7.24%) | 1 (4.35%) | 1.000 |
| Diabetes duration, years b | 8 (5, 12) | 10 (9, 12) | 0.119 |
| DPN (%) b | 15 (21.74%) | 3 (13.04%) | 0.544 |
| DPVD (%) b | 4 (5.80%) | 3 (13.04%) | 0.496 |
| Variable | Non-POD (n = 250) | POD (n = 49) | p |
|---|---|---|---|
| Distance walked (meters) | 1000 (500, 2000) | 500 (200, 1000) | <0.001 |
| Stair climbing (floors) | 2 (1, 4) | 1 (0, 2) | <0.001 |
| Use of mobility aid (%) | 61 (23.74%) | 23 (44.23%) | 0.002 |
| Exercise capacity (%) | 0.001 | ||
| Poor | 25 (10.00%) | 12 (24.49%) | |
| Ordinary | 95 (38.00%) | 24 (48.98%) | |
| Good | 130 (52.00%) | 13 (26.53%) |
| Variable | B | SE | Walds | p | OR [95% CI] |
|---|---|---|---|---|---|
| Male | −0.211 | 0.332 | 0.405 | 0.525 | 0.810 [0.422, 1.552] |
| Age, per year | 0.031 | 0.023 | 1.820 | 0.177 # | 1.031 [0.986, 1.079] |
| BMI, per kg/m2 | 0.030 | 0.043 | 0.489 | 0.484 | 1.030 [0.948, 1.120] |
| Smoker | 0.130 | 0.375 | 0.120 | 0.729 | 1.139 [0.546, 2.374] |
| Alcohol Drinker | 0.459 | 0.461 | 0.995 | 0.320 | 1.583 [0.641, 3.909] |
| Education, per year | 0.014 | 0.028 | 0.479 | 0.632 | 1.014 [0.959, 1.072] |
| Preoperative MMSE, per point | −0.061 | 0.027 | 5.111 | 0.024 # | 0.941 [0.892, 0.992] |
| ADL, per score | −0.192 | 0.092 | 4.365 | 0.037 # | 0.825 [0.689, 0.988] |
| ACCI, per score | 0.268 | 0.090 | 8.902 | 0.003 # | 1.307 [1.096, 1.559] |
| ASA classification | 0.232 | 0.322 | 0.518 | 0.472 | 1.261 [0.671, 2.370] |
| Time from injury to surgery, per hour | 0.001 | 0.001 | 2.414 | 0.120 # | 1.001 [1.000,1.002] |
| Anesthesia time, per min | 0.000 | 0.005 | 0.009 | 0.925 | 1.000 [0.991, 1.010] |
| Surgery time, per min | −0.003 | 0.005 | 0.291 | 0.590 | 0.997 [0.987, 1.007] |
| Hemoglobin, per mg L−1 | −0.012 | 0.008 | 2.656 | 0.103 # | 0.988 [0.973, 1.003] |
| Albumin, per g L−1 | −0.087 | 0.046 | 3.658 | 0.056 # | 0.917 [0.838, 1.002] |
| Hypertension | 0.537 | 0.326 | 2.715 | 0.099 # | 1.711 [0.903, 3.239] |
| Coronary heart disease | 0.134 | 0.353 | 0.144 | 0.704 | 1.144 [0.572, 2.286] |
| Kidney failure | 0.523 | 0.685 | 0.583 | 0.445 | 1.687 [0.441, 6.456] |
| Stroke history | 0.193 | 0.377 | 0.263 | 0.608 | 1.213 [0.580, 2.538] |
| Cardiac interventional therapy | 1.249 | 0.664 | 3.532 | 0.060 # | 3.486 [0.948, 12.821] |
| T2DM | 0.771 | 0.313 | 6.072 | 0.014 # | 2.161 [1.171, 3.988] |
| Diabetes duration, per year | 0.031 | 0.032 | 0.991 | 0.319 | 1.032 [0.970, 1.098] |
| DPN | −0.616 | 0.684 | 0.810 | 0.368 | 0.540 [0.141, 2.066] |
| DPVD | 0.891 | 0.805 | 1.224 | 0.269 | 2.437 [0.503,11.818] |
| Insulin administration, yes | 0.283 | 0.527 | 0.288 | 0.592 | 1.327 [0.472, 0.731] |
| Preoperative FBG, per mmol L−1 | 0.013 | 0.059 | 2.438 | 0.118 # | 0.913 [0.814,1.024] |
| HbA1c, per% | 0.094 | 0.329 | 0.156 | 0.692 | 1.139 [0.598, 2.171] |
| Exercise capacity | −0.798 | 0.222 | 12.908 | 0.000 # | 0.450 [0.292, 0.696] |
| Distance walked, per 100 m | −0.040 | 0.015 | 7.264 | 0.007 # | 0.961 [0.933, 0.989] |
| Use of mobility aid, yes | 0.971 | 0.320 | 9.217 | 0.002 # | 2.639 [1.411, 4.939] |
| Stair climbing, per floor | −0.386 | 0.109 | 12.584 | 0.000 # | 0.680 [0.550, 0.841] |
| Variable | B | SE | Wals | p | OR [95% CI] |
|---|---|---|---|---|---|
| Preoperative MMSE, per score | −0.063 | 0.330 | 3.654 | 0.056 | 0.939 [0.881, 1.002] |
| ACCI, per score | 0.239 | 0.115 | 4.319 | 0.038 | 1.270 [1.014, 1.592] |
| T2DM, yes | 1.296 | 0.405 | 10.215 | 0.001 | 3.654 [1.651, 8.089] |
| Preoperative FBG, per mmol L−1 | −0.218 | 0.077 | 8.076 | 0.004 | 0.804 [0.692, 0.935] |
| Stair climbing, per floor | −0.344 | 0.117 | 8.666 | 0.003 | 0.709 [0.564, 0.891] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, K.; Song, Y.; Yuan, Y.; Li, Z.; Wang, X.; Zhang, W.; Li, Y.; Mi, X.; Han, D.; Rong, Y.; et al. Type 2 Diabetes Mellitus with Tight Glucose Control and Poor Pre-Injury Stair Climbing Capacity May Predict Postoperative Delirium: A Secondary Analysis. Brain Sci. 2022, 12, 951. https://doi.org/10.3390/brainsci12070951
Liu K, Song Y, Yuan Y, Li Z, Wang X, Zhang W, Li Y, Mi X, Han D, Rong Y, et al. Type 2 Diabetes Mellitus with Tight Glucose Control and Poor Pre-Injury Stair Climbing Capacity May Predict Postoperative Delirium: A Secondary Analysis. Brain Sciences. 2022; 12(7):951. https://doi.org/10.3390/brainsci12070951
Chicago/Turabian StyleLiu, Kaixi, Yanan Song, Yi Yuan, Zhengqian Li, Xiaoxiao Wang, Wenchao Zhang, Yue Li, Xinning Mi, Dengyang Han, Yulan Rong, and et al. 2022. "Type 2 Diabetes Mellitus with Tight Glucose Control and Poor Pre-Injury Stair Climbing Capacity May Predict Postoperative Delirium: A Secondary Analysis" Brain Sciences 12, no. 7: 951. https://doi.org/10.3390/brainsci12070951