
The Surgical Risk Factors of Giant Intracranial Meningiomas: A Multi-Centric Retrospective Analysis of Large Case Serie

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Eligibility
- -
- Patients with confirmed histological diagnosis of meningioma performed according to the updated version of the 2021 WHO guidelines [22] at their first surgery;
- -
- patients were included in the study if their pre- and postoperative magnetic resonance imaging (MRI) was either performed at our institution or available on the picture archiving and communication system (PACS) for review;
- -
- patients were included if, in the postoperative period, could undergo a standard clinical and radiological follow-up starting from the 30th day after surgery; patients were excluded for incomplete or wrong data in clinical, radiological, and surgical records and/or being lost to follow-up;
- -
- the estimated target of the surgical procedure was the total or subtotal resection of the lesions; no biopsies were included.
- -
- Tumors classified as giant meningiomas (Group A): The contrast-enhanced lesion measured at least 5 cm along the major diameter in T1-weighted images with MRI;
- -
- tumors classified as medium/large meningiomas (Group B): The contrast-enhanced lesion measured less than 5 cm along the major diameter in T1-weighted images with MRI.
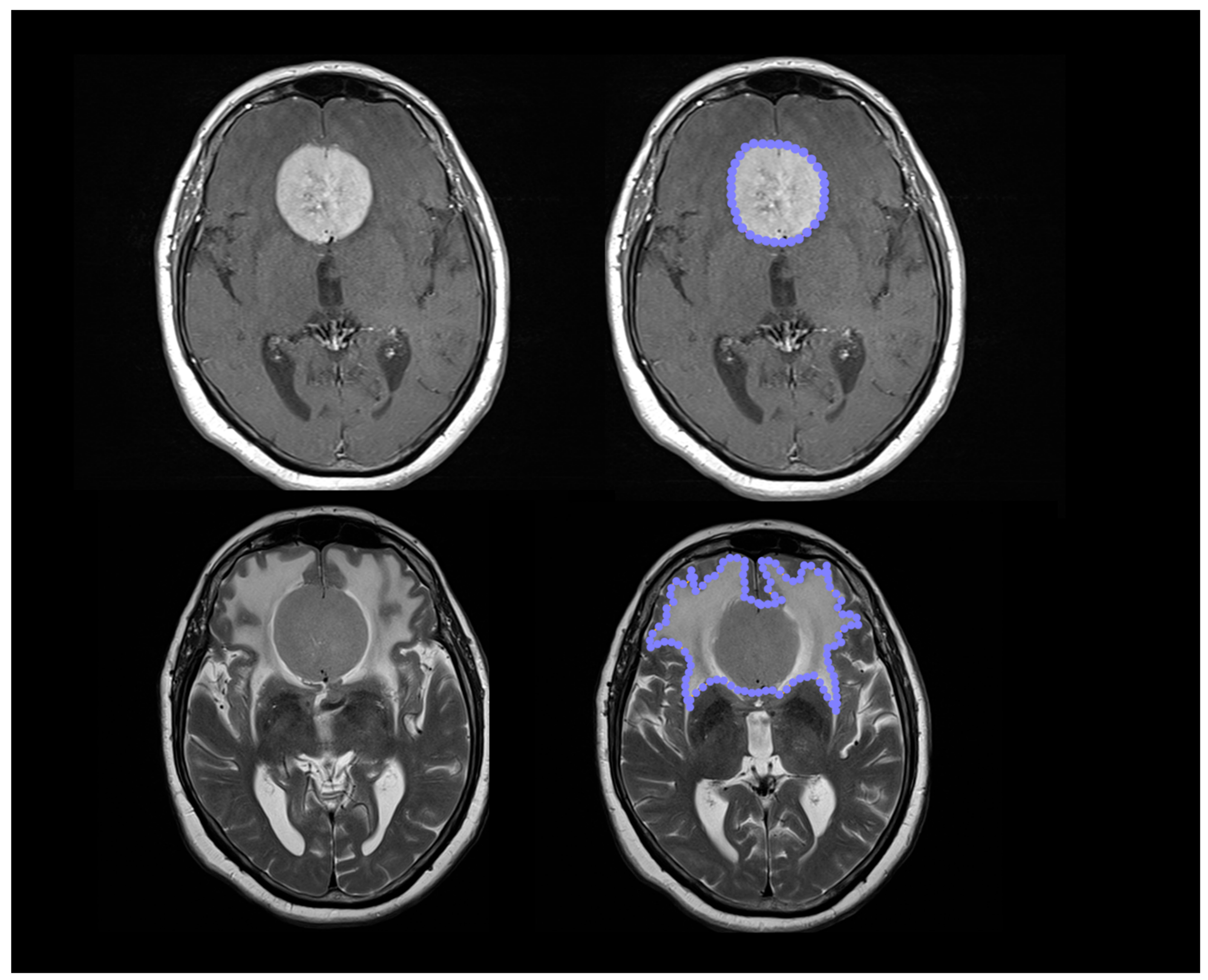
2.2. Imaging Analysis and ROI-Drawing Process
2.3. Surgical Treatment
2.4. Statistical Methods
2.5. The Potential Source of Bias and Study Size
3. Results
3.1. Descriptive Data
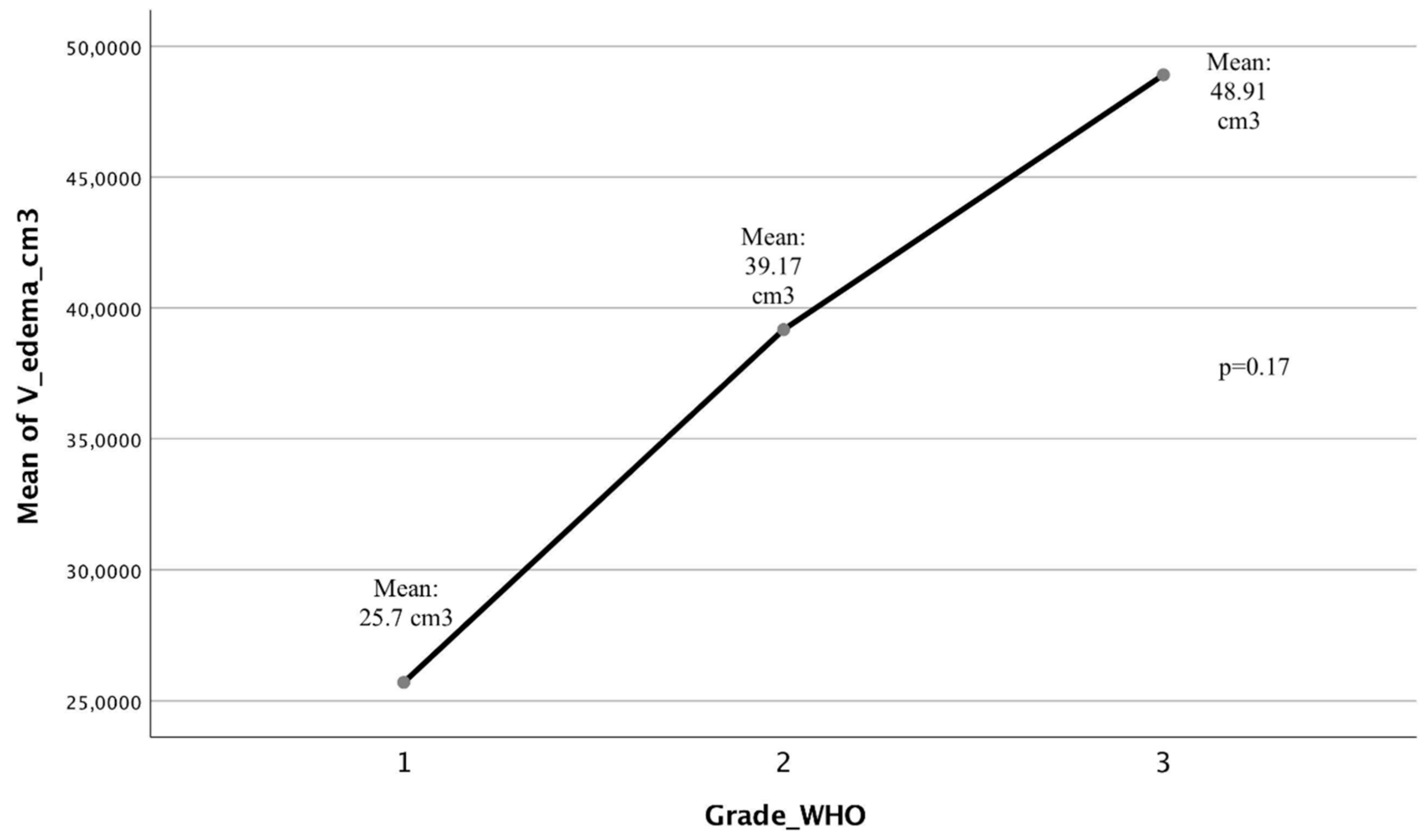
3.2. Histochemical Comparison Analysis between the Two Groups
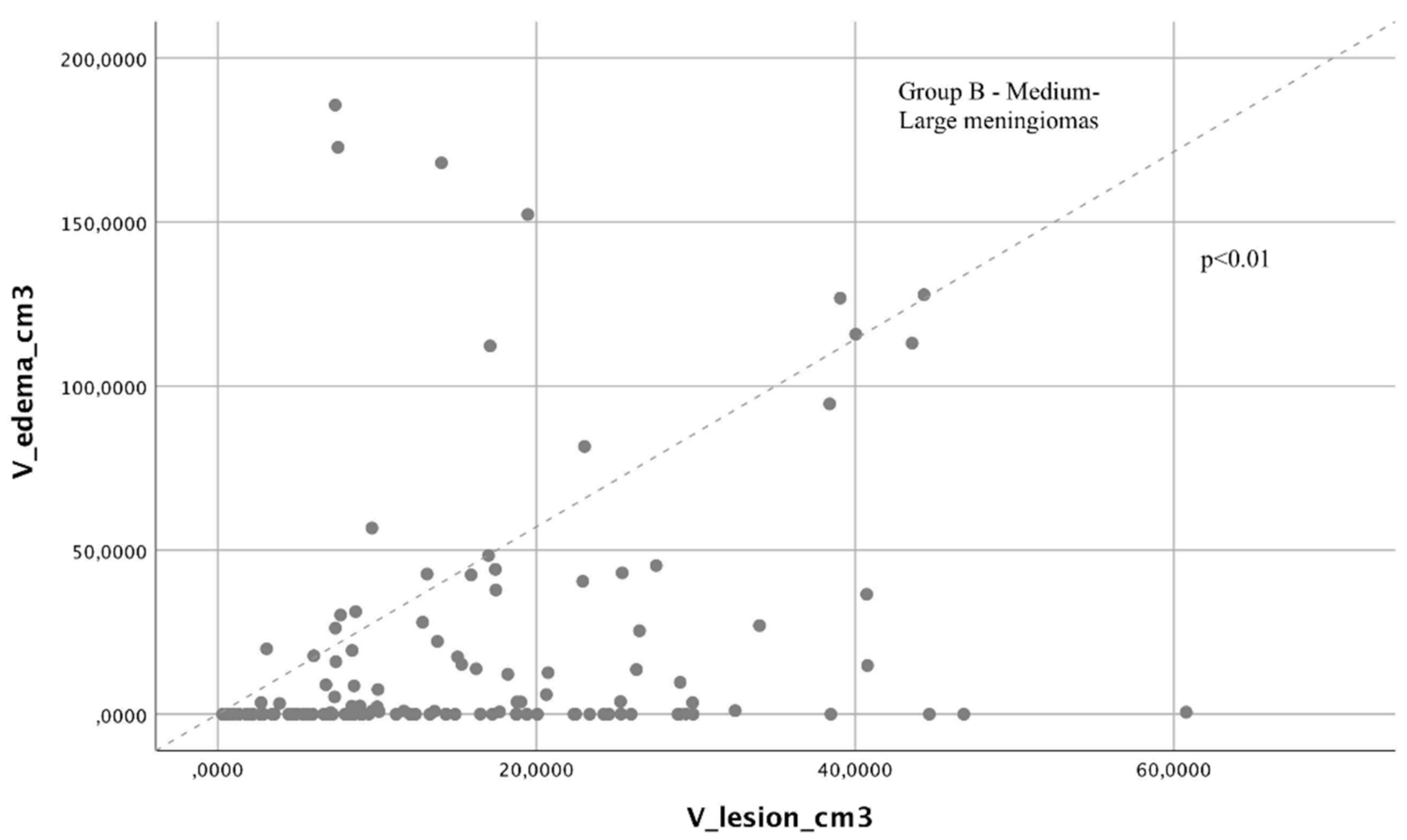
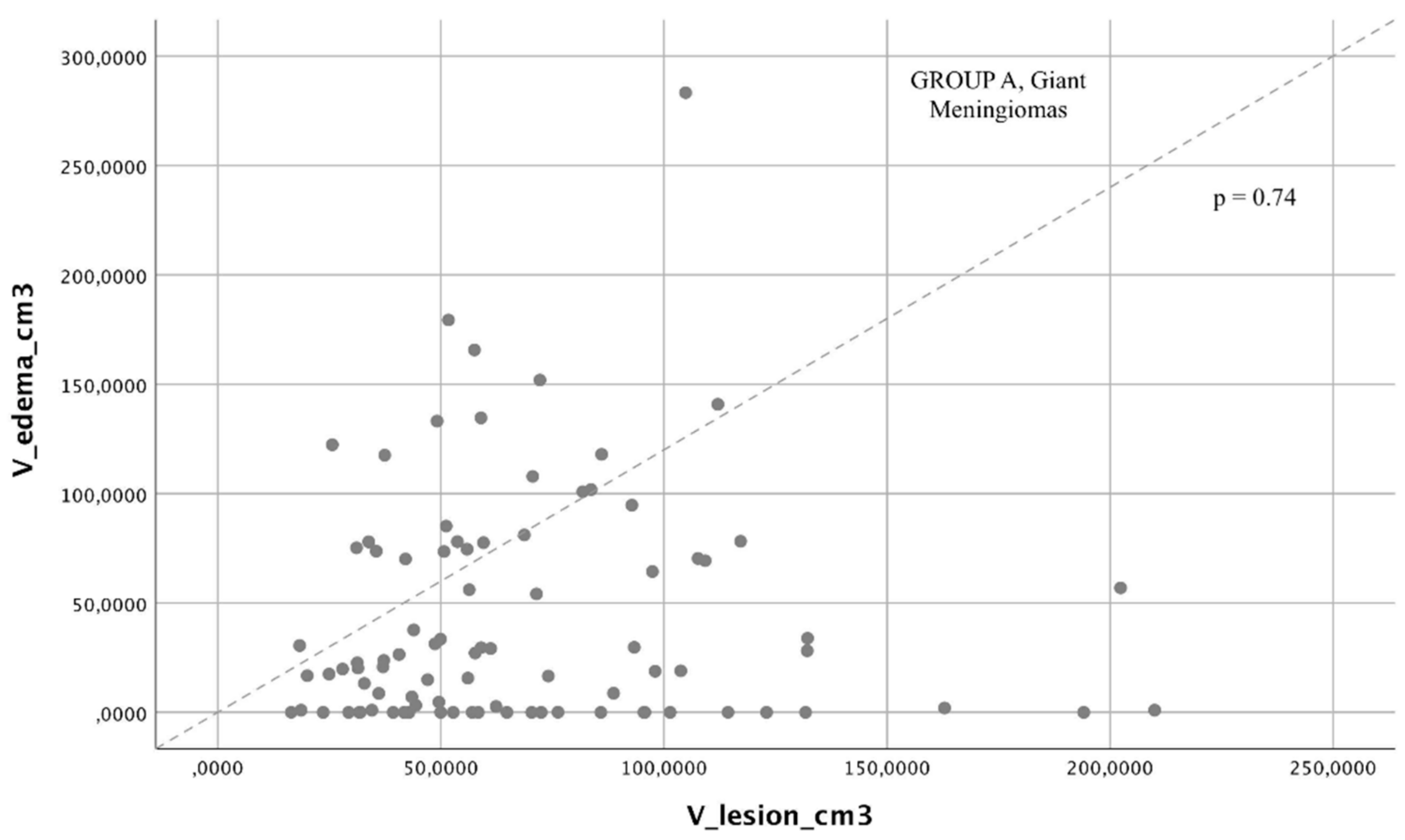
3.3. Radiological Comparison Analysis between the Two Groups
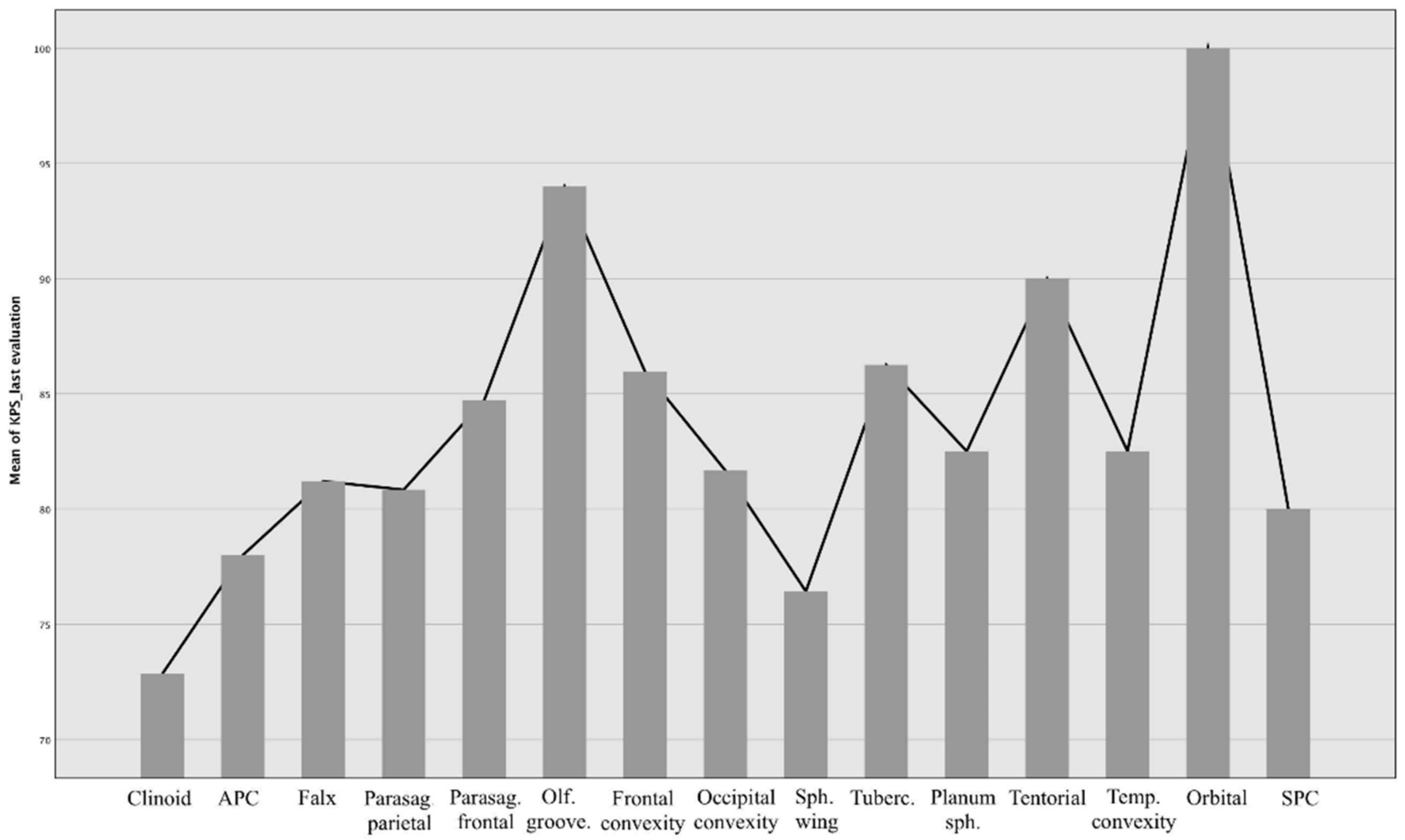
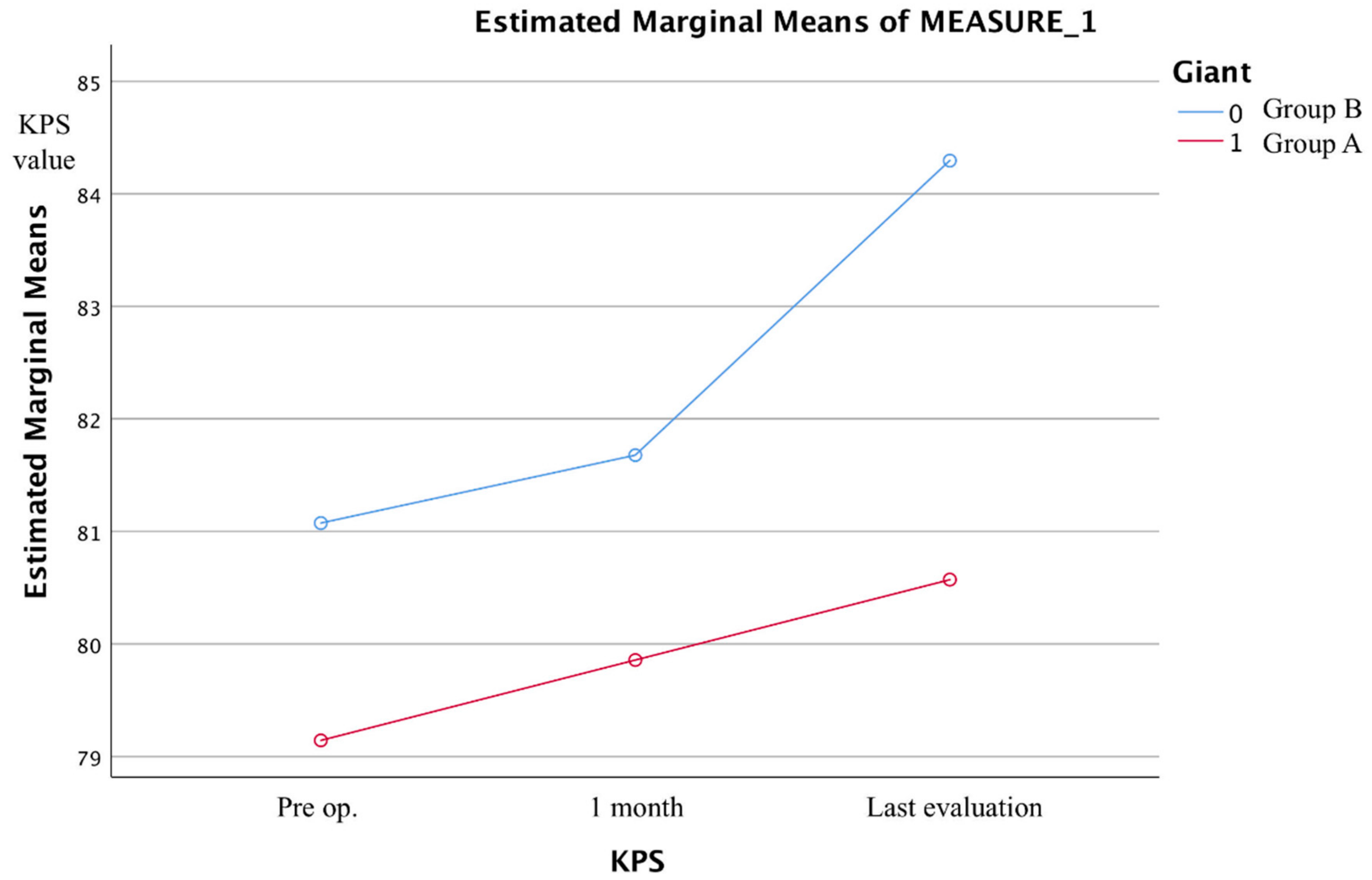
3.4. Outcome Data and Main Results
4. Discussion
5. Limitations and Further Studies
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Champagne, P.-O.; Lemoine, E.; Bojanowski, M.W. Surgical management of giant sphenoid wing meningiomas encasing major cerebral arteries. Neurosurg. Focus 2018, 44, E12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuratsu, J.-I.; Kochi, M.; Ushio, Y. Incidence and clinical features of asymptomatic meningiomas. J. Neurosurg. 2000, 92, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lu, D.; Feng, D.; Cheng, H.; Huang, Q.; Zhao, H.; Chen, P.; Qin, H.; Cai, Q. Management of incidental anterior skull base large and giant meningiomas in elderly patients. J. Neuro-Oncol. 2020, 148, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Gazzeri, R.; Galarza, M.; Gazzeri, G. Giant olfactory groove meningioma: Ophthalmological and cognitive outcome after bifrontal microsurgical approach. Acta Neurochir. 2008, 150, 1117–1126. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.-P.; Wang, A.D.; Tsai, M.-D. Resection of Giant Olfactory Groove Meningioma with Extradural Devascularization. Skull Base 2002, 12, 027–032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sughrue, M.E.; McDermott, M.W.; Parsa, A.T. Vision salvage after resection of a giant meningioma in a patient with a loss in light perception. J. Neurosurg. 2009, 110, 109–111. [Google Scholar] [CrossRef]
- Nishiguchi, T.; Iwakiri, T.; Hayasaki, K.; Ohsawa, M.; Yoneda, T.; Mitsuhashi, Y.; Nishio, A.; Dousset, V.; Miki, Y. Post-embolisation susceptibility changes in giant meningiomas: Multiparametric histogram analysis using non-contrast-enhanced susceptibility-weighted PRESTO, diffusion-weighted and perfusion-weighted imaging. Eur. Radiol. 2012, 23, 551–561. [Google Scholar] [CrossRef]
- Karthigeyan, M.; Rajasekhar, R.; Salunke, P.; Singh, A. Modified unilateral approach for mid-third giant bifalcine meningiomas: Resection using an oblique surgical trajectory and falx window. Acta Neurochir. 2018, 161, 327–332. [Google Scholar] [CrossRef]
- Sanai, N.; McDermott, M.W. A modified far-lateral approach for large or giant meningiomas of the posterior fossa. J. Neurosurg. 2010, 112, 907–912. [Google Scholar] [CrossRef] [Green Version]
- Xiao, X.; Zhang, L.; Wu, Z.; Zhang, J.; Jia, G.; Tang, J.; Meng, G. Surgical resection of large and giant petroclival meningiomas via a modified anterior transpetrous approach. Neurosurg. Rev. 2013, 36, 587–594. [Google Scholar] [CrossRef] [Green Version]
- Aref, M.; Kunigelis, K.E.; Yang, A.; Subramanian, P.S.; Ramakrishnan, V.R.; Youssef, A.S. The Effect of Preoperative Direct Ligation of Ethmoidal Arteries on the Perioperative Outcomes of Large Anterior Skull Base Meningiomas Surgery: A Clinical Study. World Neurosurg. 2018, 120, e776–e782. [Google Scholar] [CrossRef]
- Behari, S.; Giri, P.J.; Shukla, D.; Jain, V.K.; Banerji, D. Surgical strategies for giant medial sphenoid wing meningiomas: A new scoring system for predicting extent of resection. Acta Neurochir. 2008, 150, 865–877. [Google Scholar] [CrossRef]
- Tomasello, F.; De Divitiis, O.; Angileri, F.F.; Salpietro, F.M.; d’Avella, D. Large sphenocavernous meningiomas: Is there still a role for the intradural approach via the pterional-transsylvian route? Acta Neurochir. 2003, 145, 273–282. [Google Scholar] [CrossRef]
- Loewenstern, J.; Aggarwal, A.; Pain, M.; Barthélemy, E.; Costa, A.; Bederson, J.; Shrivastava, R.K. Peritumoral Edema Relative to Meningioma Size Predicts Functional Outcomes after Resection in Older Patients. Oper. Neurosurg. 2018, 16, 281–291. [Google Scholar] [CrossRef]
- Vignes, J.R.; Sesay, M.; Rezajooi, K.; Gimbert, E.; Liguoro, D. Peritumoral edema and prognosis in intracranial meningioma surgery. J. Clin. Neurosci. 2008, 15, 764–768. [Google Scholar] [CrossRef]
- Lee, K.J.; Joo, W.I.; Rha, H.K.; Park, H.K.; Cough, J.K.; Hong, Y.K.; Park, C.K. Peritumoral brain edema in meningiomas: Correla-tions between magnetic resonance imaging, angiography, and pathology. Surg Neurol. 2008, 69, 350–355. [Google Scholar] [CrossRef]
- Osawa, T.; Tosaka, M.; Nagaishi, M.; Yoshimoto, Y. Factors affecting peritumoral brain edema in meningioma: Special histological subtypes with prominently extensive edema. J. Neuro-Oncol. 2012, 111, 49–57. [Google Scholar] [CrossRef]
- Quiñones-Hinojosa, A.; Kaprealian, T.; Chaichana, K.L.; Sanai, N.; Parsa, A.T.; Berger, M.S.; McDermott, M.W. Pre-Operative Factors Affecting Resectability of Giant Intracranial Meningiomas. Can. J. Neurol. Sci. J. Can. Des Sci. Neurol. 2009, 36, 623–630. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Ma, S.-C.; Liu, Y.-H.; Wei, L.; Zhang, C.-Y.; Qi, J.-F.; Yu, C.-J. Large and giant medial sphenoid wing meningiomas involving vascular structures: Clinical features and management experience in 53 patients. Chin. Med. J. 2013, 126, 4470–4476. [Google Scholar]
- Pamir, M.N.; Belirgen, M.; Ozduman, K.; Kılıç, T.; Özek, M. Anterior clinoidal meningiomas: Analysis of 43 consecutive surgically treated cases. Acta Neurochir. 2008, 150, 625–636. [Google Scholar] [CrossRef]
- Barzaghi, L.R.; Spina, A.; Gagliardi, F.; Boari, N.; Mortini, P. Transfrontal-Sinus-Subcranial Approach to Olfactory Groove Meningiomas: Surgical Results and Clinical and Functional Outcome in a Consecutive Series of 21 Patients. World Neurosurg. 2017, 101, 315–324. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.S.; Rubinstein, L.J. Tumors of meninges and of related tissues. In Pathology of Tumors of Nervous System, 4th ed.; Russel, D.S., Rubinstein, L.J., Eds.; Williams & Wilkins Co.: Baltimore, MD, USA, 1977; pp. 65–91. [Google Scholar]
- Haeren, R.H.; Rautalin, I.; Schwartz, C.; Korja, M.; Niemelä, M. Surgery on giant meningiomas in very old patients entails frequent postoperative intracranial hemorrhages and atypical histopathology. J. Neuro-Oncol. 2021, 152, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Solheim, O.; Selbekk, T.; Lindseth, F.; Unsgård, G. Navigated resection of giant intracranial meningiomas based on intraoperative 3D ultrasound. Acta Neurochir. 2009, 151, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Balasa, A.; Hurghis, C.; Tamas, F.; Chinezu, R. Surgical Strategies and Clinical Outcome of Large to Giant Sphenoid Wing Meningiomas: A Case Series Study. Brain Sci. 2020, 10, 957. [Google Scholar] [CrossRef]
- Wang, X.; Wu, R.; Zhang, P.; Zhang, C.; Song, G.; Gao, Z. Superior Sagittal Sinus Obstruction by Giant Meningiomas: Is Total Removal Feasible? World Neurosurg. 2016, 94, 111–119. [Google Scholar] [CrossRef]
- Narayan, V.; Bir, S.C.; Mohammed, N.; Savardekar, A.R.; Patra, D.P.; Nanda, A. Surgical Management of Giant Intracranial Meningioma: Operative Nuances, Challenges, and Outcome. World Neurosurg. 2018, 110, e32–e41. [Google Scholar] [CrossRef]
- Da Silva, C.E.; de Freitas, P.E.P. Large and giant skull base meningiomas: The role of radical surgical removal. Surg. Neurol. Int. 2015, 6, 113. [Google Scholar] [CrossRef]
- Tuna, M.; Göçer, A.I.; Gezercan, Y.; Vural, A.; Ildan, F.; Haciyakupoğlu, S.; Karadayi, A. Huge Meningiomas: A Review of 93 Case. Skull Base 1999, 9, 227–238. [Google Scholar] [CrossRef]
- Kim, B.W.; Kim, M.S.; Kim, S.W.; Chang, C.H.; Kim, O.L. Peritumoral brain edema in meningiomas: Correlation of radiologic and pathologic features. J. Korean Neurosurg. Soc. 2011, 49, 26–30. [Google Scholar] [CrossRef]
- Das, K.; Gajbhiye, S.; Gosal, J.; Pandey, S. Apoplexy inside a giant medial sphenoid wing meningothelial (Grade I) meningioma: An extremely rare but a potentially dangerous complication. Asian J. Neurosurg. 2019, 14, 961–963. [Google Scholar] [CrossRef]
- Oyama, H.; Noda, S.; Negoro, M.; Kinomoto, T.; Miyachi, S.; Kuwayama, N.; Kajita, Y. Giant Meningioma Fed by the Anterior Choroidal Artery: Successful Removal Following Embolization—Case Report. Neurol. Med. Chir. 1992, 32, 839–841. [Google Scholar] [CrossRef] [Green Version]
- Mandel, M.; Li, Y.; Figueiredo, E.G.; Teixeira, M.J.; Steinberg, G.K. Presurgical Planning with Open-Source Horos Software for Superficial Brain Arteriovenous Malformations. World Neurosurg. 2021, 157, 3–12. [Google Scholar] [CrossRef]
- Armocida, D.; Arcidiacono, U.A.; Palmieri, M.; Pesce, A.; Cofano, F.; Picotti, V.; Salvati, M.; D’Andrea, G.; Garbossa, D.; Santoro, A.; et al. Intracranial Meningioma in Elderly Patients. Retrospective Multicentric Risk and Surgical Factors Study of Morbidity and Mortality. Diagnostics 2022, 12, 351. [Google Scholar] [CrossRef]
- Nabors, L.B.; Portnow, J.; Ahluwalia, M.; Baehring, J.; Brem, H.; Brem, S.; Butowski, N.; Campian, J.L.; Clark, S.W.; Fabiano, A.J.; et al. Central Nervous System Cancers, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 1537–1570. [Google Scholar] [CrossRef]
- Zygourakis, C.C.; Sughrue, M.E.; Benet, A.; Parsa, A.T.; Berger, M.S.; McDermott, M.W. Management of Planum/Olfactory Meningiomas: Predicting Symptoms and Postoperative Complications. World Neurosurg. 2014, 82, 1216–1223. [Google Scholar] [CrossRef]
- Armocida, D.; Pesce, A.; Frati, A.; Santoro, A.; Salvati, M. EGFR amplification is a real independent prognostic impact factor between young adults and adults over 45yo with wild-type glioblastoma? J. Neuro-Oncol. 2019, 146, 275–284. [Google Scholar] [CrossRef]
- Armocida, D.; Frati, A.; Salvati, M.; Santoro, A.; Pesce, A. Is Ki-67 index overexpression in IDH wild type glioblastoma a predictor of shorter Progression Free survival? A clinical and Molecular analytic investigation. Clin. Neurol. Neurosurg. 2020, 198, 106126. [Google Scholar] [CrossRef]
- Emmez, H.; Aslan, A.; Demirci, H.; Çeltikçi, E.; Kaymaz, A.; Börcek, A. The unilateral frontotemporal approach for large and giant olfactory groove meningioma: Experience with 18 consecutive patients. Neurochirurgie 2021, 68, 36–43. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Terasaka, S.; Kobayashi, H.; Asaoka, K.; Murata, J.; Houkin, K. Giant Skull Base Atypical Meningioma Presenting with Rapidly Progressive Impaired Consciousness Caused by Severe Venous Congestion—Case Report. Neurol. Med. Chir. 2011, 51, 789–792. [Google Scholar] [CrossRef] [Green Version]
- Mumoli, N.; Pulerà, F.; Vitale, J.; Camaiti, A. Frontal lobe syndrome caused by a giant meningioma presenting as depression and bipolar disorder. Singap. Med. J. 2013, 54, e158–e159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatiboglu, M.A.; Cosar, M.; Iplıkcıoglu, A.C.; Ozcan, D. Sex steroid and epidermal growth factor profile of giant meningiomas associated with pregnancy. Surg. Neurol. 2008, 69, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Tomasello, F.; Angileri, F.F.; Grasso, G.; Granata, F.; De Ponte, F.S.; Alafaci, C. Giant Olfactory Groove Meningiomas: Extent of Frontal Lobes Damage and Long-Term Outcome after the Pterional Approach. World Neurosurg. 2011, 76, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Attia, M.; Umansky, F.; Paldor, I.; Dotan, S.; Shoshan, Y.; Spektor, S. Giant anterior clinoidal meningiomas: Surgical technique and outcomes. J. Neurosurg. 2012, 117, 654–665. [Google Scholar] [CrossRef]
- Yang, J.; Liu, Y.-H.; Ma, S.-C.; Wei, L.; Lin, R.-S.; Qi, J.-F.; Hu, Y.-S.; Yu, C.-J. Subtemporal Transtentorial Petrosalapex Approach for Giant Petroclival Meningiomas: Analyzation and Evaluation of the Clinical Application. J. Neurol. Surg. Part B Skull Base 2012, 73, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Antunes, C.; Ramos, R.; Machado, M.J.; Filipe, M.A. Giant posterior fossa meningioma: The importance of early diagnosis and challenges concerning treatment. BMJ Case Rep. 2019, 12, e228454. [Google Scholar] [CrossRef]
- Yang, J.; Ma, S.-C.; Fang, T.; Qi, J.-F.; Hu, Y.-S.; Yu, C.-J. Subtemporal transpetrosal apex approach: Study on its use in large and giant petroclival meningiomas. Chin. Med. J. 2011, 124. [Google Scholar]
- Jiang, Y.-G.; Xiang, J.; Wen, F.; Zhang, L.-Y. Microsurgical Excision of the Large or Giant Cerebellopontine Angle Meningioma. Min-Minim. Invasive Neurosurg. 2006, 49, 43–48. [Google Scholar] [CrossRef]
- Armocida, D.; Marzetti, F.; Pesce, A.; Caporlingua, A.; D’Angelo, L.; Santoro, A. Purely Meningeal Intracranial Relapse of Melanoma Brain Metastases After Surgical Resection and Immunotherapy as a Unique Disease Progression Pattern: Our Experience and Review of the Literature. World Neurosurg. 2019, 134, 150–154. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Final Series | No. 340 | |
|---|---|---|
| Age | Mean: 60.38 Median: 62 Sd: 13.56 | Min: 20 Max: 90 |
| Sex (Female) | F: 238–70% | |
| Smoke | 98 = 28.8% | |
| Hypertension | 108 = 31.8% | |
| Clinical debut | Incidental (1) = 45–13.2% | Headache (4) = 46–13.5% |
| Dizziness (2) = 32–9.4% | Seizure (5) = 88–25.9% | |
| Focal deficit (3) = 80–23.5% | Mental alteration (6) = 46–13.5% | |
| Hospitalization (330 pts) | Mean: 17.76 Median: 13 Sd: 17.23 | Min: 5 Max: 209 |
| Follow-up (months) | Mean: 47.76 Median: 47 Sd: 14.82 | Min: 12 Max: 72 |
| WHO grade | Grade I: 285–83.8% | |
| Grade II: 47–13.8% | ||
| Grade III: 8–2.4% | ||
| Histological type | 1 = Meningothelial–205–60.3% | 7 = Secretory–12–3.5% |
| 2 = Psammomatose–16–4.7% | 8 = Anaplastic–7–2.1% | |
| 3 = Transitional–22–6.5% | 9 = Angiomatous–9–2.6% | |
| 4 = Microcystic–8–2.4% | 10 = Lymphoplasmacitic–1–0.3% | |
| 5 = Atypic–40–11.8% | 11 = Metaplastic–5–1.5% | |
| 6 = Fibrous–13–3.8% | ||
| Switch in a malignant form | 5/335–1.5% | |
| Multiple/meningiomatosis | 13 pts–3.8% | |
| Location/position | 1 = Clinoid–11–3.2% | 9 = Sphenoid wing–20–5.9% |
| 2 = APC–12–3.5% | 10 = Tuberculum sellae–9–2.6% | |
| 3 = Falx–39–11.5% | 11 = Planum sphenoidal–8–2.4% | |
| 4 = Parasagittal parietal–21–6.2% | 12 = Tentorial–15–4.4% | |
| 5 = Parasagittal frontal–26–7.6% | 13 = Temporal convexity–15–4.4% | |
| 6 = Olfactory groove–14–4.1% | 14 = Orbital–3–0.9% | |
| 7 = Frontal convexity–85–25% | 15 = Sphenopetroclival–12–3.5% | |
| Subtentorial–26–7.6% | ||
| Groups | Giant Meningiomas: 117 pts | Medium/Large Meningiomas: 223 pts | p-Value |
|---|---|---|---|
| Sex | M: 46–39.3% | M: 56–25.1% | 1.00 |
| F: 71–60.7% | F: 167–74.9% | ||
| Age | Min: 20 Max: 90 | Min: 25 Max: 89 | 1.00 |
| Mean: 60.62 | Mean: 60.26 | ||
| Median: 64 | Median: 60.50 | ||
| SD: 13.99 | SD: 13.35 | ||
| Smoke | 37 = 31.6% | 61 = 27.4% | 0.24 |
| Hypertension | 42 = 35.9% | 66 = 29.6% | 0.24 |
| Comorbidity CCI scale (points) | 0 = 25 | 0 = 44 | |
| 1 = 21 | 1 = 36 | 1.00 | |
| 2 = 24 | 2 = 47 | 1.00 | |
| 3 = 16 | 3 = 39 | 0.23 | |
| 4 = 21 | 4 = 31 | 0.98 | |
| >5 = 10 | >5 = 26 | 0.67 | |
| Seizure at onset | 24 pts = 20.5% | 49 pts = 22% | 0.76 |
| WHO grade | Grade I: 81–69.2% | Grade I: 204–91.5% | 1.00 |
| Grade II: 31–26.5% | Grade II: 16–7.2%. | <0.01 | |
| Grade III: 5–4.3% | Grade III: 3–1.3% | 0.09 | |
| Maximum diameter (cm) | Min: 5 Max: 10.5 | Min: 0.80 Max: 4.9 | |
| Mean: 6.26 | Mean: 3.3 | ||
| Median: 6 | Median: 3.3 | ||
| V edema cm3 | Mean: 42.52 SD: 52.77 | Mean: 18.37 SD: 38.59 | <0.01 |
| V lesion cm3 | Mean: 67.32 SD: 39.31 | Mean: 15.79 SD: 12.59 | <0.01 |
| Mitotic index/10 HPF | Mean: 1.92 SD: 2.4 | Mean: 1.2 SD: 1.9 | <0.01 |
| Ki-67 expression | Mean = 7% | Mean = 4.5% | 0.02 |
| PR+ | 12 pts | 26 pts | 0.42 |
| Simpson grade resection | 1 = 51 pts–43.6% | 1 = 102 pts–45.6% | |
| 2 = 20 pts–17.1% | 2 = 35 pts–15.7% | ||
| 3 = 5 pts–4.3% | 3 = 7 pts–3.1% | ||
| 4 = 1 pts–0.9% | 4 = 1 pts–0.7% | ||
| Hospitalization | Mean = 18.71 | Mean = 17.27 | 0.48 |
| Complications | 35 pts: 29.9% | 33 pts: 14.8% | <0.01 |
| Complications | Hydrocephalus = 2 pts–1.7% | Hydrocephalus = 5 pts–2.2% | 1.00 |
| Hemorrhage= 2 pts–1.7% | Hemorrhage= 4 pts–1.8% | 1.00 | |
| Infections= 16 pts–13.7% | Infections= 10–4.5% | <0.01 | |
| Intractable seizure = 5 pts–4.3% | Intractable seizure = 6–2.7% | 1.00 | |
| Ischemia = 10 pts–8.5% | Ischemia = 8–3.6% | 0.05 | |
| Recurrence | 17 pts = 14.5% | 20 pts = 9% | 0.11 |
| Dead at last evaluation | 14 pts: 12% | 16 pts: 7.2% | 0.14 |
| KPS at onset | Mean = 70–80 DS= 14.72 | Mean = 80 DS = 14 | 0.57 |
| KPS after procedure | Mean = 80 DS = 20 | Mean = 80 DS = 10 | 1.00 |
| KPS last evaluation | Mean = 80 | Mean = 80–90 | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armocida, D.; Catapano, A.; Palmieri, M.; Arcidiacono, U.A.; Pesce, A.; Cofano, F.; Picotti, V.; Salvati, M.; Garbossa, D.; D’Andrea, G.; et al. The Surgical Risk Factors of Giant Intracranial Meningiomas: A Multi-Centric Retrospective Analysis of Large Case Serie. Brain Sci. 2022, 12, 817. https://doi.org/10.3390/brainsci12070817
Armocida D, Catapano A, Palmieri M, Arcidiacono UA, Pesce A, Cofano F, Picotti V, Salvati M, Garbossa D, D’Andrea G, et al. The Surgical Risk Factors of Giant Intracranial Meningiomas: A Multi-Centric Retrospective Analysis of Large Case Serie. Brain Sciences. 2022; 12(7):817. https://doi.org/10.3390/brainsci12070817
Chicago/Turabian StyleArmocida, Daniele, Antonia Catapano, Mauro Palmieri, Umberto Aldo Arcidiacono, Alessandro Pesce, Fabio Cofano, Veronica Picotti, Maurizio Salvati, Diego Garbossa, Giancarlo D’Andrea, and et al. 2022. "The Surgical Risk Factors of Giant Intracranial Meningiomas: A Multi-Centric Retrospective Analysis of Large Case Serie" Brain Sciences 12, no. 7: 817. https://doi.org/10.3390/brainsci12070817