
A Multi-Modal and Multi-Atlas Integrated Framework for Identification of Mild Cognitive Impairment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Acquisition
2.3. Data Preprocessing
2.3.1. fMRI
2.3.2. sMRI
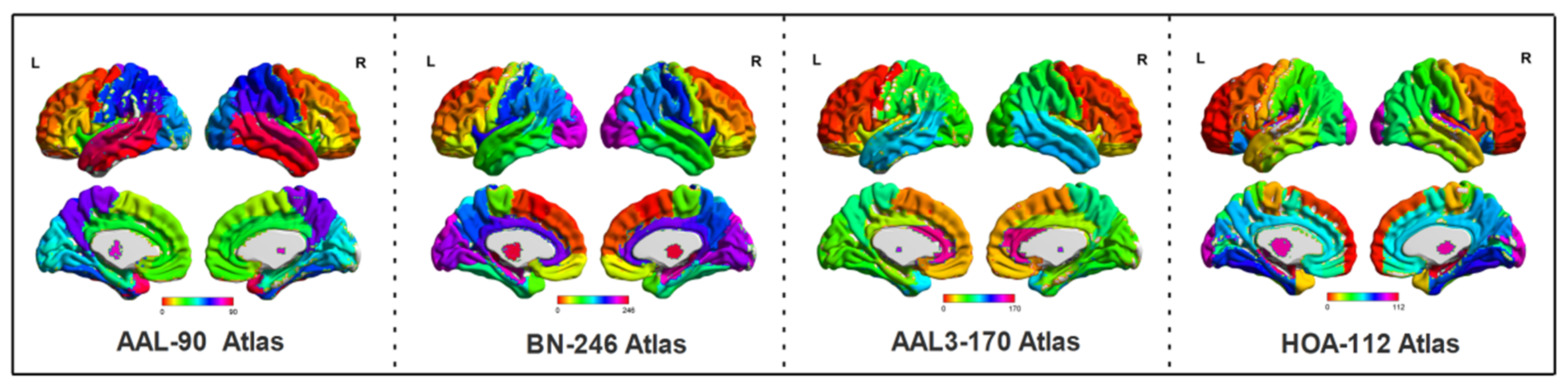
2.4. Feature Extraction under Four Atlases
2.5. Feature Selection
2.6. SVM Based Classification
3. Results
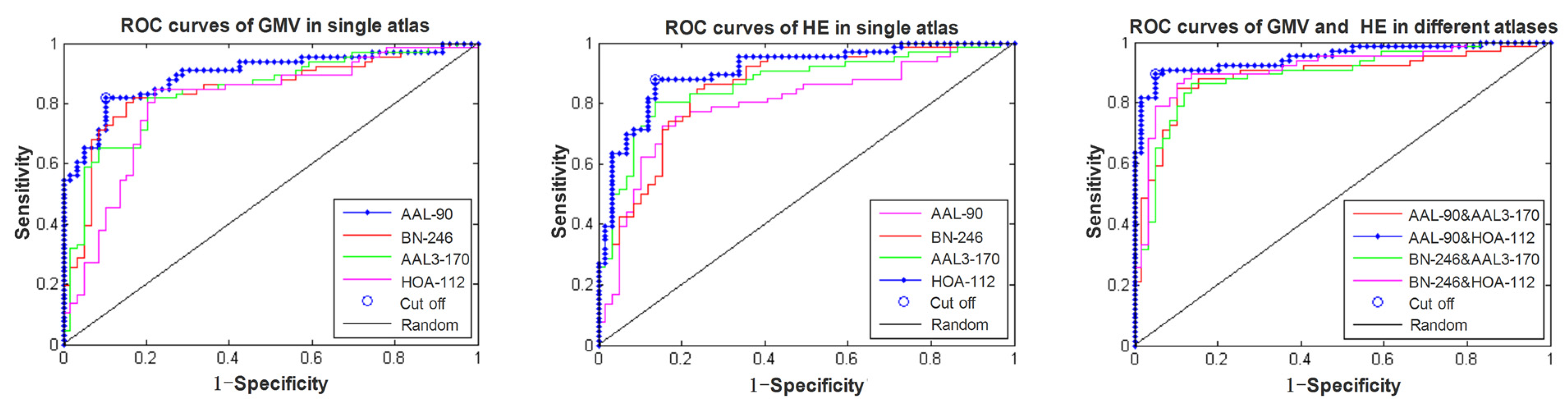
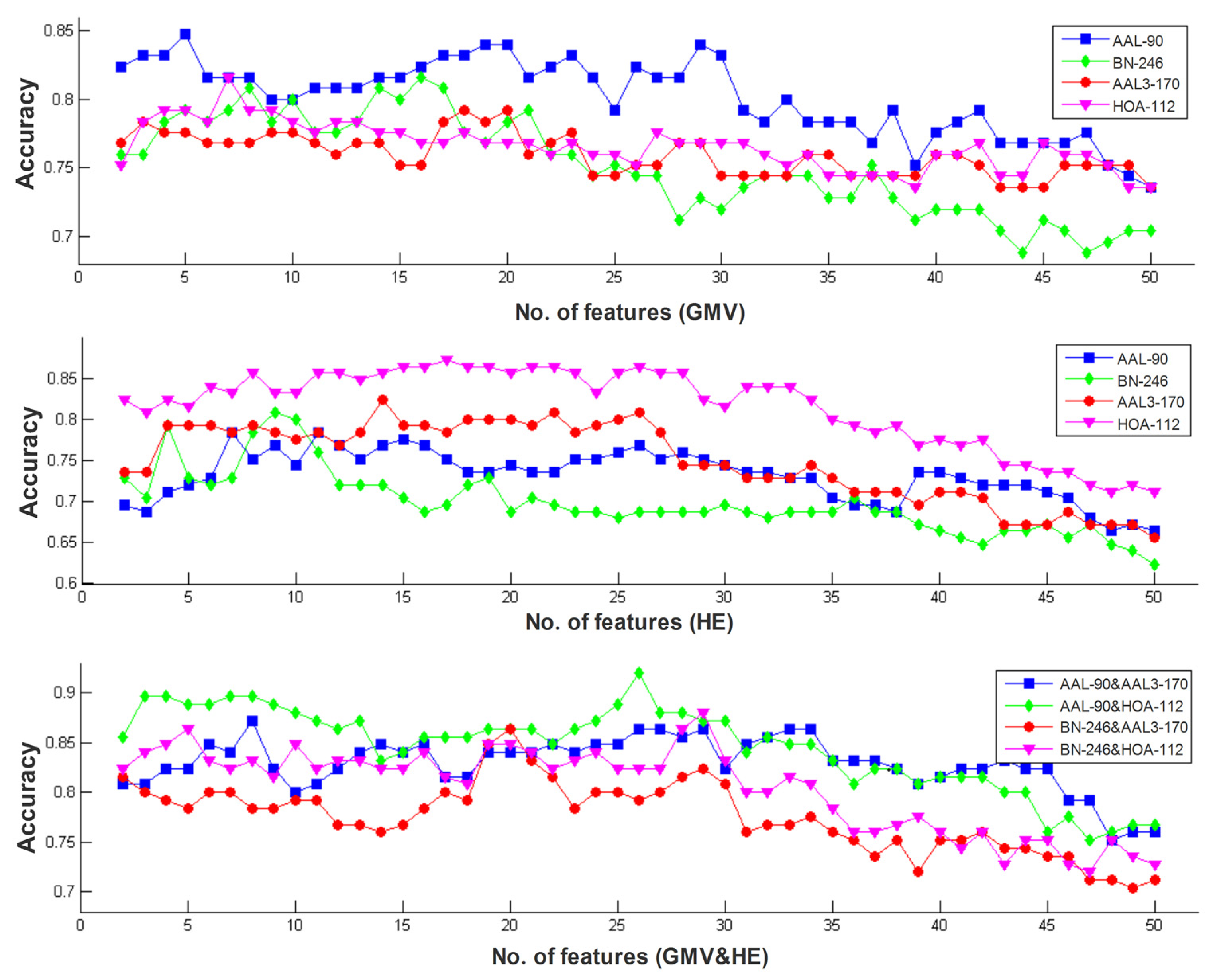
3.1. Classification Performance of Different Models
3.2. Between-Group Differences in HE Index and Gray Matter Volume
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, Z.; Liu, Y.; Jiang, T.; Zhou, B.; An, N.; Dai, H.; Wang, P.; Niu, Y.; Wang, L.; Zhang, X. Altered spontaneous activity in Alzheimer’s disease and mild cognitive impairment revealed by Regional Homogeneity. NeuroImage 2012, 59, 1429–1440. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Jing, B.; Li, Y.; Yan, H.; Li, Z.; Ma, X.; Zhuo, Z.; Wei, L.; Li, H.; Alzheimer’s Disease Neuroimaging Initiative. Identifying Mild Cognitive Impairment with Random Forest by Integrating Multiple MRI Morphological Metrics. J. Alzheimers Dis. 2020, 73, 991–1002. [Google Scholar] [CrossRef]
- Mao, Y.; Liao, Z.; Liu, X.; Li, T.; Hu, J.; Le, D.; Pei, Y.; Sun, W.; Lin, J.; Qiu, Y.; et al. Disrupted balance of long and short-range functional connectivity density in Alzheimer’s disease (AD) and mild cognitive impairment (MCI) patients: A resting-state fMRI study. Ann. Transl. Med. 2021, 9, 65. [Google Scholar] [CrossRef]
- Feng, Q.; Wang, M.; Song, Q.; Wu, Z.; Jiang, H.; Pang, P.; Liao, Z.; Yu, E.; Ding, Z. Correlation Between Hippocampus MRI Radiomic Features and Resting-State Intrahippocampal Functional Connectivity in Alzheimer’s Disease. Front. Neurosci. 2019, 13, 435. [Google Scholar] [CrossRef] [Green Version]
- Pozueta, A.; Rodríguez-Rodríguez, E.; Vazquez-Higuera, J.L.; Mateo, I.; Sánchez-Juan, P.; González-Perez, S.; Berciano, J.; Combarros, O. Detection of early Alzheimer’s disease in MCI patients by the combination of MMSE and an episodic memory test. BMC Neurol. 2011, 11, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, Z.; Jing, B.; Guo, R.; Li, B.; Cui, F.; Wang, T.; Chen, H. A Brainnetome Atlas Based Mild Cognitive Impairment Identification Using Hurst Exponent. Front. Aging Neurosci. 2018, 10, 103. [Google Scholar] [CrossRef] [Green Version]
- Desikan, R.S.; Cabral, H.J.; Hess, C.P.; Dillon, W.P.; Glastonbury, C.M.; Weiner, M.W.; Schmansky, N.J.; Greve, D.N.; Salat, D.H.; Buckner, R.L.; et al. Alzheimer’s Disease Neuroimaging Initiative. Automated MRI measures identify individuals with mild cognitive impairment and Alzheimer’s disease. Brain 2009, 132, 2048–2057. [Google Scholar] [CrossRef] [PubMed]
- Marin-Marin, L.; Palomar-García, M.Á.; Miró-Padilla, A.; Adrián-Ventura, J.; Aguirre, N.; Villar-Rodríguez, E.; Costumero, V. Bilingualism’s Effects on Resting-State Functional Connectivity in Mild Cognitive Impairment. Brain Connect. 2021, 11, 30–37. [Google Scholar] [CrossRef]
- Beheshti, I.; Demirel, H.; Alzheimer’s Disease Neuroimaging Initiative. Feature-ranking-based Alzheimer’s disease classification from structural MRI. Magn. Reson. Imaging 2016, 34, 252–263. [Google Scholar] [CrossRef] [PubMed]
- Lei, B.; Zhao, Y.; Huang, Z.; Hao, X.; Zhou, F.; Elazab, A.; Qin, J.; Lei, H. Adaptive sparse learning using multi-template for neurodegenerative disease diagnosis. Med. Image Anal. 2020, 61, 101632. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Zheng, Q.; Dyrba, M.; Rittman, T.; Li, A.; Che, T.; Chen, P.; Sun, Y.; Kang, X.; Li, Q.; et al. Alzheimer’s Disease Neuroimaging Initiative. Regional Radiomics Similarity Networks Reveal Distinct Subtypes and Abnormality Patterns in Mild Cognitive Impairment. Adv. Sci. 2022, 9, e2104538. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Ding, Y.; Han, Y.; Fan, Y.; Alexander, B.; Aaron, F.; Han, T.; Jin, D.; Liu, B.; Lu, J.; et al. Independent and reproducible hippocampal radiomic biomarkers for multisite Alzheimer’s disease: Diagnosis, longitudinal progress and biological basis. Sci. Bull. 2020, 65, 1103–1113. [Google Scholar] [CrossRef]
- Hojjati, S.H.; Ebrahimzadeh, A.; Khazaee, A.; Babajani-Feremi, A.; Alzheimer’s Disease Neuroimaging Initiative. Predicting conversion from MCI to AD by integrating rs-fMRI and structural MRI. Comput. Biol. Med. 2018, 102, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Zhou, T.; Liu, M.; Thung, K.H.; Shen, D. Latent Representation Learning for Alzheimer’s Disease Diagnosis with Incomplete Multi-Modality Neuroimaging and Genetic Data. IEEE Trans. Med. Imaging 2019, 38, 2411–2422. [Google Scholar] [CrossRef]
- Zhou, T.; Thung, K.H.; Liu, M.; Shi, F.; Zhang, C.; Shen, D. Multi-modal Latent Space Inducing Ensemble SVM Classifier for Early Dementia Diagnosis with Neuroimaging Data. Med. Image Anal. 2019, 60, 101630. [Google Scholar] [CrossRef]
- Schouten, T.M.; Koini, M.; de Vos, F.; Seiler, S.; van der Grond, J.; Lechner, A.; Hafkemeijer, A.; Möller, C.; Schmidt, R.; de Rooij, M.; et al. Combining anatomical, diffusion, and resting state functional magnetic resonance imaging for individual classification of mild and moderate Alzheimer’s disease. Neuroimage Clin. 2016, 11, 46–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, T.; Thung, K.H.; Zhu, X.; Shen, D. Effective feature learning and fusion of multimodality data using stage-wise deep neural network for dementia diagnosis. Hum. Brain Mapp. 2019, 40, 1001–1016. [Google Scholar] [CrossRef] [Green Version]
- Dyrba, M.; Grothe, M.; Kirste, T.; Teipel, S.J. Multimodal analysis of functional and structural disconnection in Alzheimer’s disease using multiple kernel SVM. Hum. Brain Mapp. 2015, 36, 2118–2131. [Google Scholar] [CrossRef]
- Dai, Z.; Yan, C.; Wang, Z.; Wang, J.; Xia, M.; Li, K.; He, Y. Discriminative analysis of early Alzheimer’s disease using multi-modal imaging and multi-level characterization with multi-classifier (M3). Neuroimage 2012, 59, 2187–2195. [Google Scholar] [CrossRef]
- Wee, C.Y.; Yap, P.T.; Zhang, D.; Denny, K.; Browndyke, J.N.; Potter, G.G.; Welsh-Bohmer, K.A.; Wang, L.; Shen, D. Identification of MCI individuals using structural and functional connectivity networks. Neuroimage 2012, 59, 2045–2056. [Google Scholar] [CrossRef] [Green Version]
- Zeng, L.L.; Shen, H.; Liu, L.; Wang, L.; Li, B.; Fang, P.; Zhou, Z.; Li, Y.; Hu, D. Identifying major depression using whole-brain functional connectivity: A multivariate pattern analysis. Brain 2012, 135, 1498–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rushmore, R.J.; Bouix, S.; Kubicki, M.; Rathi, Y.; Rosene, D.L.; Yeterian, E.H.; Makris, N. MRI-based Parcellation and Morphometry of the Individual Rhesus Monkey Brain: The macaque Harvard-Oxford Atlas (mHOA), a translational system referencing a standardized ontology. Brain Imaging Behav. 2021, 15, 1589–1621. [Google Scholar] [CrossRef]
- Fan, L.; Li, H.; Zhuo, J.; Zhang, Y.; Wang, J.; Chen, L.; Yang, Z.; Chu, C.; Xie, S.; Laird, A.R.; et al. The Human Brainnetome Atlas: A New Brain Atlas Based on Connectional Architecture. Cereb. Cortex 2016, 26, 3508–3526. [Google Scholar] [CrossRef] [PubMed]
- Rolls, E.T.; Huang, C.C.; Lin, C.P.; Feng, J.; Joliot, M. Automated anatomical labelling atlas 3. Neuroimage 2020, 206, 116189. [Google Scholar] [CrossRef]
- Li, Y.; Liu, J.; Tang, Z.; Lei, B. Deep Spatial-Temporal Feature Fusion from Adaptive Dynamic Functional Connectivity for MCI Identification. IEEE Trans. Med. Imaging 2020, 39, 2818–2830. [Google Scholar] [CrossRef] [PubMed]
- Lei, B.; Yu, S.; Zhao, X.; Frangi, A.F.; Tan, E.L.; Elazab, A.; Wang, T.; Wang, S. Diagnosis of early Alzheimer’s disease based on dynamic high order networks. Brain Imaging Behav. 2021, 15, 276–287. [Google Scholar] [CrossRef]
- Wei, M.; Qin, J.; Yan, R.; Li, H.; Yao, Z.; Lu, Q. Identifying major depressive disorder using Hurst exponent of resting-state brain networks. Psychiatry Res. 2013, 214, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Gentili, C.; Vanello, N.; Cristea, I.; David, D.; Ricciardi, E.; Pietrini, P. Proneness to social anxiety modulates neural complexity in the absence of exposure: A resting state fMRI study using Hurst exponent. Psychiatry Res. 2015, 232, 135–144. [Google Scholar] [CrossRef]
- Lai, M.C.; Lombardo, M.V.; Chakrabarti, B.; Sadek, S.A.; Pasco, G.; Wheelwright, S.J.; Bullmore, E.T.; Baron-Cohen, S.; Consortium, M.A.; Suckling, J. A shift to randomness of brain oscillations in people with autism. Biol. Psychiatry 2010, 68, 1092–1099. [Google Scholar] [CrossRef]
- Maxim, V.; Sendur, L.; Fadili, J.; Suckling, J.; Gould, R.; Howard, R.; Bullmore, E. Fractional Gaussian noise, functional MRI and Alzheimer’s disease. Neuroimage 2005, 25, 141–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wink, A.M.; Bernard, F.; Salvador, R.; Bullmore, E.; Suckling, J. Age and cholinergic effects on hemodynamics and functional coherence of human hippocampus. Neurobiol. Aging 2006, 27, 1395–1404. [Google Scholar] [CrossRef]
- Long, Z.; Huang, J.; Li, B.; Li, Z.; Li, Z.; Chen, H.; Jing, B. A Comparative Atlas-Based Recognition of Mild Cognitive Impairment with Voxel-Based Morphometry. Front. Neurosci. 2018, 12, 916. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Jing, B.; Liu, H.; Li, Y.; Gao, X.; Li, Y.; Mu, B.; Yu, H.; Cheng, J.; Barker, P.B.; et al. Frequency-Dependent Changes in the Amplitude of Low-Frequency Fluctuations in Mild Cognitive Impairment with Mild Depression. J. Alzheimers Dis. 2017, 58, 1175–1187. [Google Scholar] [CrossRef]
- Jing, B.; Long, Z.; Liu, H.; Yan, H.; Dong, J.; Mo, X.; Li, D.; Liu, C.; Li, H. Identifying current and remitted major depressive disorder with the Hurst exponent: A comparative study on two automated anatomical labeling atlases. Oncotarget 2017, 8, 90452–90464. [Google Scholar] [CrossRef] [Green Version]
- Dosenbach, N.U.F.; Nardos, B.; Cohen, A.L.; Fair, D.A.; Power, J.D.; Church, J.A.; Nelson, S.M.; Wig, G.S.; Vogel, A.C.; Lessov-Schlaggar, C.N.; et al. Prediction of individual brain maturity using fMRI. Science 2010, 329, 1358–1361. [Google Scholar] [CrossRef] [Green Version]
- Hojjati, S.H.; Ebrahimzadeh, A.; Khazaee, A.; Babajani-Feremi, A.; Alzheimer’s Disease Neuroimaging Initiative. Predicting conversion from MCI to AD using resting-state fMRI, graph theoretical approach and SVM. J. Neurosci. Methods 2017, 282, 69–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khazaee, A.; Ebrahimzadeh, A.; Babajani-Feremi, A. Application of advanced machine learning methods on resting-state fMRI network for identification of mild cognitive impairment and Alzheimer’s disease. Brain Imaging Behav. 2016, 10, 799–817. [Google Scholar] [CrossRef]
- Marco, M.D.; Beltrachini, L.; Biancardi, A.; Frangi, A.F.; Venneri, A. Machine-learning Support to Individual Diagnosis of Mild Cognitive Impairment Using Multimodal MRI and Cognitive Assessments. Alzheimer Dis. Assoc. Disord. 2017, 31, 278–286. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.; Batmanghelich, N.; Clark, C.M.; Davatzikos, C.; Alzheimer’s Disease Neuroimaging Initiative. Spatial patterns of brain atrophy in MCI patients, identified via high-dimensional pattern classification, predict subsequent cognitive decline. Neuroimage 2008, 39, 1731–1743. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Yan, C.; Zhao, C.; Qi, Z.; Zhou, W.; Lu, J.; He, Y.; Li, K. Spatial patterns of intrinsic brain activity in mild cognitive impairment and Alzheimer’s disease: A resting-state functional MRI study. Hum. Brain Mapp. 2011, 32, 1720–1740. [Google Scholar] [CrossRef]
- Han, Y.; Wang, J.; Zhao, Z.; Min, B.; Lu, J.; Li, K.; He, Y.; Jia, J. Frequency-dependent changes in the amplitude of low-frequency fluctuations in amnestic mild cognitive impairment: A resting-state fMRI study. Neuroimage 2011, 55, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Hünerli, D.; Emek-Savaş, D.D.; Çavuşoğlu, B.; Çolakoğlu, B.D.; Ada, E.; Yener, G.G. Mild cognitive impairment in Parkinson’s disease is associated with decreased P300 amplitude and reduced putamen volume. Clin. Neurophysiol. 2019, 130, 1208–1217. [Google Scholar] [CrossRef]
- Moretti, D.V.; Paternicò, D.; Binetti, G.; Zanetti, O.; Frisoni, G.B. Analysis of grey matter in thalamus and basal ganglia based on EEG α3/α2 frequency ratio reveals specific changes in subjects with mild cognitive impairment. ASN Neuro 2012, 4, e00103. [Google Scholar] [CrossRef]
- Ota, K.; Oishi, N.; Ito, K.; Fukuyama, H.; SEAD-J Study Group. A comparison of three brain atlases for MCI prediction. J. Neurosci. Methods 2014, 221, 139–150. [Google Scholar] [CrossRef] [Green Version]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef]
- Desikan, R.S.; Ségonne, F.; Fischl, B.; Quinn, B.T.; Dickerson, B.C.; Blacker, D.; Buckner, R.L.; Dale, A.M.; Maguire, R.P.; Hyman, B.T.; et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 2006, 31, 968–980. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | MCI | HC | p-values |
|---|---|---|---|
| Gender (M/F) | 66 (35/31) | 59 (28/31) | 0.53 # |
| Age (years) | 67.20 ± 7.22 | 65.22 ± 7.36 | 0.13 * |
| Education (years) | 9.83 ± 4.22 | 10.01 ± 4.29 | 0.81 * |
| CDR | 0.5 | 0 | 0 * |
| MMSE | 23.47 ± 2.71 | 27.37 ± 3.17 | <0.001 * |
| AVLT-immediate recall | 7.12 ± 3.49 | 11.58 ± 2.25 | <0.001 * |
| AVLT-delay recall | 3.67 ± 2.85 | 9.80 ± 2.80 | <0.001 * |
| AVLT-recognition | 8.01 ± 2.56 | 12.95 ± 2.97 | <0.001 * |
| Modality | Atlases | No. Selected Features | Accuracy | Specificity | Sensitivity | AUC Values |
|---|---|---|---|---|---|---|
| sMRI | AAL-90 | 5 | 84.80% | 88.14% | 81.82% | 0.8970 |
| AAL3-170 | 18 | 79.20% | 79.66% | 78.79% | 0.8405 | |
| BN-246 | 16 | 81.60% | 81.36% | 81.82% | 0.8451 | |
| HOA-112 | 7 | 81.60% | 77.97% | 84.85% | 0.8046 | |
| Bagging | 28 | 86.40% | 84.75% | 87.88% | - | |
| fMRI | AAL-90 | 7 | 78.40% | 75.76% | 81.36% | 0.8007 |
| AAL3-170 | 14 | 82.40% | 86.44% | 78.79% | 0.8644 | |
| BN-246 | 9 | 80.80% | 76.27% | 84.85% | 0.8562 | |
| HOA-112 | 17 | 87.20% | 86.44% | 87.88% | 0.9081 | |
| Bagging | 40 | 88.80% | 89.83% | 87.88% | - | |
| sMRI + fMRI | AAL-90 | 11 | 86.40% | 84.75% | 87.88% | 0.8891 |
| AAL3-170 | 12 | 82.40% | 79.66% | 84.85% | 0.8580 | |
| BN-246 | 14 | 84.80% | 83.05% | 86.36% | 0.8783 | |
| HOA-112 | 22 | 88.00% | 86.44% | 89.39% | 0.9124 | |
| AAL-90+AAL3-170 | 8 | 87.20% | 89.83% | 84.85% | 0.8903 | |
| AAL-90+HOA-112 | 26 | 92.00% | 94.92% | 89.39% | 0.9502 | |
| BN-246+AAL3-170 | 20 | 86.40% | 86.44% | 86.36% | 0.8914 | |
| BN-246+HOA-112 | 29 | 88.00% | 88.14% | 87.88% | 0.9135 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Long, Z.; Li, J.; Liao, H.; Deng, L.; Du, Y.; Fan, J.; Li, X.; Miao, J.; Qiu, S.; Long, C.; et al. A Multi-Modal and Multi-Atlas Integrated Framework for Identification of Mild Cognitive Impairment. Brain Sci. 2022, 12, 751. https://doi.org/10.3390/brainsci12060751
Long Z, Li J, Liao H, Deng L, Du Y, Fan J, Li X, Miao J, Qiu S, Long C, et al. A Multi-Modal and Multi-Atlas Integrated Framework for Identification of Mild Cognitive Impairment. Brain Sciences. 2022; 12(6):751. https://doi.org/10.3390/brainsci12060751
Chicago/Turabian StyleLong, Zhuqing, Jie Li, Haitao Liao, Li Deng, Yukeng Du, Jianghua Fan, Xiaofeng Li, Jichang Miao, Shuang Qiu, Chaojie Long, and et al. 2022. "A Multi-Modal and Multi-Atlas Integrated Framework for Identification of Mild Cognitive Impairment" Brain Sciences 12, no. 6: 751. https://doi.org/10.3390/brainsci12060751