
Efficacy of Overground Robotic Gait Training on Balance in Stroke Survivors: A Systematic Review and Meta-Analysis

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Sources and Searches
2.3. Study Selection and Data Collection Process
2.4. Risk of Bias Assessment
2.5. Data Synthesis
3. Results
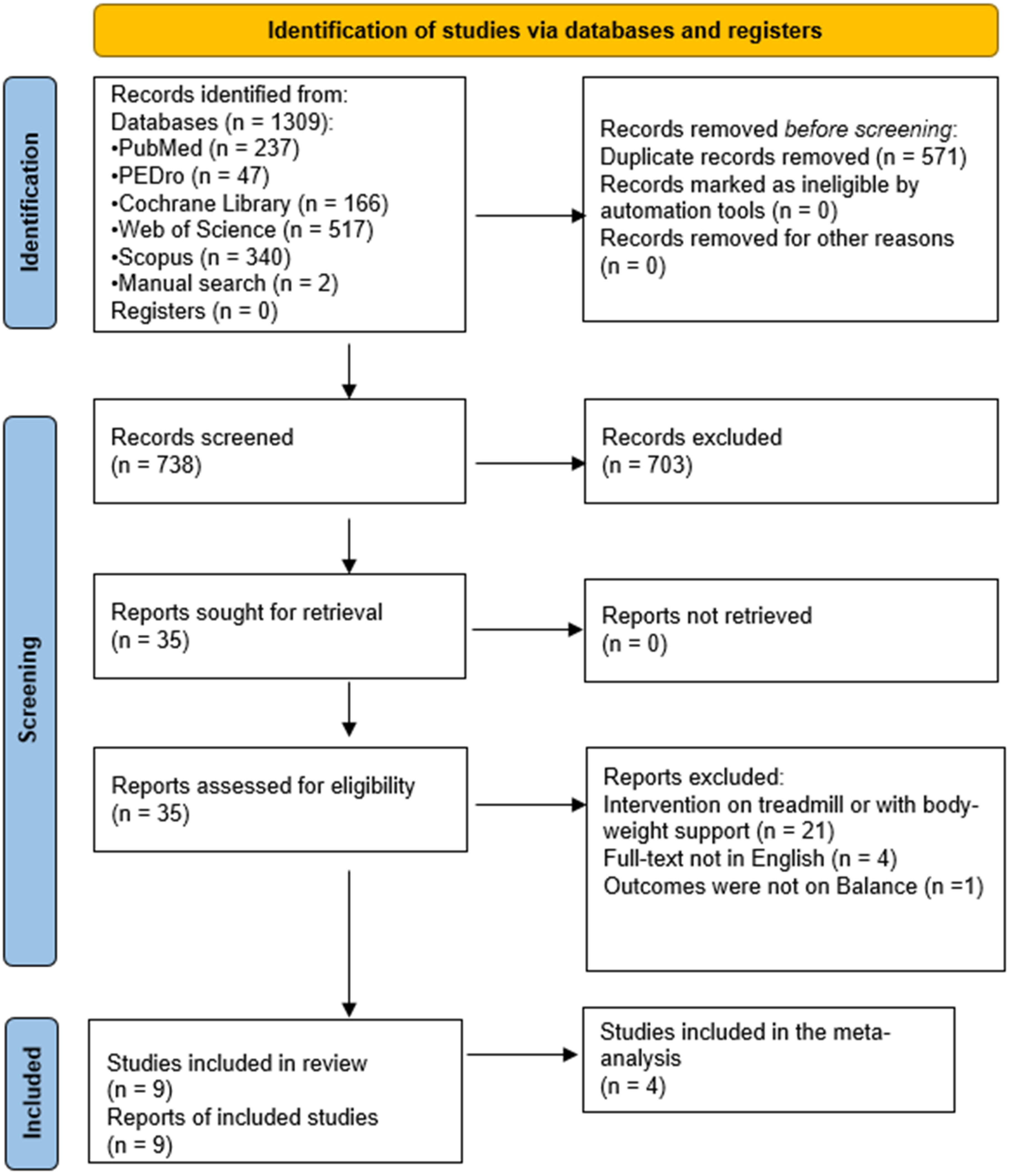
3.1. Study Selection
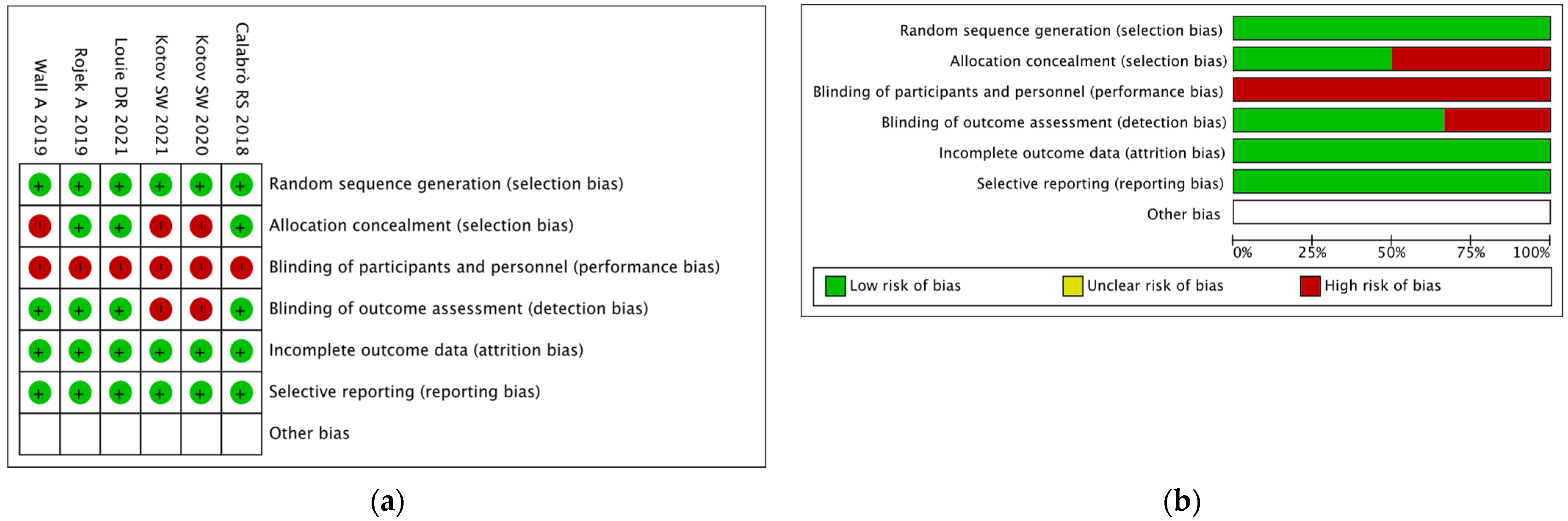
3.2. Methodological Quality Assessment
3.3. Participants
3.4. Intervention
3.5. Comparison
3.6. Outcome Measure
3.7. Meta-Analysis
3.7.1. Comparison Assessed with the Berg Balance Scale
3.7.2. Comparison Assessed with the Barthel Index
3.7.3. Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pennycott, A.; Wyss, D.; Vallery, H.; Klamroth-Marganska, V.; Riener, R. Towards more effective robotic gait training for stroke rehabilitation: A review. J. Neuroeng. Rehabil. 2012, 9, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunz, A.; Dirnagl, U.; Mergenthaler, P. Acute pathophysiological processes after ischaemic and traumatic brain injury. Best Pract Res. Clin. Anaesthesiol. 2010, 24, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Lo, W.L.; Mao, Y.R.; Ding, M.H.; Lin, Q.; Li, H.; Zhao, J.L.; Xu, Z.Q.; Bian, R.H.; Huang, D.F. Effect of Virtual Reality on Postural and Balance Control in Patients with Stroke: A Systematic Literature Review. Biomed Res. Int. 2016, 2016, 7309272. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.R.; Chiu, Y.L.; Chiang, S.L.; Chen, H.Y.; Sung, W.H. Feasibility of a smartphone-based balance assessment system for subjects with chronic stroke. Comput. Methods Programs Biomed. 2018, 161, 191–195. [Google Scholar] [CrossRef]
- Tramontano, M.; Dell’Uomo, D.; Cinnera, A.M.; Luciani, C.; Di Lorenzo, C.; Marcotulli, M.; Vona, F.; Mercuro, A.; Abbruzzese, S. Visual-spatial training in patients with sub-acute stroke without neglect: A randomized, single-blind controlled trial. Funct. Neurol. 2019, 34, 7–13. [Google Scholar]
- Tramontano, M.; Bergamini, E.; Iosa, M.; Belluscio, V.; Vannozzi, G.; Morone, G. Vestibular rehabilitation training in patients with subacute stroke: A preliminary randomized controlled trial. NeuroRehabilitation 2018, 43, 247–254. [Google Scholar] [CrossRef]
- Louie, D.R.; Eng, J.J. Berg Balance Scale score at admission can predict walking suitable for community ambulation at discharge from inpatient stroke rehabilitation. J. Rehabil. Med. 2018, 50, 37–44. [Google Scholar] [CrossRef] [Green Version]
- French, B.; Thomas, L.; Leathley, M.; Sutton, C.; McAdam, J.; Forster, A.; Langhorne, P.; Price, C.; Walker, A.; Watkins, C. Does repetitive task training improve functional activity after stroke? A Cochrane systematic review and meta-analysis. J. Rehabil. Med. 2010, 42, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Mansfield, A.; Inness, E.L.; Mcilroy, W.E. Chapter 13—Stroke. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 159, pp. 205–228. [Google Scholar] [CrossRef]
- Molteni, F.; Gasperini, G.; Gaffuri, M.; Colombo, M.; Giovanzana, C.; Lorenzon, C.; Farina, N.; Cannaviello, G.; Scarano, S.; Proserpio, D.; et al. Wearable robotic exoskeleton for overground gait training in sub-acute and chronic hemiparetic stroke patients: Preliminary results. Eur. J. Phys. Rehabil. Med. 2017, 53, 676–684. [Google Scholar] [CrossRef]
- Calabro, R.S.; Cacciola, A.; Berte, F.; Manuli, A.; Leo, A.; Bramanti, A.; Naro, A.; Milardi, D.; Bramanti, P. Robotic gait rehabilitation and substitution devices in neurological disorders: Where are we now? Neurol. Sci. 2016, 37, 503–514. [Google Scholar] [CrossRef]
- Morone, G.; Paolucci, S.; Cherubini, A.; De Angelis, D.; Venturiero, V.; Coiro, P.; Iosa, M. Robot-assisted gait training for stroke patients: Current state of the art and perspectives of robotics. Neuropsychiatr. Dis. Treat. 2017, 13, 1303–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louie, D.R.; Eng, J.J. Powered robotic exoskeletons in post-stroke rehabilitation of gait: A scoping review. J. Neuroeng. Rehabil. 2016, 13, 53. [Google Scholar] [CrossRef] [Green Version]
- Molteni, F.; Guanziroli, E.; Goffredo, M.; Calabrò, R.S.; Pournajaf, S.; Gaffuri, M.; Gasperini, G.; Filoni, S.; Baratta, S.; Galafate, D.; et al. Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects. Brain Sci. 2021, 11, 104. [Google Scholar] [CrossRef] [PubMed]
- Moucheboeuf, G.; Griffier, R.; Gasq, D.; Glize, B.; Bouyer, L.; Dehail, P.; Cassoudesalle, H. Effects of robotic gait training after stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2020, 63, 518–534. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zheng, Y.; Dang, Y.; Teng, M.; Zhang, X.; Cheng, Y.; Zhang, X.; Yu, Q.; Yin, A.; Lu, X. Effects of robot-assisted training on balance function in patients with stroke: A systematic review and meta-analysis. J. Rehabil. Med. 2021, 53, jrm00174. [Google Scholar] [CrossRef]
- Baronchelli, F.; Zucchella, C.; Serrao, M.; Intiso, D.; Bartolo, M. The Effect of Robotic Assisted Gait Training with Lokomat(R) on Balance Control After Stroke: Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 661815. [Google Scholar] [CrossRef] [PubMed]
- Postol, N.; Marquez, J.; Spartalis, S.; Bivard, A.; Spratt, N.J. Do powered over-ground lower limb robotic exoskeletons affect outcomes in the rehabilitation of people with acquired brain injury? Disabil. Rehabil. Assist. Technol. 2019, 14, 764–775. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deeks, J.J.H.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Version 6.3; John Wiley & Sons: Hoboken, NJ, USA, 2022. [Google Scholar]
- Mizukami, M.; Yoshikawa, K.; Kawamoto, H.; Sano, A.; Koseki, K.; Asakwa, Y.; Iwamoto, K.; Nagata, H.; Tsurushima, H.; Nakai, K.; et al. Gait training of subacute stroke patients using a hybrid assistive limb: A pilot study. Disabil. Rehabil. Assist. Technol. 2017, 12, 197–204. [Google Scholar] [CrossRef]
- Yoshimoto, T.; Shimizu, I.; Hiroi, Y. Sustained effects of once-a-week gait training with hybrid assistive limb for rehabilitation in chronic stroke: Case study. J. Phys. Ther. Sci. 2016, 28, 2684–2687. [Google Scholar] [CrossRef] [Green Version]
- Kotov, S.V.; Isakova, E.V.; Lijdvoy, V.Y.; Petrushanskaya, K.A.; Pismennaya, E.V.; Romanova, M.V.; Kodzokova, L.H. Robotic recovery of walking function in patients in the early recovery period of stroke. Zh. Nevrol. Psikhiatr. Im. S. S. Korsakova 2020, 120, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Kotov, S.V.; Romanov, A.I.; Silina, E.; Stupin, V.A.; Isakova, E.V.; Lijdvoy, V.Y.; Petrushanskaya, K.A.; Kotov, A.; Kodzokova, L.K.; Filatov, N.A.; et al. Efficiency of Leg Exoskeleton Use in Rehabilitation of Cerebral Stroke Patients. Serb. J. Exp. Clin. Res. 2021, 22, 257–264. [Google Scholar] [CrossRef]
- Calabro, R.S.; Naro, A.; Russo, M.; Bramanti, P.; Carioti, L.; Balletta, T.; Buda, A.; Manuli, A.; Filoni, S.; Bramanti, A. Shaping neuroplasticity by using powered exoskeletons in patients with stroke: A randomized clinical trial. J. Neuroeng. Rehabil. 2018, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Wall, A.; Borg, J.; Palmcrantz, S. Self-perceived functioning and disability after randomized conventional and electromechanically-assisted gait training in subacute stroke: A 6 months follow-up. NeuroRehabilitation 2019, 45, 501–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojek, A.; Mika, A.; Oleksy, L.; Stolarczyk, A.; Kielnar, R. Effects of Exoskeleton Gait Training on Balance, Load Distribution, and Functional Status in Stroke: A Randomized Controlled Trial. Front. Neurol. 2019, 10, 1344. [Google Scholar] [CrossRef] [Green Version]
- Louie, D.R.; Mortenson, W.B.; Durocher, M.; Schneeberg, A.; Teasell, R.; Yao, J.; Eng, J.J. Efficacy of an exoskeleton-based physical therapy program for non-ambulatory patients during subacute stroke rehabilitation: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 149. [Google Scholar] [CrossRef]
- Bortole, M.; Venkatakrishnan, A.; Zhu, F.; Moreno, J.C.; Francisco, G.E.; Pons, J.L.; Contreras-Vidal, J.L. The H2 robotic exoskeleton for gait rehabilitation after stroke: Early findings from a clinical study. J. Neuroeng. Rehabil. 2015, 12, 54. [Google Scholar] [CrossRef] [Green Version]
- Tamura, S.; Miyata, K.; Kobayashi, S.; Takeda, R.; Iwamoto, H. The minimal clinically important difference in Berg Balance Scale scores among patients with early subacute stroke: A multicenter, retrospective, observational study. Top. Stroke Rehabil. 2021, 25, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Nolan, K.J.; Karunakaran, K.K.; Chervin, K.; Monfett, M.R.; Bapineedu, R.K.; Jasey, N.N.; Oh-Park, M. Robotic Exoskeleton Gait Training During Acute Stroke Inpatient Rehabilitation. Front. Neurorobotics 2020, 14, 581815. [Google Scholar] [CrossRef] [PubMed]
- Pohl, M.; Werner, C.; Holzgraefe, M.; Kroczek, G.; Mehrholz, J.; Wingendorf, I.; Hoolig, G.; Koch, R.; Hesse, S. Repetitive locomotor training and physiotherapy improve walking and basic activities of daily living after stroke: A single-blind, randomized multicentre trial (DEutsche GAngtrainerStudie, DEGAS). Clin. Rehabil. 2007, 21, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Duschau-Wicke, A.; Caprez, A.; Riener, R. Patient-cooperative control increases active participation of individuals with SCI during robot-aided gait training. J. Neuroeng. Rehabil. 2010, 7, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, W.H.; Kim, M.S.; Huh, J.P.; Lee, P.K.; Kim, Y.H. Effects of robot-assisted gait training on cardiopulmonary fitness in subacute stroke patients: A randomized controlled study. Neurorehabilit. Neural Repair 2012, 26, 318–324. [Google Scholar] [CrossRef]
- Paolucci, S.; Di Vita, A.; Massicci, R.; Traballesi, M.; Bureca, I.; Matano, A.; Iosa, M.; Guariglia, C. Impact of participation on rehabilitation results: A multivariate study. Eur. J. Phys. Rehabil. Med. 2012, 48, 455–466. [Google Scholar]
- Tamburella, F.; Moreno, J.C.; Herrera Valenzuela, D.S.; Pisotta, I.; Iosa, M.; Cincotti, F.; Mattia, D.; Pons, J.L.; Molinari, M. Influences of the biofeedback content on robotic post-stroke gait rehabilitation: Electromyographic vs. joint torque biofeedback. J. Neuroeng. Rehabil. 2019, 16, 95. [Google Scholar] [CrossRef]
- Tamburella, F.; Moreno, J.C.; Iosa, M.; Pisotta, I.; Cincotti, F.; Mattia, D.; Pons, J.L.; Molinari, M. Boosting the traditional physiotherapist approach for stroke spasticity using a sensorized ankle foot orthosis: A pilot study. Top. Stroke Rehabil. 2017, 24, 447–456. [Google Scholar] [CrossRef]
- Belda-Lois, J.M.; Mena-del Horno, S.; Bermejo-Bosch, I.; Moreno, J.C.; Pons, J.L.; Farina, D.; Iosa, M.; Molinari, M.; Tamburella, F.; Ramos, A.; et al. Rehabilitation of gait after stroke: A review towards a top-down approach. J. Neuroeng. Rehabil. 2011, 8, 66. [Google Scholar] [CrossRef] [Green Version]
- Kopp, B.; Wolff, M. Brain mechanisms of selective learning: Event-related potentials provide evidence for error-driven learning in humans. Biol. Psychol. 2000, 51, 223–246. [Google Scholar] [CrossRef]
- Dobkin, B.H.; Duncan, P.W. Should body weight-supported treadmill training and robotic-assistive steppers for locomotor training trot back to the starting gate? Neurorehabilit. Neural Repair 2012, 26, 308–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molteni, F.; Gasperini, G.; Cannaviello, G.; Guanziroli, E. Exoskeleton and End-Effector Robots for Upper and Lower Limbs Rehabilitation: Narrative Review. PMR 2018, 10, S174–S188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamburella, F.; Lorusso, M.; Tramontano, M.; Fadlun, S.; Masciullo, M.; Scivoletto, G. Overground robotic training effects on walking and secondary health conditions in individuals with spinal cord injury: Systematic review. J. Neuroeng. Rehabil. 2022, 19, 27. [Google Scholar] [CrossRef] [PubMed]
- Dijkers, M.P.; Akers, K.G.; Dieffenbach, S.; Galen, S.S. Systematic Reviews of Clinical Benefits of Exoskeleton Use for Gait and Mobility in Neurologic Disorders: A Tertiary Study. Arch. Phys. Med. Rehabil. 2021, 102, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Missenard, O.; Mottet, D.; Perrey, S. The role of cocontraction in the impairment of movement accuracy with fatigue. Exp. Brain Res. 2008, 185, 151–156. [Google Scholar] [CrossRef]
- Dewald, J.P.; Sheshadri, V.; Dawson, M.L.; Beer, R.F. Upper-limb discoordination in hemiparetic stroke: Implications for neurorehabilitation. Top. Stroke Rehabil. 2001, 8, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cruz Martinez, A.; Munoz, J.; Palacios, F. The muscle inhibitory period by transcranial magnetic stimulation. Study in stroke patients. Electromyogr. Clin. Neurophysiol. 1998, 38, 189–192. [Google Scholar]
- Chang, W.H.; Kim, Y.H. Robot-assisted Therapy in Stroke Rehabilitation. J. Stroke 2013, 15, 174–181. [Google Scholar] [CrossRef]
- Tay, M.R.J.; Lim, C.J.; Chua, K.S.G. Functional and ambulatory benefits of robotic-assisted gait training during early subacute inpatient rehabilitation following severe stroke. Singap. Med. J. 2021. [Google Scholar] [CrossRef]
- Morone, G.; Bragoni, M.; Iosa, M.; De Angelis, D.; Venturiero, V.; Coiro, P.; Pratesi, L.; Paolucci, S. Who may benefit from robotic-assisted gait training? A randomized clinical trial in patients with subacute stroke. Neurorehabilit. Neural Repair 2011, 25, 636–644. [Google Scholar] [CrossRef]
- Calabró, R.S.; Sorrentino, G.; Cassio, A.; Mazzoli, D.; Andrenelli, E.; Bizzarini, E.; Campanini, I.; Carmignano, S.M.; Cerulli, S.; Chisari, C.; et al. Robotic-assisted gait rehabilitation following stroke: A systematic review of current guidelines and practical clinical recommendations. Eur. J. Phys. Rehabil. Med. 2021, 57, 460–471. [Google Scholar] [CrossRef]
- Sawacha, Z.; Carraro, E.; Contessa, P.; Guiotto, A.; Masiero, S.; Cobelli, C. Relationship between clinical and instrumental balance assessments in chronic post-stroke hemiparesis subjects. J. Neuroeng. Rehabil. 2013, 10, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Q.; Zheng, Y.; Lian, P.; Guo, Y.; Huang, H.; Luo, Z.; Li, W.; Chen, H.; Li, S.; Lang, S.; et al. Quantitative Static and Dynamic Assessment of Balance Control in Stroke Patients. J. Vis. Exp. 2020, 159, e60884. [Google Scholar] [CrossRef] [PubMed]
- Li, S. Ankle and foot spasticity patterns in chronic stroke survivors with abnormal gait. Toxins 2020, 12, 646. [Google Scholar] [CrossRef] [PubMed]
- Gorst, T.; Lyddon, A.; Marsden, J.; Paton, J.; Morrison, S.; Cramp, M.; Freeman, J. Foot and ankle impairments affect balance and mobility in stroke (FAiMiS): The views and experiences of people with stroke. Disabil. Rehabil. 2016, 38, 589–596. [Google Scholar] [CrossRef]
- Chen, G.; Patten, C.; Kothari, D.H.; Zajac, F.E. Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait Posture 2005, 22, 51–56. [Google Scholar] [CrossRef]
- Collin, C.; Wade, D.T.; Davies, S.; Horne, V. The Barthel ADL Index: A reliability study. Int. Disabil. Stud. 1988, 10, 61–63. [Google Scholar] [CrossRef]
- Mehrholz, J.; Wagner, K.; Rutte, K.; Meissner, D.; Pohl, M. Predictive validity and responsiveness of the functional ambulation category in hemiparetic patients after stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1314–1319. [Google Scholar] [CrossRef]
- Green, J.; Forster, A.; Young, J. A test-retest reliability study of the Barthel Index, the Rivermead Mobility Index, the Nottingham Extended Activities of Daily Living Scale and the Frenchay Activities Index in stroke patients. Disabil. Rehabil. 2001, 23, 670–676. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Reporting | External Validity | Internal Validity | Power | Total Score | |
|---|---|---|---|---|---|---|---|
| Bias | Confounding | ||||||
| Louie DR et al., 2021 [31] | RCT | 11 | 3 | 6 | 5 | 1 | 26 |
| Calabrò RS et al., 2018 [28] | RCT | 10 | 3 | 5 | 4 | 1 | 23 |
| Wall A et al., 2019 [29] | RCT | 10 | 2 | 5 | 6 | 0 | 23 |
| Rojek A et al., 2019 [30] | RCT | 8 | 3 | 5 | 3 | 0 | 19 |
| Kotov SW et al., 2020 [26] | RCT | 9 | 1 | 4 | 2 | 0 | 16 |
| Kotov SW et al., 2021 [27] | RCT | 7 | 1 | 4 | 2 | 0 | 14 |
| Mizukami M et al., [24] 2017 | Pilot study | 10 | 1 | 3 | 0 | 0 | 14 |
| Yoshimoto T et al., [25] 2016 | Case Report | 8 | 1 | 2 | 1 | 0 | 12 |
| Bortole M et al., 2015. [32] | Pilot study | 8 | 0 | 2 | 0 | 0 | 10 |
| Study | Individuals Enrolled | Individuals Completing the Trial | Demographic Features | Clinical Features | |||||
|---|---|---|---|---|---|---|---|---|---|
| Gender | Age: Mean ± SD | TSS | Recovery Phase | Stroke Type | Hemiparesis Side | Walking Independence | |||
| Louie DR et al., 2021 [31] | 36 | 36 | M: 26, F: 10 | EXP group: 59.6 ± 15.8 | EXP group: 36.7 ± 19.0 d | Subacute | i: 25, h: 11 | l: 21, r: 15 | D: 36 |
| CTRL group: 55.3 ± 10.6 | CTRL group: 40.9 ± 19.8 d | ||||||||
| Calabrò RS et al., 2018 [28] | 40 | 40 | M: 23, F: 17 | EXP group: 69 ± 4 | EXP group: 10 ± 3 m | Chronic | i: 40 | l: 23, r: 17 | D + I: 40 |
| CTRL group: 67 ± 6 | CTRL group: 11 ± 3 m | ||||||||
| Rojek A et al., 2019 [30] | 60 | 44 | M: 25, F: 19 | 69 ± 7 | 4–12 m | Subacute & Chronic | i: 44 | l: 24, r: 20 | NR |
| Wall A et al., 2019 [29] | 34 | 28 | M: 23, F: 5 | 53 ± 12 | NR | Subacute | i: 16, h: 12 | l: 20, r: 8 | D: 28 |
| Mizukami M et al., 2017 [24] | 10 | 10 | M: 5, F: 3 | 58.6 ± 16.91 | 132.6 ± 18.6 d | Subacute | i: 3, h: 5 | l: 3, r: 5 | D: 7, I: 1 |
| Yoshimoto T et al., 2016 [25] | 1 | 1 | F: 1 | ~60 | 57 m | Chronic | h: 1 | l: 1 | I: 1 |
| Kotov SW et al., 2020 [26] | 47 | 41 | M: 28, F: 19 | 62.9 ± 11.0 | 2.2 ± 1.2 m | Subacute | i: 47 | l: 29, r: 18 | D + I: 47 |
| Kotov SW et al., 2021 [27] | 42 | 42 | NR | 61.2 ± 9.3 | NR | Subacute | i: 42 | NR | D + I: 42 |
| Bortole M et al., 2015 [32] | 3 | 3 | M: 3 | 48.7 ± 8.1 | 25.7 ± 29.8 m | Chronic | NR | l: 3 | NR |
| Study | Total Number of Session for Each Group | Total Duration for Each Group | Experimental Group | Control group | ||||
|---|---|---|---|---|---|---|---|---|
| Intervention | Single Session Duration (Minutes) | Frequency (Times per Week) | Intervention | Single Session Duration (Minutes) | Frequency (Times per Week) | |||
| Louie DR et al., 2021 [31] | 40 | 8 w | EksoGT + CT | EksoGT: 45 | 3 | CT | 60 | 4–5 |
| CT: 15 | ||||||||
| CT: 60 | 1–2 | |||||||
| Calabrò RS et al., 2018 [28] | 40 | 8 w | EksoGT + CT | Exo: 45 | 5 | CT | 105 | 5 |
| CT: 60 | ||||||||
| Rojek A et al., 2019 [30] | 20 | 4 w | EksoGT + CT | Exo: 45 | 5 | CT | 105 | 5 |
| CT: 60 | ||||||||
| Wall A et al., 2019 [29] | 16 | 4 w | HAL + CT | NR | 4 | CT | NR | 4 |
| Mizukami M et al., 2017 [24] | 20–25 | 5 w | HAL + CT | HAL: 20 | 5 | N | ||
| CT: 40 | ||||||||
| Yoshimoto T et al., 2016 [25] | NR | 24 w | CT | 40 | NR | N | ||
| CT + HAL | 60 | 1 | ||||||
| CT | 40 | NR | ||||||
| Kotov SW et al., 2020 [26] | 10 | 2 w | ExoAtlet | 10–30 | 5 | Cy-E | 10–30 | 5 |
| Kotov SW et al., 2021 [27] | 10 | 2 w | ExoAtlet + CT | Exo: 10–30 | 5 | CT | 20–40 | 5 |
| CT: 20–40 | ||||||||
| Bortole M et al., 2015 [32] | 12 | 4 w | H2 | 30 | 3 | N | ||
| Study (Device Name) | Main Goal | Clinical Assessment | Instrumental Assessment | Clinical Scale Results | Instrumental Assessment Results |
|---|---|---|---|---|---|
| Louie DR et al., 2021 [31] (Ekso GT) | To compare walking independence of non-ambulatory patients using an exoskeleton versus patients who received standard physical therapy. The secondary objective was to evaluate the effect of exoskeleton-based physical therapy on additional walking and mobility outcomes (e.g., speed), leg motor impairment, balance, cognition, post-stroke depression, and quality of life. | FAC, 5 MWT, 6 MWT, number of days to achieve unassisted ambulation, FMA-LE, BBS, PHQ, MoCA, SF-36 | N | post training: Exo vs. CT BBS: Exo > CT SF-36 physical: Exo > CT SF-36 mental: Exo < CT FU: Exo vs. CT BBS: Exo < CT SF-36 physical: Exo > CT SF-36 mental: Exo < CT | N |
| Calabrò RS et al., 2018 [28] (Ekso GT) | To obtain an improvement in lower limb gait and balance at the end of the training getting the MCID for the 10 MWT, RMI, and TUG scales. | 10 MWT, RMI, TUG | EMG data, EEG data, Gait analysis data (spatio-temporal parameters) | pre vs. post training: TUG: Exo group ↓*, OGT group ↓ Δ Exo vs. Δ OGT (Δ = post - pre training): TUG: Exo < OGT * | N |
| Rojek A et al., 2019 [30] (Ekso GT) | To evaluate the effects of Ekso GT exoskeleton-assisted gait training on balance, load distribution, and functional status of patients after ischemic stroke. | BI, RMI | COP data OE and CE: L, V, length of minor axis, length of major axis, ellipse angle, deviation X, deviation Y; load distribution: total load, forefoot load, backfoot load | pre vs. post training: BI: Exo group ↑ ***, CT group ↑ * pre training: Exo vs. CT BI exo < CT *** post training: Exo vs. CT BI exo < CT * | pre vs. post training: L-OE: Exo ↓, CT ↑; L-CE: Exo ↓, CT ↑ V-OE: Exo ↓, CT ↑; V-CE: Exo ↑, CT ↑ Length of minor axis-OE: Exo ↓, CT ↑; Length of minor axis-CE: Exo ↓, CT ↑ Length of major axis-OE: Exo ↓, CT ↑; Length of major axis-CE: Exo ↓, CT ↓ deviation X-OE: Exo ↓*, CT ↓: deviation X-CE: Exo ↓, CT: ↑ deviation Y-OE: Exo ↓ *, CT ↓; deviation Y-CE: Exo ↓, CT ↓ * pre training: Exo vs. CT L-OE: Exo < CT; L-CE: Exo > CT V-OE: Exo < CT; V-CE: Exo > CT Length of minor axis-OE: Exo > CT; Length of minor axis-CE: Exo > CT Length of major axis-OE: Exo > CT; Length of major axis-CE: Exo > CT deviation X-OE: Exo > CT; deviation X-CE: Exo > CT deviation Y-OE: Exo > CT **; deviation Y-CE: Exo > CT post training: Exo vs. CT L-OE: Exo < CT *; L-CE: Exo < CT V-OE: Exo < CT *; V-CE: Exo < CT Length of minor axis-OE: Exo < CT; Length of minor axis-CE: Exo > CT Length of major axis-OE: Exo = CT; Length of major axis-CE: Exo > CT deviation X-OE: Exo < CT; deviation X-CE: Exo < CT deviation Y-OE: Exo > CT *; deviation Y-CE: Exo > CT * |
| Wall A et al., 2019 [29] (HAL) | To explore long-term effects of HAL exoskeleton usage compared to conventional gait training in the subacute stage after stroke, regarding self-perceived functioning, disability and recovery and factors associated with self-perceived recovery. | NIHSS, SIS: strength (domain 1), ADL (domain 5), mobility (domain 6), and participation (domain 8), BBS | N | pre vs. FU: BBS: ↑ both groups BI: ↑ both groups Δ Exo vs. Δ CT (Δ = baseline - FU): BBS Exo > CT BI Exo < CT Exo vs. CT (FU): SIS ADL: Exo = CT Correlation between self-perceived mobility SIS and BBS | N |
| Mizukami M et al., 2017 [24] (HAL) | To determine whether gait training with a hybrid assistive limb (HAL) device was safe and could increase functional mobility and gait ability in subacute stroke patients. | MWS, SWS, 2 MWT, FAC, FMA, BBS, PCI | N | pre vs. post training: BBS: ↑ | N |
| Yoshimoto T et al., 2016 [25] (HAL) | To investigate the accumulated and sustained effects of Hybrid Assistive Limb gait training in a subject with chronic stroke. | 10 MWT, number of steps and cadence, TUG, FRT, 2 ST, BBS | N | pre vs. post CT period and pre vs. post HAL period: TUG ↓, BBS ↑, FRT ↑ post HAL-FU: TUG ↑, BBS ↑, FRT ↓ | N |
| Kotov SW et al., 2020 [26] (ExoAtlet) | To compare the effectiveness of restoration of walking function in patients with ischemic stroke using a lower limb exoskeleton and an active-passive pedal bicycle trainer. | MRC, MAS, BBS, HAI, 10 MWT, Rankin scale, BI | COP data: L, surface area of the statokinesiogram, energy consumption during Romberg Test with OE or CE; Biomechanichal and EMG data during walking. | pre vs. post training: BBS: Exo ↑ ***, Cy-E ↑ *** BI: Exo ↑ ***, Cy-E ↑ *** Δ Exo vs. Δ Moto (Δ = post - pre training): BBS: Exo > Cy-E * BI: Exo > Cy-E * | pre vs. post training: L-OE: Exo ↓ ***, Cy-E ↓ *** L-CE: Exo ↓ ***, Cy-E ↓ * S-OE: Exo ↓ ***, Cy-E ↓ *** S-CE: Exo ↓ *, Cy-E ↓ *** Ei-OE: Exo ↓ ***, Cy-E ↓ *** Ei-CE: Exo ↓ ***, Cy-E ↓ *** Δ Exo vs. Δ Moto (Δ = post - pre training): L-OE: Exo > Cy-E *** |
| Kotov SW et al., 2021 [27] (ExoAtlet) | To evaluate the effectiveness of ExoAtlet usage in restoring the functional and motor activity, including the walking function, in patients after ischemic stroke in the middle cerebral artery, compared with the traditional methods of rehabilitation. | MRC, Rankin scale, BI, HAI, BBS, 10 MWT | COP data: L, surface area of the statokinesiogram, energy consumption during Romberg Test with OE or CE | pre training: Exo vs. CT BBS: Exo = CT BI: Exo = CT post training: Exo vs. CT BBS: Exo > CT BI: Exo > CT Δ Exo vs. Δ CT (Δ = post - pre training): BBS: Exo > CT * BI: Exo > CT | pre training: Exo vs. CT COP data: L-OE: Exo < CT; L-CE: Exo < CT S-OE: Exo < CT; S-CE: Exo < CT Ei-OE: Exo < CT; Ei-CE: Exo < CT * post training: Exo vs. CT COP data: L-OE: Exo < CT ***; L-CE: Exo < CT * S-OE: Exo < CT ***; S-CE: Exo < CT ** Ei-OE: Exo < CT ***; Ei-CE: Exo < CT *** |
| Bortole M et al., 2015 [32] (H2) | To demonstrate safety and usability of the H2 robotic exoskeleton in post-stroke hemiparetic patients in a rehabilitation framework. | BBS, BI, FGI, FMA-LE, TUG, 6 MWT | N | pre vs. post training: BBS: patient 1 ↑, patient 2 e 3 = TUG: patient 1 ↑, patient 2 e 3 ↓ BI ADL: patient 1 e 3 = patient 2 ↑ | N |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorusso, M.; Tramontano, M.; Casciello, M.; Pece, A.; Smania, N.; Morone, G.; Tamburella, F. Efficacy of Overground Robotic Gait Training on Balance in Stroke Survivors: A Systematic Review and Meta-Analysis. Brain Sci. 2022, 12, 713. https://doi.org/10.3390/brainsci12060713
Lorusso M, Tramontano M, Casciello M, Pece A, Smania N, Morone G, Tamburella F. Efficacy of Overground Robotic Gait Training on Balance in Stroke Survivors: A Systematic Review and Meta-Analysis. Brain Sciences. 2022; 12(6):713. https://doi.org/10.3390/brainsci12060713
Chicago/Turabian StyleLorusso, Matteo, Marco Tramontano, Matteo Casciello, Andrea Pece, Nicola Smania, Giovanni Morone, and Federica Tamburella. 2022. "Efficacy of Overground Robotic Gait Training on Balance in Stroke Survivors: A Systematic Review and Meta-Analysis" Brain Sciences 12, no. 6: 713. https://doi.org/10.3390/brainsci12060713