
A Depression Prediction Algorithm Based on Spatiotemporal Feature of EEG Signal



Abstract
:1. Introduction
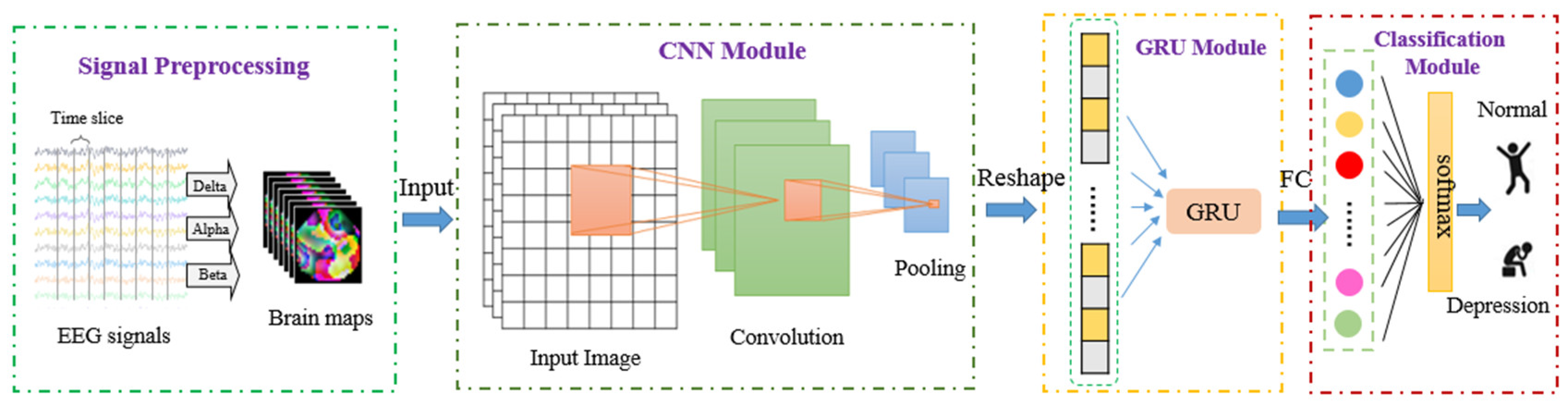
- In signal preprocessing, the signal frequency domain information, the space domain information between the electrodes of the acquisition equipment, and timing characteristics are fully utilized. The extraction of features with this strategy can be implemented automatically without manual acquisition. The model explores the GRU network with CNN layers whereby the CNN layers extract features and the GRU block provides sequence learning.
- A model was proposed with relatively few layers (6 layers), and consequently, a relatively low level of complexity.
2. Materials and Methods
2.1. Subjects
2.2. Proposed Classification Method
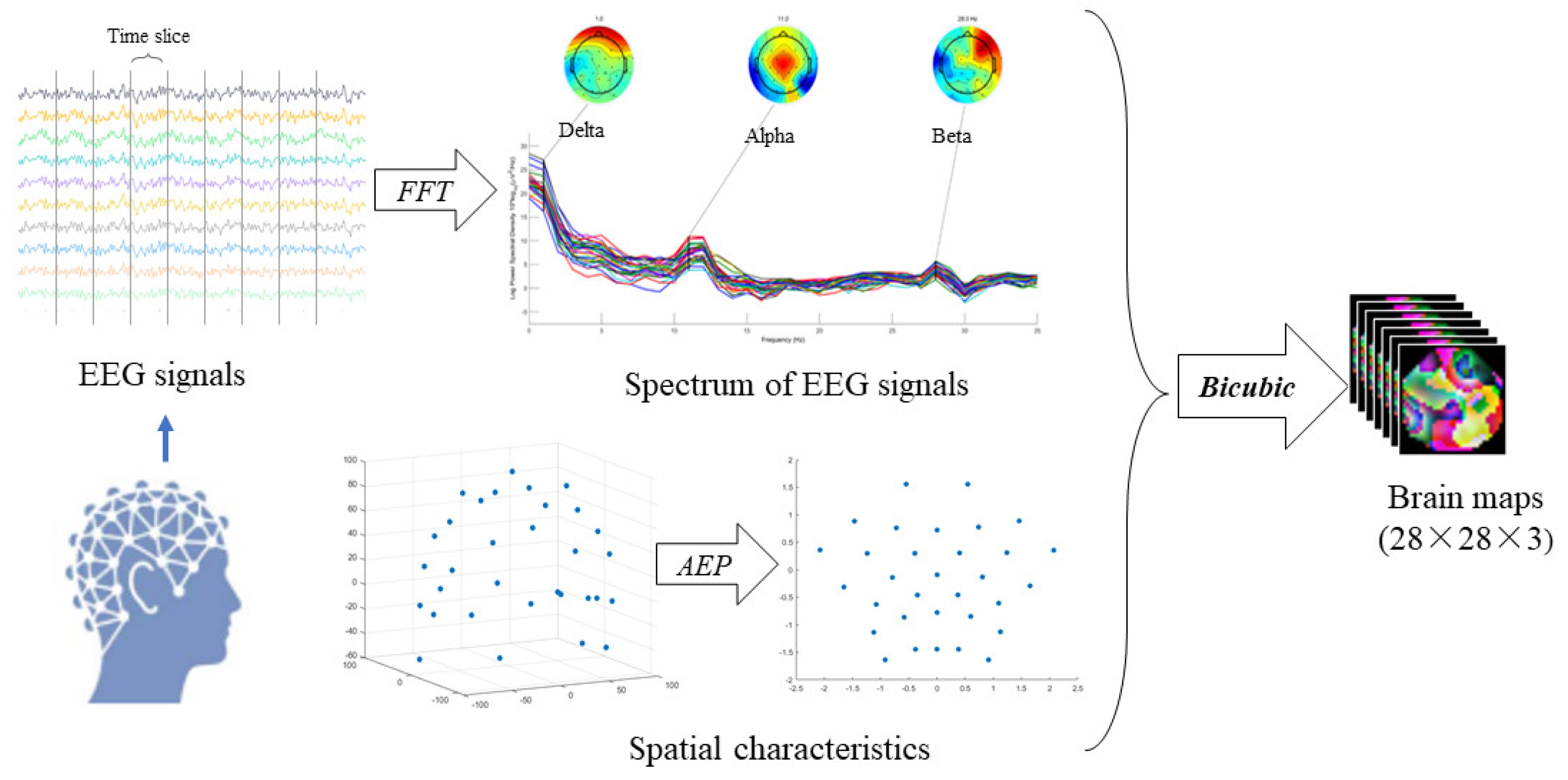
2.2.1. EEG Signal Preprocessing
- The EEG signal was processed by Fast ICA to obtain several independent components whereby the independent components include the independent component containing the EEG artifact and the independent component without the EEG artifact;
- Wavelet transforms and the differential evolution algorithm were used to process the independent component containing the artifact to obtain the artifact component;
- Based on wavelet reconstruction and inverse transformation, an EEG signal was obtained to remove the artifacts according to the artifact component.
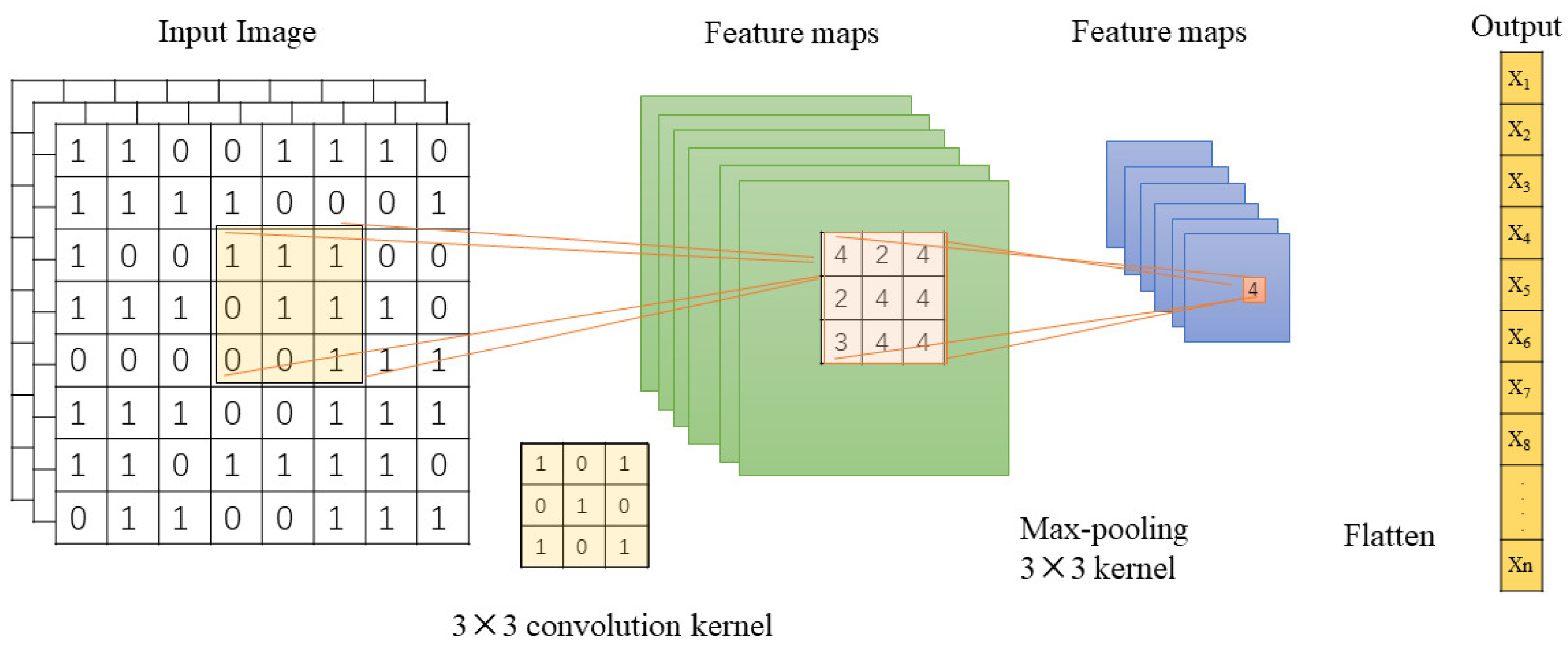
2.2.2. Extraction Using CNN
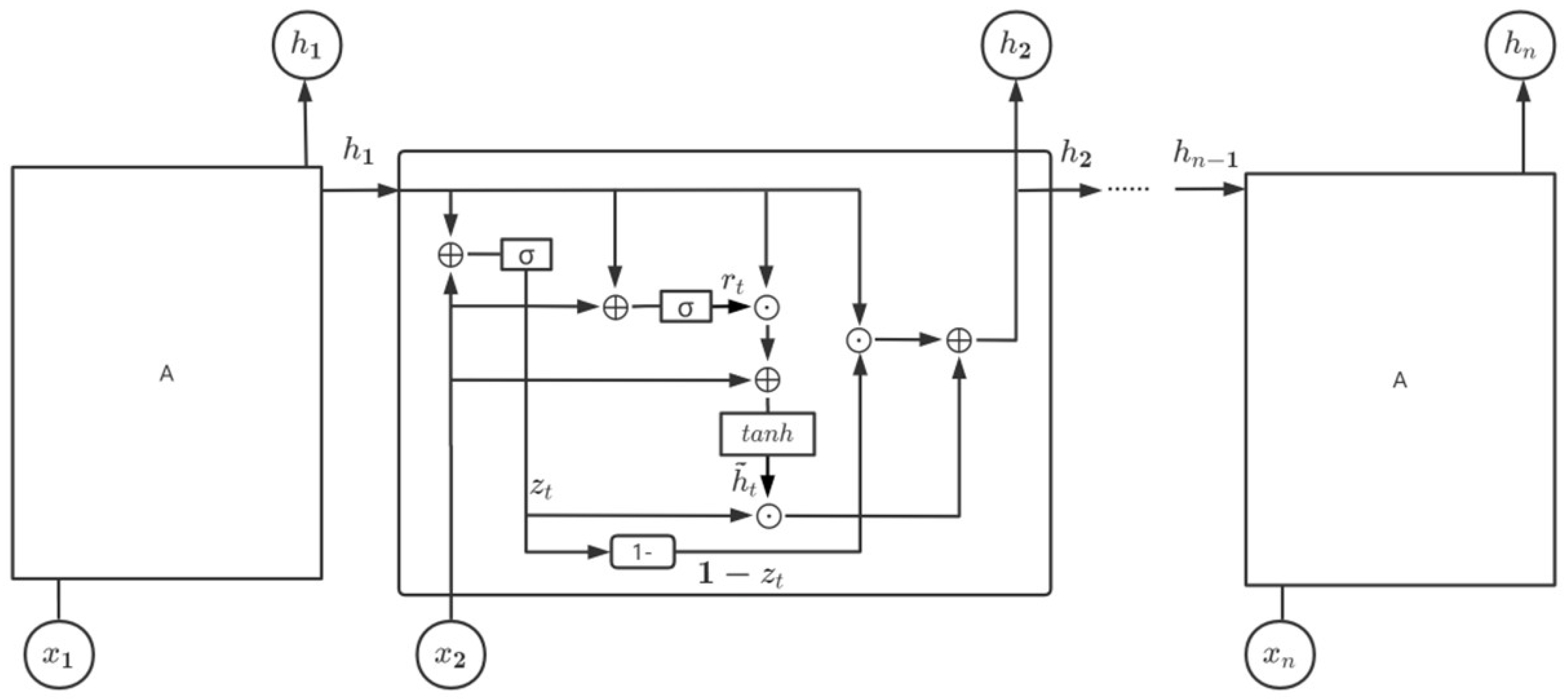
2.2.3. Learning Model with GRU
2.2.4. Validation
3. Results
3.1. The Effect of Data Augmentation
3.2. The Influence of The number of CNN Layers
3.3. Comparison with Other Methods
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; Technical Report; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Friedrich, M.J. Depression is the leading cause of disability around the world. JAMA 2017, 317, 1517. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- World Health Organization. Depression: A Global Crisis; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Preedy, V.R.; Watson, R.R. International Classification of Disease; Springer: New York, NY, USA, 2010. [Google Scholar]
- Arbanas, G. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Association: Washington, DC, USA, 2015. [Google Scholar]
- Jur Jurysta, F.; Kempenaers, C.; Lancini, J.; Lanquart, J.P.; Van De Borne, P.; Linkowski, P. Altered interaction between cardiac vagal influence and delta sleep eeg suggests an altered neuroplasticity in patients suffering from major depressive disorder. Acta Psychiatr. Scand. 2010, 121, 236–239. [Google Scholar] [CrossRef]
- Saeidi, M.; Karwowski, W.; Farahani, F.V.; Fiok, K.; Taiar, R.; Hancock, P.A.; Al-Juaid, A. Neural Decoding of EEG Signals with Machine Learning: A Systematic Review. Brain Sci. 2021, 11, 1525. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Achuth, P.V.; Deb, D.; Puthankattil, S.D.; Acharya, U.R. An Automated Diagnosis of Depression Using Three-Channel Bandwidth-Duration Localized Wavelet Filter Bank with EEG Signals. Cogn. Syst. Res. 2018, 52, 508–520. [Google Scholar] [CrossRef]
- Liao, S.C.; Wu, C.T.; Huang, H.C.; Cheng, W.-T.; Liu, Y.-H. Major Depression Detection from EEG Signals Using Kernel Eigen-Filter-Bank Common Spatial Patterns. Sensors 2017, 17, 1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhat, S.; Acharya, U.R.; Hagiwara, Y.; Dadmehr, N.; Adeli, H. Parkinson’s disease: Cause factors, measurable indicators, and early diagnosis. Comput. Biol. Med. 2018, 102, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Acharya, U.R.; Vinitha Sree, S.; Swapna, G.; Martis, R.J.; Suri, J.S. Automated EEG analysis of epilepsy: A review. Knowl.-Based Syst. 2013, 45, 147–165. [Google Scholar] [CrossRef]
- Kayser, J.; Tenke, C.E. In search of the Rosetta Stone for scalp EEG: Converging on reference-free techniques. Clin. Neurophysiol. 2010, 121, 1973–1975. [Google Scholar] [CrossRef] [Green Version]
- Acharya, U.R.; Hagiwara, Y.; Deshpande, S.N.; Suren, S.; Koh, J.E.W.; Oh, S.L.; Arunkumar, N.; Ciaccio, E.J.; Lim, C.M. Characterization of focal EEG signals: A review. Future Gener. Comput. Syst. 2019, 91, 290–299. [Google Scholar] [CrossRef]
- Gu, X.; Yang, B.; Gao, S.; Yan, L.F.; Xu, D.; Wang, W. Application of bi-modal signal in the classification and recognition of drug addiction degree based on machine learning. Math. Biosci. Eng. 2021, 18, 6926–6940. [Google Scholar] [CrossRef]
- Gao, Y.; Cao, Z.; Liu, J.; Zhang, J. A novel dynamic brain network in arousal for brain states and emotion analysis. Math. Biosci. Eng. 2021, 18, 7440–7463. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y. Comparative analysis of electroencephalogram in patients with neurological disorders and depression. J. Shanxi Med. Univ. 2005, 36, 96–97. [Google Scholar]
- Siuly, S.; Li, Y.; Zhang, Y. EEG signal analysis and classification. IEEE Trans. Neural. Syst. Rehabil. Eng. 2016, 11, 141–144. [Google Scholar]
- Campisi, P.; La Rocca, D. Brain waves for automatic biometric-based user recognition. IEEE Trans. Inform. Forensics Secur. 2014, 9, 782–800. [Google Scholar] [CrossRef]
- Kumar, J.S.; Bhuvaneswari, P. Analysis of electroencephalography (EEG) signals and its categorization–A study. Procedia Eng. 2012, 38, 2525–2536. [Google Scholar] [CrossRef] [Green Version]
- Novik, O.; Smirnov, F.; Volgin, M. Structures of the brain. In Electromagnetic Geophysical Fields; Springer: Cham, Switzerland, 2019; pp. 69–89. [Google Scholar]
- Khosla, A.; Khandnor, P.; Chand, T. A comparative analysis of signal processing and classification methods for different applications based on EEG signals. Biocybern. Biomed. Eng. 2020, 40, 619–690. [Google Scholar] [CrossRef]
- Bachmann, M.; Päeske, L.; Kalev, K.; Aarma, K.; Lehtmets, A.; Ööpik, P.; Lass, J.; Hinrikus, H. Methods for classifying depression in single channel EEG using linear and nonlinear signal analysis. Comput. Methods Programs Biomed. 2018, 155, 11–17. [Google Scholar] [CrossRef]
- Koller-Schlaud, K.; Ströhle, A.; Bärwolf, E.; Behr, J.; Rentzsch, J. EEG frontal asymmetry and theta power in unipolar and bipolar depression. J. Affect. Disord. 2020, 276, 501–510. [Google Scholar] [CrossRef]
- Kang, M.; Kwon, H.; Park, J.H.; Kang, S.; Lee, Y. Deep-asymmetry: Asymmetry matrix image for deep learning method in pre-screening depression. Sensors 2020, 20, 6526. [Google Scholar] [CrossRef]
- Liu, W.; Zhang, C.; Wang, X.; Xu, J.; Chang, Y.; Ristaniemi, T.; Cong, F. Functional connectivity of major depression disorder using ongoing EEG during music perception. Clin. Neurophysiol. 2020, 131, 2413–2422. [Google Scholar] [CrossRef]
- Grin-Yatsenko, V.A.; Baas, I.; Ponomarev, V.A.; Kropotov, J.D. Independent component approach to the analysis of EEG recordings at early stages of depressive disorders. Clin. Neurophysiol. 2010, 121, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Heinsfeld, A.S.; Franco, A.R.; Craddock, R.C.; Buchweitz, A.; Meneguzzi, F. Identification of autism spectrum disorder using deep learning and the ABIDE dataset. Neuroimage Clin. 2018, 17, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Grotegerd, D.; Suslow, T.; Bauer, J.; Ohrmann, P.; Arolt, V.; Stuhrmann, A.; Heindel, W.; Kugel, H.; Dannlowski, U. Discriminating unipolar and bipolar depression by means of fMRI and pattern classification: A pilot study. Eur. Arch. Psychiatry Clin. Neurosci. 2013, 263, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Kermany, D.S.; Goldbaum, M.; Cai, W.; Valentim, C.C.S.; Liang, H.; Baxter, S.L.; McKeown, A.; Yang, G.; Wu, X.; Yan, F.; et al. Identifying medical diagnoses and treatable diseases by image-based deep learning. Cell 2018, 172, 1122. [Google Scholar] [CrossRef] [PubMed]
- Hannesdóttir, D.K.; Doxie, J.; Bell, M.A.; Ollendick, T.H.; Wolfe, C.D. A longitudinal study of emotion regulation and anxiety in middle childhood: Associations with frontal EEG asymmetry in early childhood. Dev. Psychobiol. 2010, 52, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Avram, J.; Baltes, F.R.; Miclea, M.; Miu, A.C. Frontal EEG activation asymmetry reflects cognitive biases in anxiety: Evidence from an emotional face Stroop task. Appl. Psychophysiol. Biofeedback 2010, 35, 285–292. [Google Scholar] [CrossRef]
- Thibodeau, R.; Jorgensen, R.S.; Kim, S. Depression, anxiety, and resting frontal EEG asymmetry: A meta-analytic review. Abnorm. Psychol. 2006, 115, 715–729. [Google Scholar] [CrossRef] [Green Version]
- Hosseinifard, B.; Moradi, M.H.; Rostami, R. Classifying depression patients and normal subjects using machine learning techniques and nonlinear features from EEG signal. Comput. Methods Programs Biomed. 2013, 109, 339–345. [Google Scholar] [CrossRef]
- Field, T.; Diego, M. Maternal depression effects on infant frontal EEG asymmetry. Int. J. Neurosci. 2008, 118, 1081–1108. [Google Scholar] [CrossRef]
- Iosifescu, D.V.; Greenwald, S.; Devlin, P.; Mischoulon, D.; Denninger, J.W.; Alpert, J.; Fava, M. Frontal EEG predictors of treatment outcome in major depressive disorder. Eur. Neuropsychopharmacol. 2009, 19, 772–777. [Google Scholar] [CrossRef]
- Bisch, J.; Kreifelts, B.; Bretscher, J.; Wildgruber, D.; Fallgatter, A.; Ethofer, T. Emotion perception in adult attention-deficit hyperactivity disorder. Neural Transm. 2016, 123, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Yahya, N.; Musa, H.; Zhong, Y.O.; Ong, Z.Y.; Elamvazuthi, I. Classification of Motor Functions from Electroencephalogram (EEG) Signals Based on an Integrated Method Comprised of Common Spatial Pattern and Wavelet Transform Framework. Sensors 2019, 19, 4878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadlou, M.; Adeli, H.; Adeli, A. Fractality analysis of frontal brain in major depressive disorder. Int. J. Psychophysiol. 2012, 85, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Faust, O.; Ang, P.C.A.; Puthankattil, S.D.; Joseph, P.K. Depression diagnosis support system based on EEG signal entropies. Mech. Med. Biol. 2014, 14, 1450035. [Google Scholar] [CrossRef]
- Bairy, G.M.; Niranjan, U.; Puthankattil, S.D. Automated classification of depression EEG signals using wavelet entropies and energies. Mech. Med. Biol. 2016, 16, 1650035. [Google Scholar] [CrossRef]
- Acharya, U.R.; Oh, S.L.; Hagiwara, Y.; Tan, J.H.; Adeli, H.; Subha, D.P. Automated EEG-based screening of depression using deep convolutional neural network. Comput. Methods Programs Biomed. 2018, 161, 103–113. [Google Scholar] [CrossRef]
- Ay, B.; Yildirim, O.; Talo, M.; Baloglu, U.B.; Aydin, G.; Puthankattil, S.D.; Acharya, U.R. Automated depression detection using deep representation and sequence learning with EEG signals. Med. Syst. 2019, 4, 205. [Google Scholar] [CrossRef]
- Sharma, G.; Parashar, A.; Joshi, A.M. DepHNN: A novel hybrid neural network for electroencephalogram (EEG)-based screening of depression. Biomed. Signal Processing Control 2021, 66, 102393. [Google Scholar] [CrossRef]
- Cai, H.; Gao, Y.; Sun, S.; Li, N.; Tian, F.; Xiao, H.; Li, J.; Yang, Z.; Li, X.; Zhao, Q.; et al. MODMA dataset: A multi-modal open dataset for mental disorder analysis. arXiv 2020, arXiv:2002.09283. [Google Scholar]
- Almars, A.M. Attention-Based Bi-LSTM Model for Arabic Depression Classification. CMC-Comput. Mater. Contin. 2022, 71, 3091–3106. [Google Scholar] [CrossRef]
- Li, X.; Zhang, X.; Zhu, J.; Mao, W.; Sun, S.; Wang, Z.; Xia, C.; Hu, B. Depression recognition using machine learning methods with different feature generation strategies. Artif. Intell. Med. 2019, 99, 101696. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A. 3D to 2D bijection for spherical objects under equidistant fisheye projection. Comput. Vis. Image Underst. 2014, 125, 172–183. [Google Scholar] [CrossRef]
- Wang, Z.; Du, X.; Wu, Q.; Dong, Y. Research on the multi-classifier features of the motor imagery EEG signals in the brain computer interface. In Proceedings of the Tenth International Conference on Digital Image Processing (ICDIP 2018), International Society for Optics and Photonics, Shanghai, China, 11–14 May 2018. [Google Scholar]
- Cho, K.; Van Merrienboer, B.; Gulcehre, C.; Bahdanau, D.; Bougares, F.; Schwenk, H.; Bengio, Y. Learning Phrase Representations using RNN Encoder-Decoder for Statistical Machine Translation. In Proceedings of the Empiricial Methods in Natural Language Processing (EMNLP 2014), Doha, Qatar, 25–29 October 2014. [Google Scholar]
- Shuting, S.; Jianxiu, L.; Huayu, C.; Tao, G.; Xiaowei, L.; Bin, H. A study of resting-state EEG biomarkers for depression recognition. arXiv 2020, arXiv:2002.11039. [Google Scholar]
- Wang, Y.; Liu, F.; Yang, L. EEG-Based Depression Recognition Using Intrinsic Time-scale Decomposition and Temporal Convolution Network. In Proceedings of the Fifth International Conference on Biological Information and Biomedical Engineering, Hangzhou, China, 20–21 July 2021. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Properties | MODMA Dataset | Private Dataset |
|---|---|---|
| No. of participants | 53 | 32 |
| No. of depression cases | 24 | 16 |
| Depression diagnostics | Diagnosis | Diagnosis, BDI |
| Male/female ratio | 33/20 | 16/16 |
| No. of channels | 128 | 16 |
| Sampling rate, Hz | 250 | 100 |
| Method | Data Set | AC (Mean ± Std) | SE (Mean ± Std) | SP (Mean ± Std) | F1 (Mean ± Std) |
|---|---|---|---|---|---|
| 1s slicing | MODMA | 89.63 ± 1.3 | 90.24 ±1.9 | 89.63 ± 1.3 | 90.19 ± 1.3 |
| private dataset | 88.56 ± 1.3 | 88.56 ± 1.5 | 88.54 ± 1.8 | 88.68 ± 1.5 | |
| 2s slicing | MODMA | 90.62 ± 2.1 | 87.81 ± 3.2 | 87.48 ± 2.1 | 88.79 ± 2.1 |
| private dataset | 89.84 ± 2.1 | 87.82 ± 3.4 | 87.36 ± 1.7 | 88.79 ± 2.1 | |
| 3s slicing | MODMA | 87.01 ± 1.5 | 87.01 ± 1.5 | 87.01 ± 1.5 | 88.01 ± 1.5 |
| private dataset | 87.72 ± 1.6 | 87.32 ± 1.6 | 86.72 ± 1.6 | 88.72 ± 1.6 |
| Layers | Time (s) | Parameters | AC | SE | SP | F1 |
|---|---|---|---|---|---|---|
| 1 | 172 | 896 | 87.98 | 88.38 | 88.98 | 87.79 |
| 2 | 224 | 10,272 | 86.68 | 85.46 | 85.48 | 85.63 |
| 3 | 340 | 28,768 | 75.68 | 78.18 | 78.16 | 78.58 |
| Methods | Features | Accuracy (%) |
|---|---|---|
| LR + ReliefF [51] | linear | 66.40 |
| LR + ReliefF [51] | nonlinear | 67.17 |
| LR + ReliefF [51] | PLI | 82.31 |
| LR + ReliefF [51] | Linear + PLI | 80.99 |
| LR + ReliefF [51] | Nonlinear + PLI | 81.79 |
| TCN [52] | ITD + statistical features | 85.23 |
| L-TCN [52] | ITD + statistical features | 86.87 |
| BrainMap + CNN + GRU | BrainMap features | 89.63 |
| Method | Dataset | AC | SE | SP | F1 |
|---|---|---|---|---|---|
| SVM | MODMA | 78.12 | 78.12 | 78.12 | 77.31 |
| Private dataset | 75.18 | 74.92 | 75.12 | 74.31 | |
| GRU | MODMA | 83.12 | 86.67 | 76.57 | 87.55 |
| Private dataset | 81.36 | 82.49 | 78.91 | 82.55 | |
| CNN | MODMA | 84.32 | 85.76 | 79.86 | 87.96 |
| Private dataset | 82.34 | 84.35 | 79.91 | 83.31 | |
| TCN | MODMA | 85.23 | 89.67 | 76.57 | 87.55 |
| Private dataset | 82.38 | 82.47 | 82.47 | 82.55 | |
| L-TCN | MODMA | 86.87 | 90.15 | 83.83 | 90.51 |
| Private dataset | 85.64 | 85.87 | 81.23 | 86.55 | |
| BrainMap + CNN | MODMA | 87.34 | 89.48 | 88.56 | 87.37 |
| Private dataset | 83.65 | 82.59 | 82.31 | 82.55 | |
| BrainMap + CNN + GRU | MODMA | 89.63 | 90.24 | 89.63 | 90.19 |
| Private dataset | 88.56 | 88.56 | 88.54 | 88.68 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, W.; Jia, K.; Wang, Z.; Ma, Z. A Depression Prediction Algorithm Based on Spatiotemporal Feature of EEG Signal. Brain Sci. 2022, 12, 630. https://doi.org/10.3390/brainsci12050630
Liu W, Jia K, Wang Z, Ma Z. A Depression Prediction Algorithm Based on Spatiotemporal Feature of EEG Signal. Brain Sciences. 2022; 12(5):630. https://doi.org/10.3390/brainsci12050630
Chicago/Turabian StyleLiu, Wei, Kebin Jia, Zhuozheng Wang, and Zhuo Ma. 2022. "A Depression Prediction Algorithm Based on Spatiotemporal Feature of EEG Signal" Brain Sciences 12, no. 5: 630. https://doi.org/10.3390/brainsci12050630