

Short- and Long-Term Efficacy and Safety of Deep-Brain Stimulation in Parkinson’s Disease Patients aged 75 Years and Older
Abstract
:1. Introduction
1.1. Materials and Methods
1.1.1. Patients
1.1.2. Inclusion and Exclusion Criteria
1.1.3. Surgical Methods
1.1.4. Statistical Analysis
2. Results
2.1. Clinical Characteristics of DBS in Elderly PD Patients
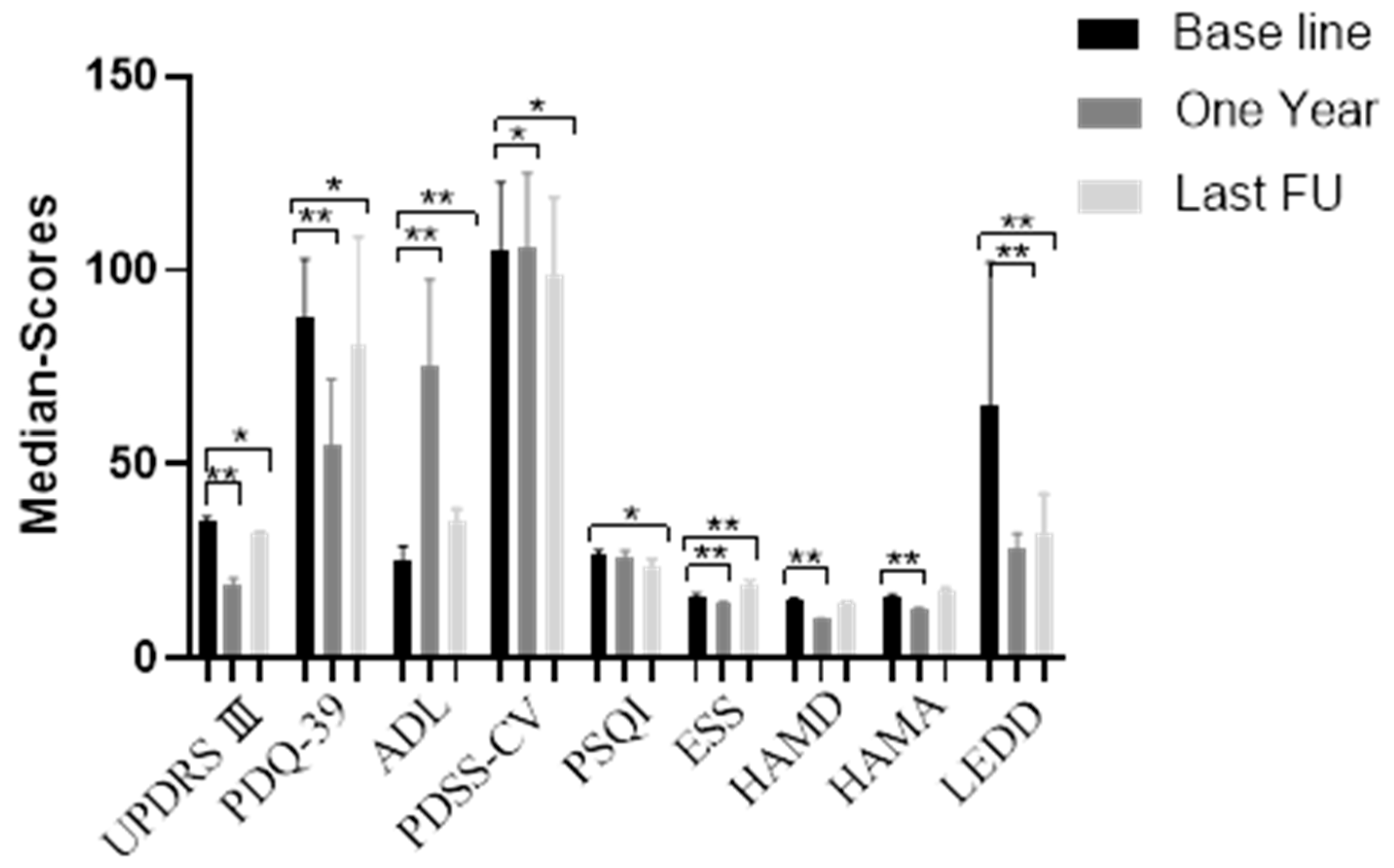
2.2. Postoperative Efficacy of DBS in Elderly PD Patients
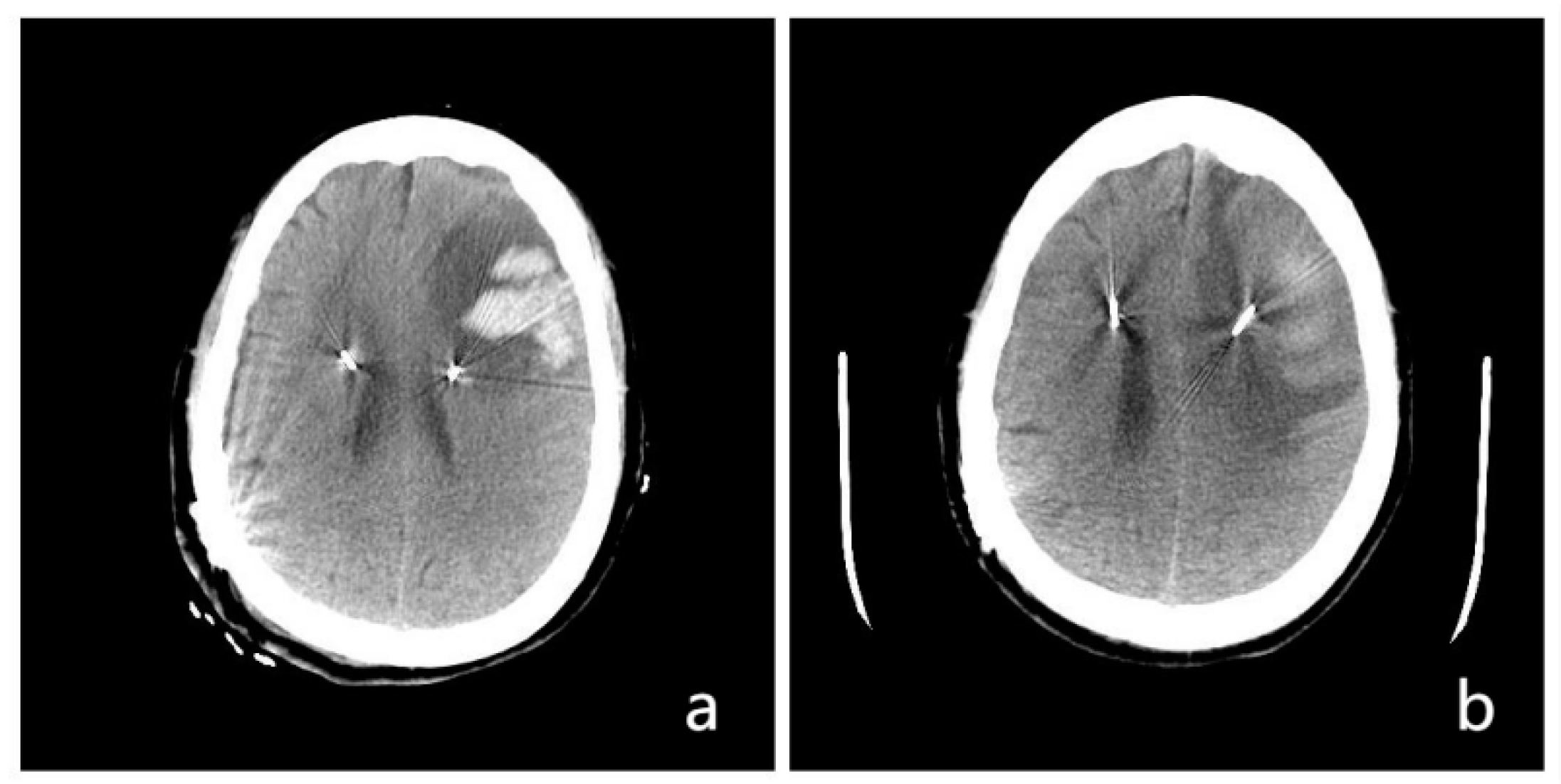
2.3. Complications of DBS Surgery in Older (≥75 years old) PD Patients
3. Discussion
3.1. Motor Symptom Changes after DBS
3.2. LEDD Changes after DBS
3.3. Non-Motor Symptom Changes after DBS
3.4. Complications
Future Work
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PD | Parkinson’s disease |
| DBS | Deep-brain stimulation |
| LEDD | Levodopa equivalent daily dose |
| UPDRS III | Unified Parkinson Disease Rating Scale III |
| ADL | Activities of Daily Living |
| PDSS-CV | Parkinson’s Disease Sleep Scale—Chinese version |
| PDQ-39 | 39-item Parkinson’s Disease Questionnaire |
| PSQI | Pittsburgh Sleep Quality Index |
| ESS | Epworth Sleeping Scale |
| MoCA | Montreal Cognitive Assessment |
| HAMA | Hamilton Anxiety Scale |
| HAMD | Hamilton Depression Scale |
| DOS | Duration of symptoms |
| Vin | Thalamic ventral intermediate nucleus |
| STN | Subthalamic nucleus |
| GPi | Globus pallidus internus |
| FU | Follow-up |
References
- Weaver, F.M.; Follett, K.; Stern, M.; Hur, K.; Harris, C.; Marks, W.J.; Rothlind, J., Jr.; Sagher, O.; Reda, D.; Moy, C.S.; et al. Bilateral deep brain stimulation vs best medical therapy for patients with advanced Parkinson disease: A randomized controlled trial. JAMA 2009, 301, 63–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Follett, K.A.; Weaver, F.M.; Stern, M.; Hur, K.; Harris, C.L.; Luo, P.; Marks, W.J.; Rothlind, J., Jr.; Sagher, O.; Moy, C.; et al. Pallidal versus subthalamic deep-brain stimulation for Parkinson’s disease. N. Engl. J. Med. 2010, 362, 2077–2091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.; Gill, S.; Varma, T.; Jenkinson, C.; Quinn, N.; Mitchell, R.; Scott, R.; Ives, N.; Rick, C.; Daniels, J.; et al. Deep brain stimulation plus best medical therapy versus best medical therapy alone for advanced Parkinson’s disease (PD SURG trial): A randomised, open-label trial. Lancet Neurol. 2010, 9, 581–591. [Google Scholar] [CrossRef] [Green Version]
- Odekerken, V.J.; van Laar, T.; Staal, M.J.; Mosch, A.; Hoffmann, C.F.; Nijssen, P.C.; Beute, G.N.; van Vugt, J.P.; Lenders, M.W.; Contarino, M.F.; et al. Subthalamic nucleus versus globus pallidus bilateral deep brain stimulation for advanced Parkinson’s disease (NSTAPS study): A randomised controlled trial. Lancet Neurol. 2013, 12, 37–44. [Google Scholar] [CrossRef]
- Rughani, A.; Schwalb, J.M.; Sidiropoulos, C.; Pilitsis, J.; Ramirez-Zamora, A.; Sweet, J.A.; Mittal, S.; Espay, A.J.; Martinez, J.G.; Abosch, A.; et al. Congress of neurological surgeons systematic review and evidencebased guideline on subthalamic nucleus and globus pallidus internus deep brain stimulation for the treatment of patients with parkinson’s disease: Executive summary. Neurosurgery 2018, 82, 753–756. [Google Scholar] [CrossRef] [Green Version]
- Deuschl, G.; Paschen, S.; Witt, K. Clinical outcome of deep brain stimulation for Parkinson’s disease. Handb. Clin. Neurol. 2013, 116, 107–128. [Google Scholar] [PubMed]
- Deuschl, G.; Schüpbach, M.; Knudsen, K.; Pinsker, M.O.; Cornu, P.; Rau, J.; Agid, Y.; Schade-Brittinger, C. Stimulation of the subthalamic nucleus at an earlier disease stage of Parkinson’s disease: Concept and standards of the EARLYSTIM-study. Park. Relat. Disord. 2013, 19, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Deuschl, G.; Schade-Brittinger, C.; Krack, P.; Volkmann, J.; Schäfer, H.; Bötzel, K.; Daniels, C.; Deutschländer, A.; Dillmann, U.; Eisner, W.; et al. A randomized trial of deep brain stimulation for Parkinson’s disease. N. Engl. J. Med. 2006, 355, 896–908. [Google Scholar] [CrossRef] [Green Version]
- Figueiras-Méndez, R.; Marín-Zarza, F.; Antonio Molina, J.; Jiménez-Jiménez, F.J.; Ortí-Pareja, M.; Magariños, C.; López-Pino, M.A.; Martínez, V. Subthalamic nucleus stimulation improves directly levodopa induced dyskinesias in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1999, 66, 549–550. [Google Scholar] [CrossRef]
- Okun, M.S.; Fernandez, H.H.; Wu, S.S.; Kirsch-Darrow, L.; Bowers, D.; Bova, F.; Suelter, M.; Jacobson, C.E.; Wang, X., IV; Gordon, C.W.; et al. Cognition and mood in Parkinson’s disease in subthalamic nucleus versus globus pallidus interna deep brain stimulation: The COMPARE trial. Ann. Neurol. 2009, 65, 586–595. [Google Scholar] [CrossRef]
- Anderson, V.C.; Burchiel, K.J.; Hogarth, P.; Favre, J.; Hammerstad, J.P. Pallidal vs subthalamic nucleus deep brain stimulation in Parkinson disease. Arch. Neurol. 2005, 62, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Mathkour, M.; Garces, J.; Scullen, T.; Hanna, J.; Valle-Giler, E.; Kahn, L.; Arrington, T.; Houghton, D.; Lea, G.; Biro, E.; et al. Short- and Long-Term Outcomes of Deep Brain Stimulation in Patients 70 Years and Older with Parkinson Disease. World Neurosurg. 2017, 97, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, P.; Aquino, C.C.; Fasano, A. Surgical Management of Parkinson’s Disease in the Elderly. Mov. Disord. Clin. Pract. 2021, 8, 500–509. [Google Scholar] [CrossRef]
- Sharma, V.D.; Lyons, K.E.; Nazzaro, J.M.; Pahwa, R. Deep brain stimulation of the subthalamic nucleus in Parkinson’s disease patients over 75 years of age. J. Neurol. Sci. 2019, 399, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Mattson, M.P.; Arumugam, T.V. Hallmarks of brain aging: Adaptive and pathological modification by metabolic states. Cell Metab. 2018, 27, 1176–1199. [Google Scholar] [CrossRef] [Green Version]
- Parkinson’s Disease, Movement Disorder Society Task Forceon Rating Scalesfor. The Unified Parkinson’s Disease Rating Scale (UPDRS): Status and recommendations. Mov. Disord. Off. J. Mov. Disord. Soc. 2003, 18, 738–750. [Google Scholar] [CrossRef]
- Jenkinson, C.; Fitzpatrick, R.; Peto, V.; Greenhall, R.; Hyman, N. The Parkinson’s Disease Questionnaire (PDQ-39): Development and validation of a Parkinson’s disease summary index score. Age Ageing 1997, 26, 353–357. [Google Scholar] [CrossRef] [Green Version]
- Eto, F.; Tanaka, M.; Chishima, M.; Igarashi, M.; Mizoguchi, T.; Wada, H.; Iijima, S. Comprehensive activities of daily living (ADL) index for the elderly. Nihon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 1992, 29, 841–848. [Google Scholar] [CrossRef] [Green Version]
- Wang, G.; Cheng, Q.; Zeng, J.; Bai, L.; Liu, G.D.; Zhang, Y.; Tan, Y.Y.; Pan, J.; Hong, Z.; Wang, Y.; et al. Sleep disorders in Chinese patients with Parkinson’s disease: Validation study of a Chinese version of Parkinson’s disease sleep scale. J. Neurol. Sci. 2008, 271, 153–157. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Matza, L.S.; Morlock, R.; Sexton, C.; Malley, K.; Feltner, D. Identifying HAM-A cutoffs for mild, moderate, and severe generalized anxiety disorder. International Journal of Methods in Psychiatric Research Int. J. Methods Psychiatr. 2010, 19, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, M.; Martinez, J.H.; Young, D.; Chelminski, I.; Dalrymple, K. Severity classification on the Hamilton Depression Rating Scale. J. Affect. Disord. 2013, 150, 384–388. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2010, 25, 2649–2653. [Google Scholar] [CrossRef]
- Defer, G.L.; Widner, H.; Marie, R.M.; Remy, P.; Levivier, M. Core assessment program for surgical interventional therapies in Parkinson’s disease (CAPSIT-PD). Mov. Disord. 1999, 14, 572–584. [Google Scholar] [CrossRef]
- Cabrera, L.Y.; Goudreau, J.; Sidiropoulos, C. Critical appraisal of the recent US FDA approval for earlier DBS intervention. Neurology 2018, 91, 133–136. [Google Scholar] [CrossRef]
- Artusi, C.A.; Lopiano, L.; Morgante, F. Deep Brain Stimulation Selection Criteria for Parkinson’s Disease: Time to Go beyond CAPSIT-PD. J. Clin. Med. 2020, 9, 3931. [Google Scholar] [CrossRef]
- Antonini, A.; Stoessl, A.J.; Kleinman, L.S.; Skalicky, A.M.; Marshall, T.S.; Sail, K.R.; Onuk, K.; Odin, P.L.A. Developing consensus among movement disorder specialists on clinical indicators for identification and management of advanced Parkinson’s disease: A multi-country Delphi-panel approach. Curr. Med. Res. Opin. 2018, 34, 2063–2073. [Google Scholar] [CrossRef]
- Cui, Z.; Pan, L.; Song, H.; Xu, X.; Xu, B.; Yu, X.; Ling, Z. Intraoperative MRI for optimizing electrode placement for deep brain stimulation of the subthalamic nucleus in Parkinson disease. J. Neurosurg. 2016, 124, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Cui, Z.; Pan, L.; Liang, S.; Mao, Z.; Xu, X.; Yu, X.; Ling, Z. Early detection of cerebral ischemic events on intraoperative magnetic resonance imaging during surgical procedures for deep brain stimulation. Acta Neurochir. 2019, 161, 1545–1558. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Chen, T.; Wang, J.; Jiang, C.; Gao, Q.; Mao, Z.; Pan, L.; Ling, Z.; Zhang, J.; Li, X. The Long-Term Efficacy, Prognostic Factors, Safety, and Hospitalization Costs Following Denervation and Myotomy of the Affected Muscles and Deep Brain Stimulation in 94 Patients with Spasmodic Torticollis. Brain Sci. 2022, 12, 881. [Google Scholar] [CrossRef] [PubMed]
- Charles, P.D.; Van Blercom, N.; Krack, P.; Lee, S.L.; Xie, J.; Besson, G.; Benabid, A.L.; Pollak, P. Predictors of effective bilateral subthalamic nucleus stimulation for PD. Neurology 2002, 59, 932–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russmann, H.; Ghika, J.; Villemure, J.G.; Robert, B.; Bogousslavsky, J.; Burkhard, P.R.; Vingerhoets, F.J. Subthalamic nucleus deep brain stimulation in Parkinson disease patients over age 70 years. Neurology 2004, 63, 1952–1954. [Google Scholar] [CrossRef]
- Derost, P.P.; Ouchchane, L.; Morand, D.; Ulla, M.; Llorca, P.M.; Barget, M.; Debilly, B.; Lemaire, J.J.; Durif, F. Is DBS-STN appropriate to treat severe parkinson disease in an elderly population? Neurology 2007, 68, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Ory-Magne, F.; Brefel-Courbon, C.; Simonetta-Moreau, M.; Fabre, N.; Lotterie, J.A.; Chaynes, P.; Berry, I.; Lazorthes, Y.; Rascol, O. Does ageing influence deep brain stimulation outcomes in parkinson’s disease? Mov. Disord. 2007, 22, 1457–1463. [Google Scholar] [CrossRef] [PubMed]
- Parent, B.; Awan, N.; Berman, S.B.; Suski, V.; Moore, R.; Crammond, D.; Kondziolka, D. The relevance of age and disease duration for intervention with subthalamic nucleus deep brain stimulation surgery in Parkinson disease. J. Neurosurg. 2011, 114, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Wang, F.; Li, W.; Wang, N.; Han, C.; Fan, S.; Li, P.; Xu, L.; Zhang, J.; Meng, F. Relationship between electrode position of deep brain stimulation and motor symptoms of Parkinson’s disease. BMC Neurol. 2021, 21, 122. [Google Scholar] [CrossRef] [PubMed]
- Afentou, N.; Jarl, J.; Gerdtham, U.G.; Saha, S. Economic evaluation of interventions in Parkinson’s Disease: A systematic literature review. Mov. Disord. Clin. Pract. 2019, 6, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Gruber, D.; Calmbach, L.; Kühn, A.A.; Krause, P.; Kopp, U.A.; Schneider, G.H.; Kupsch, A. Longterm outcome of cognition, affective state, and quality of life following subthalamic deep brain stimulation in Parkinson’s disease. J. Neural. Transm. 2019, 126, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Zuzuárregui, J.R.P.; Ostrem, J.L. The Impact of Deep Brain Stimulation on Sleep in Parkinson’s Disease: An update. J. Park. Dis. 2020, 10, 393–404. [Google Scholar] [CrossRef] [Green Version]
- Chopra, A.; Abulseoud, O.A.; Sampson, S.; Lee, K.H.; Klassen, B.T.; Fields, J.A.; Matsumoto, J.Y.; Adams, A.C.; Stoppel, C.J.; Geske, J.R.; et al. Mood stability in Parkinson disease following deep brain stimulation: A 6-month prospective follow-up study. Psychosomatics 2014, 55, 478–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seritan, A.L.; Spiegel, L.L.; Weinstein, J.L.; Racine, C.A.; Brown, E.G.; Volz, M.; de Hemptinne, C.; Starr, P.A.; Ostrem, J.L. Elevated Mood States in Patients With Parkinson’s Disease Treated With Deep Brain Stimulation: Diagnosis and Management Strategies. J. Neuropsychiatry Clin. Neurosci. 2021, 33, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Lo Buono, V.; Lucà Trombetta, M.; Palmeri, R.; Bonanno, L.; Cartella, E.; Di Lorenzo, G.; Bramanti, P.; Marino, S.; Corallo, F. Subthalamic nucleus deep brain stimulation and impulsivity in Parkinson’s disease: A descriptive review. Acta Neurol. Belg. 2021, 121, 837–847. [Google Scholar] [CrossRef]
- Dafsari, H.S.; Reker, P.; Stalinski, L.; Silverdale, M.; Rizos, A.; Ashkan, K.; Barbe, M.T.; Fink, G.R.; Evans, J.; Steffen, J.; et al. Quality of life outcome after subthalamic stimulation in Parkinson’s disease depends on age. Mov. Disord. 2018, 33, 99–107. [Google Scholar] [CrossRef]
- Couto, M.I.; Monteiro, A.; Oliveira, A.; Lunet, N.; Massano, J. Depression and anxiety following deep brain stimulation in Parkinson’s disease: Systematic review and meta-analysis. Acta Med. Port. 2014, 27, 372–382. [Google Scholar] [CrossRef]
- Smeding, H.M.M.; Speelman, J.D.; Huizenga, H.M.; Schuurman, P.R.; Schmand, B. Predictors of cognitive and psychosocial outcome after STN DBS in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2011, 82, 754–760. [Google Scholar] [CrossRef] [Green Version]
- Odekerken, V.J.; Boel, J.A.; Geurtsen, G.J.; Schmand, B.A.; Dekker, I.P.; de Haan, R.J.; Schuurman, P.R.; de Bie, R.M. Neuropsychological outcome after deep brain stimulation for Parkinson disease. Neurology 2015, 84, 1355–1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parsons, T.D.; Rogers, S.A.; Braaten, A.J.; Woods, S.P.; Tröster, A.I. Cognitive sequelae of subthalamic nucleus deep brain stimulation in Parkinson’s disease: A meta-analysis. Lancet Neurol. 2006, 5, 578–588. [Google Scholar] [CrossRef]
- DeLong, M.; Huang, K.; Gallis, J.; Lokhnygina, Y.; Parente, B.; Hickey, P.; Turner, D.; Lad, S. Effect of advancing age on outcomes of deep brain stimulation for Parkinson disease. JAMA Neurol. 2014, 71, 1290–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakim, A.A.; Mattar, J.B.; Lambert, M.; Ponce, F.A. Perioperative complications of deep brain stimulation among patients with advanced age: A single-institution retrospective analysis. J. Neurosurg. 2021, 12, 1–8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. | Sex | Age (Y) | DOS (M) | Basic Disease and Surgical History | DBS Target | Lead Model | FU (M) | Complications |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 76 | 63 | — | B-STN | PINSL301 | 83 | — |
| 2 | F | 75 | 180 | Cholecystectomy | B-STN | PINSL301 | 52 | — |
| 3 | M | 76 | 111 | Thyroidectomy; | B-STN | PINSL301 | 36 | — |
| 4 | M | 76 | 180 | — | B-STN | Medt3389 | 30 | Hallucinations |
| 5 | F | 78 | 123 | Thyroidectomy; cholecystectomy | B-STN | PINSL301 | 36 | — |
| 6 | F | 75 | 60 | — | B-STN | PINSL301 | 30 | — |
| 7 | F | 75 | 192 | Hypertension | B-STN | PINSL301 | 30 | Left frontal hematoma |
| 8 | M | 77 | 96 | Diabetes; cholecystectomy | B-STN | PINSL301 | 33 | — |
| 9 | M | 76 | 72 | — | B-STN | PINSL301 | 21 | — |
| 10 | F | 76 | 120 | Thyroidectomy | B-STN | Medt3389 | 108 | — |
| 11 | F | 77 | 72 | Hypertension; left pallidotomy | R-Gpi | Medt3387 | 94 | Hallucinations |
| 12 | M | 75 | 60 | Hypertension; diabetes | B-STN | Medt3389 | 69 | — |
| 13 | M | 75 | 72 | Hypertension | B-STN | Medt3389 | 65 | — |
| 14 | M | 75 | 48 | Diabetes | B-STN | Medt3389 | 65 | — |
| 15 | M | 75 | 96 | Thyroidectomy | B-STN | Medt3389 | 21 | Dyskinesia |
| 16 | M | 81 | 120 | — | B-ViM | Medt3387 | 105 | — |
| 17 | M | 75 | 96 | — | L-ViM, R-STN | Medt3389 | 41 | Scalp incision delayed healing |
| 18 | M | 80 | 432 | — | B-STN | Medt3389 | 41 | — |
| 19 | M | 77 | 121 | Hypertension; cholecystectomy | B-STN | PINSL301 | 31 | — |
| 20 | F | 75 | 72 | — | B-STN | Medt3389 | 72 | Dyskinesia |
| 21 | M | 77 | 144 | — | B-STN | PINSL301 | 66 | — |
| 22 | M | 83 | 60 | Hypertension | B-Gpi | Medt3387 | 60 | — |
| 23 | M | 85 | 180 | Hypertension | B-STN | Medt3389 | 78 | — |
| 24 * | M | 76 | 62 | — | B-STN | Medt3389 | — | — |
| 25 * | M | 75 | 276 | — | B-STN | Medt3389 | — | — |
| 26 * | M | 86 | 444 | Diabetes; resection of rectal cancer | B-Gpi | Medt3387 | — | — |
| 27 * | M | 83 | 84 | — | B-STN | Medt3389 | — | — |
| Evaluation Scale | UPDRS III | PDQ-39 | ADL-Barthel |
|---|---|---|---|
| Range of score | 0–108 | 0–100 | 0–100 |
| Baseline | 35(4) | 88(17) | 25(15) |
| 1 Year | |||
| (Stimulation-on) | 19(8) * | 55(31) * | 75(30) * |
| Z/t | 19.230 | 11.390 | −4.205 |
| p | <0.001 | <0.001 | <0.001 |
| (Stimulation-off) | 39(10) | 85(13) | 15(15) |
| Z/t | 3.456 | −1.287 | −3.225 |
| p | 0.002 | 0.198 | 0.01 |
| last FU | |||
| (Stimulation-on) | 32(2) * | 81(34) * | 35(10) * |
| Z/t | −4.030 | 2.142 | −4.034 |
| p | <0.001 | 0.044 | <0.001 |
| (Stimulation-off) | 45(4) | 99(39) | 15(5) |
| Z/t | −4.207 | −2.801 | −3.959 |
| p | <0.001 | 0.005 | <0.001 |
| Evaluation Scale | Sleep | Cognition | Emotion | LEDD (mg) | ||||
|---|---|---|---|---|---|---|---|---|
| PDSS-CV | PSQI | ESS | MMSE | MoCA | HAMD | HAMA | LEDD | |
| Range of score | 0–150 | 0–42 | 0–24 | 0–30 | 0–30 | 0–76 | 0–56 | |
| Baseline | 105(17) | 26.43 ± 5.91 | 16(5) | 28(2) | 27(1) | 15(4) | 15.91 ± 4.47 | 650(573) |
| 1 Year | 106(18) * | 26.04 ± 6.56 | 14(4) * | 28(1) | 28(0) * | 10(2) * | 12.43 ± 4.17 * | 280(150) * |
| Z/t | 3.669 | 0.883 | 8.398 | 2.07 | 3.153 | 4.216 | 8.654 | 4.094 |
| P | <0.001 | 0.387 | <0.001 | 0.038 | 0.002 | <0.001 | <0.001 | <0.001 |
| last FU | 99(20) * | 23.74 ± 7.58 * | 19(6) * | 28(1) | 27(1) * | 14(5) | 17.13 ± 6.45 | 325(300) * |
| Z/t | 3.072 | 4.389 | 19.23 | 0.144 | 2.646 | 0.884 | 1.494 | 3.926 |
| p | 0.002 | <0.001 | <0.001 | 0.885 | 0.008 | 0.377 | 0.149 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, C.; Wang, J.; Chen, T.; Li, X.; Cui, Z. Short- and Long-Term Efficacy and Safety of Deep-Brain Stimulation in Parkinson’s Disease Patients aged 75 Years and Older. Brain Sci. 2022, 12, 1588. https://doi.org/10.3390/brainsci12111588
Jiang C, Wang J, Chen T, Li X, Cui Z. Short- and Long-Term Efficacy and Safety of Deep-Brain Stimulation in Parkinson’s Disease Patients aged 75 Years and Older. Brain Sciences. 2022; 12(11):1588. https://doi.org/10.3390/brainsci12111588
Chicago/Turabian StyleJiang, Chao, Jian Wang, Tong Chen, Xuemei Li, and Zhiqiang Cui. 2022. "Short- and Long-Term Efficacy and Safety of Deep-Brain Stimulation in Parkinson’s Disease Patients aged 75 Years and Older" Brain Sciences 12, no. 11: 1588. https://doi.org/10.3390/brainsci12111588