Trait-Related Impulsivity, Affective Temperaments and Mood Disorders: Results from a Real-World Multicentric Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Procedures and Measures
2.1.1. Socio-Demographics Characteristics
2.1.2. Psychopathological Assessments
2.1.3. Statistical Analyses
3. Results
3.1. Main Socio-Demographic and Clinical Characteristics of the Total Sample
3.2. Differences among Patients with and without Impulsivity
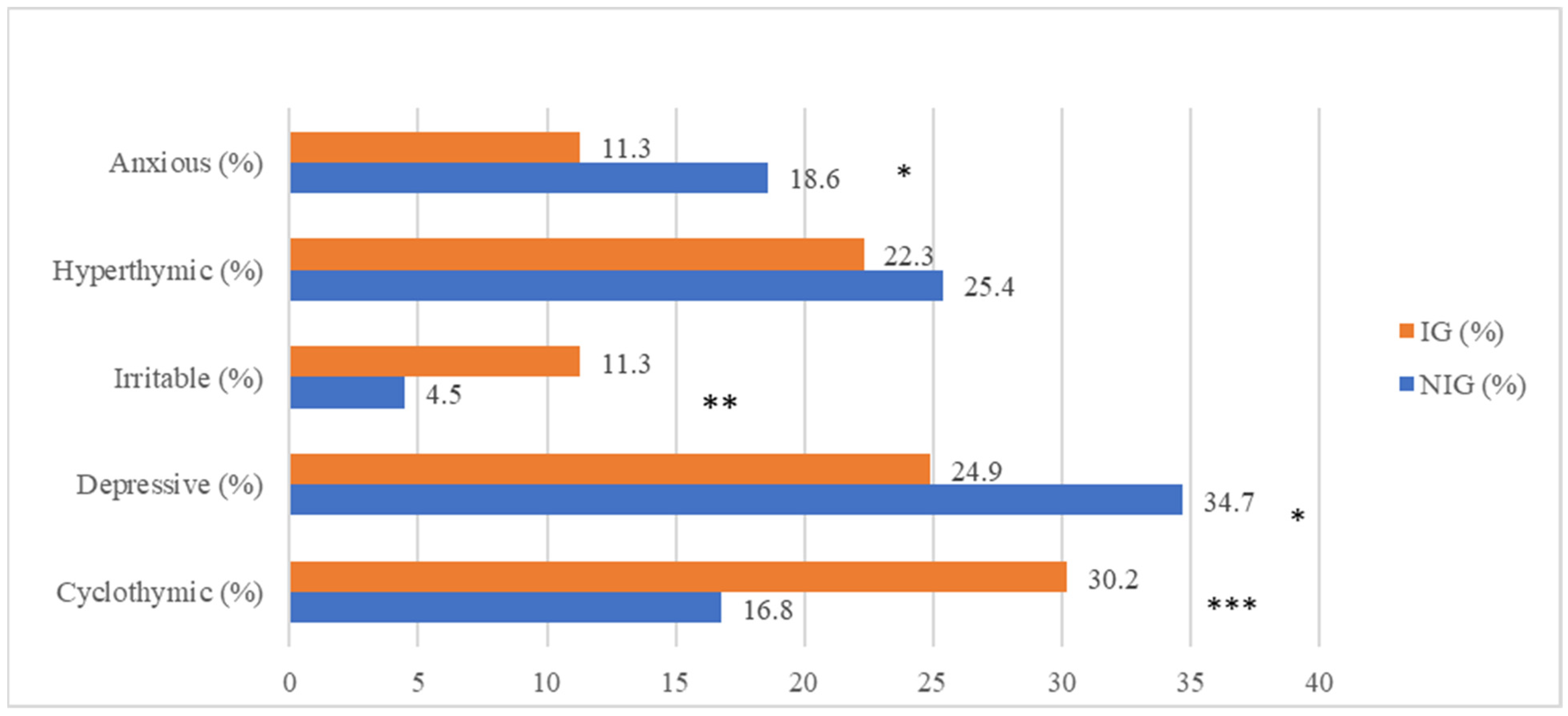
3.3. Impulsivity and Affective Temperaments
3.4. Logistic Regression Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moeller, F.G.; Barratt, E.S.; Dougherty, D.M.; Schmitz, J.M.; Swann, A.C. Psychiatric aspects of impulsivity. Am. J. Psychiatry 2001, 158, 1783–1793. [Google Scholar] [CrossRef] [PubMed]
- Turek, A.; Machalska, K.; Chrobak, A.A.; Siwek, M.; Dudek, D. Impulsiveness and cyclothymic traits of affective temperament as predictors of risky gambling behavior. Psychiatr. Pol. 2020, 54, 537–552. [Google Scholar] [CrossRef] [PubMed]
- Edmiston, E.K.; Fournier, J.C.; Chase, H.W.; Bertocci, M.A.; Greenberg, T.; Aslam, H.A.; Lockovich, J.; Graur, S.; Bebko, G.; Forbes, E.E.; et al. Assessing Relationships Among Impulsive Sensation Seeking, Reward Circuitry Activity, and Risk for Psychopathology: A Functional Magnetic Resonance Imaging Replication and Extension Study. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2020, 5, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Correll, C.U.; Arango, C.; Berk, M.; Patel, V.; Ioannidis, J.P.A. Preventive psychiatry: A blueprint for improving the mental health of young people. World Psychiatry 2021, 20, 200–221. [Google Scholar] [CrossRef]
- American Psychiatric Association. Structured Clinical Interview for DSM-5 (SCID-5); American Psychiatric Association Publishing: Washington, DC, USA, 2013. [Google Scholar]
- First, M.B.; Gaebel, W.; Maj, M.; Stein, D.J.; Kogan, C.S.; Saunders, J.B.; Poznyak, V.B.; Gureje, O.; Lewis-Fernández, R.; Maercker, A.; et al. An organization- and category-level comparison of diagnostic requirements for mental disorders in ICD-11 and DSM-5. World Psychiatry 2021, 20, 34–51. [Google Scholar] [CrossRef]
- Henna, E.; Hatch, J.P.; Nicoletti, M.; Swann, A.C.; Zunta-Soares, G.; Soares, J.C. Is impulsivity a common trait in bipolar and unipolar disorders? Bipolar Disord. 2013, 15, 223–227. [Google Scholar] [CrossRef] [Green Version]
- Feki, I.; Moalla, M.; Baati, I.; Trigui, D.; Sellami, R.; Masmoudi, J. Impulsivity in bipolar disorders in a Tunisian sample. Asian J. Psychiatry 2016, 22, 77–80. [Google Scholar] [CrossRef]
- Newman, A.L.; Meyer, T.D. Impulsivity: Present during euthymia in bipolar disorder?—A systematic review. Int. J. Bipolar Disord. 2014, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Ramírez-Martín, A.; Ramos-Martín, J.; Mayoral-Cleries, F.; Moreno-Küstner, B.; Guzman-Parra, J. Impulsivity, decision-making and risk-taking behaviour in bipolar disorder: A systematic review and meta-analysis. Psychol. Med. 2020, 50, 2141–2153. [Google Scholar] [CrossRef]
- Dervic, K.; Garcia-Amador, M.; Sudol, K.; Freed, P.; Brent, D.A.; Mann, J.J.; Harkavy-Friedman, J.M.; Oquendo, M.A. Bipolar I and II versus unipolar depression: Clinical differences and impulsivity/aggression traits. Eur. Psychiatry 2015, 30, 106–113. [Google Scholar] [CrossRef]
- Swann, A.C.; Dougherty, D.M.; Pazzaglia, P.J.; Pham, M.; Steinberg, J.L.; Moeller, F.G. Increased impulsivity associated with severity of suicide attempt history in patients with bipolar disorder. Am. J. Psychiatry 2005, 162, 1680–1687. [Google Scholar] [CrossRef] [PubMed]
- Ozten, M.; Erol, A.; Karayilan, S.; Kapudan, H.; Orsel, E.S.; Kumsar, N.A. Impulsivity in bipolar and substance use disorders. Compr. Psychiatry 2015, 59, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Nery, F.G.; Hatch, J.P.; Monkul, E.S.; Matsuo, K.; Zunta-Soare, G.B.; Bowden, C.L.; Soares, J.C. Trait impulsivity is increased in bipolar disorder patients with comorbid alcohol use disorders. Psychopathology 2013, 46, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Shakeel, M.K.; Hodgins, D.C.; Goghari, V.M. A Comparison of Self-Reported Impulsivity in Gambling Disorder and Bipolar Disorder. J. Gambl. Stud. 2019, 35, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Oquendo, M.A.; Lizardi, D.; Greenwald, S.; Weissman, M.M.; Mann, J.J. Rates of lifetime suicide attempt and rates of lifetime major depression in different ethnic groups in the United States. Acta Psychiatr. Scand. 2004, 110, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, D.; Iosue, M.; Wuestefeld, A.; Carli, V. Adaptation of evidence-based suicide prevention strategies during and after the COVID-19 pandemic. World Psychiatry 2020, 19, 294–306. [Google Scholar] [CrossRef]
- Rote, J.; Dingelstadt, A.M.; Aigner, A.; Bauer, M.; Fiebig, J.; König, B. Impulsivity predicts illness severity in long-term course of bipolar disorder: A prospective approach. Aust. N. Z. J. Psychiatry 2018, 52, 876–886. [Google Scholar] [CrossRef]
- Kim, E.Y.; Hwang, S.S.; Lee, N.Y.; Kim, S.H.; Lee, H.J.; Kim, Y.S.; Ahn, Y.M. Intelligence, temperament, and personality are related to over- or under-reporting of affective symptoms by patients with euthymic mood disorder. J. Affect. Disord. 2013, 148, 235–242. [Google Scholar] [CrossRef]
- Victor, S.E.; Johnson, S.L.; Gotlib, I.H. Quality of life and impulsivity in bipolar disorder. Bipolar Disord. 2011, 13, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Taipale, H.; Tanskanen, A.; Mehtälä, J.; Vattulainen, P.; Correll, C.U.; Tiihonen, J. 20-year follow-up study of physical morbidity and mortality in relationship to antipsychotic treatment in a nationwide cohort of 62,250 patients with schizophrenia (FIN20). World Psychiatry 2020, 19, 61–68. [Google Scholar] [CrossRef]
- Plana-Ripoll, O.; Musliner, K.L.; Dalsgaard, S.; Momen, N.C.; Weye, N.; Christensen, M.K.; Agerbo, E.; Iburg, K.M.; Laursen, T.M.; Mortensen, P.B.; et al. Nature and prevalence of combinations of mental disorders and their association with excess mortality in a population-based cohort study. World Psychiatry 2020, 19, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Patapoff, M.; Ramsey, M.; Titone, M.; Kaufmann, C.N.; Malhotra, A.; Ancoli-Israel, S.; Wing, D.; Lee, E.; Eyler, L.T. Temporal relationships of ecological momentary mood and actigraphy-based sleep measures in bipolar disorder. J. Psychiatr. Res. 2022, 150, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Belzeaux, R.; Boyer, L.; Mazzola-Pomietto, P.; Michel, P.; Correard, N.; Aubin, V.; Bellivier, F.; Bougerol, T.; Olie, E.; Courtet, P.; et al. Adherence to medication is associated with non-planning impulsivity in euthymic bipolar disorder patients. J. Affect. Disord. 2015, 184, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Akiskal, H.S.; Mallya, G. Criteria for the “soft” bipolar spectrum: Treatment implications. Psychopharmacol. Bull. 1987, 23, 68–73. [Google Scholar] [PubMed]
- Akiskal, H.S.; Pinto, O. The evolving bipolar spectrum. Prototypes, I, II, III, and IV. Psychiatr. Clin. N. Am. 1999, 22, 517–534. [Google Scholar] [CrossRef]
- Akiskal, H.S. Validating “hard” and “soft” phenotypes within the bipolar spectrum: Continuity or discontinuity? J. Affect. Disord. 2003, 73, 1–5. [Google Scholar] [CrossRef]
- Benazzi, F.; Akiskal, H.S. How best to identify a bipolar-related subtype among major depressive patients without spontaneous hypomania: Superiority of age at onset criterion over recurrence and polarity? J. Affect. Disord. 2008, 107, 77–88. [Google Scholar] [CrossRef]
- Kraepelin, E. Manic-Depressive Insanity and Paranoia; Churchill Livingstone: Edinburgh, UK, 1921. [Google Scholar]
- Heckers, S.; Kendler, K.S. The evolution of Kraepelin’s nosological principles. World Psychiatry 2020, 19, 381–388. [Google Scholar] [CrossRef]
- Akiskal, H.S.; Akiskal, K.K. Cyclothymic, hyperthymic, and depressive temperaments as subaffective variants of mood disorders. Am. Psychiatr. Press Rev. Psychiatry 1992, 11, 43–62. [Google Scholar]
- Akiskal, H.S.; Placidi, G.F.; Maremmani, I.; Signoretta, S.; Liguori, A.; Gervasi, R.; Mallya, G.; Puzantian, V.R. TEMPS-I: Delineating the most discriminant traits of the cyclothymic, depressive, hyperthymic and irritable temperaments in a nonpatient population. J. Affect. Disord. 1998, 51, 7–19. [Google Scholar] [CrossRef]
- Dolenc, B.; Dernovšek, M.Z.; Sprah, L.; Tavcar, R.; Perugi, G.; Akiskal, H.S. Relationship between affective temperaments and aggression in euthymic patients with bipolar mood disorder and major depressive disorder. J. Affect. Disord. 2015, 174, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Kesebir, S.; Işitmez, S.; Gündoğar, D. Compulsive buying in bipolar disorder: Is it a comorbidity or a complication? J. Affect. Disord. 2012, 136, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, E.; Arias, B.; Mitjans, M.; Goikolea, J.M.; Ruíz, V.; Brat, M.; Sáiz, P.A.; García-Portilla, M.P.; Burón, P.; Bobes, J.; et al. Clinical features, impulsivity, temperament and functioning and their role in suicidality in patients with bipolar disorder. Acta Psychiatr. Scand. 2016, 133, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Luciano, M.; Steardo, L., Jr.; Sampogna, G.; Caivano, V.; Ciampi, C.; Del Vecchio, V.; Di Cerbo, A.; Giallonardo, V.; Zinno, F.; De Fazio, P.; et al. Affective Temperaments and Illness Severity in Patients with Bipolar Disorder. Medicina 2021, 57, 54. [Google Scholar] [CrossRef]
- Özsoy, F.; Taşcı, G.; Atmaca, M. Investigating the Association of Criminal Behavior with Childhood Traumas, Impulsivity, and Dominant Temperaments in Bipolar I Disorder. Prim. Care Companion CNS Disord. 2022, 24, 21m03103. [Google Scholar] [CrossRef]
- Maremmani, I.; Perugi, G.; Pacini, M.; Akiskal, H.S. Toward a unitary perspective on the bipolar spectrum and substance abuse: Opiate addiction as a paradigm. J. Affect. Disord. 2006, 93, 1–12. [Google Scholar] [CrossRef]
- Beşirli, A. The relationship between impulsivity and panic disorder-agoraphobia: The role of affective temperament. Psychiatry Res. 2018, 264, 169–174. [Google Scholar] [CrossRef]
- Scumaci, E.; Marzola, E.; Abbate-Daga, G.; Pellegrini, M.; Ponzo, V.; Goitre, I.; Benso, A.; Broglio, F.; Belcastro, S.; Crespi, C.; et al. Affective temperaments and obesity: Is there an association with binge eating episodes and multiple weight cycling? J. Affect. Disord. 2021, 295, 967–973. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Bipolar Disorder: Assessment and Management. 2020. Available online: https://www.nice.org.uk/guidance/cg185 (accessed on 25 October 2022).
- National Institute for Health and Care Excellence (NICE). Depression in Adults. 2011. Available online: https://www.nice.org.uk/guidance/qs8/history (accessed on 25 October 2022).
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Young, R.C.; Biggs, J.T.; Ziegler, V.E.; Meyer, D.A. A rating scale for mania: Reliability, validity and sensitivity. Br. J. Psychiatry 1978, 133, 429–435. [Google Scholar] [CrossRef]
- Fossati, A.; Di Ceglie, A.; Acquarini, E.; Barratt, E.S. Psychometric properties of an Italian version of the Barratt Impulsiveness Scale-11 (BIS-11) in nonclinical subjects. J. Clin. Psychol 2001, 57, 815–828. [Google Scholar] [CrossRef] [PubMed]
- Stanford, M.S.; Mathias, C.W.; Dougherty, D.M.; Lake, S.L.; Anderson, N.E.; Patton, J.H. Fifty years of the Barratt Impulsiveness Scale: An update and review. Personal. Individ. Differ. 2009, 47, 385–395. [Google Scholar] [CrossRef]
- Fico, G.; Luciano, M.; Sampogna, G.; Zinno, F.; Steardo, L., Jr.; Perugi, G.; Pompili, M.; Tortorella, A.; Volpe, U.; Fiorillo, A.; et al. Validation of the brief TEMPS-M temperament questionnaire in a clinical Italian sample of bipolar and cyclothymic patients. J. Affect. Disord. 2020, 260, 458–462. [Google Scholar] [CrossRef]
- Sterne, J.A.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef] [PubMed]
- Musil, C.M.; Warner, C.B.; Yobas, P.K.; Jones, S.L. A comparison of imputation techniques for handling missing data. West. J. Nurs. Res. 2002, 24, 815–829. [Google Scholar] [CrossRef]
- Dawson, E.L.; Shear, P.K.; Howe, S.R.; Adler, C.M.; DelBello, M.P.; Fleck, D.E.; Strakowski, S.M. Impulsivity predicts time to reach euthymia in adults with bipolar disorder. Bipolar Disord. 2014, 16, 846–856. [Google Scholar] [CrossRef]
- Etain, B.; Mathieu, F.; Liquet, S.; Raust, A.; Cochet, B.; Richard, J.R.; Gard, S.; Zanouy, L.; Kahn, J.P.; Cohen, R.F.; et al. Clinical features associated with trait-impulsiveness in euthymic bipolar disorder patients. J. Affect. Disord. 2013, 144, 240–247. [Google Scholar] [CrossRef]
- Di Nicola, M.; Tedeschi, D.; Mazza, M.; Martinotti, G.; Harnic, D.; Catalano, V.; Bruschi, A.; Pozzi, G.; Bria, P.; Janiri, L. Behavioural addictions in bipolar disorder patients: Role of impulsivity and personality dimensions. J. Affect. Disord 2010, 125, 82–88. [Google Scholar] [CrossRef]
- Squeglia, L.M. Alcohol and the developing adolescent brain. World Psychiatry 2020, 19, 393–394. [Google Scholar] [CrossRef]
- McIntyre, R.S.; Lee, Y. Preventing suicide in the context of the COVID-19 pandemic. World Psychiatry 2020, 19, 250–251. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, X.; Yang, G.; Feng, Z. Impulsiveness indirectly affects suicidal ideation through depression and simultaneously moderates the indirect effect: A moderated mediation path model. Front. Psychiatry 2022, 27, 913680. [Google Scholar] [CrossRef]
- Miller, A.H. Beyond depression: The expanding role of inflammation in psychiatric disorders. World Psychiatry 2020, 19, 108–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldman, I.D.; Poore, H.E.; Luningham, J.M.; Yang, J. Testing structural models of psychopathology at the genomic level. World Psychiatry 2020, 19, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Roige, S.; Fontanillas, P.; Elson, S.L.; Gray, J.C.; de Wit, H.; MacKillop, J.; Palmer, A.A. Genome-Wide Association Studies of Impulsive Personality Traits (BIS-11 and UPPS-P) and Drug Experimentation in up to 22,861 Adult Research Participants Identify Loci in the CACNA1I and CADM2 genes. J. Neurosci. 2019, 39, 2562–2572. [Google Scholar]
- Arango, C.; Dragioti, E.; Solmi, M.; Cortese, S.; Domschke, K.; Murray, R.M.; Jones, P.B.; Uher, R.; Carvalho, A.F.; Reichenberg, A.; et al. Risk and protective factors for mental disorders beyond genetics: An evidence-based atlas. World Psychiatry 2021, 20, 417–436. [Google Scholar] [CrossRef]
- Leyton, M.; Okazawa, H.; Diksic, M.; Paris, J.; Rosa, P.; Mzengeza, S.; Young, S.N.; Blier, P.; Benkelfat, C. Brain Regional alpha-[11C]methyl-L-tryptophan trapping in impulsive subjects with borderline personality disorder. Am. J. Psychiatry 2001, 158, 775–782. [Google Scholar] [CrossRef]
- Klonsky, E.D.; Dixon-Luinenburg, T.; May, A.M. The critical distinction between suicidal ideation and suicide attempts. World Psychiatry 2021, 20, 439–441. [Google Scholar] [CrossRef]
- Peluso, M.A.M.; Hatch, J.P.; Glahn, D.C.; Monkul, E.S.; Sanches, M.; Najt, P.; Bowden, C.L.; Barratt, E.S.; Soares, J.C. Trait impulsivity in patients with mood disorders. J. Affect. Disord. 2007, 100, 227–231. [Google Scholar] [CrossRef]
- Krueger, R.F.; Hobbs, K.A.; Conway, C.C.; Dick, D.M.; Dretsch, M.N.; Eaton, N.R. Validity and utility of Hierarchical Taxonomy of Psychopathology (HiTOP): II. Externalizing superspectrum. World Psychiatry 2021, 20, 171–193. [Google Scholar] [CrossRef]
- Hasler, G. Understanding mood in mental disorders. World Psychiatry 2020, 19, 56–57. [Google Scholar] [CrossRef]
- Maj, M.; Stein, D.J.; Parker, G.; Zimmerman, M.; Fava, G.A.; De Hert, M.; Demyttenaere, K.; McIntyre, R.S.; Widiger, T.; Wittchen, H.U. The clinical characterization of the adult patient with depression aimed at personalization of management. World Psychiatry 2020, 19, 269–293. [Google Scholar] [CrossRef]
- Reynolds, C.F. Optimizing personalized management of depression: The importance of real-world contexts and the need for a new convergence paradigm in mental health. World Psychiatry 2020, 19, 266–268. [Google Scholar] [CrossRef]
- Stein, D.J.; Craske, M.G.; Rothbaum, B.O.; Chamberlain, S.R.; Fineberg, N.A.; Choi, K.W.; de Jonge, P.; Baldwin, D.S.; Maj, M. The clinical characterization of the adult patient with an anxiety or related disorder aimed at personalization of management. World Psychiatry 2021, 20, 336–356. [Google Scholar] [CrossRef]
- Kim, H.; Turiano, N.A.; Forbes, M.K.; Kotov, R.; Krueger, R.F.; Eaton, N.R. HiTOP Utility Workgroup. Internalizing psychopathology and all-cause mortality: A comparison of transdiagnostic vs. diagnosis-based risk prediction. World Psychiatry 2021, 20, 276–282. [Google Scholar] [CrossRef]
- Shah, J.L.; Scott, J.; McGorry, P.D.; Cross, S.P.M.; Keshavan, M.S.; Nelson, B.; Wood, S.J. Transdiagnostic clinical staging in youth mental health: A first international consensus statement. World Psychiatry 2020, 19, 233–242. [Google Scholar] [CrossRef]
- Barlow, D.H.; Harris, B.A.; Eustis, E.H.; Farchione, T.J. The unified protocol for transdiagnostic treatment of emotional disorders. World Psychiatry 2020, 19, 245–246. [Google Scholar] [CrossRef]
- Perugi, G.; Akiskal, H.S. The soft bipolar spectrum redefined: Focus on the cyclothymic, anxious-sensitive, impulse-dyscontrol, and binge-eating connection in bipolar II and related conditions. Psychiatr. Clin. N. Am. 2002, 25, 713–737. [Google Scholar] [CrossRef]
- Barbuti, M.; Carignani, G.; Weiss, F.; Calderone, A.; Santini, F.; Perugi, G. Mood disorders comorbidity in obese bariatric patients: The role of the emotional dysregulation. J. Affect. Disord. 2021, 279, 46–52. [Google Scholar] [CrossRef]
- Quaranta, G.; Barbuti, M.; Pallucchini, A.; Colombini, P.; Moriconi, M.; Gemmellaro, T.; Tripodi, B.; Palagini, L.; Schiavi, E.; Perugi, G. Relationships among Delayed Sleep Phase Disorder, Emotional Dysregulation, and Affective Temperaments in Adults with Attention Deficit Hyperactivity Disorder and Cyclothymia. J. Nerv. Ment. Dis. 2020, 208, 857–862. [Google Scholar] [CrossRef]
- Royston, P.; Altman, D.G.; Sauerbrei, W. Dichotomizing continuous predictors in multiple regression: A bad idea. Stat. Med. 2006, 25, 127–141. [Google Scholar] [CrossRef]


{kind=link}
| Total Sample (n = 653) | |
|---|---|
| Age (M ± DS) | 46.9 ± 14.1 |
| Gender, M, % (n) | 41.8 (275) |
| Living situation, with partner yes % (n) | 39 (256) |
| Years of education (M ± DS) | 13.3 ± 3.6 |
| Employed, yes, % (n) | 54.7 (360) |
| Age at onset (M ± DS) | 31.3 ± 13.1 |
| Diagnosis, % (n) | |
| Bipolar disorder | 55.7 (364) |
| Major depression | 35.8 (234) |
| Cyclothymic disorder | 8.4 (55) |
| Number of affective episodes (M ± DS) | 4.5 ± 5.0 |
| Number of hospitalizations (M ± DS) | 2.4 ± 2.5 |
| Number of involuntary hospitalizations (M ± DS) | 1.5 ± 0.9 |
| Suicide attempts, yes, % (n) | 17.9 (118) |
| Seasonality, yes, % (n) | 32.5 (212) |
| Presence of psychotic symptoms during acute phases, yes, % (n) | 29.5 (195) |
| Trait-related impulsivity (BIS-11 total score ≥ 72), yes, % (n) | 54.4 (356) |
| Prevalent impulsivity dimensions, % (n) | |
| Motor | 36.0 (128) |
| Non-planning | 12.1 (43) |
| Attentional impulsiveness | 52.0 (185) |
| NIG (n = 298) | IG (n = 356) | |
|---|---|---|
| Age (M ± DS) | 48.9 ± 14.1 | 45.2 ± 13.7 |
| Gender, M, % (n) | 38.9 (116) | 43.8 (156) |
| Living situation, with partner yes % (n) | 45.3 (135) | 33.4 (119) |
| Years of education (M ± DS) | 13.3 ± 3.7 | 13.3 ± 3.5 |
| Employed, yes, % (n) | 55.4 (165) | 54.2 (193) |
| Age at onset (M ± DS) | 33.5 ± 13.8 | 29.4 ± 12.1 *** |
| Diagnosis, % (n) | ||
| Bipolar disorder | 37.6 (137) | 62.4 (227) *** |
| Major depression | 56.4 (132) | 43.6 (102) * |
| Cyclothymic disorder | 50.9 (28) | 49.1 (27) |
| Number of affective episodes (M ± DS) | 3.9 ± 4.3 | 5.1 ± 5.5 *** |
| Number of hospitalizations (M ± DS) | 2.1 ± 1.6 | 2.5 ± 2.9 |
| Number of involuntary hospitalizations (M ± DS) | 1.2 ± 0.5 | 1.6 ± 1.1 * |
| Suicide attempts, yes, % (n) | 6.7 (20) | 27.5 (98) *** |
| Seasonality, yes, % (n) | 26.2 (78) | 37.6 (134) ** |
| Presence of psychotic symptoms during acute phases, yes, % (n) | 20.8 (62) | 37.1 (132) *** |
| BIS-11 Total Score ≥ 72 | Motor Impulsiveness | Attentional Impulsiveness | Non-Planning Impulsiveness | |
|---|---|---|---|---|
| Cyclothymic temperament | 0.156 *** | 0.036 | −0.017 | −0.022 |
| Depressive temperament | −0.108 * | −0.156 * | −0.026 | 0.164 ** |
| Irritable temperament | 0.124 * | 0.059 | 0.029 | −0.075 |
| Hyperthymic temperament | −0.036 | 0.051 | 0.026 | −0.065 |
| Anxious temperament | −0.102 * | 0.037 | −0.004 | −0.032 |
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||
| Age at onset | 0.98 * | 0.97 | 0.99 | 0.98 * | 0.97 | 0.99 |
| Diagnosis of bipolar disorder | 1.16 ** | 0.62 | 2.18 | 1.21 | 0.63 | 2.33 |
| Diagnosis of major depression | 0.80 * | 0.43 | 1.50 | 1.04 | 0.54 | 1.99 |
| Diagnosis of Cyclothymic disorder | 0.91 | 0.49 | 1.03 | 0.89 | 0.59 | 1.31 |
| Number of affective episodes | 1.00 | 0.96 | 1.04 | 1.00 | 0.96 | 1.04 |
| Number of involuntary hospitalizations | 1.25 | 0.88 | 1.78 | 1.32 | 0.92 | 1.89 |
| Suicide attempts | 4.21 *** | 2.56 | 6.92 | 3.99 **** | 2.41 | 6.63 |
| Seasonality | 1.44 * | 0.99 | 2.09 | 1.43 * | 0.98 | 2.09 |
| Psychotic symptoms during affective episodes | 1.56 * | 1.03 | 2.35 | 1.57 * | 1.03 | 2.41 |
| Cyclothymic temperament | - | - | - | 2.12 ** | 1.29 | 3.49 |
| Depressive temperament, no | - | - | - | 0.87 | 0.53 | 1.40 |
| Irritable Temperament, no | - | - | - | 3.11 ** | 1.48 | 6.52 |
| Anxious Temperament, no | - | - | - | 0.84 | 0.47 | 1.48 |
| Motor Impulsiveness | Attentional Impulsiveness | Non-planning Impulsiveness | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |||||||||||||
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |||||||
| Lower Bound | Upper Bound | Lower Bound | Upper Bound | Lower Bound | Upper Bound | Lower Bound | Upper Bound | Lower Bound | Upper Bound | Lower Bound | Upper Bound | |||||||
| Age at onset | 1.01 | 0.99 | 1.03 | 1.01 | 0.99 | 1.02 | 0.99 | 0.97 | 1.02 | 0.99 | 0.96 | 1.01 | 0.99 | 0.965 | 1.01 | 0.99 | 0.96 | 1.01 |
| Diagnosis of bipolar disorder | 0.55 | 0.24 | 1.25 | 0.52 | 0.22 | 1.24 | 3.42 | 0.43 | 26.89 | 3.16 | 0.39 | 25.08 | 3.42 | 0.435 | 26.89 | 3.16 | 0.39 | 25.08 |
| Diagnosis of major depression | 0.32 * | 0.13 | 0.76 | 0.36 * | 0.15 | 0.89 | 5.33 | 0.68 | 41.82 | 5.41 | 0.68 | 42.99 | 5.33 | 0.678 | 41.82 | 5.41 | 0.68 | 42.99 |
| Number of affective episodes | 1.07 * | 1.02 | 1.13 | 1.07 * | 1.02 | 1.13 | 0.97 | 0.89 | 1.06 | 0.97 | 0.89 | 1.06 | 0.98 | 0.892 | 1.06 | 0.97 | 0.89 | 1.06 |
| Number of involuntary hospitalizations | 1.06 | 0.74 | 1.52 | 1.08 | 0.75 | 1.54 | 0.89 | 0.52 | 1.55 | 0.89 | 0.51 | 1.56 | 0.89 | 0.516 | 1.55 | 0.89 | 0.51 | 1.56 |
| Suicide attempts | 0.60 | 0.35 | 1.03 | 0.67 | 0.38 | 1.15 | 0.51 | 0.23 | 1.14 | 0.52 | 0.23 | 1.17 | 0.51 | 0.226 | 1.13 | 0.52 | 0.23 | 1.17 |
| Seasonality | 1.56 | 0.96 | 2.54 | 1.59 | 0.97 | 2.62 | 1.24 | 0.61 | 2.49 | 1.23 | 0.61 | 2.49 | 1.23 | 0.615 | 2.49 | 1.23 | 0.61 | 2.49 |
| Psychotic symptoms during affective episodes | 0.70 | 0.41 | 1.17 | 0.72 | 0.42 | 1.23 | 1.41 | 0.69 | 2.88 | 1.46 | 0.71 | 3.00 | 1.41 | 0.694 | 2.87 | 1.46 | 0.71 | 3.00 |
| Cyclothymic temperament | - | - | - | 0.99 | 0.45 | 2.21 | - | - | - | 1.03 | 0.33 | 3.18 | - | - | - | 1.03 | 0.33 | 3.18 |
| Depressive temperament | - | - | - | 0.47 | 0.19 | 1.12 | - | - | - | 0.89 | 0.28 | 2.87 | - | - | - | 0.89 | 0.28 | 2.87 |
| Irritable Temperament | - | - | - | 1.15 | 0.45 | 2.89 | - | - | - | 1.51 | 0.42 | 5.45 | - | - | - | 1.51 | 0.42 | 5.45 |
| Anxious Temperament | - | - | - | 1.15 | 0.50 | 2.62 | - | - | - | 1.17 | 0.37 | 3.72 | - | - | - | 1.17 | 0.37 | 3.72 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luciano, M.; Sampogna, G.; Mancuso, E.; Simonetti, A.; De Fazio, P.; Di Nicola, M.; Di Lorenzo, G.; Pepe, M.; Sambataro, F.; Signorelli, M.S.; et al. Trait-Related Impulsivity, Affective Temperaments and Mood Disorders: Results from a Real-World Multicentric Study. Brain Sci. 2022, 12, 1554. https://doi.org/10.3390/brainsci12111554
Luciano M, Sampogna G, Mancuso E, Simonetti A, De Fazio P, Di Nicola M, Di Lorenzo G, Pepe M, Sambataro F, Signorelli MS, et al. Trait-Related Impulsivity, Affective Temperaments and Mood Disorders: Results from a Real-World Multicentric Study. Brain Sciences. 2022; 12(11):1554. https://doi.org/10.3390/brainsci12111554
Chicago/Turabian StyleLuciano, Mario, Gaia Sampogna, Emiliana Mancuso, Alessio Simonetti, Pasquale De Fazio, Marco Di Nicola, Giorgio Di Lorenzo, Maria Pepe, Fabio Sambataro, Maria Salvina Signorelli, and et al. 2022. "Trait-Related Impulsivity, Affective Temperaments and Mood Disorders: Results from a Real-World Multicentric Study" Brain Sciences 12, no. 11: 1554. https://doi.org/10.3390/brainsci12111554