

Risk Factors for Hiccups after Deep Brain Stimulation of Subthalamic Nucleus for Parkinson’s Disease
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
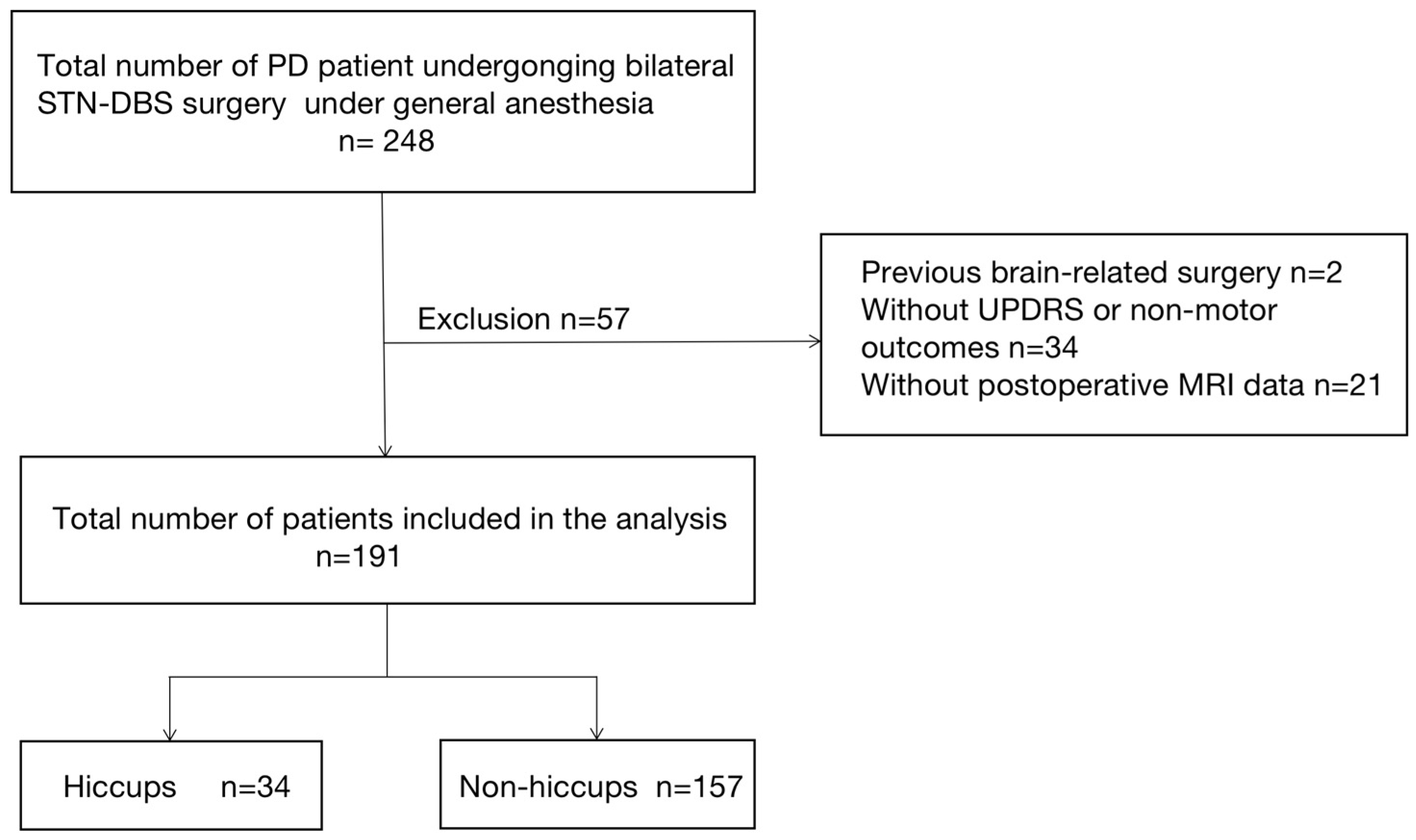
2.1. Subjects
2.2. Surgical Procedure
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Characteristics of Hiccups
3.3. Univariate and Multivariate Analysis Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steger, M.; Schneemann, M.; Fox, M. Systemic review: The pathogenesis and pharmacological treatment of hiccups. Aliment. Pharmacol. Ther. 2015, 42, 1037–1050. [Google Scholar] [CrossRef] [PubMed]
- Arsanious, D.; Khoury, S.; Martinez, E.; Nawras, A.; Filatoff, G.; Ajabnoor, H.; Darr, U.; Atallah, J. Ultrasound-Guided Phrenic Nerve Block for Intractable Hiccups following Placement of Esophageal Stent for Esophageal Squamous Cell Carcinoma. Pain Physician 2016, 19, E653–E656. [Google Scholar] [CrossRef] [PubMed]
- Becker, D.E. Nausea, vomiting, and hiccups: A review of mechanisms and treatment. Anesth. Prog. 2010, 57, 150–157. [Google Scholar] [CrossRef]
- Kumar, A. Gag reflex for arrest of hiccups. Med. Hypotheses 2005, 65, 1206. [Google Scholar] [CrossRef]
- Kolodzik, P.W.; Eilers, M.A. Hiccups (singultus): Review and approach to management. Ann. Emerg. Med. 1991, 20, 565–573. [Google Scholar] [CrossRef]
- Younce, J.R.; Campbell, M.C.; Hershey, T.; Tanenbaum, A.B.; Milchenko, M.; Ushe, M.; Karimi, M.; Tabbal, S.D.; Kim, A.E.; Snyder, A.Z.; et al. Resting-State Functional Connectivity Predicts STN DBS Clinical Response. Mov. Disord. 2021, 36, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Jochim, A.; Castrop, F.; Gempt, J.; Haslinger, B. Periodic hiccup in patients with subthalamic deep brain stimulation for Parkinson′s disease. Parkinsonism Relat. Disord. 2015, 21, 1117–1118. [Google Scholar] [CrossRef] [PubMed]
- Hendrix, K.; Wilson, D.; Kievman, M.J.; Jatoi, A. Perspectives on the Medical, Quality of Life, and Economic Consequences of Hiccups. Curr. Oncol. Rep. 2019, 21, 113. [Google Scholar] [CrossRef]
- Schrock, L.E.; Patriat, R.; Goftari, M.; Kim, J.; Johnson, M.D.; Harel, N.; Vitek, J.L. 7T MRI and Computational Modeling Supports a Critical Role of Lead Location in Determining Outcomes for Deep Brain Stimulation: A Case Report. Front. Hum. Neurosci. 2021, 15, 631778. [Google Scholar] [CrossRef]
- Menon, M. Gabapentin in the treatment of persistent hiccups in advanced malignancy. Indian J. Palliat. Care 2012, 18, 138–140. [Google Scholar] [CrossRef]
- Friedman, N.L. Hiccups: A treatment review. Pharmacotherapy 1996, 16, 986–995. [Google Scholar] [PubMed]
- Palard-Novello, X.; Drapier, S.; Bonnet, A.; Girard, A.; Robert, G.; Houvenaghel, J.F.; Sauleau, P.; Verin, M.; Haegelen, C.; Le Jeune, F. Deep brain stimulation of the internal globus pallidus does not affect the limbic circuit in patients with Parkinson′s disease: A PET study. J. Neurol. 2021, 268, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Lertxundi, U.; Marquinez, A.C.; Domingo-Echaburu, S.; Solinis, M.A.; Calvo, B.; Del Pozo-Rodriguez, A.; Garcia, M.; Aguirre, C.; Isla, A. Hiccups in Parkinson′s disease: An analysis of cases reported in the European pharmacovigilance database and a review of the literature. Eur. J. Clin. Pharmacol. 2017, 73, 1159–1164. [Google Scholar] [CrossRef]
- Marshall, J.M.; Ladd, M.D.; Weldon, B.C. Prevention of persistent postoperative hiccups with dexmedetomidine. J. Clin. Anesth. 2019, 52, 50. [Google Scholar] [CrossRef]
- Kohse, E.K.; Hollmann, M.W.; Bardenheuer, H.J.; Kessler, J. Chronic Hiccups: An Underestimated Problem. Anesth. Analg. 2017, 125, 1169–1183. [Google Scholar] [CrossRef] [PubMed]
- Chang, F.Y.; Lu, C.L. Hiccup: Mystery, nature and treatment. J. Neurogastroenterol. Motil. 2012, 18, 123–130. [Google Scholar] [CrossRef] [Green Version]
- Hansen, B.J.; Rosenberg, J. Persistent postoperative hiccups: A review. Acta Anaesthesiol. Scand. 1993, 37, 643–646. [Google Scholar] [CrossRef]
- Miwa, H.; Kondo, T. Hiccups in Parkinson′s disease: An overlooked non-motor symptom? Parkinsonism Relat. Disord. 2010, 16, 249–251. [Google Scholar] [CrossRef]
- Amirjamshidi, A.; Abbassioun, K.; Parsa, K. Hiccup and neurosurgeons: A report of 4 rare dorsal medullary compressive pathologies and review of the literature. Surg. Neurol. 2007, 67, 395–402. [Google Scholar] [CrossRef]
- De Seze, J.; Zephir, H.; Hautecoeur, P.; Mackowiak, A.; Cabaret, M.; Vermersch, P. Pathologic laughing and intractable hiccups can occur early in multiple sclerosis. Neurology 2006, 67, 1684–1686. [Google Scholar] [CrossRef]
- Park, M.H.; Kim, B.J.; Koh, S.B.; Park, M.K.; Park, K.W.; Lee, D.H. Lesional location of lateral medullary infarction presenting hiccups (singultus). J. Neurol. Neurosurg. Psychiatry 2005, 76, 95–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musumeci, A.; Cristofori, L.; Bricolo, A. Persistent hiccup as presenting symptom in medulla oblongata cavernoma: A case report and review of the literature. Clin. Neurol. Neurosurg. 2000, 102, 13–17. [Google Scholar] [CrossRef]
- De Bie, R.M.; Speelman, J.D.; Schuurman, P.R.; Bosch, D.A. Transient hiccups after posteroventral pallidotomy for Parkinson′s disease. J. Neurol. Neurosurg. Psychiatry 1999, 67, 124–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giugni, J.; Seijo, D.; Micheli, F. Are hiccups non-motor symptoms? Parkinsonism Relat. Disord. 2010, 16, 690. [Google Scholar] [CrossRef] [PubMed]
- Lester, J.; Raina, G.B.; Uribe-Roca, C.; Micheli, F. Hiccup secondary to dopamine agonists in Parkinson′s disease. Mov. Disord. 2007, 22, 1667–1668. [Google Scholar] [CrossRef]
- Coletti Moja, M. Hiccups associated with non-ergoline dopamine agonists in Parkinson′s disease. Mov. Disord. 2010, 25, 1292. [Google Scholar] [CrossRef]
- Gerschlager, W.; Bloem, B.R. Hiccups associated with levodopa in Parkinson′s disease. Mov. Disord. 2009, 24, 621–622. [Google Scholar] [CrossRef]
- Stegmeier-Petroianu, A.; Petroianu, G.A. Hiccups and dopamine. Am. J. Health. Syst. Pharm. 2008, 65, 2092–2094. [Google Scholar] [CrossRef]
- Sharma, P.; Morgan, J.C.; Sethi, K.D. Hiccups associated with dopamine agonists in Parkinson disease. Neurology 2006, 66, 774. [Google Scholar] [CrossRef]
- Collins, D.R.; Wanklyn, P. Hiccoughs—An unusual dyskinetic side-effect of L-Dopa. Age Ageing 2002, 31, 405–406. [Google Scholar] [CrossRef]
- Jiang, N.; Ling, Y.T.; Yang, C.; Liu, Y.; Xian, W.B.; Zhang, L.N.; Guo, Q.Q.; Jin, X.Y.; Wu, B.; Zhang, C.M.; et al. Optimized Propofol Anesthesia Increases Power of Subthalamic Neuronal Activity in Patients with Parkinson′s Disease Undergoing Deep Brain Stimulation. Neurol. Ther. 2021, 10, 785–802. [Google Scholar] [CrossRef] [PubMed]
- Saitoh, T.; Enatsu, R.; Mikami, T.; Suzuki, Y.; Kanno, A.; Kitagawa, M.; Mikuni, N. Peri-electrode edema after deep brain stimulation. J. Clin. Neurosci. 2019, 59, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.W.; Kim, R.B.; Go, S.I.; Cho, H.S.; Lee, S.J.; Hui, D.; Bruera, E.; Kang, J.H. Gender Differences in Hiccup Patients: Analysis of Published Case Reports and Case-Control Studies. J. Pain Symptom Manag. 2016, 51, 278–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rey, E.; Elola-Olaso, C.M.; Rodriguez-Artalejo, F.; Locke, G.R., 3rd; Diaz-Rubio, M. Prevalence of atypical symptoms and their association with typical symptoms of gastroesophageal reflux in Spain. Eur. J. Gastroenterol. Hepatol. 2006, 18, 969–975. [Google Scholar] [CrossRef]
- Englot, D.J.; Glastonbury, C.M.; Larson, P.S. Abnormal T2-weighted MRI signal surrounding leads in a subset of deep brain stimulation patients. Stereotact. Funct. Neurosurg. 2011, 89, 311–317. [Google Scholar] [CrossRef]
- Kim, J.W.; Hwang, J.H.; Kim, I.K.; Kim, Y.E.; Yang, H.J.; Ehm, G.; Kim, H.J.; Kim, D.G.; Paek, S.H.; Jeon, B.S. Acute brain reaction to DBS electrodes after deep brain stimulation: Chronological observation. Acta Neurochir. 2013, 155, 2365–2371. [Google Scholar] [CrossRef]
- Askenasy, J.J.; Boiangiu, M.; Davidovitch, S. Persistent hiccup cured by amantadine. N. Engl. J. Med. 1988, 318, 711. [Google Scholar]
- Wilcox, S.K.; Garry, A.; Johnson, M.J. Novel use of amantadine: To treat hiccups. J. Pain Symptom Manag. 2009, 38, 460–465. [Google Scholar] [CrossRef]
- Nausheen, F.; Mohsin, H.; Lakhan, S.E. Neurotransmitters in hiccups. Springerplus 2016, 5, 1357. [Google Scholar] [CrossRef] [Green Version]
- Rouse, S.; Wodziak, M. Intractable Hiccups. Curr. Neurol. Neurosci. Rep. 2018, 18, 51. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Non-Hiccups | Hiccups | p Value | |
|---|---|---|---|---|
| n = 191 | n = 157 | n = 34 | ||
| Demographic characteristics | ||||
| Age (years) | 59.90 ± 9.26 | 60.29 ± 9.11 | 58.09 ± 9.86 | 0.21 |
| Age at onset of PD (years) | 48.77 ± 11.76 | 48.93 ± 11.68 | 48.03 ± 12.25 | 0.69 |
| Male sex | 118 (61.78) | 85 (54.14) | 33 (97.06) | <0.01 |
| Body mass index (kg/m2) | 23.92 ± 14.74 | 23.81 ± 16.22 | 24.44 ± 2.51 | <0.01 |
| Diabetes | 15 (7.85) | 12 (7.64) | 3 (8.82) | 0.82 |
| Hypertension | 47 (24.61) | 38 (24.20) | 9 (26.47) | 0.78 |
| Smoker (current/former) | 25 (13.09) | 17 (10.83) | 8 (23.53) | 0.05 |
| Duration of PD (years) | 9.79 ± 3.99 | 9.97 ± 4.15 | 8.97 ± 3.01 | 0.19 |
| Drug duration (years) | 8.76 ± 3.55 | 8.86 ± 3.62 | 8.30 ± 3.22 | 0.40 |
| Clinical evaluations | ||||
| Hoehn and Yahr stage, off | 3.186 ± 0.72 | 3.30 ± 0.73 | 2.99 ± 0.65 | 0.08 |
| Hoehn and Yahr stage, on | 2.178 ± 0.66 | 2.17 ± 0.66 | 2.24 ± 0.65 | 0.58 |
| MDS-UPDRS III off | 50.43 ± 16.28 | 50.82 ± 16.71 | 48.65 ± 14.21 | 0.48 |
| Tremor domination | 101 (52.88) | 80 (50.96) | 21 (61.76) | 0.26 |
| Levodopa challenge test (%) | 61.70 ± 12.77 | 61.41 ± 13.06 | 63.02 ± 11.41 | 0.51 |
| Dysarthria | 149 (78.01) | 120 (76.43) | 29 (85.29) | 0.26 |
| Apathy | 35 (18.32) | 29 (18.47) | 6 (17.65) | 0.91 |
| MMSE score | 27.20 ± 3.16 | 27.05 ± 3.40 | 27.88 ± 1.57 | 0.17 |
| HAMA score | 0.01 | |||
| <8, normal | 121 (63.35) | 93 (59.24) | 28 (82.35) | |
| 8–14, anxiety, may be | 51 (26.70) | 45 (28.66) | 6 (17.65) | |
| 15–21, anxiety (mild) | 13 (6.81) | 13 (8.28) | 0 | |
| >21, anxiety (moderate/severe) | 6 (3.14) | 6 (10.19) | 0 | |
| HAMD score | 0.02 | |||
| <8, normal | 99 (51.83) | 76 (48.41) | 23 (67.65) | |
| 8–20, suspicious depression | 77 (40.31) | 66 (42.04) | 11 (32.35) | |
| >20, depression | 15 (7.85) | 15 (9.55) | 0 | |
| Constipation | 143 (74.87) | 116 (73.89) | 27 (79.41) | 0.50 |
| Total number of MER trajectories | 2.66 ± 1.18 | 2.66 ± 1.20 | 2.68 ± 1.07 | 0.64 |
| Anesthesia time (minutes) | 420.87 ± 63.92 | 422.64 ± 63.67 | 412.71 ± 65.38 | 0.41 |
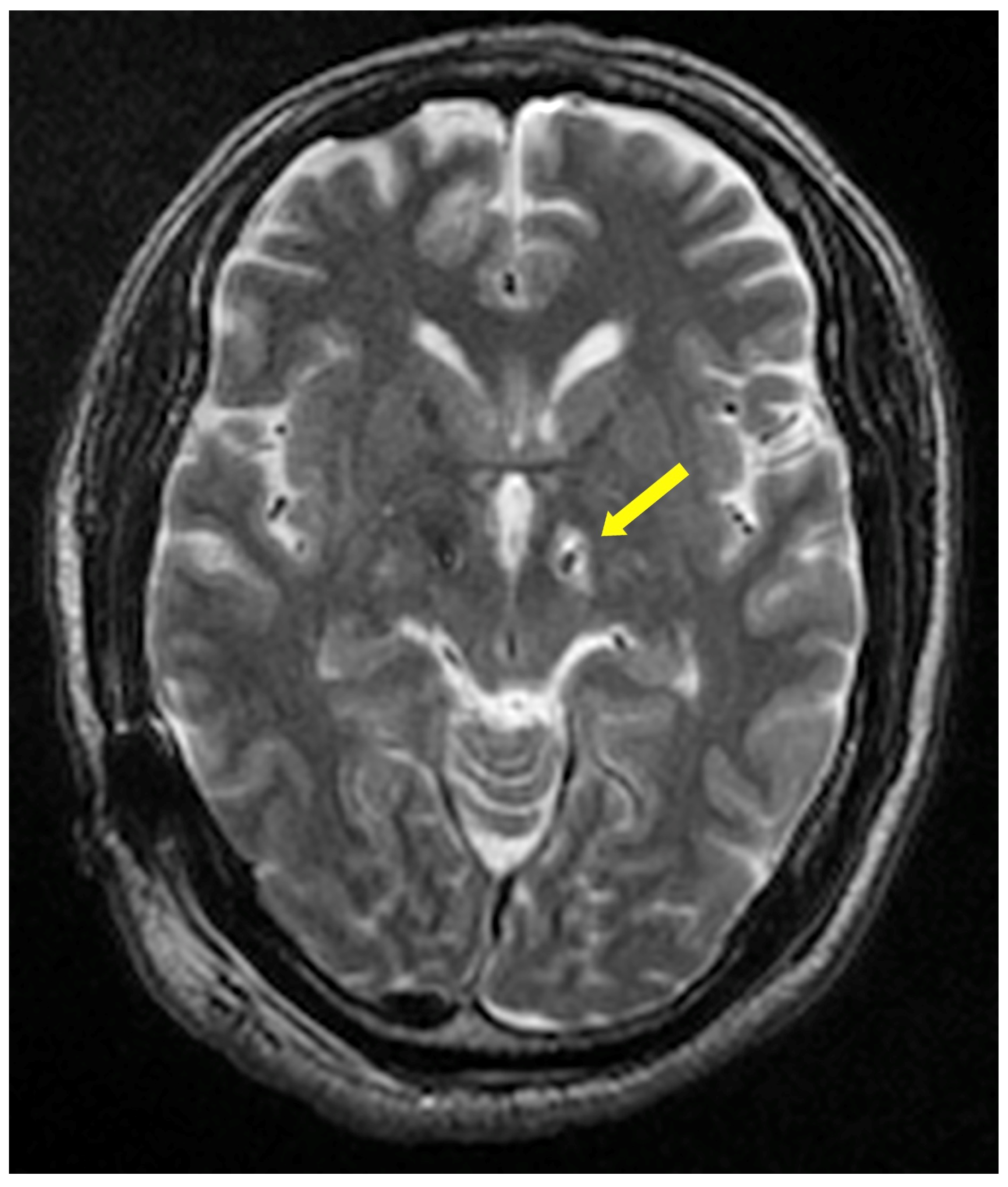
| Limited peri-electrode edema on T2 | 145 (75.92) | 121 (70.07) | 32 (94.12) | 0.04 |
| Extensive T2 hyperintensity in surface white matter around the electrode | 153 (80.10) | 121 (70.07) | 24 (70.59) | 0.42 |
| Medications | ||||
| LEDD (mg) | 818.85 ± 375.63 | 817.64 ± 399.83 | 824.43 ± 237.92 | 0.92 |
| Amantadine | 26 (13.61) | 18 (11.46) | 8 (23.53) | 0.07 |
| Trihexyphenidyl | 24 (12.57) | 17 (10.83) | 7 (20.59) | 0.13 |
| Pramipexole | 102 (52.88) | 83 (52.87) | 19 (55.88) | 0.75 |
| Piribedil | 43 (22.51) | 32 (20.38) | 11 (32.35) | 0.13 |
| Ropinirole | 11 (5.76) | 9 (5.73) | 2 (5.88) | 0.97 |
| COMT inhibitors | 89 (46.60) | 76 (48.41) | 13 (38.24) | 0.28 |
| MAOB inhibitors | 44 (23.04) | 33 (21.02) | 11 (32.35) | 0.16 |
| Preoperative antipsychotics | 22 (11.52) | 20 (12.74) | 2 (5.88) | 0.27 |
| Preoperative hypnotics | 64 (33.51) | 59 (37.58) | 5 (14.71) | 0.02 |
| Intraoperative use of etomidate | 39 (20.42) | 34 (21.66) | 5 (14.71) | 0.37 |
| Postoperative use of dexamethasone | 127 (66.49) | 101 (64.33) | 26 (76.47) | 0.18 |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Odds Ratio | Lower | Upper | p Value | Odds Ratio | Lower | Upper | p Value | |
| Male | 27.95 | 3.73 | 209.47 | <0.01 | 14.00 | 1.74 | 112.43 | 0.01 |
| Body mass index | 3.60 | 1.75 | 7.40 | <0.01 | 3.50 | 1.46 | 8.36 | 0.01 |
| Smoker (current/former) | 2.53 | 0.99 | 6.48 | 0.05 | - | - | - | - |
| Hoehn and Yahr tage, off | 0.60 | 0.34 | 1.06 | 0.08 | - | - | - | - |
| HAMA score | 0.34 | 0.15 | 0.78 | 0.01 | - | - | - | - |
| HAMD score | 0.43 | 0.22 | 0.87 | 0.02 | - | - | - | - |
| Limited peri-electrode edema on T2 | 4.76 | 1.09 | 20.8 | 0.04 | 7.63 | 1.37 | 42.37 | 0.02 |
| Amantadine | 2.38 | 0.94 | 6.04 | 0.07 | 3.64 | 1.08 | 12.28 | 0.04 |
| Preoperative hypnotic | 0.29 | 0.11 | 0.78 | 0.02 | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, B.; Ling, Y.; Zhang, C.; Liu, Y.; Xuan, R.; Xu, J.; Li, Y.; Guo, Q.; Wang, S.; Liu, L.; et al. Risk Factors for Hiccups after Deep Brain Stimulation of Subthalamic Nucleus for Parkinson’s Disease. Brain Sci. 2022, 12, 1447. https://doi.org/10.3390/brainsci12111447
Wu B, Ling Y, Zhang C, Liu Y, Xuan R, Xu J, Li Y, Guo Q, Wang S, Liu L, et al. Risk Factors for Hiccups after Deep Brain Stimulation of Subthalamic Nucleus for Parkinson’s Disease. Brain Sciences. 2022; 12(11):1447. https://doi.org/10.3390/brainsci12111447
Chicago/Turabian StyleWu, Bin, Yuting Ling, Changming Zhang, Yi Liu, Ruoheng Xuan, Jiakun Xu, Yongfu Li, Qianqian Guo, Simin Wang, Lige Liu, and et al. 2022. "Risk Factors for Hiccups after Deep Brain Stimulation of Subthalamic Nucleus for Parkinson’s Disease" Brain Sciences 12, no. 11: 1447. https://doi.org/10.3390/brainsci12111447