
The Link between ADHD Symptoms and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence


1
Paul Baerwald School of Social Work and Social Welfare, The Hebrew University of Jerusalem, Jerusalem 9190501, Israel
2
Seymour Fox School of Education, The Hebrew University of Jerusalem, Jerusalem 9190501, Israel
*
Author to whom correspondence should be addressed.
Brain Sci. 2022, 12(10), 1336; https://doi.org/10.3390/brainsci12101336
Submission received: 30 August 2022
/
Revised: 26 September 2022
/
Accepted: 27 September 2022
/
Published: 3 October 2022
(This article belongs to the Special Issue Advances in ADHD)
Abstract
:Numerous studies have established the link between ADHD and antisocial behavior, one of the most serious functional impairments caused by the disorder. However, research on protective factors that mitigate this link is still lacking. The Salutogenic Model of Health offers the “Sense of Coherence” (SOC), establishing that individuals who see their lives as logical, meaningful, and manageable are more resistant to various risk factors and diseases. The present study examines for the first time whether SOC is also a protective factor against different ADHD-related types of antisocial behaviors (severe/mild violent behavior, verbal violence, property crimes, public disorder, and drug abuse). A total of 3180 participants aged 15–50 completed online questionnaires assessing the level of ADHD symptoms, antisocial behaviors, and SOC. Structural equation modeling was applied to examine the research hypothesis. An interaction between ADHD symptoms and SOC was found in predicting each type of antisocial behavior (beta = −0.06–−0.17, p < 0.01). The link between ADHD symptoms and antisocial behavior was significantly weaker for high than low SOC participants, regardless of age group. The current study found that people with high SOC are protected against the effect of ADHD symptoms on one of the most serious functional impairments, antisocial behavior. These findings suggest that SOC is a protective factor from the adverse effects of ADHD symptoms, justifying further prospective and intervention studies.
1. Introduction
1.1. The Link between ADHD and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence
ADHD is a common neurodevelopmental condition defined by symptoms of inattention, hyperactivity, and impulsivity, accompanied by academic, occupational, or social functional impairment [1]. The functional impairment that this study focuses on is antisocial behavior. This term refers to a range of antisocial behaviors, both criminal and noncriminal (such as verbal aggression) [2].
1.2. ADHD and Antisocial Behavior
Numerous studies have indicated that ADHD is associated with antisocial behavior and delinquent acts [3]. The results of these studies demonstrated that, in comparison to individuals without ADHD, adolescents, young adults, and middle-aged adults with ADHD tend to be more involved in the criminal justice system, are arrested and convicted at an earlier age, and have an increased risk of conviction, incarceration, and criminal recidivism [4].
The prevalence of ADHD among incarcerated people is high and estimated at around 25–45%, varying depending on the measurement method [5]. Longitudinal studies that examined childhood ADHD found that it predicts a higher prevalence of antisocial behavior in adulthood [6]. In the general population, levels of ADHD symptoms predict antisocial behavior even after controlling for additional risk factors [7]. Similarly, the association between ADHD and antisocial behavior remained significant after controlling for a wide range of psychosocial variables [4,5]. It seems, therefore, that there is a clear correlation between ADHD and antisocial behavior. Still, most people with ADHD do not engage in antisocial behavior, suggesting that other factors influence the relationship. Therefore, we suggest looking for a factor that mitigates the link between ADHD symptoms and antisocial behavior.
1.3. Interaction in the Prediction of Antisocial Behavior
Various variables that interact with ADHD symptoms in the prediction of antisocial behavior have been examined in the research literature. For example, it was found that targeted drug therapy for ADHD decreases antisocial behavior by 30–40% [3,4]. Other studies reported an interaction between ADHD and variables such as substance use and past arrest in predicting delinquent behavior [8,9,10]. Notably, these moderating variables are in themselves on the spectrum of antisocial behavior. Therefore, to understand how ADHD leads to antisocial behavior, it is crucial to find other factors that do not constitute a type of antisocial behavior themselves.
Several studies focused on religiosity as a potential moderator, yielding inconsistent results. In one study, religiosity increased the risk of antisocial behavior such that, for religious people, ADHD was a weaker predictor of antisocial behavior. In another study, high ADHD symptoms combined with high religious participation predicted increased levels of antisocial behavior [11]. A prospective study, which examined the effect of childhood ADHD on adolescent antisocial behavior, found that a good parent–child relationship moderated and decreased the risk of antisocial behavior. Thus, among 15-year-old adolescents whose parents showed a more considerable decrease in parental involvement, increases in hyperactivity/impulsivity predicted higher levels of antisocial behaviors.
In contrast, among adolescents whose parents showed a more considerable or no decrease in parental involvement, increases in hyperactivity/impulsivity symptoms did not predict antisocial behaviors [12]. Another study found positive parenting to moderate the relation between ADHD symptoms and positive alcohol expectancies among children in grades 4–12 [13]. ADHD symptoms predicted higher positive alcohol expectancies at high levels of positive parenting, whereas, at low levels of positive parenting, ADHD symptoms predicted lower positive alcohol expectancies. As alcohol expectancies are highly related to alcohol use, this moderation effect was not in the expected direction, yet it shows that contextual characteristics may affect the relation between ADHD symptoms and antisocial behaviors [14]. Furthermore, it was found that an agreeable personality moderated the relation between ADHD symptoms and antisocial behavior. Specifically, among adults with a childhood history of ADHD symptoms and conduct problems, higher levels of agreeableness weakened the association between inattention and level of criminal involvement [15].
To summarize, a literature review demonstrates the paucity of research on psychosocial factors that do not constitute antisocial behavior by themselves but moderate the relation between ADHD symptoms and antisocial behavior. The present study aims to fill in this gap.
1.4. Sense of Coherence
The Salutogenic Model of Health focuses on health promotion, setting out against what is termed the “pathogenic approach”: the assumption that the basic human condition is health, hence focusing on risk factors involved in disease generation [16,17,18]. On the other hand, the Salutogenic Model assumes that health is under constant threat by various risk factors, thus focusing on factors contributing to defense mechanisms, which help to generate health [18]. Analogously, other researchers claimed that ADHD symptoms exist on a spectrum and do not necessarily entail functional impairment [19,20] and that the severity of both symptoms and functional impairment can be recompensated by various protective factors [21,22]. Therefore, it is vital to study the protective factors that decrease various risks associated with ADHD symptoms.
The Salutogenic Model of Health offers the concept of the “Sense of Coherence” (SOC) as a protective factor. SOC consists of three components (usually treated as a unified concept): comprehensibility (the cognitive component)—the degree to which one perceives the world as logical, consistent, and predictable; meaningfulness (the emotional component)—the degree to which one sees her or his life as meaningful and worthy of effort; and manageability (the behavioral component)—the degree to which one views oneself as competent and capable of influencing reality [17,23]. The theory contends that individuals with high SOC, who see their lives as logical, meaningful, and manageable, are more resistant to various risk factors.
Numerous studies highlighted the relation between SOC and normative behavior [24]. For example, it was found that poor SOC was associated with a higher level of criminal offenses in young males and with recidivism [25,26]. High SOC was associated with decreased antisocial behavior, such as smoking, alcohol consumption, and violent behavior [27,28]. Moreover, a study that was conducted on 5000 participants showed that patterns of substance use in the peer group predicted substance use of adolescents better in subjects with low SOC than in subjects with high SOC [10], suggesting that coherence is a moderator of the link between risk factors and antisocial behavior.
Only a few studies examined SOC in the context of ADHD. A longitudinal study demonstrated both an association and an interaction between SOC and ADHD. Thus, 16-year-old adolescents with ADHD reported lower SOC. Moreover, ADHD scores at age 16 predicted ADHD scores at age 21 more strongly for people with lower SOC [29]. It was also found that the high SOC was positively related to life satisfaction in ADHD students [30].
To summarize, the literature suggests that high SOC constitutes a protective factor against antisocial behavior. Furthermore, it may moderate various risk factors, including ADHD symptoms, and adverse outcomes, including antisocial behavior. Therefore, the research hypothesis is that the association between ADHD symptoms and antisocial behavior will be moderated by the level of coherence and reduced among subjects with high SOC.
2. Materials and Methods
2.1. Participants and Procedure
The study was authorized by the Hebrew University School of Social Work and Social Welfare’s ethics committee. The participants were recruited by convenience sampling, using an online questionnaire distributed on social networks (Whatsapp, Instagram, Facebook, and emails) in Israel in October–November 2020. We explained that our research goal was to understand individuals’ thoughts, feelings, behaviors, and coping strategies in various life situations. For those interested in participating, we offered a lottery of purchase tickets in a separate link (the winning ratio was 1:50 and the ticket value was about USD 12). We also asked the participants to answer the questionnaires and further distribute it. A total of 3415 participants between the ages of 15 and 50 responded to the questionnaire. A total of 235 participants were excluded since they did not answer any questionnaires or answered the questionnaires randomly, resulting in 3180 that were included in the statistical analyses. Participants were asked to complete scales that measure behavior, emotions, and perceptions in different life domains. Participants were provided information regarding the study procedures and how their privacy and confidentiality will be secured.
2.2. Measures
Antisocial behavior was measured using a scale based on the Self-Report Antisocial behavior (SRD) [31]. In its full version, the scale includes 47 items, which describe illegal or non-normative actions, and the respondent is requested to note the number of times the actions were performed in the last year. Internal consistency of the original scale was high (alpha = 0.91) [32]. The scale was translated to Hebrew using the back-translation method; the internal consistency of the Hebrew version was high (Cronbach’s α = 0.908) [33]. The scale was shortened and adapted so it included a wide range of ages. The adapted version of the scale consisted of 23 items, which referred to the following measures: four types of violent crimes: serious physical assault (4 items, ω = 0.729), mild physical assault (4 items, ω = 0.769), verbal assault (4 items, ω = 0.790), and indirect violence (3 items, ω = 0.559)); property crimes (5 items, ω = 0.784); and crimes against the public order (3 items, ω = 0.738). As the internal consistency of the indirect violence scale was poor, this scale was not further analyzed.
Drug use was measured using a scale developed by Johnston, O’Malley, and Bachman (1995), widely used in Hebrew translation in Israel [34]. Participants were asked to indicate their substance use in the last year. Specifically, they rated their use of cannabis (2 items), alcohol (2 items), and cigarette smoking (1 item) on a 7-point Likert scale (0 = never to 5 = 30 times or more). The internal consistency of the scale was acceptable (ω = 0.756).
The Hebrew version of the Adult ADHD Self-Report Scale (ASRS-v1.1) was used to measure the level of ADHD symptoms [35]. A total ASRS score was given by averaging all 18 items. In order to measure positive attention and impulse regulation behaviors in the general population, the wording of the 18 ADHD symptoms was phrased positively, in a similar manner to the SWAN questionnaire [36]. The internal consistency of the scale was good (ω = 0.887). The convergent validity of the scale was confirmed by a strong correlation (r = 0.655) with the Hyperactivity Problems subscale of the Strengths and Difficulties Questionnaire (see below).
A 13-item version of the SOC was used. The original scale has a high consistency and validity, and the internal consistency in the current study was good as well (ω = 0.888) [16,17]. The different components of the scale were analyzed as one variable [23].
Emotional problems were measured by the Strengths and Difficulties Questionnaire, which measures emotional and social adaptation (SDQ) [37]. The questionnaire consists of 25 items yielding five subscales. We used the emotional problems subscale as a covariate in the present study. We also used the Hyperactivity Problems scales for testing the convergent validity of the adapted ADHD symptoms scale. The reliability and validity of the scale have been established both for children and adults [38,39].
The participants filled out a socio-demographic questionnaire that included variables related to antisocial behavior and that were comparable between adolescents and adults: age, gender, and religiosity. Religiosity was measured by the question, “what is the level of your religiosity from 0 to 6? (0 = not religious, 6 = very religious)”. Age was categorized as late adolescence (15–18 years), young adulthood (19–30 years), and mid-adulthood (31–50 years).
2.3. Analytic Approach
The overall score of each scale was obtained by averaging the items of each respondent. We computed descriptive statistics of the dependent, independent, and covariates and the first-order correlations among the variables. We applied a structural equation modeling (SEM) using AMOS 26 [40] with a maximum-likelihood estimation method to examine the research hypotheses. SEM has several advantages over a series of regressions (e.g., PROCESS) as it can simultaneously test multiple hypotheses regarding multiple dependent variables in a single model and, thus, avoid alpha inflation. Another advantage of SEM is its ability to treat missing data using the full information maximum likelihood. We, therefore, modeled ADHD symptoms as a predictor of the six facets of antisocial behavior, with coherence as a moderator. Age, gender, religiousness, and emotional symptoms were modeled as covariates. Prior to analysis, ADHD symptoms and coherence were centered to their means to ensure a nonbiased interpretation of the results [41]. The six dependent variables were allowed to covariate in order to account for their potential associations. We tested the significance of the model’s effects using a p-value approach accompanied by a 95% CI based on 20,000 bias-corrected and accelerated bootstrap samples, which are more robust to violation of distributional assumptions. Significant ADHD symptoms by coherence interactions were probed into the conditional effects (i.e., simple slopes) of ADHD symptoms on antisocial behavior at high (mean + 1SD) and low (mean—1SD) levels of coherence. To further explore whether the moderation effect of coherence is stable across age groups, we used a multi-group analysis in SEM. Specifically, we contrasted two models, one in which the moderation effect was freely estimated in the two age groups and a second model in which the moderation effects in the age groups were constrained to equality. A significant chi-square difference between the two models (free vs. constrained) indicates that age further modifies the moderation effect of coherence. In contrast, a nonsignificant chi-square difference suggests that the moderation effect of coherence is equivalent across age groups.
3. Results
3.1. Descriptive Statistics
The means, standard deviations, medians, and minimum–maximum values of the demographic characteristics, ADHD symptoms, coherence, and antisocial behavior types are presented in Table 1. In total, 54.5% were women (N = 1614), 89.7% identified as Jewish, and 87.3% were born in Israel. Age groups consisted of 1125 late adolescents (38%), 925 young adults (31.3%), and 910 mid-adults (30.7%). The average religiosity level (on a 0 to 6 scale, see below) was 2.77 (SD = 1.44), and the average emotional problem score (on a 1 to 3 scale, see below) was 1.56 (SD = 0.48). Notably, 10.2% of the participants reported a diagnosis of ADHD.
3.2. Correlations
Spearman’s rho correlation coefficients were computed between demographic variables and ADHD symptoms, antisocial behavior types, and coherence (see Table S1 in the supplementary materials). ADHD symptoms were negatively correlated with age and religiosity and positively correlated with emotional symptoms. All antisocial behavior types were negatively correlated with age, gender, and religiosity (except for mild physical antisocial behavior, which was not significantly correlated with religiosity). Coherence was positively correlated with age and religiosity and negatively correlated with emotional symptoms and was higher in men than in women.
Spearman’s rho correlation coefficients were also computed between ADHD, antisocial behavior types, and coherence (Table 2). ADHD symptoms were positively correlated with all types of antisocial behavior (severe physical, mild physical, verbal, property, public order, and drugs). The Bonferroni method was used to correct for multiple analyses. Coherence was negatively correlated with ADHD symptoms and all types of antisocial behavior. Pearson correlations were also computed, resulting in a similar pattern (see Table S2 in the supplementary materials).
3.3. Moderation Analysis
We used SEM to conduct moderation analyses on the six facets of antisocial behavior. To allow an easier-to-follow presentation of the complex tested model (i.e., 36 main effects, six interactions, and six dependent variables), we herein present the results per each of the six dependent variables.
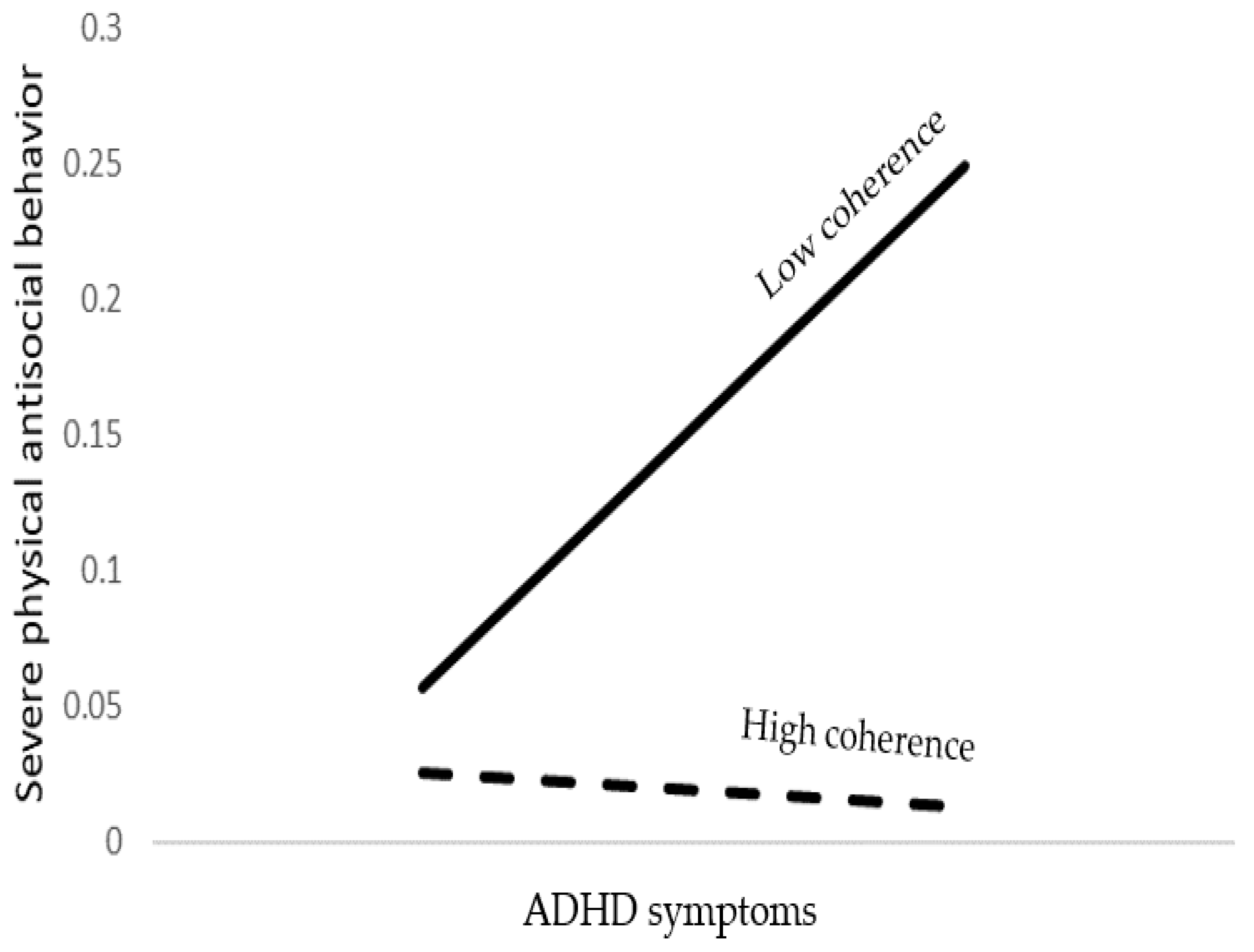
The model accounted for 15% of the severe physical antisocial behavior variance. As shown in Table 3, young age, male gender, lower emotional symptoms, higher ADHD symptoms, and lower coherence were significant predictors of severe physical antisocial behavior. In addition, ADHD symptoms by coherence interaction was found to be significant. Probing the interaction into conditional effects, as presented at the bottom of Table 3 and Figure 1, indicates that ADHD symptoms predicted severe physical antisocial behavior when coherence was low but not when coherence was high.
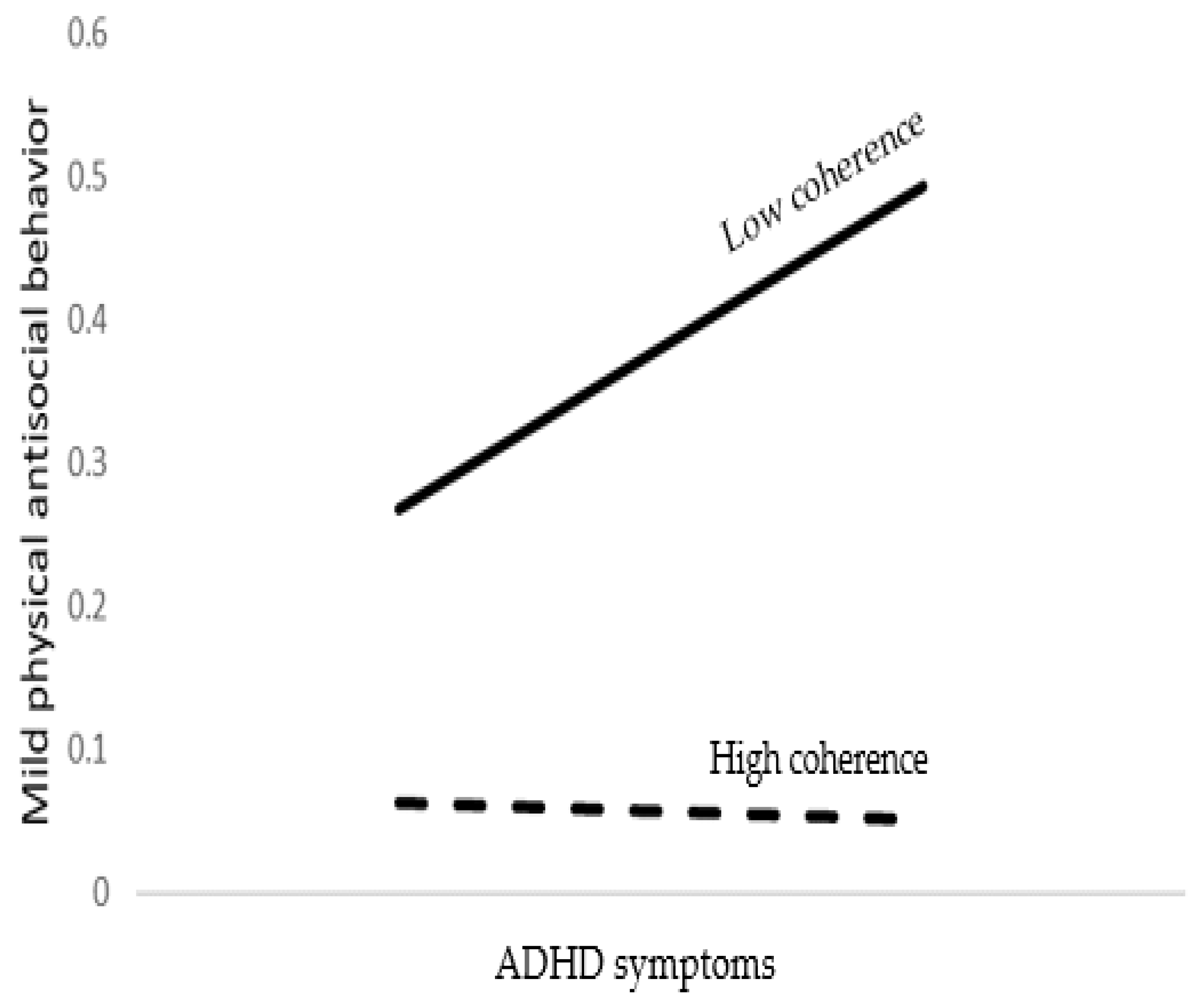
With regard to mild physical antisocial behavior, the model accounted for 20% of the variance. As shown in Table 4, young age, male gender, religiosity, lower emotional symptoms, higher ADHD symptoms, and lower coherence were significant predictors of mild physical antisocial behavior. As expected, an ADHD symptoms by coherence interaction was found to be significant. As shown at the bottom of Table 4 and Figure 2, ADHD symptoms predicted antisocial property behavior when coherence was low but not when coherence was high.
The SEM model accounted for 22% of the variance in verbal antisocial behavior. As shown in Table 5, young age, male gender, lower religiosity levels, lower emotional symptoms, higher ADHD symptoms, and lower coherence were significant predictors of verbal antisocial behavior. In addition, ADHD symptoms by coherence interaction was found to be significant. Probing the interaction into the conditional effects, as presented at the bottom of Table 5 and Figure 3, ADHD symptoms predicted verbal antisocial behavior more strongly when coherence was low than when coherence was high.
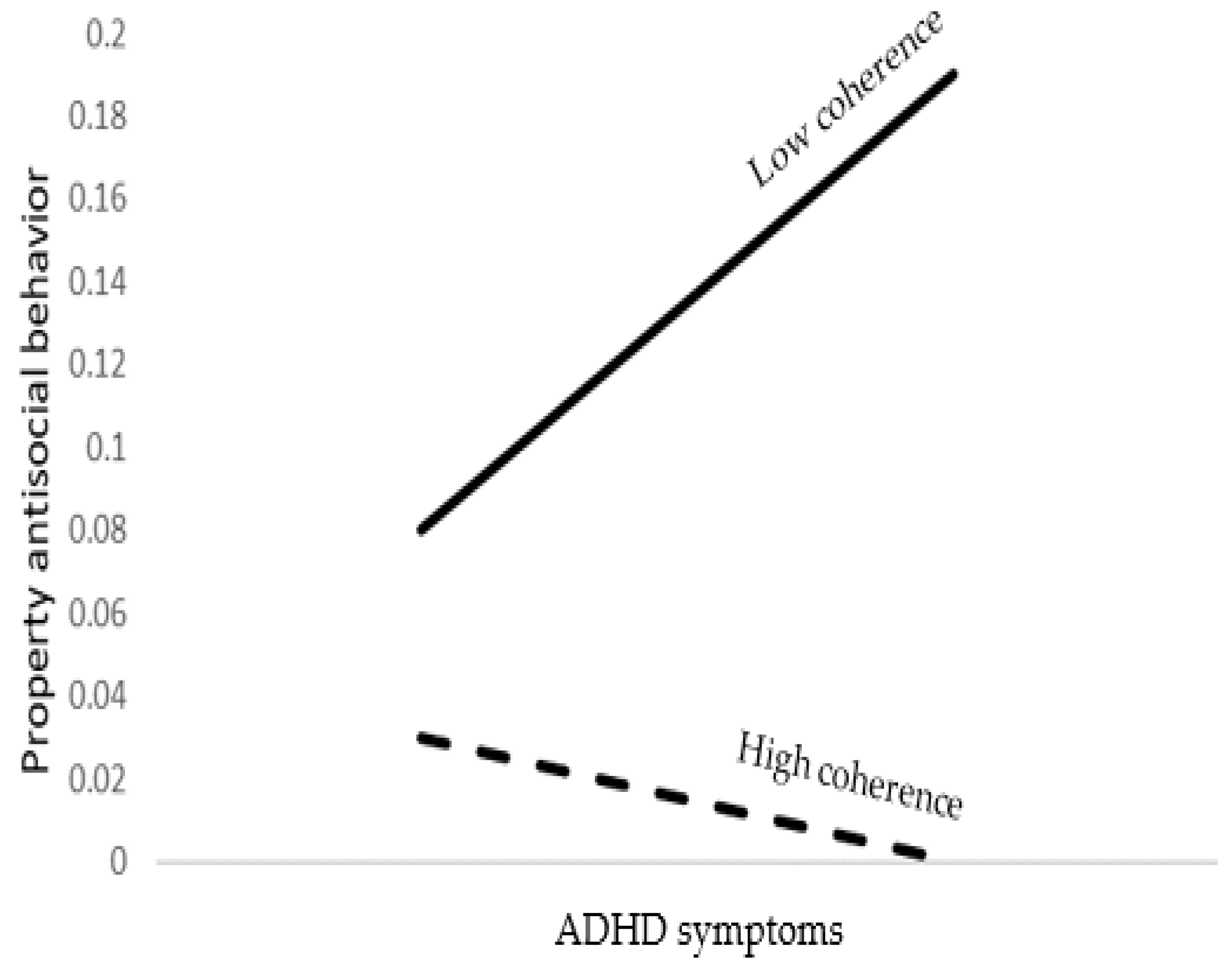
The tested model accounted for 12% of the variance in property crimes. As shown in Table 6, young age, male gender, lower religiosity levels, lower emotional symptoms, higher ADHD symptoms, and lower coherence were significant predictors of property crimes. As expected, a significant ADHD symptoms by coherence interaction was found. As shown at the bottom of Table 6 and Figure 4, ADHD symptoms predicted property crimes when coherence was low but not when high.
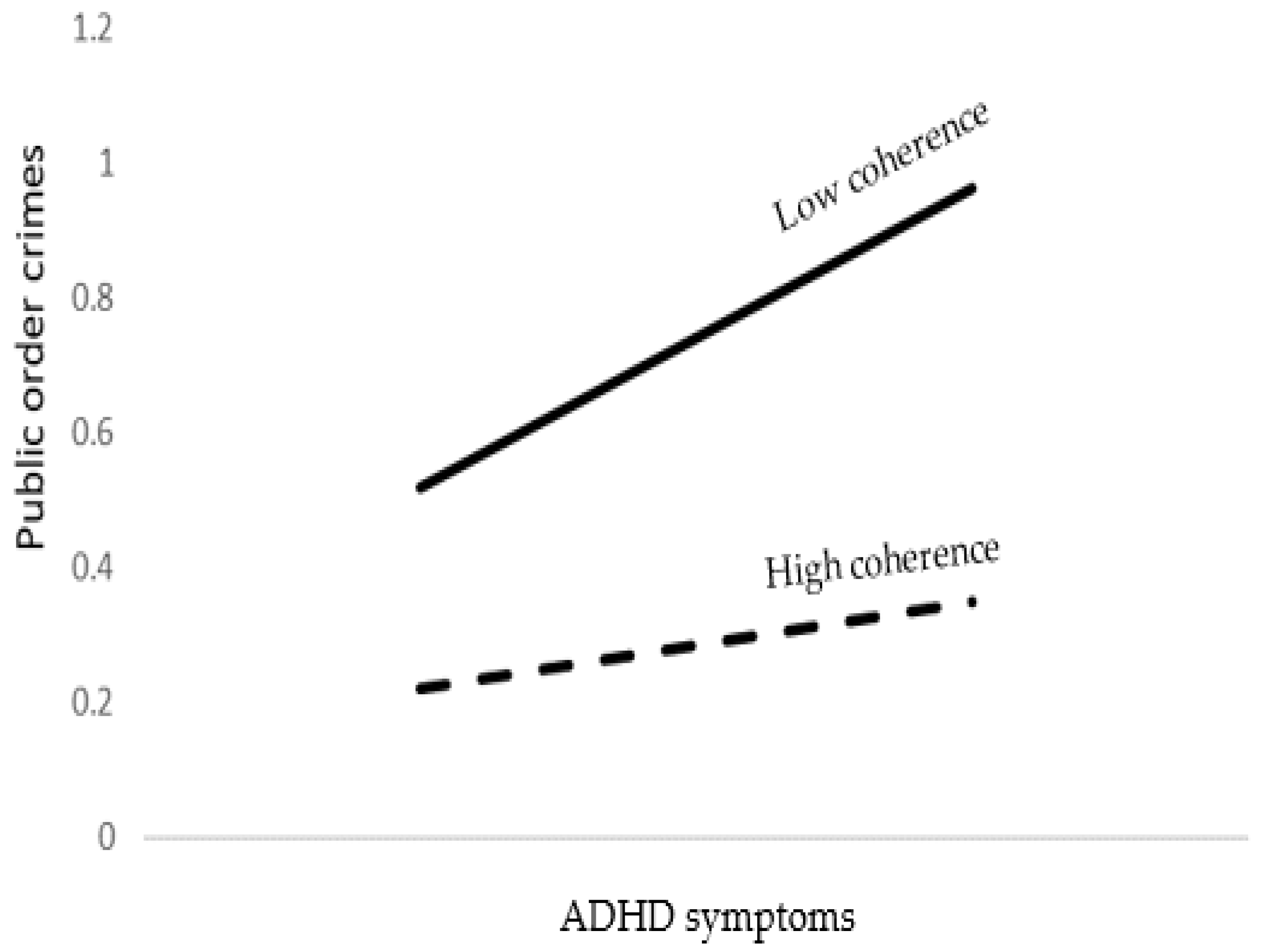
With regard to public order antisocial behavior, the model accounted for 20% of the variance. As shown in Table 7, young age, male gender, lower religiosity levels, lower emotional symptoms, higher ADHD symptoms, and lower coherence were significant predictors of public order antisocial behavior. In addition, ADHD symptoms by coherence interaction was found to be significant. Probing the interaction into conditional effects, as presented at the bottom of Table 7 and Figure 5, indicates that ADHD symptoms predicted public order antisocial behavior more strongly when coherence was low than high.
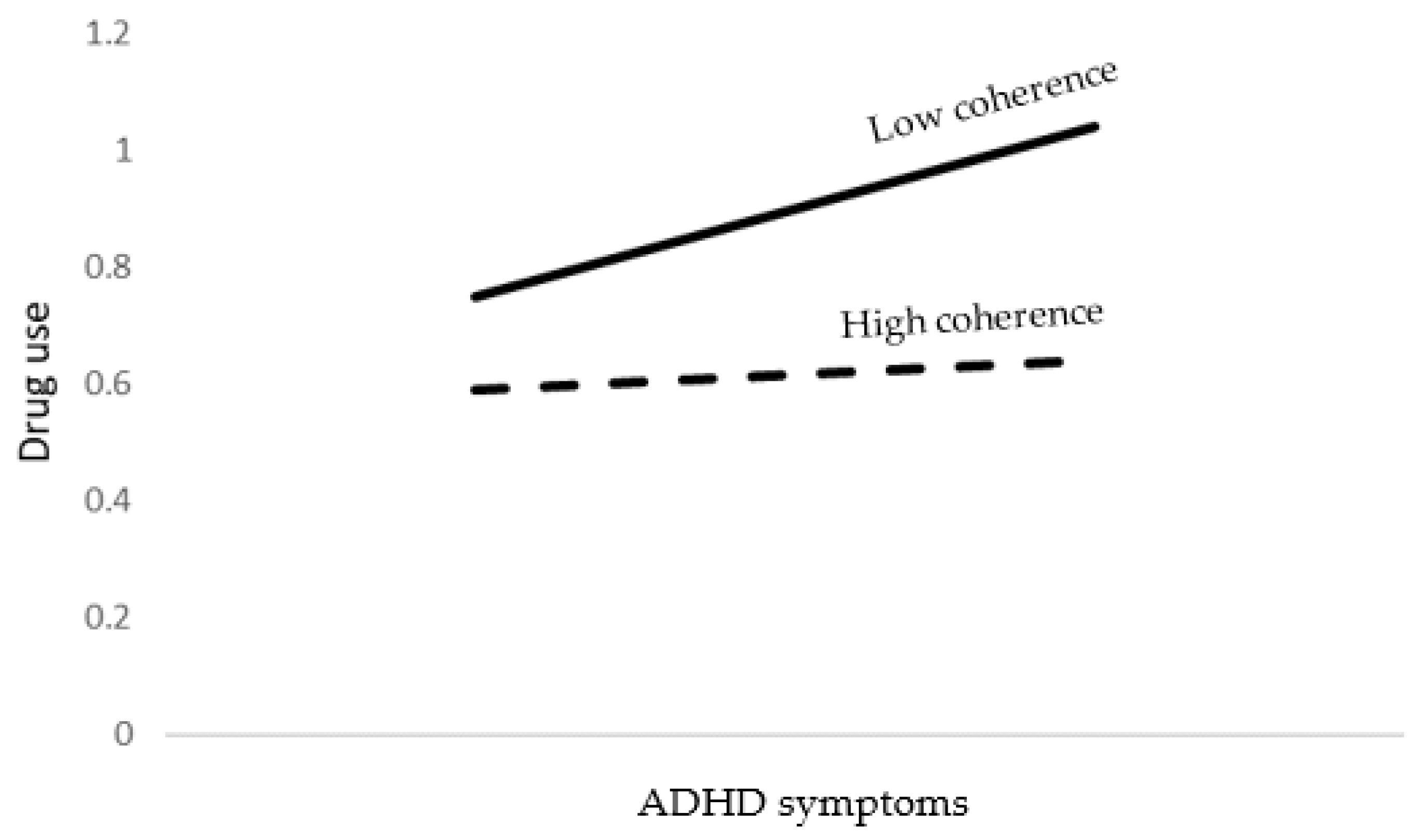
The SEM model accounted for 18% of the drug’s antisocial behavior variance. As shown in Table 8, older age, male gender, lower religiosity levels, lower emotional symptoms, higher ADHD symptoms, and lower coherence were significant predictors of drug use. In addition, ADHD symptoms by coherence interaction was found to be significant. As shown at the bottom of Table 8 and Figure 6, ADHD symptoms predicted drug use when coherence was low but not when high.
3.4. Age as a Moderator
We tested an additional model in which we added the age group as a moderating variable to examine whether the ADHD symptoms by coherence interaction is stable across age groups. Using a multigroup approach in SEM, we contrasted the fit indices of a free model versus a constrained model in which the ADHD symptoms by coherence interaction was forced to equality across age groups. Results indicated that the difference between the model was not significant (ΔChi-square = 9.13, df = 6, p = 0.168). This suggests that the age group does not significantly modify the moderation effect of coherence and that the reported conditional effects of ADHD symptoms on the six facets of antisocial behavior are similar across age groups.
4. Discussion
The present study examined the interaction between ADHD symptoms and the sense of coherence (SOC) in predicting various types of antisocial behavior. The research hypothesis was that SOC, which constitutes a protective factor in coping with diseases and neutralizing other risk factors, will also be a protective factor moderating the antisocial behavior risk that stems from ADHD symptoms [42].
This study examined several types of antisocial behavior and found that SOC moderated the relation between ADHD symptoms and antisocial behavior; for people with a strong SOC, the relation between ADHD symptoms and antisocial behavior decreased; in certain types of antisocial behavior, it was neutralized; and, in some cases, a negative association was found between ADHD symptoms and antisocial behavior. The research findings suggest that SOC constitutes a protective factor for the antisocial behavior risk of ADHD symptoms, similar to its ability to moderate another kind of risk for antisocial behavior, namely, peer influence. Specifically, the peer group’s patterns of substance use predicted adolescents’ substance use better in subjects with low SOC than in subjects with high SOC [10].
Assuming that SOC indeed decreases the levels of antisocial behavior, the generalizability question arises, i.e., whether SOC specifically protects against antisocial behavior or constitutes a general protective factor that decreases all functional impairments related to ADHD symptoms, including the impairment in well-being. The moderating role of coherence in protecting against other risks to well-being has been examined in many studies [42]. For example, a study investigating the relationship between work characteristics and well-being found that SOC has a moderating role in the relationships between specific risk factors and well-being. In another study, the association between social relations at work and well-being was stronger among subjects with a very low SOC, whereas these associations were less critical in determining well-being in subjects with a stronger SOC [43]. This question of moderating the risk of ADHD symptoms to other functional impairments is especially pertinent to the present study’s findings, since, in this study, ADHD symptoms were measured by self-report without an ADHD diagnosis. As ADHD diagnosis relies on the combination of ADHD symptoms and self-report of functional impairment, it is possible that participants who reported high SOC are those whose symptoms did not cause functional impairment and would not meet the criteria of ADHD diagnosis.
The main contribution of this study is showing that ADHD symptoms constitute a risk factor for antisocial behavior only when combined with further factors. This approach corresponds to the WHO’s International Classification of Functioning, Disability and Health (ICF) manual [44]. The ICF distinguishes between several concepts: impairments—problems in body function and structure, such as significant deviation or loss; activity limitation—difficulties an individual may have in executing activities; and participation restriction—problems an individual may experience in involvement in life situations. The individual’s functioning and health consist of the interactions between these three components with personal and developmental factors [44]. The ICF model was implemented in previous studies of ADHD [22,45,46]. The present study adds to the existing literature by implementing the ICF model in the context of ADHD symptoms and antisocial behavior.
Antisocial behavior can be defined as one of the central functional impairments associated with ADHD, which creates a participation restriction in normative society. The findings call for the application of the ICF model in the domain of ADHD and antisocial behavior, suggesting that the antisocial behavior stemming from ADHD is a product of the interaction between ADHD symptoms and a personal factor (SOC). This finding is consistent with the growing trend in the research literature calling for examining resilience factors for the risks for functional impairments associated with ADHD [12,21,22,45,46,47,48,49,50,51].
5. Limitations
Notably, since this research is cross-sectional, one cannot infer causality, and this issue needs to be examined using longitudinal and interventional designs. Findings of previous longitudinal studies indicate that SOC constitutes a protective factor for other outcome variables. For example, it was found that a strong SOC moderates the risk for long-term persistence of ADHD [29]. In addition, the phrasing of the items in the present study may also suggest that higher levels of SOC preceded the decrease in antisocial behavior. While participants were requested to refer to a general SOC in their life, in the antisocial behavior scale (SRD), they were requested to refer only to the last year.
The measuring of antisocial behavior relied on participants’ self-report without collateral support from other sources, such as partners’ reports or criminal records. However, it allows referring to antisocial behaviors that are not documented in criminal records. Notably, criminal records might contain a certain rate of false convictions due to false confessions, which are more prevalent among individuals with ADHD [52].
Another limitation is that the study examined ADHD symptoms in the past six months. Referring only to adulthood ADHD symptoms might supply a partial picture, since ADHD symptoms tend to be less conspicuous in adults [6]. Additionally, measuring ADHD symptoms using only self-report tends to lessen the actual level of ADHD symptoms [53]. Furthermore, in some studies, Adult ADHD Self-Report Scale had low specificity [54,55]. It is important to note that the research focuses on ADHD symptoms in the general population and not on diagnosed ADHD. Further research is needed to determine whether these correlations exist also in the diagnosed population. Finally, the study was conducted during a global pandemic, which might have influenced the level and severity of antisocial behavior [56].
6. Conclusions
Our study highlights the SOC as a protective factor that can be influenced by therapeutic intervention, similarly to what has been performed in the context of other disorders [57,58,59,60,61]. In light of the research findings, there is a need to explore the ICF model in the context of ADHD, using longitudinal studies, based on the understanding that functional impairments, such as antisocial behavior, are possible products of a relation between ADHD symptoms and other protective factors. Moreover, an interventional study is also needed to explore new methods of strengthening SOC among individuals with ADHD.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/brainsci12101336/s1, Table S1: Nonparametric Correlations between demographic characteristics, ADHD symptoms, antisocial behavior types and coherence; Table S2: Pearson correlations between the research variables.
Author Contributions
Conceptualization, H.D., M.K.-K. and Y.P.; Formal analysis, H.D. and Y.P.; Supervision, M.K.-K. and Y.P.; Writing—original draft, H.D.; Writing—review and editing, M.K.-K. and Y.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the ethics committee of the School of Social Work and Social Welfare’s, The Hebrew University of Jerusalem (15 May 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available because they contain self-reported criminal behavior.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviation List
| Amos | Analysis of Moment Structures |
| SOC | Sense Of Coherence |
| ADHD | Attention Deficit Hyperactivity Disorder |
| ICF | International Classification of Functioning, Disability and Health |
| WHO | World Health Organization |
| SWAN | Strengths and Weaknesses of Attention-Deficit/Hyperactivity Symptoms and Normal Behavior |
References
- Faraone, S.V.; Banaschewski, T.; Coghill, D.; Zheng, Y.; Biederman, J.; Bellgrove, M.A.; Newcorn, J.H.; Gignac, M.; Al Saud, N.M.; Manor, I.; et al. The World Federation of ADHD International Consensus Statement: 208 Evidence-based conclusions about the disorder. Neurosci. Biobehav. Rev. 2021, 128, 789–818. [Google Scholar] [CrossRef] [PubMed]
- Cuevas, C.A.; Finkelhor, D.; Shattuck, A.; Turner, H.A.; Hamby, S.L. Children’s exposure to violence and the intersection between delinquency and victimization. In The Societal Burden of Child Abuse; Taylor & Francis Group: London, UK, 2015. [Google Scholar]
- Retz, W.; Ginsberg, Y.; Turner, D.; Barra, S.; Retz-Junginger, P.; Larsson, H.; Asherson, P. Attention-Deficit/Hyperactivity Disorder (ADHD), antisociality and delinquent behavior over the lifespan. Neurosci. Biobehav. Rev. 2020, 120, 236–248. [Google Scholar] [CrossRef] [PubMed]
- Young, S.; Cocallis, K. ADHD and offending. J. Neural Transm. 2021, 128, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Baggio, S.; Fructuoso, A.; Guimaraes, M.; Fois, E.; Golay, D.; Heller, P.; Perroud, N.; Aubry, C.; Young, S.; Delessert, D.; et al. Prevalence of Attention Deficit Hyperactivity Disorder in Detention Settings: A Systematic Review and Meta-Analysis. Front. Psychiatry 2018, 9, 331. [Google Scholar] [CrossRef] [Green Version]
- Cherkasova, M.V.; Roy, A.; Molina, B.S.; Scott, G.; Weiss, G.; Barkley, R.A.; Biederman, J.; Uchida, M.; Hinshaw, S.P.; Owens, E.B.; et al. Review: Adult Outcome as Seen through Controlled Prospective Follow-up Studies of Children with Attention-Deficit/Hyperactivity Disorder Followed into Adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2021, 61, 378–391. [Google Scholar] [CrossRef]
- Mohr-Jensen, C.; Steinhausen, H.-C. A meta-analysis and systematic review of the risks associated with childhood attention-deficit hyperactivity disorder on long-term outcome of arrests, convictions, and incarcerations. Clin. Psychol. Rev. 2016, 48, 32–42. [Google Scholar] [CrossRef]
- van der Maas, M.; Kolla, N.J.; Erickson, P.G.; Wickens, C.M.; Mann, R.E.; Vingilis, E. Examining the effect of social bonds on the relationship between ADHD and past arrest in a representative sample of adults. Crim. Behav. Ment. Health 2017, 28, 120–131. [Google Scholar] [CrossRef]
- Breuer, D.; von Wirth, E.; Mandler, J.; Schürmann, S.; Döpfner, M. Predicting delinquent behavior in young adults with a childhood diagnosis of ADHD: Results from the Cologne Adaptive Multimodal Treatment (CAMT) Study. Eur. Child Adolesc. Psychiatry 2020, 31, 553–564. [Google Scholar] [CrossRef]
- García, B.H.; Vázquez, A.L.; Moses, J.O.; Cromer, K.D.; Morrow, A.S.; Villodas, M.T. Risk for substance use among adolescents at-risk for childhood victimization: The moderating role of ADHD. Child Abus. Negl. 2021, 114, 104977. [Google Scholar] [CrossRef]
- Dew, R.E.; Kollins, S.H.; Koenig, H.G. ADHD, Religiosity, and Psychiatric Comorbidity in Adolescence and Adulthood. J. Atten. Disord. 2020, 26, 307–318. [Google Scholar] [CrossRef]
- Giannotta, F.; Rydell, A.M. The prospective links between hyperactive/impulsive, inattentive, and oppositional-defiant behaviors in childhood and antisocial behavior in adolescence: The moderating influence of gender and the parent–child relationship quality. Child Psychiatry Hum. Dev. 2016, 47, 857–870. [Google Scholar] [CrossRef] [PubMed]
- Morse, M. ADHD Symptoms and Alcohol Expectancies: The Moderating Roles of Parenting and School Climate. Ph.D. Thesis, University of South Carolina, Columbia, SC, USA, 2020. [Google Scholar]
- Armeli, S.; Carney, M.A.; Tennen, H.; Affleck, G.; O’Neil, T.P. Stress and alcohol use: A daily process examination of the stressor–vulnerability model. J. Pers. Soc. Psychol. 2000, 78, 979–994. [Google Scholar] [CrossRef] [PubMed]
- Sagar, S. The Role of Protective Factors in Relation to Attentional Abilities in Emerging Adults. Ph.D. Thesis, University of Windsor, Windsor, ON, Canada, 2021. [Google Scholar]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 1987; ISBN 1555420281. [Google Scholar]
- Antonovsky, A. The structure and properties of the sense of coherence scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef]
- Haugan, G.; Eriksson, M. Health Promotion in Health Care—Vital Theories and Research; Springer Nature: Cham, Switzerlan, 2021. [Google Scholar]
- Faraone, S.V.; Biederman, J. Can Attention-Deficit/Hyperactivity Disorder Onset Occur in Adulthood? JAMA Psychiatry 2016, 73, 655–656. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.J.; Martin, J.; Lu, Y.; Brikell, I.; Lundström, S.; Larsson, H.; Lichtenstein, P. Association of Genetic Risk Factors for Psychiatric Disorders and Traits of These Disorders in a Swedish Population Twin Sample. JAMA Psychiatry 2019, 76, 280–289. [Google Scholar] [CrossRef]
- Lasky, A.K.; Weisner, T.S.; Jensen, P.S.; Hinshaw, S.P.; Hechtman, L.; Arnold, L.E.; Murray, D.W.; Swanson, J.M. ADHD in context: Young adults’ reports of the impact of occupational environment on the manifestation of ADHD. Soc. Sci. Med. 2016, 161, 160–168. [Google Scholar] [CrossRef] [Green Version]
- Sedgwick, J.A.; Merwood, A.; Asherson, P. The positive aspects of attention deficit hyperactivity disorder: A qualitative investigation of successful adults with ADHD. ADHD Atten. Deficit Hyperact. Disord. 2018, 11, 241–253. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, M.; Lindström, B. Validity of Antonovsky’s sense of coherence scale: A systematic review. J. Epidemiol. Community Health 2005, 59, 460–466. [Google Scholar] [CrossRef]
- Eriksson, M.; Lindström, B. Antonovsky’s sense of coherence scale and its relation with quality of life: A systematic review. J. Epidemiol. Community Health 2007, 61, 938–944. [Google Scholar] [CrossRef] [Green Version]
- Ristkari, T.; Sourander, A.; Ronning, J.; Helenius, H. Self-reported psychopathology, adaptive functioning and sense of coherence, and psychiatric diagnosis among young men: A population-based study. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 523–531. [Google Scholar] [CrossRef]
- Kishi, K.; Suzuki, J.; Monma, T.; Asanuma, T.; Takeda, F. Psychosocial and criminological factors related to recidivism among Japanese criminals at offender rehabilitation facilities. Cogent Soc. Sci. 2018, 4, 1489458. [Google Scholar] [CrossRef]
- Nilsson, K.W.; Starrin, B.; Simonsson, B.; Leppert, J. Alcohol-related problems among adolescents and the role of a sense of coherence. Int. J. Soc. Welf. 2006, 16, 159–167. [Google Scholar] [CrossRef]
- Mattila, M.-L.; Rautava, P.; Honkinen, P.-L.; Ojanlatva, A.; Jaakkola, S.; Aromaa, M.; Suominen, S.; Helenius, H.; Sillanpää, M. Sense of coherence and health behaviour in adolescence. Acta Paediatr. 2011, 100, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Edbom, T.; Malmberg, K.; Lichtenstein, P.; Granlund, M.; Larsson, J.-O.; Rn, T.E.; Larsson, J. High sense of coherence in adolescence is a protective factor in the longitudinal development of ADHD symptoms. Scand. J. Caring Sci. 2010, 24, 541–547. [Google Scholar] [CrossRef]
- Allah-Gholilo, K.; Abolghasemi, A.; Dehghan, H.; Imani, H. The Association of Alexithymia and Sense of Coherence With Life Satisfaction in Attention Deficit Hyperactivity Disorder. Zahedan J. Res. Med. Sci. 2015, 17. [Google Scholar] [CrossRef] [Green Version]
- Elliott, D.S.; Ageton, S.S. Reconciling Race and Class Differences in Self-Reported and Official Estimates of Delinquency. Am. Sociol. Rev. 1980, 45, 95–110. [Google Scholar] [CrossRef]
- Liau, A.K.; Barriga, A.Q.; Gibbs, J.C. Relations between self-serving cognitive distortions and overt vs. Covert antisocial behavior in adolescents. Aggress. Behav. 1998, 24, 335–346. [Google Scholar] [CrossRef]
- Elizur, Y.; Spivak, A.; Ofran, S.; Jacobs, S. A Gender-Moderated Model of Family Relationships and Adolescent Adjustment. J. Clin. Child Adolesc. Psychol. 2007, 36, 430–441. [Google Scholar] [CrossRef]
- Schiff, M.; Benbenishty, R.; Hamburger, R. Adolescents’ Exposure to Negative Life Events and Substance Use: Risk and Protective Factors—Comparison between Adolescents Who Were Born in the Former Soviet Union and Those Who Were Born in Israel; Final report; Israel Anti-Drug Authority: Jerusalem, Pakistan, 2008. [Google Scholar]
- Zohar, A.H.; Konfortes, H. Diagnosing ADHD in Israeli adults: The psychometric properties of the adult ADHD Self Report Scale (ASRS) in Hebrew. Isr. J. Psychiatry Relat. Sci. 2010, 47, 308. [Google Scholar]
- Swanson, J.M.; Schuck, S.; Porter, M.M.; Carlson, C.; Hartman, C.A.; Sergeant, J.A.; Clevenger, W.; Wasdell, M.; McCleary, R.; Lakes, K.; et al. Categorical and Dimensional Definitions and Evaluations of Symptoms of ADHD: History of the SNAP and the SWAN Rating Scales. Int. J. Educ. Psychol. Assess. 2012, 10, 51–70. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Brann, P.; Lethbridge, M.J.; Mildred, H. The young adult Strengths and Difficulties Questionnaire (SDQ) in routine clinical practice. Psychiatry Res. 2018, 264, 340–345. [Google Scholar] [CrossRef]
- Arbuckle, J.L. Ibm Spss Amos 21; Amos Development Corporation: Chicago, IL, USA, 2012. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Mittelmark, M.B.; Bull, T.; Daniel, M.; Urke, H. Specific resistance resources in the salutogenic model of health. In The Handbook of Salutogenesis; Springer: Cham, Switzerlan, 2017. [Google Scholar]
- Feldt, T. The role of sense of coherence in well-being at work: Analysis of main and moderator effects. Work Stress 1997, 11, 134–147. [Google Scholar] [CrossRef]
- World Health Organization. How to Use the ICF: A Practical Manual for Using the International Classification of Functioning, Disability and Health (ICF); Exposure draft for comment; WHO: Geneva, Switzerland; Volume 13.
- Davis, L.M. A Study of the Factors Associated with Academic and Vocational Success in Five Women with co-Occurring ADHD and LD; Alliant International University: Alhambra, CA, USA, 2014. [Google Scholar]
- Dvorsky, M.R.; Langberg, J.M. A Review of Factors that Promote Resilience in Youth with ADHD and ADHD Symptoms. Clin. Child Fam. Psychol. Rev. 2016, 19, 368–391. [Google Scholar] [CrossRef] [PubMed]
- Climie, E.A.; Mastoras, S.M. ADHD in schools: Adopting a strengths-based perspective. Can. Psychol. Can. 2015, 56, 295–300. [Google Scholar] [CrossRef]
- Jia, R.M.; Mikami, A.Y.; Normand, S. Social Resilience in Children with ADHD: Parent and Teacher Factors. J. Child Fam. Stud. 2021, 30, 839–854. [Google Scholar] [CrossRef]
- Lee, S.S.; Sibley, M.H.; Epstein, J.N. Attention-deficit/hyperactivity disorder across development: Predictors, resilience, and future directions. J. Abnorm. Psychol. 2016, 125, 151–153. [Google Scholar] [CrossRef]
- Lesch, K.-P. ‘Shine bright like a diamond!’: Is research on high-functioning ADHD at last entering the mainstream? J. Child Psychol. Psychiatry 2017, 59, 191–192. [Google Scholar] [CrossRef] [Green Version]
- Schoenfelder, E.N.; Kollins, S. Topical Review: ADHD and Health-Risk Behaviors: Toward Prevention and Health Promotion. J. Pediatr. Psychol. 2015, 41, 735–740. [Google Scholar] [CrossRef] [Green Version]
- Gudjonsson, G.H.; Gonzalez, R.A.; Young, S. The Risk of Making False Confessions: The Role of Developmental Disorders, Conduct Disorder, Psychiatric Symptoms, and Compliance. J. Atten. Disord. 2019, 25, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Brikell, I.; Kuja-Halkola, R.; Larsson, H. Heritability of attention-deficit hyperactivity disorder in adults. Am. J. Med. Genet. Part B Neuropsychiatr. Genet. 2015, 168, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, B.W.; Wu, R.; Helms, K. Performance of the Adult ADHD Self-Report Scale-v1.1 in Adults with Major Depressive Disorder. Behav. Sci. 2018, 8, 37. [Google Scholar] [CrossRef]
- van de Glind, G.; Brink, W.V.D.; Koeter, M.W.; Carpentier, P.-J.; Oortmerssen, K.V.E.-V.; Kaye, S.; Skutle, A.; Bu, E.-T.H.; Franck, J.; Konstenius, M.; et al. Validity of the Adult ADHD Self-Report Scale (ASRS) as a screener for adult ADHD in treatment seeking substance use disorder patients. Drug Alcohol Depend. 2013, 132, 587–596. [Google Scholar] [CrossRef] [Green Version]
- Cheung, L.; Gunby, P. Crime and mobility during the COVID-19 lockdown: A preliminary empirical exploration. N. Z. Econ. Pap. 2021, 56, 106–113. [Google Scholar] [CrossRef]
- Jensen, J.F.; Egerod, I.; Bestle, M.; Christensen, D.F.; Elklit, A.; Hansen, R.L.; Knudsen, H.; Grode, L.; Overgaard, D. A recovery program to improve quality of life, sense of coherence and psychological health in ICU survivors: A multicenter randomized controlled trial, the RAPIT study. Intensiv. Care Med. 2016, 42, 1733–1743. [Google Scholar] [CrossRef] [PubMed]
- Mayer, C.-H.; Boness, C. Interventions to promoting sense of coherence and transcultural competences in educational contexts. Int. Rev. Psychiatry 2011, 23, 516–524. [Google Scholar] [CrossRef]
- Odajima, Y.; Kawaharada, M.; Wada, N. Development and validation of an educational program to enhance sense of coherence in patients with diabetes mellitus type 2. Nagoya J. Med. Sci. 2017, 79, 363–374. [Google Scholar] [CrossRef]
- Tan, K.K.; Chan, S.W.-C.; Wang, W.; Vehviläinen-Julkunen, K. A salutogenic program to enhance sense of coherence and quality of life for older people in the community: A feasibility randomized controlled trial and process evaluation. Patient Educ. Couns. 2016, 99, 108–116. [Google Scholar] [CrossRef]
- Uzdil, N.; Ceyhan, Ö.; Şimşek, N. The effect of salutogenesis-based care on the sense of coherence in peritoneal dialysis patients. J. Clin. Nurs. 2021, 31, 184–195. [Google Scholar] [CrossRef]
Figure 1.
The association between ADHD symptoms and severe physical antisocial behavior as moderated by coherence.
Figure 1.
The association between ADHD symptoms and severe physical antisocial behavior as moderated by coherence.

Figure 2.
The association between ADHD symptoms and mild physical antisocial behavior as moderated by coherence.
Figure 2.
The association between ADHD symptoms and mild physical antisocial behavior as moderated by coherence.

Figure 3.
The association between ADHD symptoms and verbal antisocial behavior as moderated by coherence.
Figure 3.
The association between ADHD symptoms and verbal antisocial behavior as moderated by coherence.

Figure 4.
The association between ADHD symptoms and property crimes as moderated by coherence.

Figure 5.
The association between ADHD symptoms and public order crimes as moderated by coherence.

Figure 6.
The association between ADHD symptoms and drug use as moderated by coherence.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Descriptive statistics of the demographic characteristics, ADHD, and antisocial behavior types.
Table 1.
Descriptive statistics of the demographic characteristics, ADHD, and antisocial behavior types.
| N | Median | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|---|
| Religiosity | 3165 | 3.00 | 2.76 | 1.44 | 0.00 | 4.00 |
| Emotional symptoms | 2804 | 1.40 | 1.56 | 0.48 | 1.00 | 3.00 |
| ADHD symptoms | 3179 | 1.28 | 1.37 | 0.72 | 0.00 | 4.00 |
| Coherence | 2963 | 4.92 | 4.78 | 1.16 | 1.00 | 7.00 |
| Severe physical antisocial behavior | 3079 | 0.00 | 0.11 | 0.35 | 0.00 | 4.00 |
| Mild physical antisocial behavior | 3079 | 0.00 | 0.24 | 0.52 | 0.00 | 4.00 |
| Verbal antisocial behavior | 3079 | 0.75 | 1.01 | 0.93 | 0.00 | 4.00 |
| Property crimes | 3079 | 0.00 | 0.09 | 0.33 | 0.00 | 4.00 |
| Public order crimes | 3070 | 0.33 | 0.51 | 0.76 | 0.00 | 4.00 |
| Drug use | 2834 | 0.40 | 0.77 | 1.13 | 0.00 | 7.00 |
Table 2.
Nonparametric correlations between ADHD, antisocial behavior types, and coherence.
| ADHD | Severe Physical Antisocial Behavior | Mild Physical Antisocial Behavior | Verbal Antisocial Behavior | Property Crimes | Public Order Crimes | Drug Use | Coherence | |
|---|---|---|---|---|---|---|---|---|
| ADHD symptoms | 1.000 | |||||||
| Severe physical antisocial behavior | 0.175 ** | 1.000 | ||||||
| Mild physical antisocial behavior | 0.207 ** | 0.542 ** | 1.000 | |||||
| Verbal antisocial behavior | 0.234 ** | 0.403 ** | 0.520 ** | 1.000 | ||||
| Property crimes | 0.176 ** | 0.459 ** | 0.418 ** | 0.365 ** | 1.000 | |||
| Public order crimes | 0.246 ** | 0.335 ** | 0.382 ** | 0.464 ** | 0.346 ** | 1.000 | ||
| Drug use | 0.117 ** | 0.130 ** | 0.143 ** | 0.203 ** | 0.186 ** | 0.254 ** | 1.000 | |
| Coherence | −0.424 ** | −0.195 ** | −0.283 ** | −0.363 ** | −0.259 ** | −0.288 ** | −0.086 ** | 1.000 |
**. correlation is significant at the 0.01 level (2-tailed).
Table 3.
ADHD as a predictor of severe physical antisocial behavior moderated by coherence.
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.127 | 0.062 | 0.009 | 6.79 | <0.001 | 0.041 | 0.083 |
| Coherence | −0.190 | −0.057 | 0.007 | −8.51 | <0.001 | −0.077 | −0.043 |
| ADHD symptoms × Coherence | −0.172 | −0.061 | 0.006 | −10.18 | <0.001 | −0.089 | −0.034 |
| Age | −0.159 | −0.143 | 0.015 | −9.48 | <0.001 | −0.191 | −0.102 |
| Gender | −0.094 | −0.066 | 0.012 | −5.58 | <0.001 | −0.089 | −0.039 |
| Religiosity | −0.006 | −0.002 | 0.004 | −0.37 | 0.711 | −0.010 | 0.007 |
| Emotional symptoms | −0.105 | −0.076 | 0.016 | −4.87 | <0.001 | −0.122 | −0.041 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.299 | 0.133 | 0.011 | 12.76 | <0.001 | 0.113 | 0.154 |
| High coherence | −0.045 | −0.009 | 0.012 | −0.68 | 0.491 | −0.033 | 0.016 |
Table 4.
ADHD symptoms as a predictor of mild physical antisocial behavior moderated by coherence.
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.102 | 0.074 | 0.013 | 5.57 | <0.001 | 0.049 | 0.103 |
| Coherence | −0.311 | −0.138 | 0.010 | −14.28 | <0.001 | −0.171 | −0.117 |
| ADHD symptoms × Coherence | −0.135 | −0.070 | 0.009 | −8.17 | <0.001 | −0.098 | −0.044 |
| Age | −0.186 | −0.247 | 0.022 | −11.34 | <0.001 | −0.311 | −0.183 |
| Gender | −0.099 | −0.103 | 0.017 | −6.00 | <0.001 | −0.139 | −0.073 |
| Religiosity | 0.056 | 0.020 | 0.006 | 3.35 | <0.001 | 0.011 | 0.038 |
| Emotional symptoms | −0.109 | −0.116 | 0.022 | −5.19 | <0.001 | −0.171 | −0.069 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.237 | 0.156 | 0.015 | 10.35 | <0.001 | 0.126 | 0.185 |
| High coherence | −0.033 | −0.008 | 0.018 | −0.46 | 0.643 | −0.044 | 0.027 |
Table 5.
ADHD symptoms as a predictor of verbal antisocial behavior moderated by coherence.
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.098 | 0.128 | 0.023 | 5.46 | <0.001 | 0.088 | 0.168 |
| Coherence | −0.371 | −0.297 | 0.017 | −17.31 | <0.001 | −0.334 | −0.264 |
| ADHD symptoms × Coherence | −0.059 | −0.055 | 0.015 | −3.65 | <0.001 | −0.088 | −0.029 |
| Age | −0.159 | −0.380 | 0.038 | −9.89 | <0.001 | −0.468 | −0.278 |
| Gender | −0.113 | −0.211 | 0.030 | −6.97 | <0.001 | −0.285 | −0.156 |
| Religiosity | −0.051 | −0.033 | 0.011 | −3.11 | 0.002 | −0.053 | −0.014 |
| Emotional symptoms | −0.108 | −0.207 | 0.040 | −5.23 | <0.001 | −0.296 | −0.127 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.157 | 0.19 | 0.027 | 7.23 | <0.001 | 0.140 | 0.245 |
| High coherence | 0.039 | 0.63 | 0.032 | 1.97 | 0.048 | 0.001 | 0.126 |
Table 6.
ADHD as a predictor of property crimes moderated by coherence.
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.063 | 0.029 | 0.009 | 3.29 | 0.001 | 0.001 | 0.046 |
| Coherence | −0.190 | −0.053 | 0.006 | −8.34 | <0.001 | −0.069 | −0.040 |
| ADHD symptoms × Coherence | −0.135 | −0.044 | 0.006 | −7.78 | <0.001 | −0.079 | −0.022 |
| Age | −0.109 | −0.091 | 0.014 | −6.34 | <0.001 | −0.134 | −0.049 |
| Gender | −0.112 | −0.073 | 0.011 | −6.50 | <0.001 | −0.104 | −0.049 |
| Religiosity | −0.081 | −0.018 | 0.004 | −4.62 | <0.001 | −0.027 | −0.009 |
| Emotional symptoms | −0.065 | −0.043 | 0.015 | −2.94 | 0.003 | −0.073 | −0.016 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.198 | 0.080 | 0.010 | 8.08 | <0.001 | 0.061 | 0.099 |
| High coherence | −0.072 | −0.023 | 0.012 | −1.91 | 0.055 | −0.046 | 0.001 |
Table 7.
ADHD symptoms as a predictor of public order antisocial behavior moderated by coherence.
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.166 | 0.176 | 0.019 | 9.09 | <0.001 | 0.135 | 0.212 |
| Coherence | −0.279 | −0.182 | 0.014 | −12.84 | <0.001 | −0.213 | −0.145 |
| ADHD symptoms × Coherence | −0.099 | −0.075 | 0.013 | −5.99 | <0.001 | −0.104 | −0.046 |
| Age | −0.164 | −0.319 | 0.032 | −10.05 | <0.001 | −0.404 | −0.251 |
| Gender | −0.072 | −0.110 | 0.025 | −4.41 | <0.001 | −0.159 | −0.064 |
| Religiosity | −0.096 | −0.051 | 0.009 | −5.75 | <0.001 | −0.070 | −0.033 |
| Emotional symptoms | −0.154 | −0.241 | 0.033 | −7.36 | <0.001 | −0.304 | −0.174 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.265 | 0.264 | 0.022 | 11.99 | <0.001 | 0.221 | 0.307 |
| High coherence | 0.067 | 0.088 | 0.026 | 3.33 | <0.001 | 0.036 | 0.139 |
Table 8.
ADHD symptoms as a predictor of drug use moderated by coherence.
| Beta | B | S.E. | t | P | 95%CI | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| ADHD symptoms | 0.075 | 0.119 | 0.029 | 4.09 | <0.001 | 0.070 | 0.188 |
| Coherence | −0.122 | −0.118 | 0.021 | −5.55 | <0.001 | −0.165 | −0.074 |
| ADHD symptoms × Coherence | −0.062 | −0.071 | 0.019 | −3.73 | <0.001 | −0.118 | −0.023 |
| Age | 0.092 | 0.267 | 0.048 | 5.59 | <0.001 | 0.166 | 0.386 |
| Gender | −0.323 | −0.732 | 0.038 | −19.43 | <0.001 | −0.814 | −0.656 |
| Religiosity | −0.235 | −0.185 | 0.013 | −13.96 | <0.001 | −0.216 | −0.156 |
| Emotional symptoms | −0.067 | −0.156 | 0.049 | −3.17 | 0.002 | −0.261 | −0.060 |
| Conditional effects of ADHD symptoms | |||||||
| Low coherence | 0.137 | 0.201 | 0.033 | 6.08 | <0.001 | 0.137 | 0.266 |
| High coherence | 0.013 | 0.036 | 0.040 | 0.92 | 0.355 | −0.041 | 0.115 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Dayan, H.; Khoury-Kassabri, M.; Pollak, Y. The Link between ADHD Symptoms and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence. Brain Sci. 2022, 12, 1336. https://doi.org/10.3390/brainsci12101336
AMA Style
Dayan H, Khoury-Kassabri M, Pollak Y. The Link between ADHD Symptoms and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence. Brain Sciences. 2022; 12(10):1336. https://doi.org/10.3390/brainsci12101336
Chicago/Turabian StyleDayan, Haym, Mona Khoury-Kassabri, and Yehuda Pollak. 2022. "The Link between ADHD Symptoms and Antisocial Behavior: The Moderating Role of the Protective Factor Sense of Coherence" Brain Sciences 12, no. 10: 1336. https://doi.org/10.3390/brainsci12101336
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.