Neuroimaging of Basal Ganglia in Neurometabolic Diseases in Children

 ,
,  ,
,
Abstract
:1. Introduction
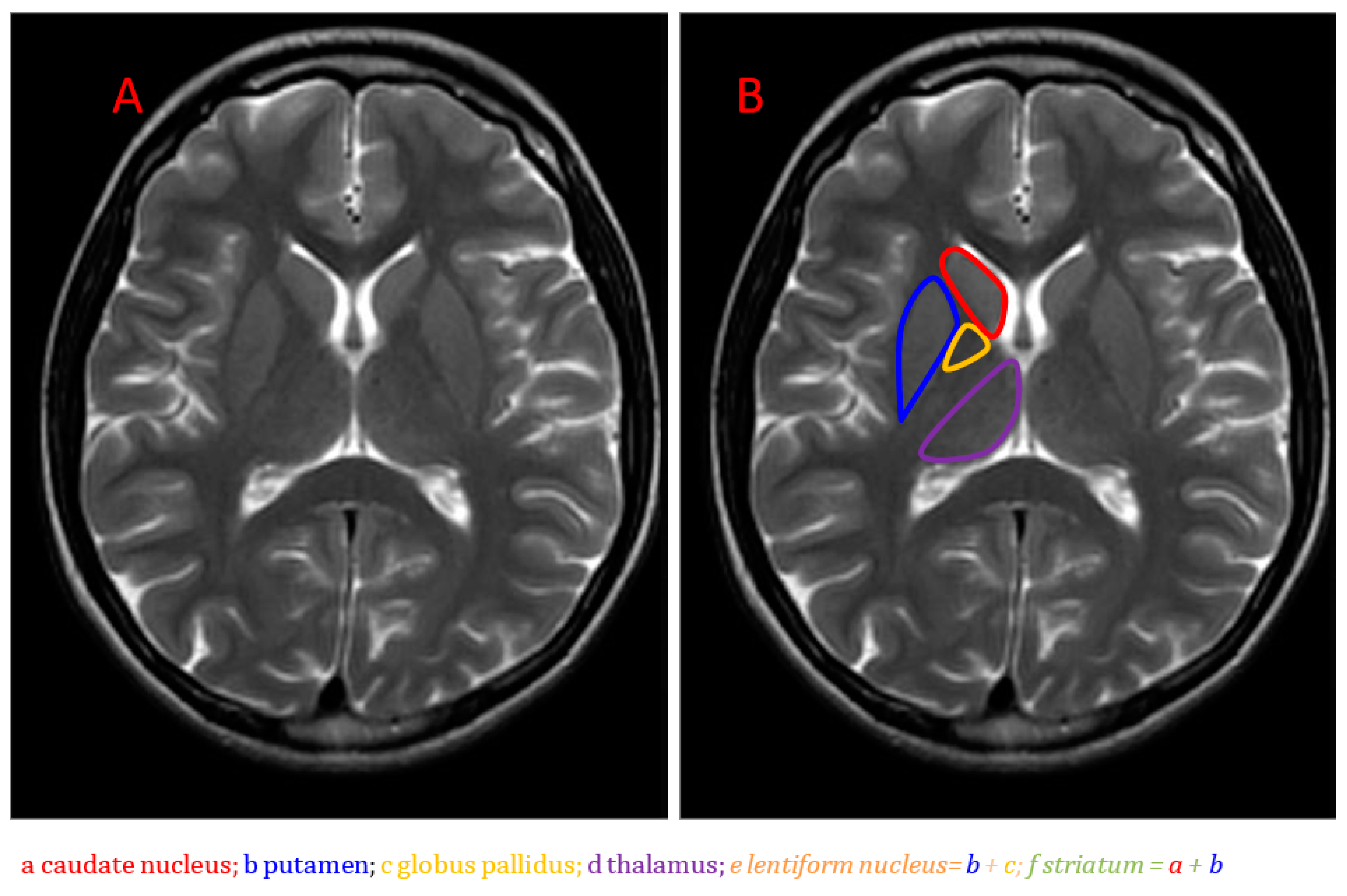
2. MRI Abnormalities of the Basal Ganglia Depending on the Anatomical Localization
2.1. Globus Pallidus
- succinic semialdehyde dehydrogenase (SSADH);
- methylmalonic acidemia;
- isovaleric acidemia;
- pyruvate dehydrogenase deficiency (due to mutation in the dihydrolipoamide acetyltransferase gene and in the E2 component);
- guanidinoacetate methyltransferase (GAMT) deficiency;
- carbon monoxide poisoning;
- normal T2 signal intensity indicates chronic hepatic disease;
2.2. Caudate and Putamen (Striatum)
- mitochondrial disorders (Leigh syndrome, mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS);
- glutaric aciduria;
- propionic acidemia;
- Wilson disease;
- juvenile Huntington disease;
- molybdenum cofactor deficiency;
- isolated sulfite oxidase deficiency;
- hypoxic-ischemic injury;
- hypoglycemia;
- glutaric aciduria type 1 with striatal hyperintensity is associated with enlarged subarachnoid spaces, particularly in the anterior Sylvian fissures, and hyperintense signal changes on T2-WI (suspicion of delayed maturation) in the thalamus, substantia nigra, nucleus dentatus, the central tegmental tract and the supratentorial white matter;
- isolated sulfite oxidase deficiency causes rapidly progressive multicystic encephalomalacia of the cerebral white matter;
- striatum calcification in Cockayne disease;
2.3. Thalamus
- mitochondrial disorders typically with putaminal changes;
- Wilson disease with putaminal involvement;
- Canavan disease with globus pallidus abnormalities;
- nonmetabolic diseases often involving the thalamus (profound neonatal asphyxia with the damage to the ventrolateral thalamus, posterior putamen and the perirolandic cortex);
- acute necrotizing encephalopathy (ANE) with hyperintensity in the thalamus and dorsal brainstem on T2-WI [10].
3. Basal Ganglia MRI Involvement Depending on the Disease
4. Neurometabolic Disorders
4.1. Mitochondrial Disorders
4.2. Neurodegeneration with Brain Iron Accumulation (NBIA)
4.3. Biotin-Thiamine-Responsive Basal Ganglia Disease (BTBGD)
4.4. Pyruvate Dehydrogenase Deficiency (PDHD)
4.5. Glutaric Aciduria (GA) Type 1
4.6. Gangliosidosis (GM1 and GM2)
- in GM1, hyperintensities of posterior putamen and globi pallidi on T1-WI with susceptibility effects on T2-WI were found;
- in GM2, thalamic hyperintensity on T1-WI, mixed striatum signal intensity on T2-WI, hypointense white matter on T2-WI (Tay–Sachs syndrome: hypointense on T2-WI (ventral thalamus) hyperintense on T2-WI (dorsal thalamus); Sandhoff disease: T2 hypointense thalami).
4.7. Wilson Disease
4.8. In Methylmalonic Aciduria (MMA)
4.9. Fabry Disease
4.10. Canavan Disease (CD)
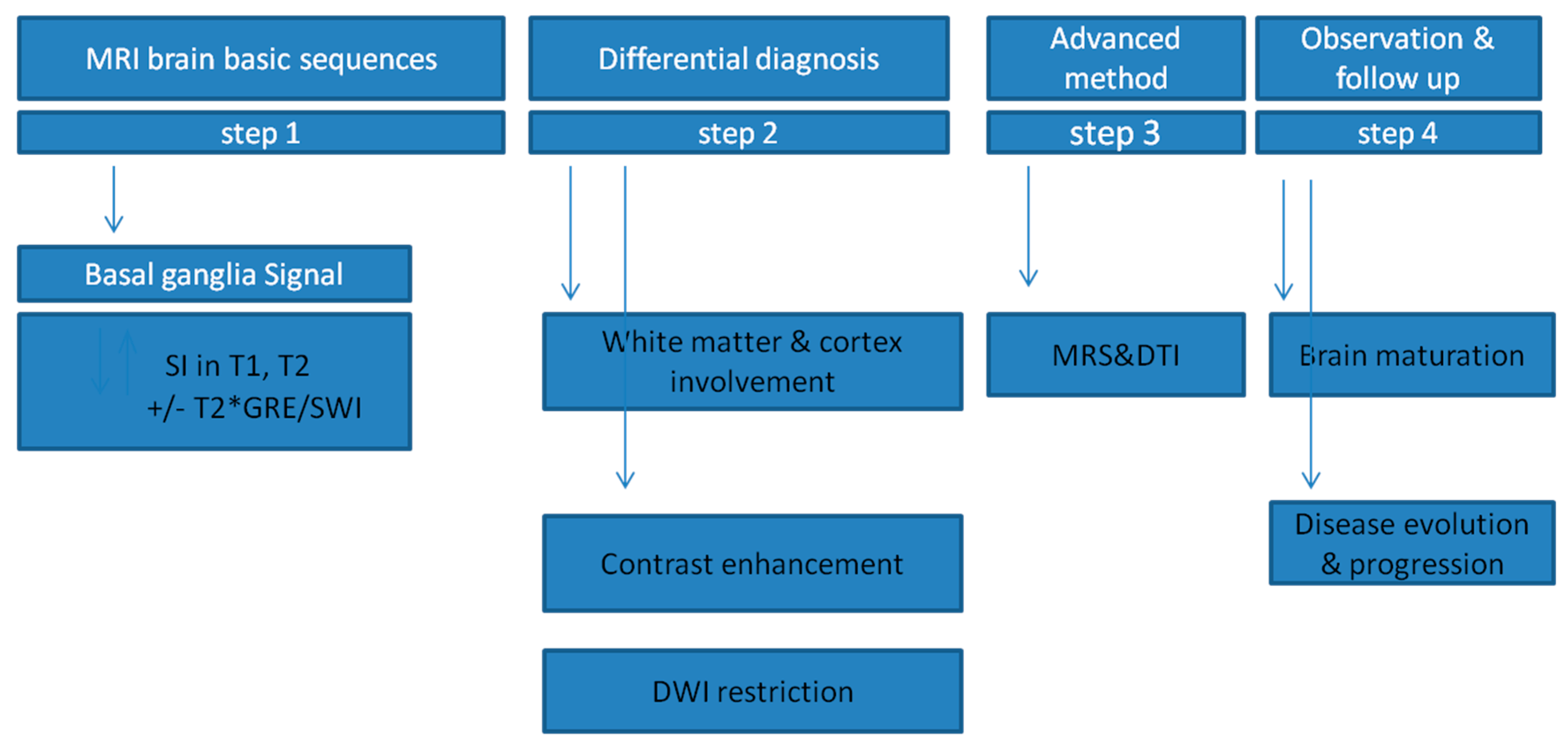
5. Differential Diagnosis
- chromosomal abnormalities: SLC20A2 8p11.21 PDGFRB 5q32 PDGFB 22q13.1 XPR1 1q25.3 MYORG 9p13.3;
- primary or secondary forms of the following: hypoparathyroidism, secondary hypoparathyroidism, infections (brucellosis, AIDS, toxoplasmosis, TORCH complex), autoimmune diseases (SLE);
- other conditions such as pseudohypoparathyroidism, Cockayne syndrome I and II, Aicardi–Goutières syndrome, mitochondrial diseases (MELAS, MERRF), Coats’ syndrome, toxic exposure to carbon monoxide, lead or other metals, neuroferritinopathy and NBIA.
- Step 1
- Step 2
- Step 3
- Step 4
6. Summary
Author Contributions
Funding
Conflicts of Interest
References
- Anderson, J.C.; Costantino, M.M.; Stratford, T. Basal ganglia: Anatomy, pathology, and imaging characteristics. Curr. Probl. Diagn. Radiol. 2004, 33, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Seger, C.A. How do the basal ganglia contribute to categorization? Their role in generalization, response selection, and learning via feedback. Neurosci. Biobehav. Rev. 2008, 32, 265–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shohamy, D.; Myers, C.E.; Kalanithi, J.; Gluck, M.A. Basal ganglia and Dopamine Contributions to Probabilistic Category Learning. Neurosci. Biobehav. Rev. 2008, 32, 219–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riva, D.; Taddei, M.; Bulgheroni, S. The neuropsychology of basal ganglia. Eur. J. Paediatr. Neurol. 2018, 22, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Mink, J.W. Basal ganglia mechanisms in action selection, plasticity and dystonia. Eur. J. Pediatr. Neurol. 2018, 22, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Beudel, M.; Macerollo, A.; Brown, M.; Chen, R. The role of the basal ganglia in somatosensory-motor interactions: Evidence from neurophysiology and behaviour. Front. Hum. Neurosci. 2020, 13, 451. [Google Scholar] [CrossRef] [PubMed]
- Zuccoli, G.; Yannes, M.P.; Nardone, R.; Bailey, A.; Goldstein, A. Bilateral symmetrical basal ganglia and thalamic lesions in children: An update. Neuroradiology 2015, 57, 973–989. [Google Scholar] [CrossRef]
- Hegde, A.N.; Mohan, S.; Lath, N.; Tchoyoson, L. Differential Diagnosis for Bilateral Abnormalities of the Basal Ganglia and Thalamus. RadioGraphics 2011, 31, 5–30. [Google Scholar] [CrossRef]
- Pols, T.; de Vries, L.S.; Salamon, A.S.; Nikkels, P.G.J.; Lichtenbelt, K.D.; Mulder-de Tollenaer, S.M.; van Wezel-Meijler, G. Symmetrical Thalamic Lesions in the Newborn: A Case Series. Neuropediatrics 2019, 50, 152–159. [Google Scholar] [CrossRef] [Green Version]
- Saudubray, J.-M.; Cazorla, A.G. Specific Neurosensorial, Neurophysiological and Neuroradiological Signs and Symptoms (at any Age). In Inborn Metabolic Diseases, Diagnosis and Treatment, 6th ed.; Saudubray, J.-M., Baumgartner, M.R., Walter, J., Eds.; Springer: Berlin, Germany, 2016; pp. 45–52. [Google Scholar]
- Baertling, F.; Klee, D.; Haack, T.B.; Prokisch, H.; Meitinger, T.; Mayatepek, E.; Schaper, J.; Distelmaier, F. The many faces of paediatric mitochondrial disease on neuroimaging. Childs Nerv. Syst. 2016, 32, 2077–2083. [Google Scholar] [CrossRef]
- Jde Beaurepaire, I.; Grévent, D.; Rio, M.; Desguerre, I.; de Lonlay, P.; Levy, R.; Dangouloff-Ros, V.; Bonnefont, J.P.; Barcia, G.; Funalot, B.; et al. High predictive value of brain MRI imaging in primary mitochondrial respiratory chain deficiency. Med. Genet. 2018, 55, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Martikainen, M.H.; Ng, Y.S.; Gorman, G.S.; Alston, C.L.; Blakely, E.L.; Schaefer, A.M.; Chinnery, P.F.; Burn, D.J.; Taylor, R.W.; McFarland, R.; et al. Clinical, Genetic, and Radiological Features of Extrapyramidal Movement Disorders in Mitochondrial Disease. JAMA Neurol. 2016, 73, 668–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraser, J.L.; Venditti, C.P. Methylmalonic and propionic acidemias: Clinical management update. Curr. Opin. Pediatr. 2016, 28, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Almuqbil, M.; Chinsky, J.M.; Srivastava, S. Metabolic strokes in propionic acidemia: Transient hemiplegic events without encephalopathy. Child Neurol. Open 2019, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hogarth, P. Neurodegeneration with brain iron accumulation: Diagnosis and management. J. Mov. Disord. 2015, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.A. Neurodegeneration with brain iron accumulation. Curr. Neurol Neurosci. Rep. 2016, 16, 9. [Google Scholar] [CrossRef] [PubMed]
- Salomão, R.P.; Pedroso, J.L.; Gama, M.T.; Dutra, L.A.; Maciel, R.H.; Godeiro-Junior, C.; Chien, H.F.; Teive, H.A.; Cardoso, F.; Barsottini, O.G. A diagnostic approach for neurodegeneration with brain iron accumulation: Clinical features, genetics and brain imaging. Arq. Neuropsiquiatr. 2016, 74, 587–596. [Google Scholar] [CrossRef] [Green Version]
- Alfadhel, M.; Almuntashri, M.; Jadah, R.H.; Bashiri, F.A.; Al Rifai, M.T.; Al Shalaan, H.; Al Balwi, M.; Al Rumayan, A.; Eyaid, W.; Al-Twaijri, W. Biotin-responsive basal ganglia disease should be renamed biotin-thiamine-responsive basal ganglia disease: A retrospective review of the clinical, radiological and molecular findings of 18 new cases. Orphanet. J. Rare. Dis. 2013, 8, 83. [Google Scholar] [CrossRef] [Green Version]
- Kassem, H.; Wafaie, A.; Alsuhibani, S.; Farid, T. Biotin-responsive basal ganglia disease: Neuroimaging features before and after treatment. AJNR 2014, 35, 1990–1995. [Google Scholar] [CrossRef] [Green Version]
- Kamaşak, T.; Havalı, C.; İnce, H.; Eyüboğlu, İ.; Çebi, A.H.; Sahin, S.; Cansu, A.; Aydin, K. Are diagnostic magnetic resonance patterns life-saving in children with biotin-thiamine-responsive basal ganglia disease? Eur. J. Paediatr. Neurol. 2018, 22, 1139–1149. [Google Scholar] [CrossRef]
- Algahtani, H.; Ghamdi, S.; Shirah, B.; Alharbi, B.; Algahtani, R.; Bazaid, A. Biotin-thiamine-responsive basal ganglia disease: Catastrophic consequences of delay in diagnosis and treatment. Neurol. Res. 2017, 39, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.P.; O’Brien, T.W.; Subramony, S.H.; Shuster, J.; Stacpoole, P.W. The spectrum of pyruvate dehydrogenase complex deficiency: Clinical, biochemical and genetic features in 371 patients. Mol. Genet. Metab. 2012, 105, 34–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harting, I.; Neumaier-Probst, E.; Seitz, A.; Maier, E.M.; Assmann, B.; Baric, I.; Troncoso, M.; Mühlhausen, C.; Zschocke, J.; Boy, N.P.; et al. Dynamic changes of striatal and extrastriatal abnormalities in glutaric aciduria type I. Brain 2009, 132, 1764–1782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boy, N.; Mühlhausen, C.; Maier, E.M.; Heringer, J.; Assmann, B.; Burgard, P.; Dixon, M.; Fleissner, S.; Greenberg, C.R.; Harting, I.; et al. Proposed recommendations for diagnosing and managing individuals with glutaric aciduria type I: Second revision. Additional individual contributors. J. Inherit. Metab. Dis. 2017, 40, 75–101. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, S.A.; Abdelkhalek, H.S.; Ahmed, K.A.; Zaki, O.K. Glutaric aciduria type 1: Neuroimaging features with clinical correlation. Pediatr. Radiol. 2015, 45, 1696–1705. [Google Scholar] [CrossRef]
- Renaud, D.; Brodsky, M. GM2-Gangliosidosis, AB Variant: Clinical, Ophthalmological, MRI, and Molecular Findings. JIMD Rep. 2016, 25, 83–86. [Google Scholar]
- Yu, X.E.; Gao, S.; Yang, R.M.; Han, Y.Z. MR Imaging of the Brain in Neurologic Wilson Disease. AJNR 2019, 40, 178–183. [Google Scholar] [CrossRef]
- Członkowska, A.; Litwin, T.; Chabik, G. Wilson disease: Neurologic features. Handb. Clin. Neurol. 2017, 142, 101–119. [Google Scholar]
- De Benedictis, F.M.; de Benedictis, D. The value of neuroimaging in the assessment and follow-up of early-onset methylmalonic aciduria and homocystinuria. Mol. Genet. Metab. Rep. 2014, 1, 60. [Google Scholar] [CrossRef]
- Cocozza, S.; Russo, C.; Pontillo, G.; Pisani, A.; Brunetti, A. Neuroimaging in Fabry disease: Current knowledge and future directions. Insights Imaging. 2018, 9, 1077–1088. [Google Scholar] [CrossRef] [Green Version]
- Israni, A.V.; Mandal, A. Canavan disease with typical brain MRI and MRS findings. Neurol. India. 2017, 65, 1191–1192. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, M.; Di Marzo, G.; Chiarotti, F.; Andreoli, C.; Colajacomo, M.C.; Ruggieri, A.; Papoff, P. Early Post-cooling Brain Magnetic Resonance for the Prediction of Neurodevelopmental Outcome in Newborns with Hypoxic-Ischemic Encephalopathy. J. Pediatr. Neurosci. 2019, 14, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; de Vries, L.S.; Alderliesten, T.; Wagenaar, N.; van der Aa, N.E.; Lequin, M.H.; Benders, M.J.N.L.; van Haastert, I.C.; Groenendaal, F. MRI Changes in the Thalamus and Basal Ganglia of Full-Term Neonates with Perinatal Asphyxia. Neonatology 2018, 114, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Rennie, J.; Rosenbloom, L. How long have we got to get the baby out? A review of the effects of acute and profound intrapartum hypoxia and ischaemia. Obstet. Gynaecol. 2011, 13, 169–174. [Google Scholar] [CrossRef]
- Baxter, P. Markers of perinatal hypoxia-ischaemia and neurological injury: Assessing the impact of insult duration. Dev. Med. Child. Neurol. 2019, 62, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Salido-Vallejo, R.; Ruano, J.; Garnacho-Saucedo, G.; Godoy-Gijón, E.; Llorca, D.; Gómez-Fernández, C.; Moreno-Giménez, J.C. Facial Angiofibroma Severity Index (FASI): Reliability assessment of a new tool developed to measure severity and responsiveness to therapy in tuberous sclerosis-associated facial angiofibroma. Clin. Exp. Dermatol. 2014, 39, 888–893. [Google Scholar] [CrossRef]
- Safadi, M.A.; Berezin, E.N.; Farhat, C.K.; Carvalho, E.S. Clinical presentation and follow up of children with congenital toxoplasmosis in Brazil. Braz. J. Infect. Dis. 2003, 7, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Giannattasio, A.; Bruzzese, D.; Di Costanzo, P.; Capone, E.; Romano, A.; D’Amico, A.; Bravaccio, C.; Grande, C.; Capasso, L.; Raimondi, F. Neuroimaging Profiles and Neurodevelopmental Outcome in Infants With Congenital Cytomegalovirus Infection. Pediatr. Infect. Dis. J. 2018, 37, 1028–1033. [Google Scholar] [CrossRef]
- Salel, M.; Tanchoux, F.; Viguier, A.; Cognard, C.; Larrue, V.; Bonneville, F. Reversible bilateral basal ganglia lesions related to Epstein-Barr virus encephalitis. J. Neuroradiol. 2013, 40, 370–372. [Google Scholar]
- Al-Ansari, A.; Robertson, N.P. Autoimmune encephalitis: Frequency and prognosis. J. Neurol. 2019, 266, 1287–1289. [Google Scholar] [CrossRef] [Green Version]
- Pohl, D.; Alper, G.; Van Haren, K.; Kornberg, A.J.; Lucchinetti, C.F.; Tenembaum, S.; Belman, A.L. Acute disseminated encephalomyelitis: Updates on an inflammatory CNS syndrome. Neurology 2016, 87 (Suppl. 2), S38–S45. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Wu, W.; Pan, W.; Wu, L.; Liu, K.; Zhang, H.L. Acute necrotizing encephalopathy: An underrecognized clinicoradiologic disorder. Mediators Inflamm. 2015, 2015, 792578. [Google Scholar] [CrossRef]
- Ekici, A.; Yakut, A.; Yimenicioglu, S.; Bora Carman, K.; Saylısoy, S. Clinical and Neuroimaging Findings of Sydenham’s Chorea. Iran. J. Pediatr. 2014, 24, 300–306. [Google Scholar] [PubMed]
- Aravamuthan, B.R.; Waugh, J.L. Localisation of basal ganglia and thalamic damage in dyskinetic cerebral palsy. Pediatr Neur 2016, 54, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Monbaliu, E.; Himmelmann, K.; Lin, J.P.; Ortibus, E.; Bonouvrié, L.; Feys, H.; Vermeulen, R.J.; Dan, B. Clinical presentation and management of dyskinetic cerebral palsy. Lancet. Neurol. 2017, 16, 741–749. [Google Scholar] [CrossRef]
- Préel, M.; Rackauskaite, G.; Larsen, M.L.; Laursen, B.; Lorentzen, J.; Born, A.P.; Langhoff-Roos, J.; Uldall, P.; Hoei-Hansen, C.E. Children with dyskinetic cerebral palsy are severely affected as compared to bilateral spastic cerebral palsy. Acta Pediatr. 2019, 108, 1850–1856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozcan, N.; Ozcam, G.; Kosar, P.; Ozcan, A.; Basar, H.; Kaymak, C. Correlation of computed tomography, magnetic resonance imaging and clinical outcome in acute carbon monoxide poisoning. Braz. J. Anesthesiol. 2016, 66, 529–532. [Google Scholar] [CrossRef] [Green Version]
- Prockop, L.D.; Chichkova, R.I. Carbon monoxide intoxication: An updated review. J. Neurosci. Sci. 2007, 262, 122–130. [Google Scholar] [CrossRef]
- Marcucci, G.; Cianferotti, L.; Brandi, M.L. Clinical presentation and management of hypoparathyroidism. Best. Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 927–939. [Google Scholar] [CrossRef]
- Albajara Sáenz, A.; Villemonteix, T.; Massat, I. Structural and functional neuroimaging in attention-deficit/hyperactivity disorder. Dev. Med. Child. Neurol. 2019, 61, 399–405. [Google Scholar] [CrossRef] [Green Version]
- Qiu, A.; Crocetti, D.; Adler, M.; Mahone, M.; Denckla Miller, M.I.; Mostofsky, S.H. Basal Ganglia Volume and Shape in Children With Attention Deficit Hyperactivity Disorder. Am. J. Psychiatry 2009, 166, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, K.; Brandenburg, C.; Orsati, F.; Soghomonian, J.J.; Hussman, J.P.; Blatt, G.J. Basal ganglia and autism—A translational perspective. Autism. Res. 2017, 10, 1751–1775. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, Y.; Kagitani-Shimono, K.; Jung, M.; Makita, K.; Takiguchi, S.; Fujisawa, T.X.; Tachibana, M.; Nakanishi, M.; Mohri, I.; Taniike, M. Tomoda. Structural brain abnormalities in children and adolescents with comorbid autism spectrum disorder and attention-deficit/hyperactivity disorder. Transl. Psychiatry 2019, 9, 332. [Google Scholar] [CrossRef] [PubMed]
- Tonduti, D.; Panteghini, C.; Pichiecchio, A.; Decio, A.; Carecchio, M.; Reale, C.; Moroni, I.; Nardocci, N.; Campistol, J.; Garcia-Cazorla, A.; et al. Encephalopathies with intracranial calcification in children: Clinical and genetic characterization. Orphanet. J. Rare Dis. 2018, 1, 135. [Google Scholar] [CrossRef]
- Donzuso, G.; Mostile, G.; Nicoletti, A.; Zappia, M. Basal ganglia calcifications (Fahr’s syndrome): Related conditions and clinical features. Neurol. Sci. 2019, 40, 2251–2263. [Google Scholar] [CrossRef] [Green Version]
- Halefoglu, A.M.; Yousem, D.M. Susceptibility weighted imaging: Clinical applications and future directions. World J. Radiol. 2018, 10, 30–45. [Google Scholar] [CrossRef]
- Hodges, K.; Brewer, S.S.; Labbé, C.; Soto-Ortolaza, A.I.; Walton, R.L.; Strongosky, A.J.; Uitti, R.J.; van Gerpen, J.A.; Ertekin-Taner, N.; Kantarci, K.; et al. RAB39B gene mutations are not a common cause of Parkinson’s disease or dementia with Lewy bodies. Neurobiol. Aging. 2016, 45, 107–108. [Google Scholar] [CrossRef] [Green Version]
- Hussain, S.A.; Tsao, J.; Li, M.; Schwarz, M.D.; Zhou, R.; Wu, J.Y.; Salamon, N.; Sankar, R. Risk of vigabatrin-associated brain abnormalities on MRI in the treatment of infantile spasms is dose-dependent. Epilepsia 2017, 58, 674–682. [Google Scholar] [CrossRef]
- Aschner, J.L.; Anderson, A.; Slaughter, J.C.; Aschner, M.; Steele, S.; Beller, A.; Mouvery, A.; Furlong, H.M.; Maitre, N.L. Neuroimaging identifies increased manganese deposition in infants receiving parenteral nutrition. Am. J. Clin. Nutr. 2015, 102, 1482–1489. [Google Scholar] [CrossRef] [Green Version]
- Shrot, S.; Poretti, A.; Tucker, E.W.; Soares, B.P.; Huisman, T.A. Acute brain injury following illicit drug abuse in adolescent and young adult patients: Spectrum of neuroimaging findings. Neuroradiol. J. 2017, 30, 144–150. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Basal Ganglia MRI Signal Intensity | Disease |
|---|---|
| T2 hyper = increased signal on T2-WI | Hypoxic-ischemic encephalopathy (early) CO toxicity Kernicterus Mitochondrial diseases (e.g., Leigh disease) Infantile bilateral striatal necrosis Hypoglycemia Infarction Rasmussen encephalitis NF1 Myelinolysis Intoxications |
| T2 hypo = decreased signal on T2-WI | (acute) Deoxyhemoglobin Hypoxia |
| T1 hyper = increased signal on T1-WI | Gadolinium concentration after chelate administration Hypoxic-ischemic encephalopathy (late) CO toxicity NF1 Manganese toxicity (subacute) Methemoglobin Liver failure |
| T1 hypo = decreased signal on T1-WI | Infarction Infantile bilateral striatal necrosis |
| DWI restriction = increased signal on DWI with corresponding decreased signal on apparent diffusion coefficient (ADC) maps | Infarction Hypoxic-ischemic encephalopathy CO toxicity Mitochondrial diseases Encephalitis of different origin Wilson disease |
| Disease | Thalamus | Pallidum | Putamen |
|---|---|---|---|
| Respiratory chain disorders | + | + | + |
| Biotin-thiamine-responsive basal ganglia disease | + | ||
| Pyruvate dehydrogenase deficiency | + | + | + |
| Coenzyme Q10 deficiency | + | ||
| Mitochondrial thiamine pyrophosphate transporter | + | ||
| Cerebrotendinous xanthomatosis | + | ||
| Alpha-methylacyl-CoA racemase deficiency | + | ||
| GM1 gangliosidosis | + | ||
| Fabry disease | + | ||
| Methylmalonic aciduria | + | ||
| Succinic semialdehyde dehydrogenase deficiency | + | ||
| Urea cycle disorders | + | ||
| Glutaric aciduria type 1 | + | ||
| Wilson disease | + | + | + |
| Aceruloplasminemia | + | + | + |
| Neuroferritinopathy | + | + | |
| Pantothenate kinase-associated neurodegeneration | + | ||
| Infantile neuroaxonal dystrophy | + | ||
| Hypermanganemia | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paprocka, J.; Machnikowska-Sokołowska, M.; Gruszczyńska, K.; Emich-Widera, E. Neuroimaging of Basal Ganglia in Neurometabolic Diseases in Children. Brain Sci. 2020, 10, 849. https://doi.org/10.3390/brainsci10110849
Paprocka J, Machnikowska-Sokołowska M, Gruszczyńska K, Emich-Widera E. Neuroimaging of Basal Ganglia in Neurometabolic Diseases in Children. Brain Sciences. 2020; 10(11):849. https://doi.org/10.3390/brainsci10110849
Chicago/Turabian StylePaprocka, Justyna, Magdalena Machnikowska-Sokołowska, Katarzyna Gruszczyńska, and Ewa Emich-Widera. 2020. "Neuroimaging of Basal Ganglia in Neurometabolic Diseases in Children" Brain Sciences 10, no. 11: 849. https://doi.org/10.3390/brainsci10110849