


The Effect of Airflow Velocity through a Laminar Airflow Ceiling (LAFC) on the Assessment of Thermal Comfort in the Operating Room

Abstract
:1. Introduction
2. Materials and Methods
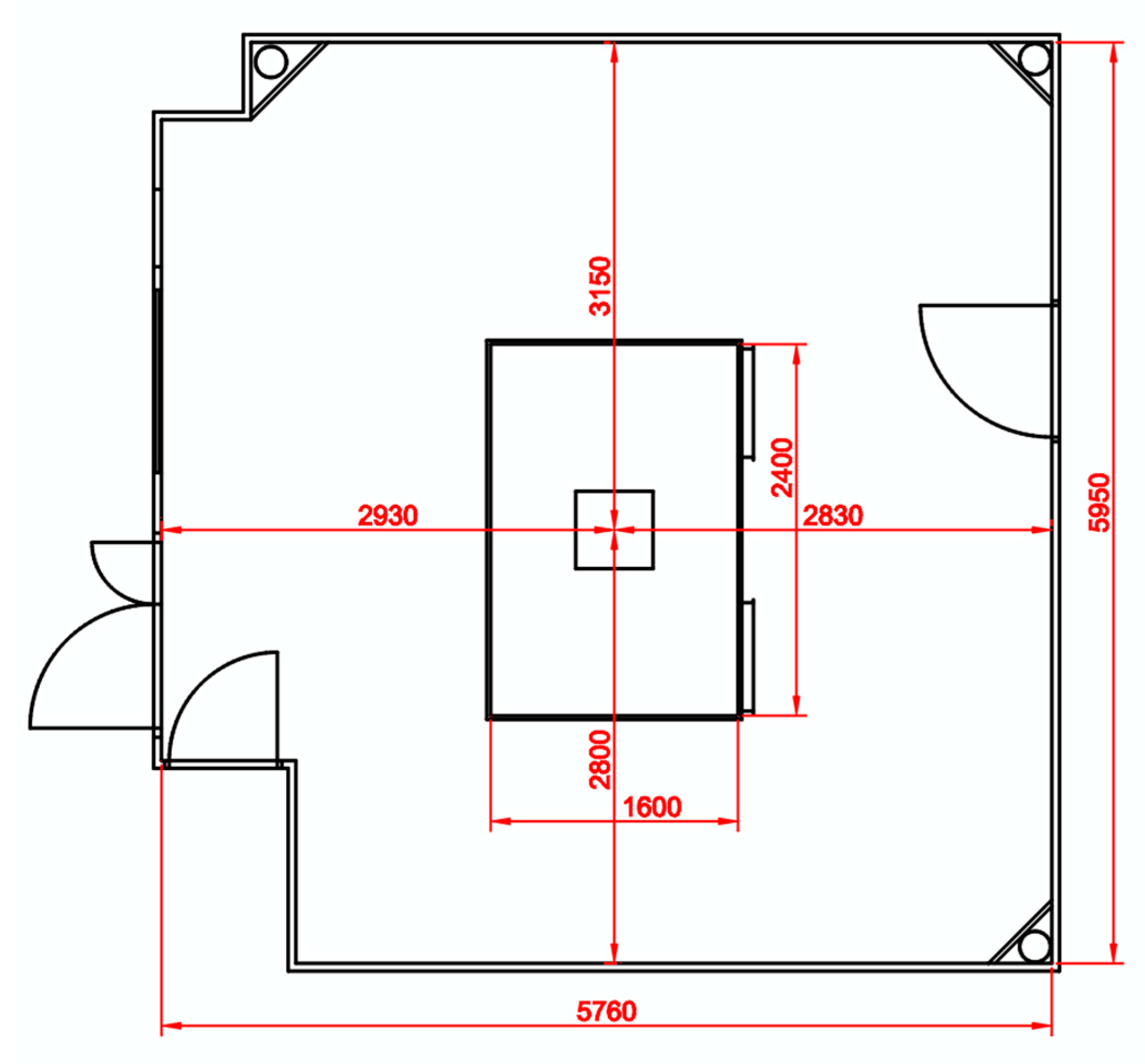
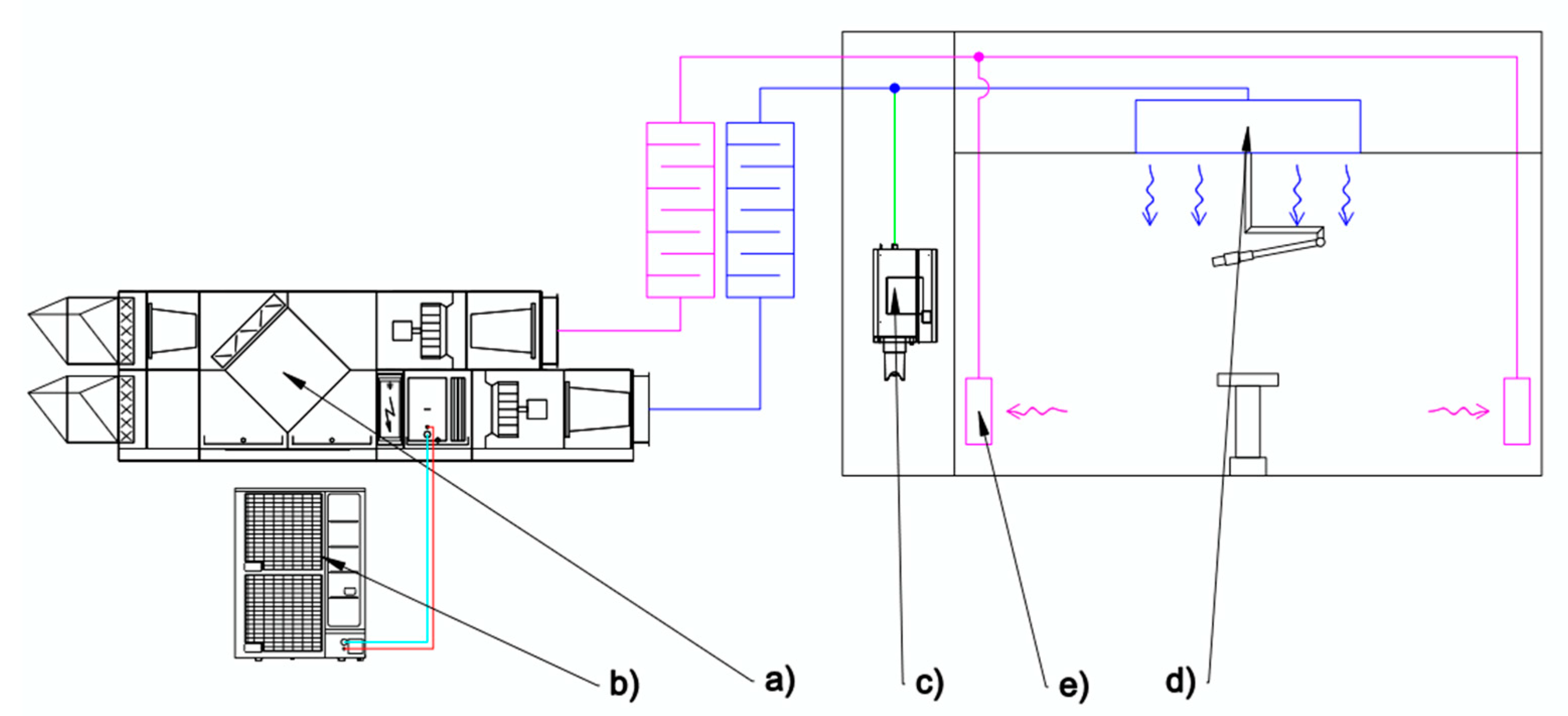
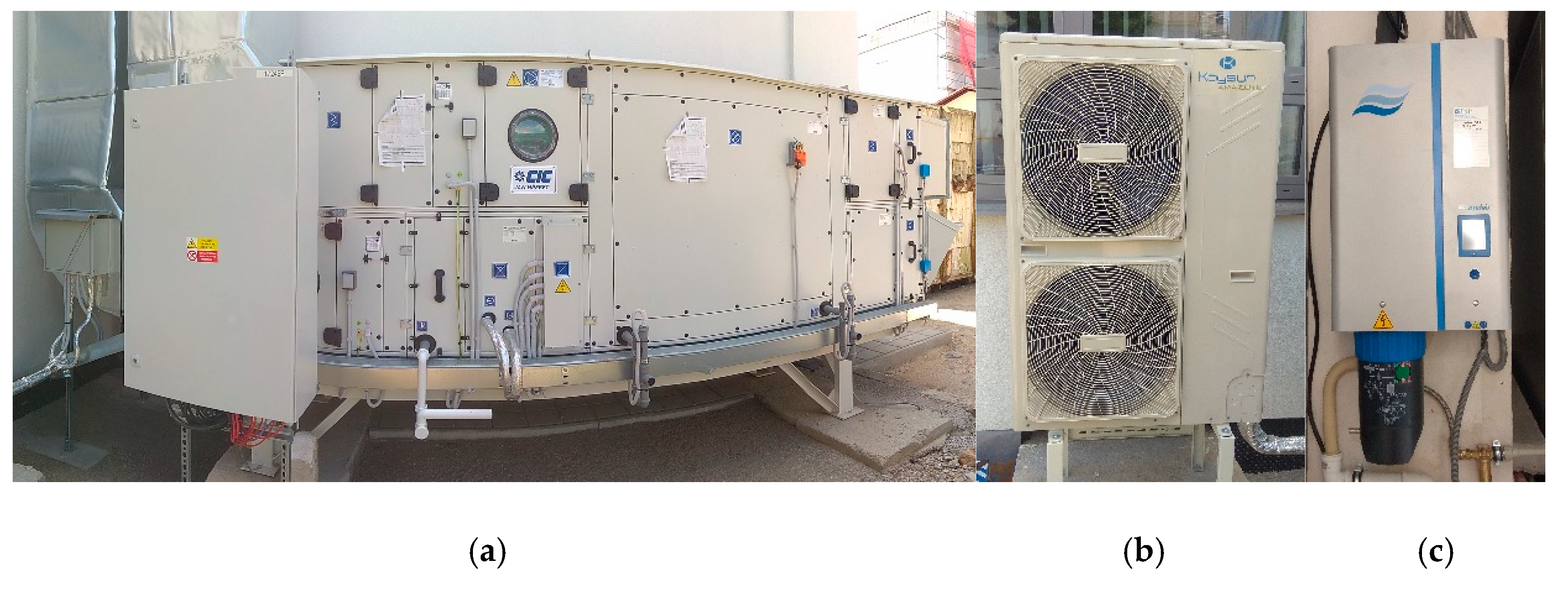
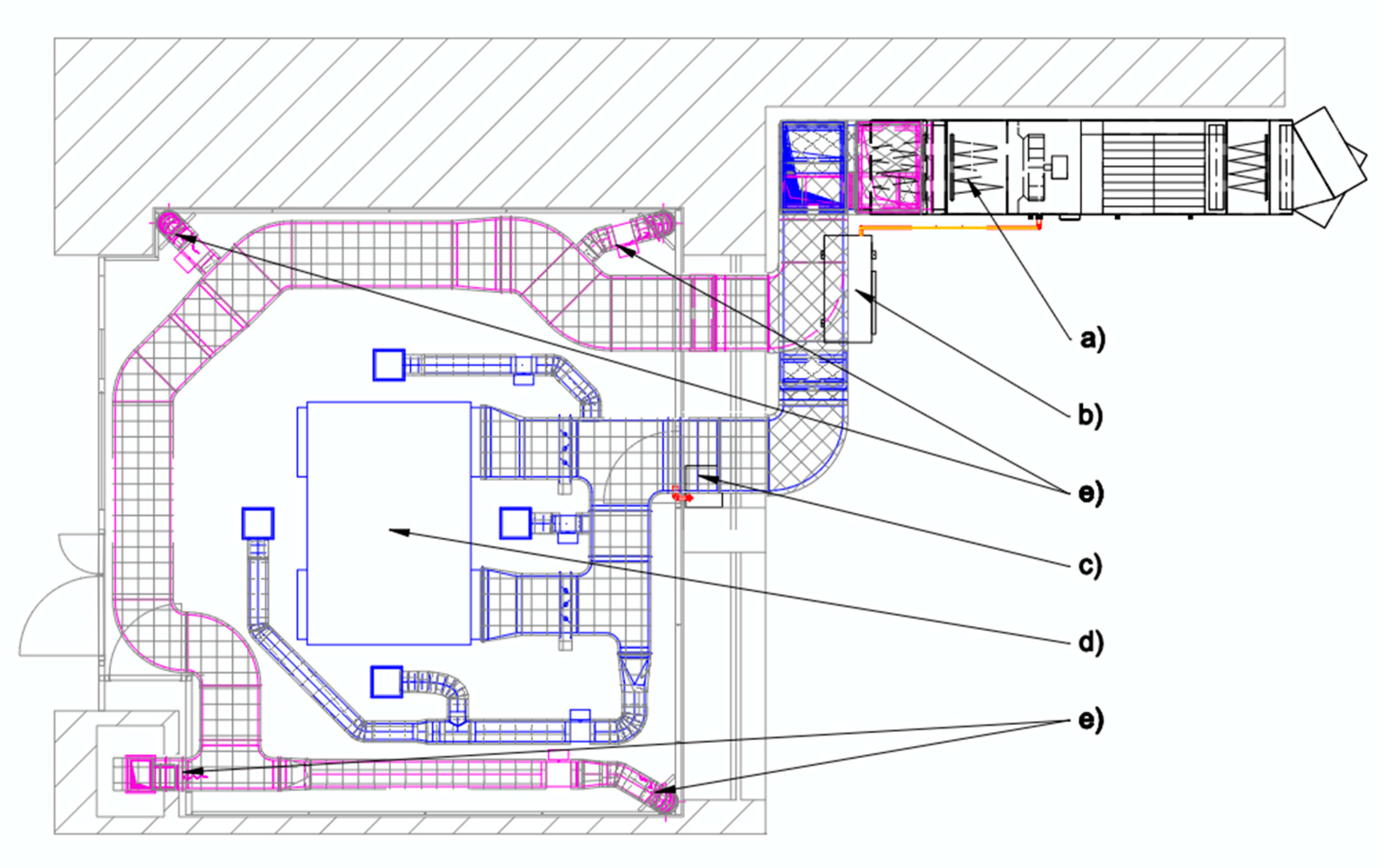
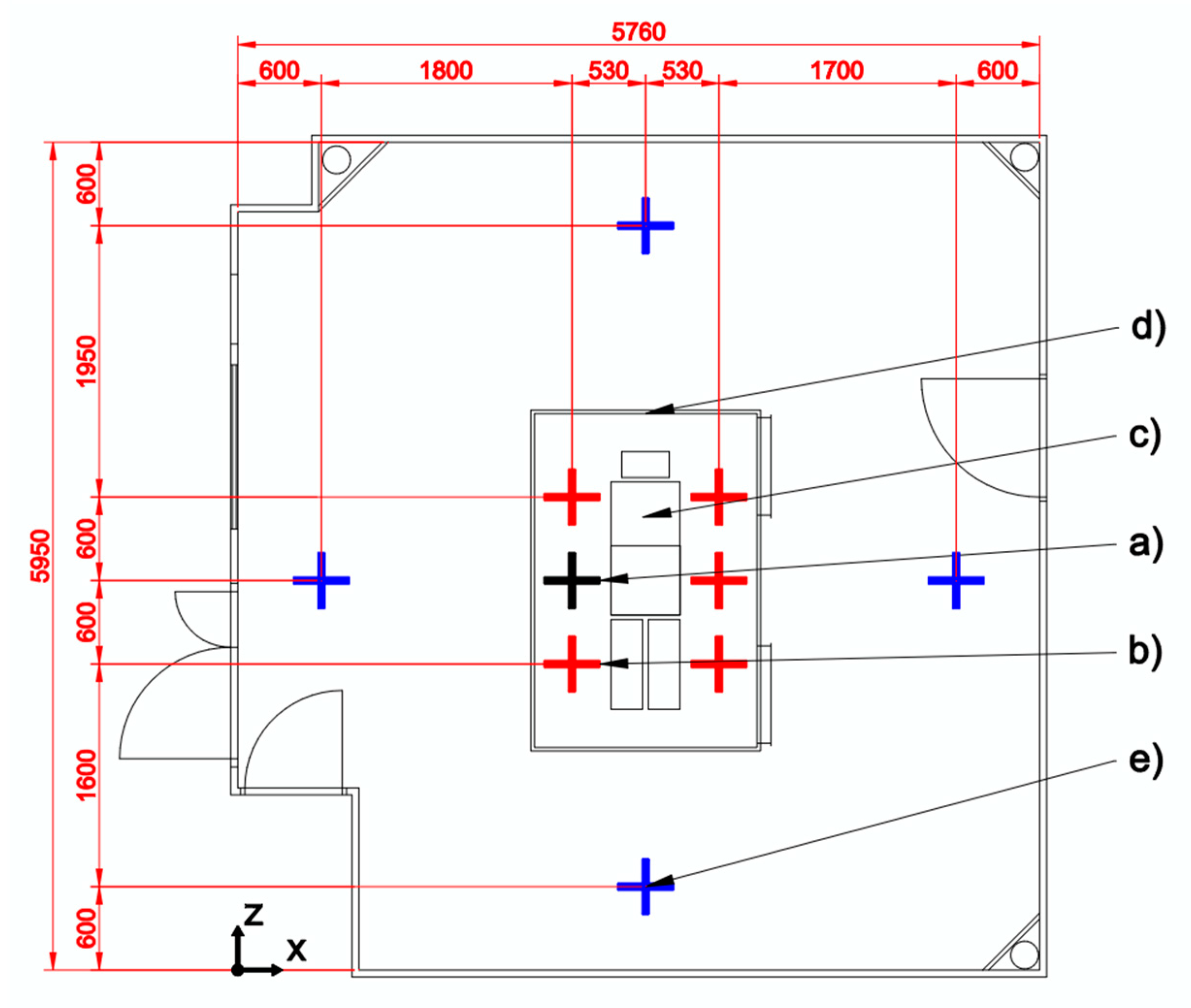
2.1. Operating Room Model
2.2. Evaluation of Thermal Comfort
- qq—total density of heat flow from the human body (W/m2)
- Rcl—thermal resistance of clothing (CLO) (m2K/W)
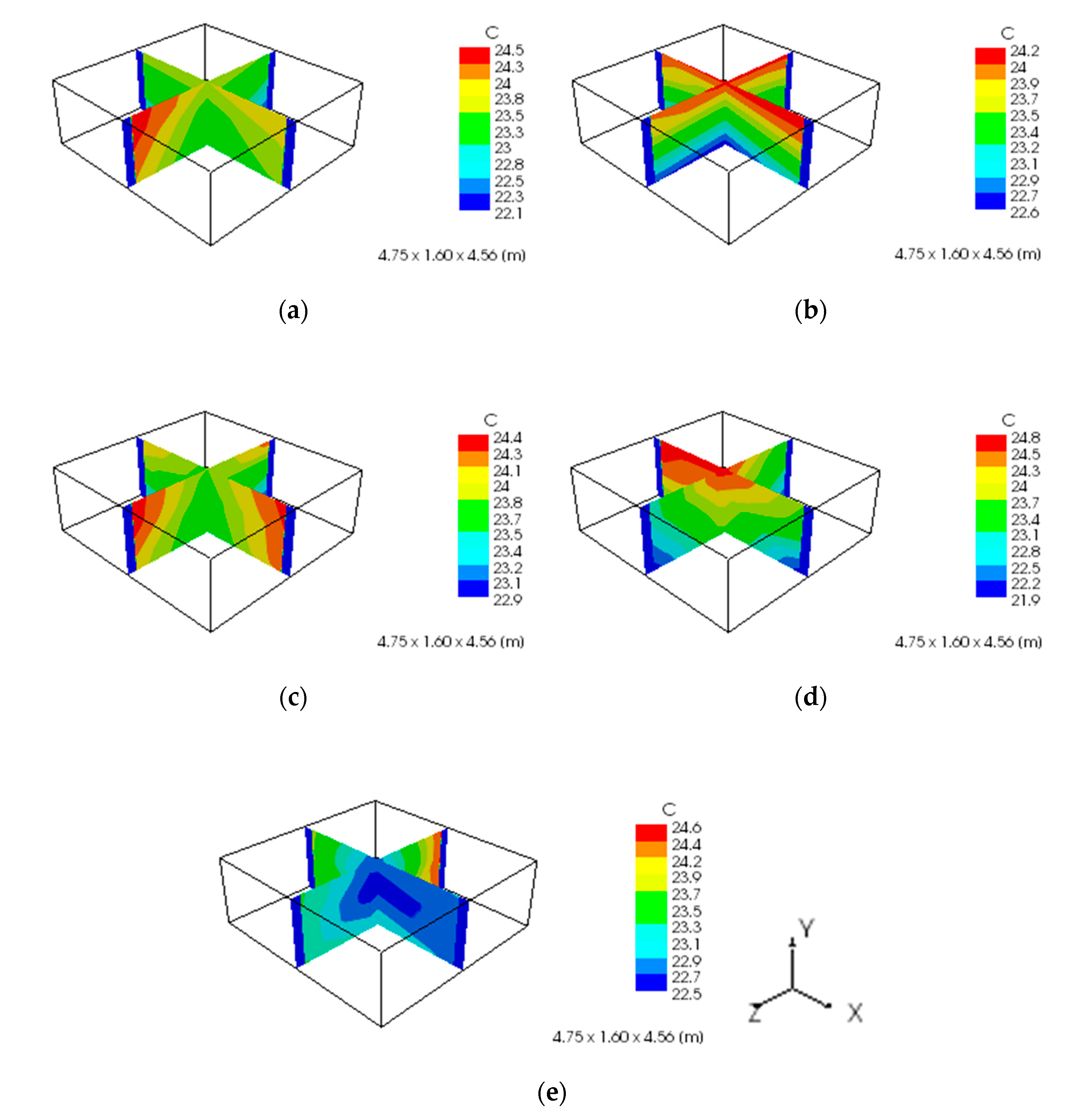
- θi—indoor air temperature (°C)
- pi—partial pressure of the water vapor of the internal air (Pa)
- vi—indoor air flow rate (m/s)
- θu—average radiant temperature (°C)
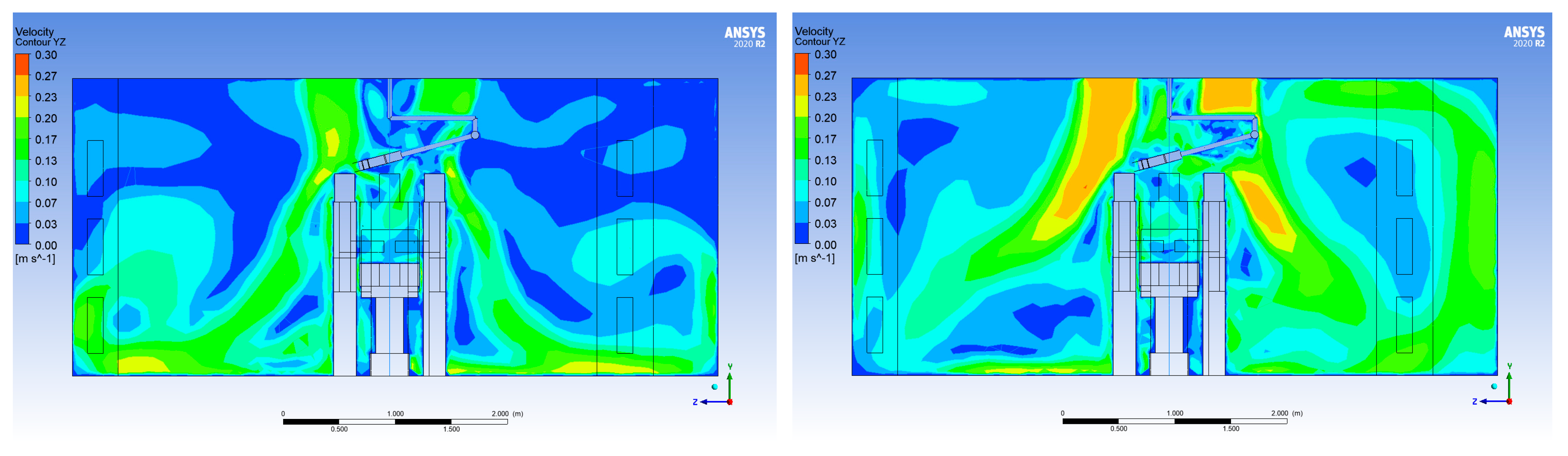
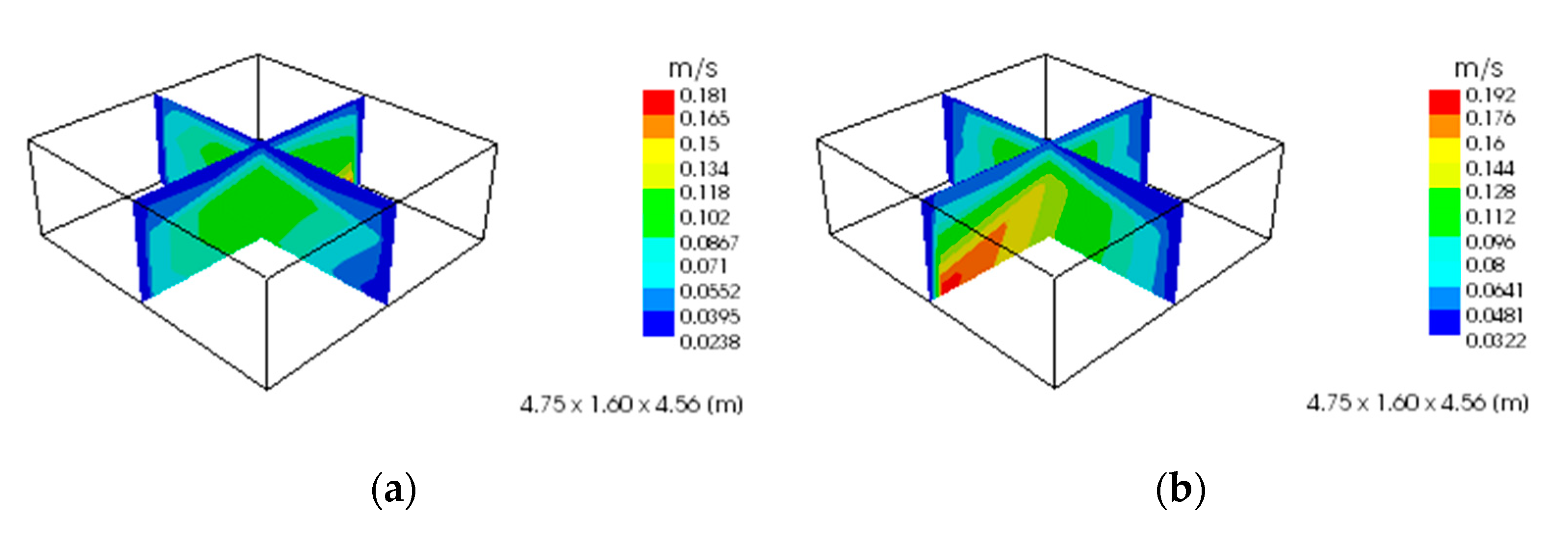
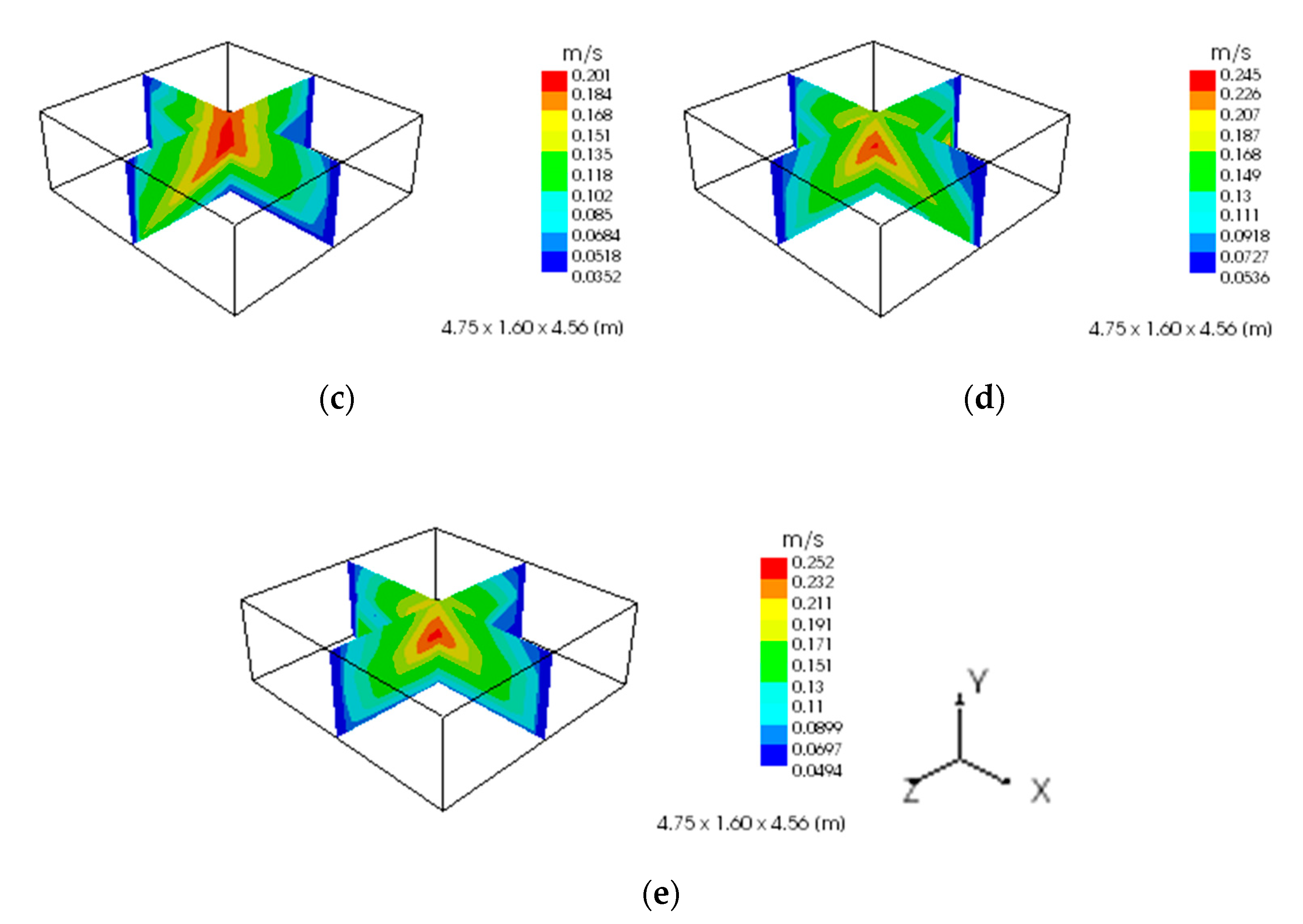
3. Results and Discussion
- —air flow of the supply distribution element (m3/h)
- —speed of the air flowing from the supply distribution element (m/s)
- —free outlet surface of the supply distribution element (m2)
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- EN ISO 14644-1; Cleanrooms and Associated Controlled Environments-Part 1: Classification of Air Cleanliness by Particle Concentration. International Organization for Standardization: London, UK, 2015.
- Vyhláška č. 259/2008 Z. z., Vyhláška Ministerstva Zdravotníctva Slovenskej Republiky o Podrobnostiach o Požiadavkách na Vnútorné Prostredie Budov a o Minimálnych Požiadavkách na Byty Nižšieho Štandardu a na Ubytovacie Zariadenia. Available online: https://www.epi.sk/zz/2008-259 (accessed on 20 February 2023).
- ASHRAE Standard 55-2020; Thermal Environmental Conditions for Human Occupancy. ASHRAE: Washington, DC, USA, 2020.
- EN ISO 15251; Indoor Environmental Input Parameters for Design and Assessment of Energy Performance of Buildings Addressing Indoor Air Quality, Thermal Environment, Lighting and Acoustics. International Organization for Standardization: London, UK, 2008.
- Walenkamp, G.H.I.M. Beheersplan Luchtbehandeling Voor de Operatieafdeling; Werkgroep Infectiepreventie: Maastricht, The Netherlands, 2005. [Google Scholar]
- VDI 2167; Technische Gebäudeausrüstung von Krankenhäusen. Verein Deutscher Ingenieure: Alexisbad, Germany, 2007.
- Deutsches Institut für Normung e.V. DIN 1946, Teil 4: Raumlufttechnische Anlagen in Krankenhäusern. Krankenh. Up2date 2007, 1, 69–81. [Google Scholar]
- ASHRAE/ASHE Standard 170; Ventilation of Health Care Facilities. R. American Society for Heating, Air-Conditioning Engineers Inc.: Washington, DC, USA, 2008.
- Standard 170-2013; Ventilation of Health Care Facilities. ASHRAE: Washington, DC, USA, 2013.
- Whyte, W. Cleanroom Design, 2nd ed.; John Wiley & Sons Ltd.: Choichester, UK, 1999; ISBN 0-471-94294-9. [Google Scholar]
- Balaras, C.A.; Dascalaki, E.; Gaglia, A. HVAC and indoor thermal conditions in hospital operating rooms. Energy Build. 2007, 39, 454–470. [Google Scholar] [CrossRef]
- Uścinowicz, P.; Chludzińska, M.; Bogdan, A. Thermal environment conditions in Polish operating rooms. Build. Env. 2015, 94, 296–304. [Google Scholar] [CrossRef]
- Verheyen, J.; Theys, N.; Allonsius, L.; Descamps, F. Thermal comfort of patients: Objective and subjective measurements in patient rooms of a Belgian healthcare facility. Build. Env. 2011, 46, 1195–1204. [Google Scholar] [CrossRef]
- Zoon, W.; Heijden, M.; Loomans, M.; Hensen, J. On the applicability of the laminar flow index when selecting surgical lighting. Build. Env. 2010, 45, 1976–1983. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, A.; Cardoso, J.; Guerra, N.; Ribeiro, E.; Viegas, C.; Cabo Verde, S.; Sousa-Uva, A. Exposure and Health Effects of Bacteria in Healthcare Units: An Overview. Appl. Sci. 2022, 12, 1958. [Google Scholar] [CrossRef]
- Chow, T.T. The integrated effect of medical lamp position and diffuser discharge velocity on ultra-clean ventilation performance in an operating theatre. Indoor Built. Env. 2006, 15, 315–331. [Google Scholar] [CrossRef]
- Ham, P.J. Handboek Ziekenhuisventilatie; TNO Kwaliteit van Leven: Leiden, The Netherlands, 2004. [Google Scholar]
- De Giuli, V.; Zecchin, R.; Salmaso, L.; Corain, L.; De Carli, M. Measured and perceived indoor environmental quality: Padua hospital case study. Build Env. 2013, 59, 211–226. [Google Scholar] [CrossRef]
- Mičko, P.; Hečko, D.; Kapjor, A.; Nosek, R.; Kolková, Z.; Hrabovský, P.; Kantová, N.Č. Impact of the Speed of Airflow in a Cleanroom on the Degree of Air Pollution. Appl. Sci. 2022, 12, 2466. [Google Scholar] [CrossRef]
- Zhao, F.Y.; Cheng, J.; Liu, B.; Huang, Z.R. Regional flow motion and heat energy balance analysis of a 10,000 class pharmaceutical cleanroom with secondary return air conditioning system. Int. J. Refrig. 2021, 129, 237–249. [Google Scholar] [CrossRef]
- Geaver, R.V.; Jacobs, V.A.; Diltoer, M.; Oeeters, L.; Vanlanduit, S. Thermal comfort of the surgical staff in the operating room. Build. Environ. 2014, 81, 37–41. [Google Scholar] [CrossRef]
- Yang, B.; Liu, P.; Liu, Y.; Jin, D.; Wang, F. Assessment of Thermal Comfort and Air Quality of Room Conditions by Impinging Jet Ventilation Integrated with Ductless Personalized Ventilation. Sustainability 2022, 14, 12526. [Google Scholar] [CrossRef]
- Yang, J.; Zhao, Y.; Zou, Y.; Xia, D.; Lou, S.; Guo, T.; Zhong, Z. Improving the Thermal Comfort of an Open Space via Landscape Design: A Case Study in Hot and Humid Areas. Atmosphere 2022, 13, 1604. [Google Scholar] [CrossRef]
- Peeters, L.; Dear, R.D.; Hensen, J.; Dhaeseleer, W. Thermal comfort in residential buildings: Comfort values and scales for building energy simulation. Appl. Energy 2009, 86, 772–780. [Google Scholar] [CrossRef] [Green Version]
- Laouadi, A. A New General Formulation for the PMV Thermal Comfort Index. Buildings 2022, 12, 1572. [Google Scholar] [CrossRef]
- Mičko, P.; Kapjor, A.; Holubčík, M.; Hečko, D. Experimental Verification of CFD Simulation When Evaluating the Operative Temperature and Mean Radiation Temperature for Radiator Heating and Floor Heating. Processes 2021, 9, 1041. [Google Scholar] [CrossRef]
- ISO 7730; Moderate Thermal Environments-Determination of the PMV and PPD Indices and Specification of the Conditions for Thermal Comfort. ISO: Geneva, Switzerland, 2005.
- Gagge, A.P. The linearity criterion as applied to partitional calorimetry. Am. J. Physiol. 1946, 116, 656–668. [Google Scholar] [CrossRef]
- Houghten, F.C.; Yagloglou, C.P. Determining lines of equal comfort. Trans. Am. Soc. Heat. Vent. Eng. 1923, 29, 165–176. [Google Scholar]
- Gagge, A.P.; Fobelets, A.P.; Berglund, L.G. A standard predictive index of human response to the thermal environment. ASHARE Trans. 1986, 92, 709–731. [Google Scholar]
- Fanger, P.O. Thermal Comfort-Analysis and Applications in Environmental Engineering; Danish Technical Press: Copenhagen, Denmark, 1970. [Google Scholar]
- Krawczyk, B. The Heat Balance of the Human Body as Basis for the Bioclimatic Divide of the Health Resort Iwonicz; Redaktor Techniczny Adam Przylibski: Wrocław, Poland, 1979. [Google Scholar]
- Melhado, M.; Hensen, J.; Loomans, M. Literature review of staff thermal comfort and patient “thermal risk” in operating rooms. In Proceedings of the 8th International Healthy Buildings Conference, Lisboa, Portugal, 4–8 June 2006. [Google Scholar]
- Wang, F.J.; Zheng, Y.R.; Lai, C.M.; Chiang, C.M. Evaluation of Thermal Comfort and Contamination Control for a Cleanroom. J. Appl. Sci. 2008, 8, 1684–1691. [Google Scholar] [CrossRef] [Green Version]
- Angelova, R.A.; Velichkova, R. Thermophysiological Comfort of Surgeons and Patient in an Operating Room Based on PMV-PPD and PHS Indexes. Appl. Sci. 2020, 10, 1801. [Google Scholar] [CrossRef] [Green Version]
- Gilani, S.I.U.; Khan, M.H.; Pao, W. Thermal Comfort Analysis of PMV Model Prediction in Air Conditioned and Naturally Ventilated Buildings. Energy Procedia 2015, 75, 1373–1379. [Google Scholar] [CrossRef] [Green Version]
- Dyvia, H.A.; Arif, C. Analysis of thermal comfort with predicted mean vote (PMV) index using artificial neural network. Earth Environ. Sci. 2021, 622, 012019. [Google Scholar] [CrossRef]
- Cheung, T.; Schiavon, S.; Parkinson, T.; Li, P.; Brager, G. Analysis of the accuracy on PMV–PPD model using the ASHRAE Global Thermal Comfort Database II. Build. Environ. 2019, 153, 205–217. [Google Scholar] [CrossRef] [Green Version]
- Bogdan, A.; Sudoł-Szopińska, I.; Szopiński, T. Assessment of textiles for use in operating theatres with respect to the thermal comfort of surgeons. Fibres Text. East. Eur. 2011, 19, 65–69. [Google Scholar]
- S. Verein Von Wärme-Und Klima Ingenieuren. Richtlinie 99–103: Heizungs-, Lüftungs-Und Klimaanlagen in Spitalbauten (Planung, Bau, Betreib). 2003. Available online: https://www.sciencedirect.com/science/article/pii/S0360132314001875 (accessed on 6 April 2023).
- Novoselac, A.; Srebric, J. Comparison of air exchange efficiency and contaminant removal effectiveness as IAQ indices. ASHRAE Trans. 2003, 109, 339–349. [Google Scholar]
- Zhao, F.-Y.; Cheng, J.; Liu, B.; Huang, Z.-R.; Li, X. Indoor airflow and pollutant spread inside the cleanroom with micro-porous supplying panel and different ventilation schemes: Analytical, numerical and experimental investigations. J. Build. Eng. 2020, 31, 101405. [Google Scholar] [CrossRef]
- Pereira, P.F.D.C.; Broday, E.E.; Xavier, A.A.D.P. Thermal Comfort Applied in Hospital Environments: A Literature Review. Appl. Sci. 2020, 10, 7030. [Google Scholar] [CrossRef]
- Atmaca, I.; Kaynakli, O.; Yigit, A. Effects of radiant temperature on thermal comfort. Build. Environ. 2007, 42, 3210–3220. [Google Scholar] [CrossRef]
- Brager, G.S.; Dear, R.D. Climate, comfort & natural ventilation: A new adaptive comfort standard for ASHRAE Standard 55. In Proceedings of the Moving Thermal Comfort Standards into the 21st Century, Windsor, UK, 5–8 April 2001. [Google Scholar]
- Tschudi, W.; Mills, E.; Tenfang, X.; Rumsey, P. Measuring and managing cleanroom energy use. Heat. Pip. Air Cond. Eng. 2005, 77, 29–35. [Google Scholar]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Standard | Supply Air Temperature ta (°C) | Relative Humidity (%) | Supply Air Velocity (m/s) |
|---|---|---|---|
| EN ISO 14 644-1 [1] | 22–26 | 40–60 | 0.1 |
| ZZ 259/2012 [2] | ta > 25 | 30–70 | - |
| DIN 1946 [7] | 19–26 | - | v ≥ 0.23 |
| VDI 2167 [6] | 22 | 30–50 | v ≥ 0.23 |
| ASHRAE 170 [8] | 20–24 | 30–60 | 0.13–0.18 |
| ASHRAE application handbook [9] | 17–27 | 45–55 | 1.3–1.8 |
| Mark Measuring Element | Measured Quantity | Thermal Comfort Parameter | Accuracy of Measurement | Vertical Position Y (m) |
|---|---|---|---|---|
| H1 H2 H3 | ta—air temperature | ta—air temperature | ± 0.2 °C | 0.1 1.1 1.7 |
| va—indoor air flow rate | va—indoor air flow rate | ±0.02 m/s | ||
| OT | to—operative temperature | tr—average radiant temperature | ±0.2 °C | 1.1 |
| RH | φ—relative humidity | pp—partial pressure of water vapor | ±2% | 1.8 |
| Variant | vSUP (m/s) | VSUP (m3/h) |
|---|---|---|
| 1 | 0.150 | 1916 |
| 2 | 0.175 | 2235 |
| 3 | 0.200 | 2555 |
| 4 | 0.225 | 2874 |
| 5 | 0.250 | 3194 |
| Measuring Element | Unit | Variant | ||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||
| H1 | ta (°C) | 23.1 | 22.6 | 23.5 | 23.7 | 23.0 |
| H2 | ta (°C) | 23.4 | 23.5 | 23.7 | 24.3 | 22.5 |
| H3 | ta (°C) | 23.8 | 24.1 | 23.8 | 24.8 | 22.7 |
| H1 | va (m/s) | 0.10 | 0.14 | 0.05 | 0.11 | 0.09 |
| H2 | va (m/s) | 0.12 | 0.15 | 0.20 | 0.24 | 0.25 |
| H3 | va (m/s) | 0.03 | 0.05 | 0.19 | 0.19 | 0.20 |
| OT | to (°C) | 23.4 | 23.4 | 23.5 | 24.1 | 22.6 |
| RH | φ (%) | 44 | 44 | 42 | 40 | 45 |
| PMV Index | Variant | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| position H1 [-] | −0.62 | −0.90 | −0.80 | −0.81 | −1.25 |
| position H2 [-] | −0.70 | −0.91 | −1.18 | −1.25 | −1.86 |
| position H3 [-] | −0.53 | −0.62 | −1.16 | −1.10 | −1.71 |
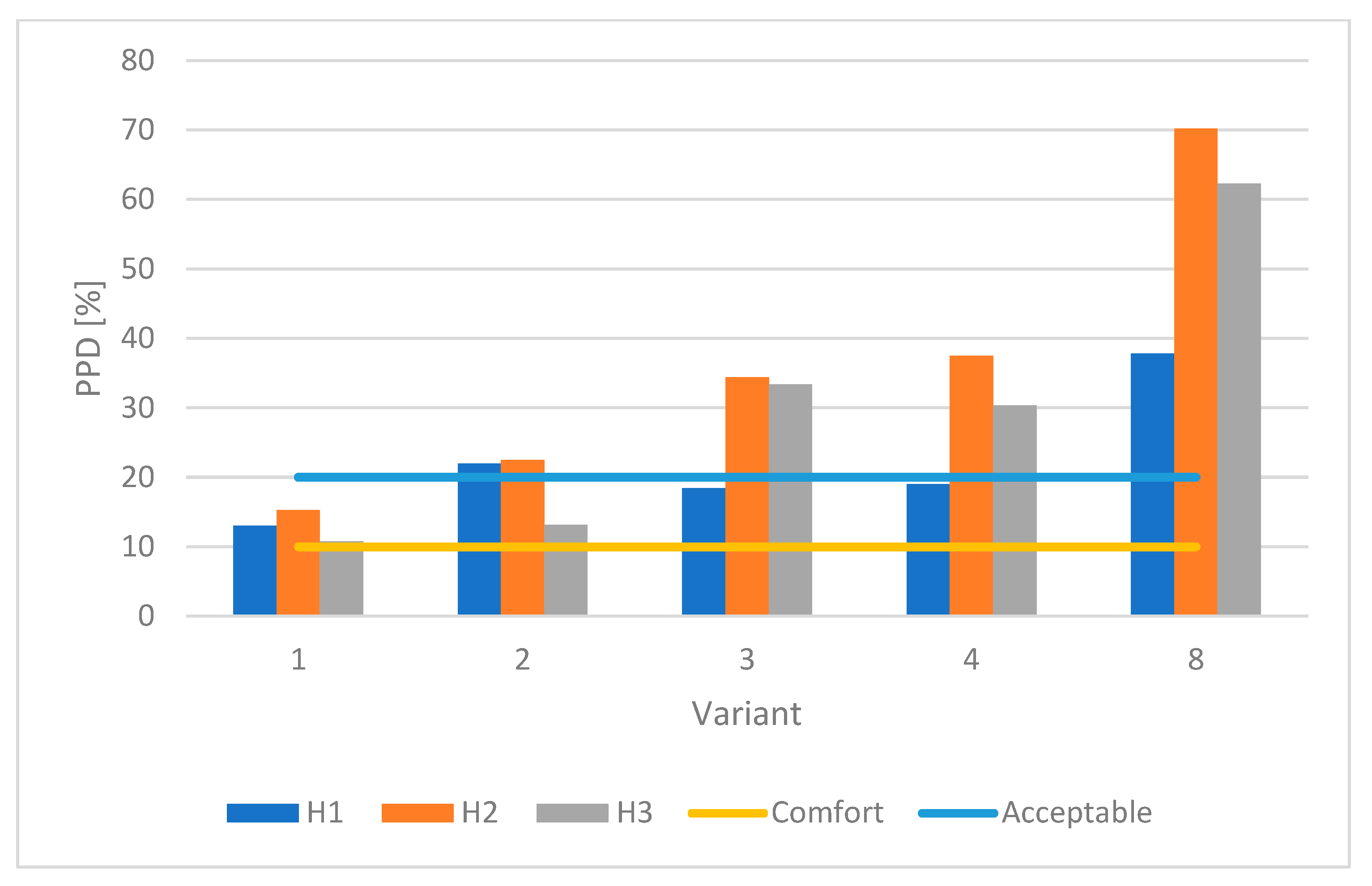
| PPD Index | Variant | ||||
| 1 | 2 | 3 | 4 | 5 | |
| position H1 [%] | 13.04 | 21.95 | 18.45 | 19.01 | 37.77 |
| position H2 [%] | 15.26 | 22.47 | 34.35 | 37.50 | 70.20 |
| position H3 [%] | 10.79 | 13.12 | 33.34 | 30.31 | 62.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mičko, P.; Nosek, R.; Hrabovský, P.; Hečko, D. The Effect of Airflow Velocity through a Laminar Airflow Ceiling (LAFC) on the Assessment of Thermal Comfort in the Operating Room. Appl. Sci. 2023, 13, 4860. https://doi.org/10.3390/app13084860
Mičko P, Nosek R, Hrabovský P, Hečko D. The Effect of Airflow Velocity through a Laminar Airflow Ceiling (LAFC) on the Assessment of Thermal Comfort in the Operating Room. Applied Sciences. 2023; 13(8):4860. https://doi.org/10.3390/app13084860
Chicago/Turabian StyleMičko, Pavol, Radovan Nosek, Peter Hrabovský, and Dávid Hečko. 2023. "The Effect of Airflow Velocity through a Laminar Airflow Ceiling (LAFC) on the Assessment of Thermal Comfort in the Operating Room" Applied Sciences 13, no. 8: 4860. https://doi.org/10.3390/app13084860