
MRONJ Treatment Strategies: A Systematic Review and Two Case Reports

 ,
,  , , , , , , , ,
, , , , , , , ,  ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
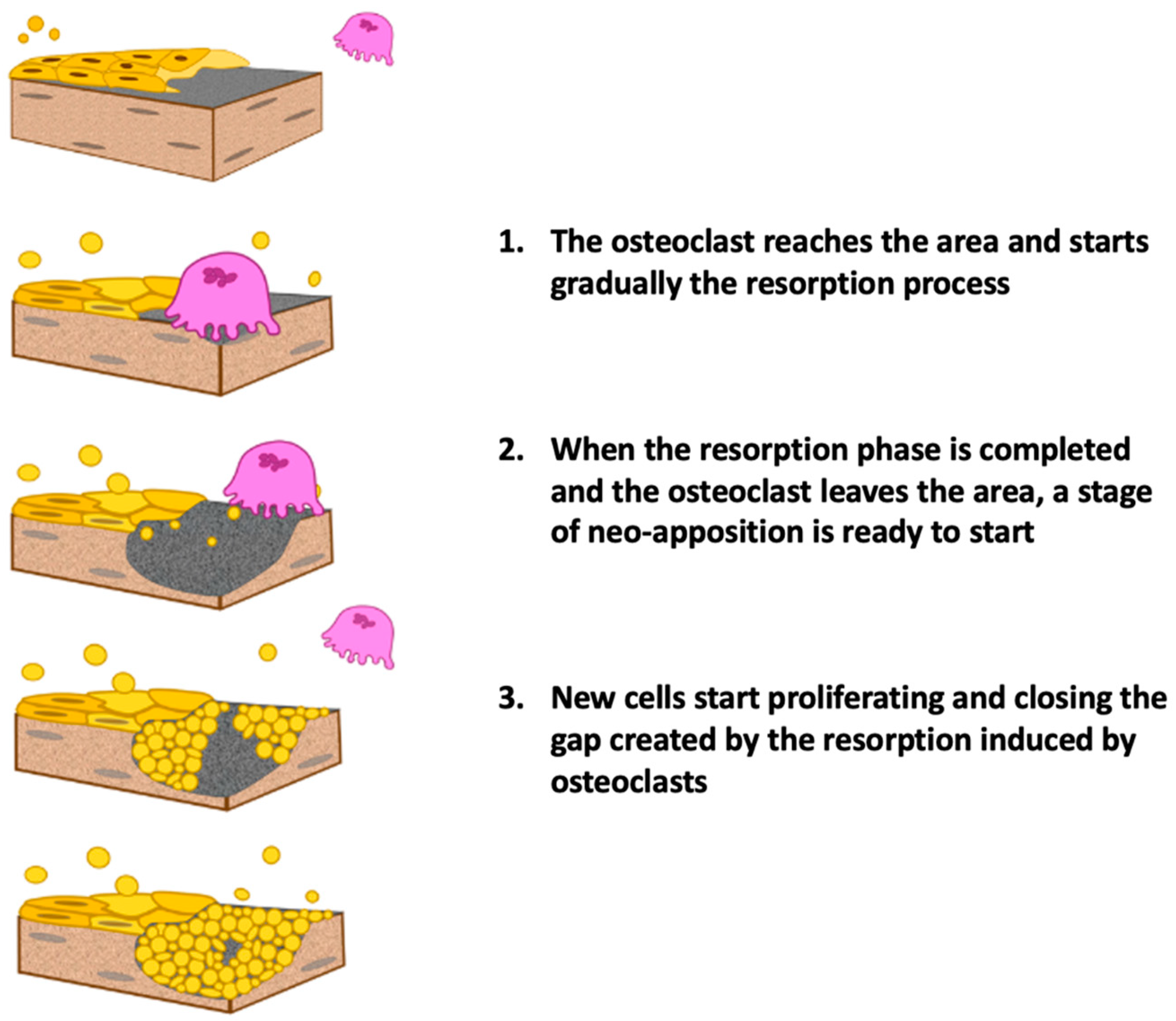
1.1. Pathogenesis
- More rapid bone turnover than in the long bones;
- Terminal-type vascularization;
- Mucoperiosteal lining overlying the bone tissue is easily subject to trauma;
- Presence of microflora/biofilm in the oral cavity;
1.2. Most Associated Drugs with MRONJ
- Tyrosine kinase inhibitors (TKIs) such as sunitinib;
- Additional monoclonal antibodies, angiogenesis inhibitors, such as bevacizumab;
- Fusion proteins such as aflibercept;
- mTOR inhibitors such as everolimus;
- Radiopharmaceuticals such as radium-223;
- Estrogen inhibitors such as raloxifene;
- Immunomodulators (methotrexate and corticosteroids) [14].
1.3. Half-Life
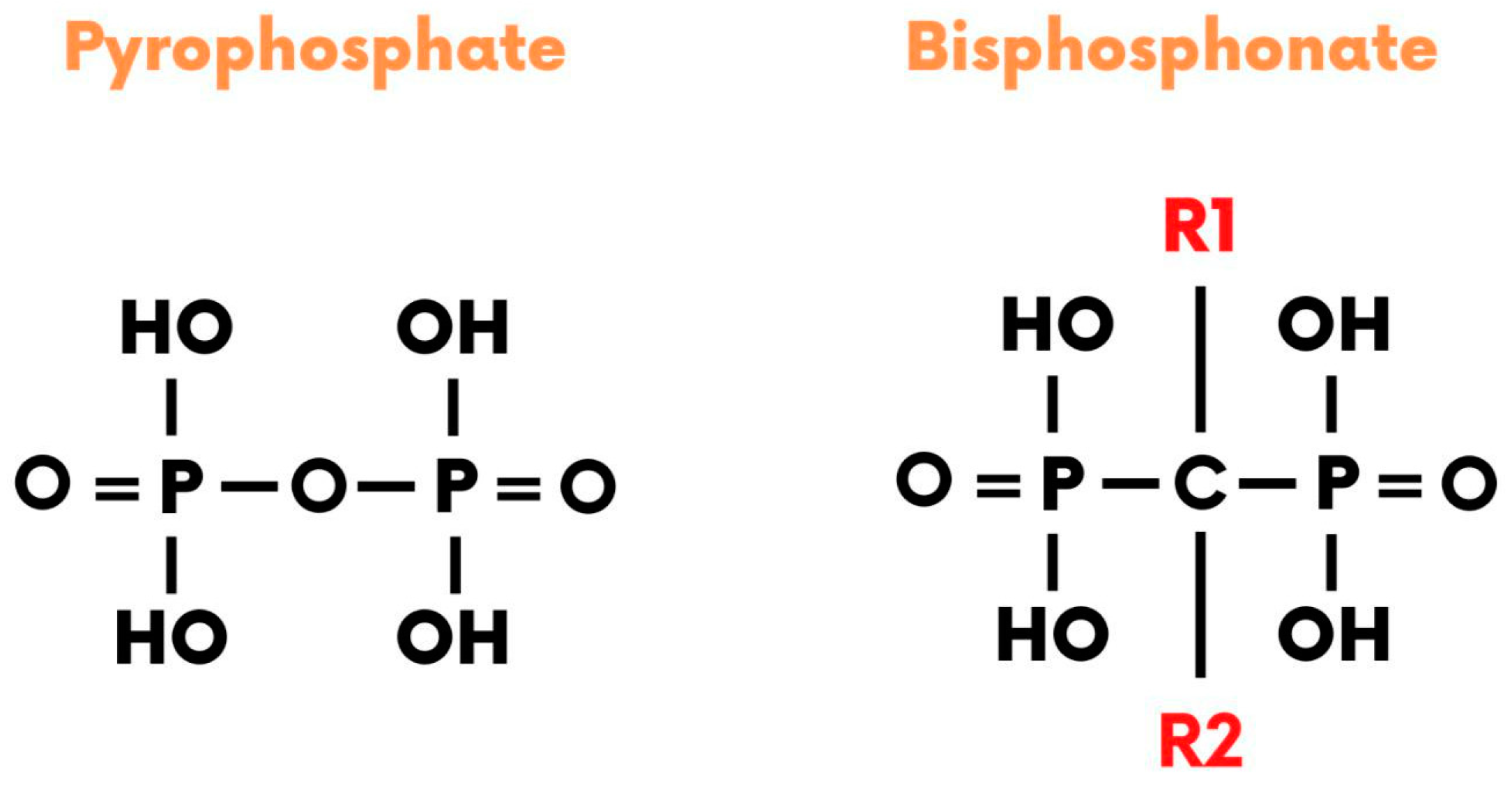
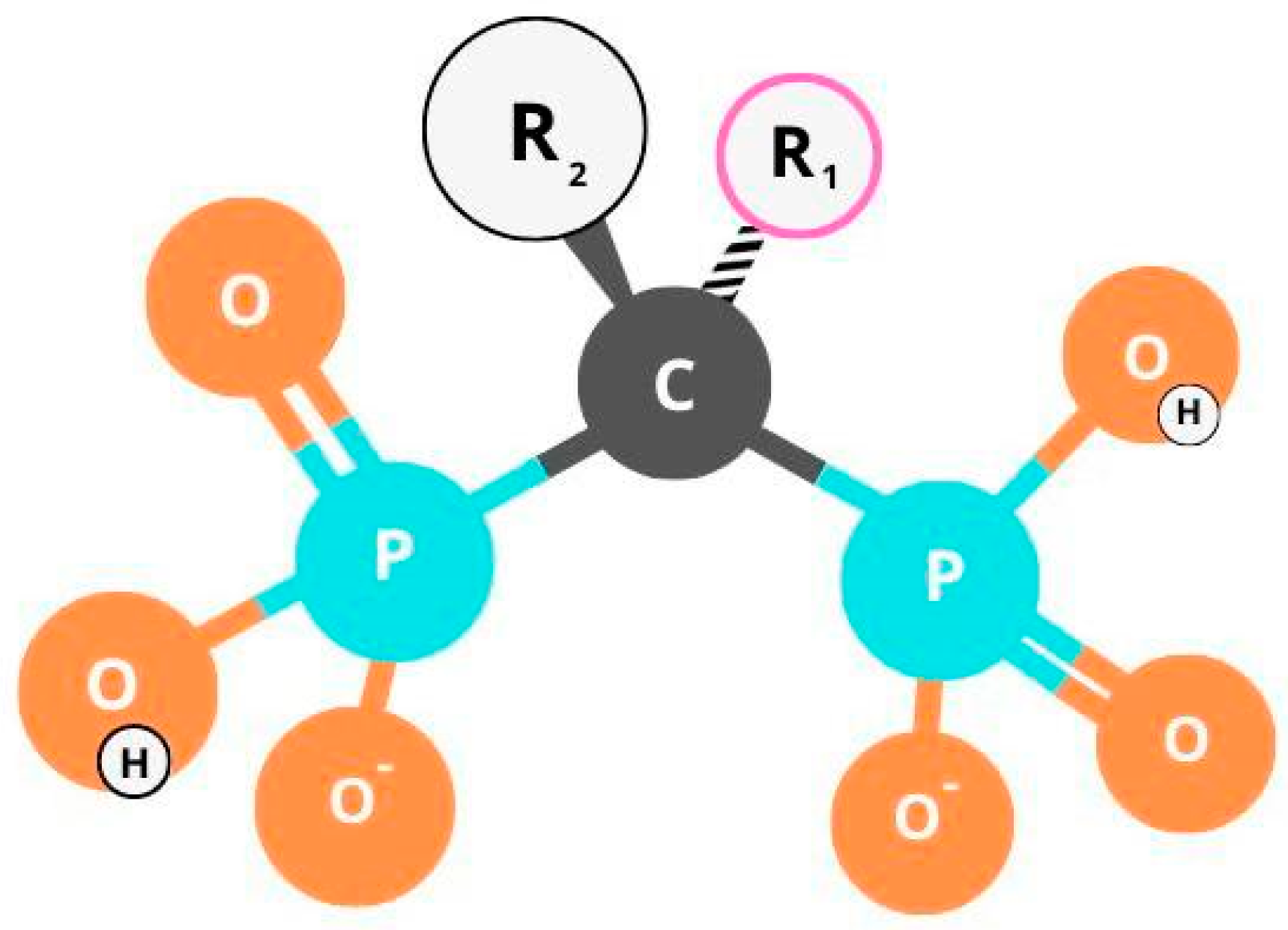
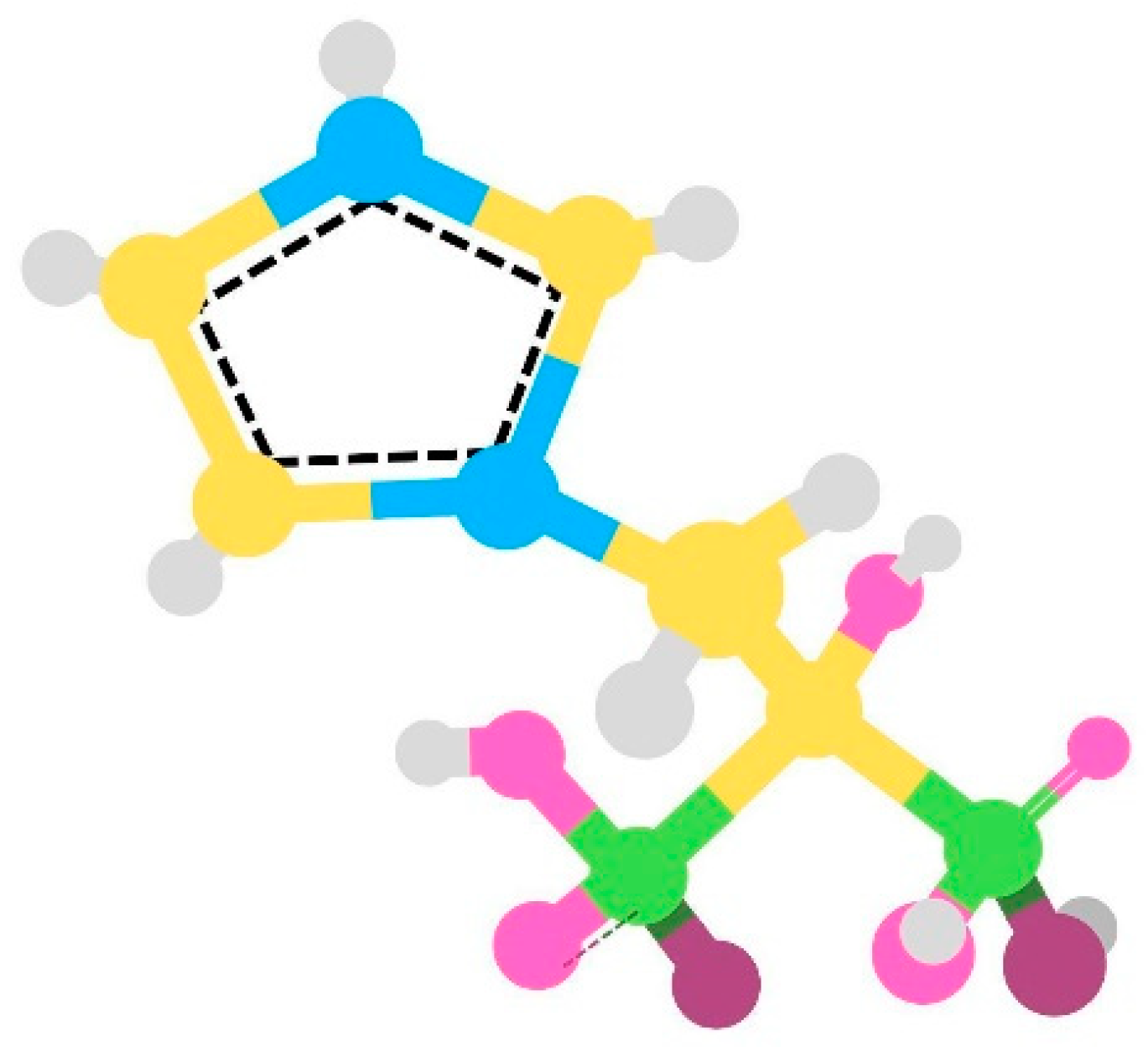
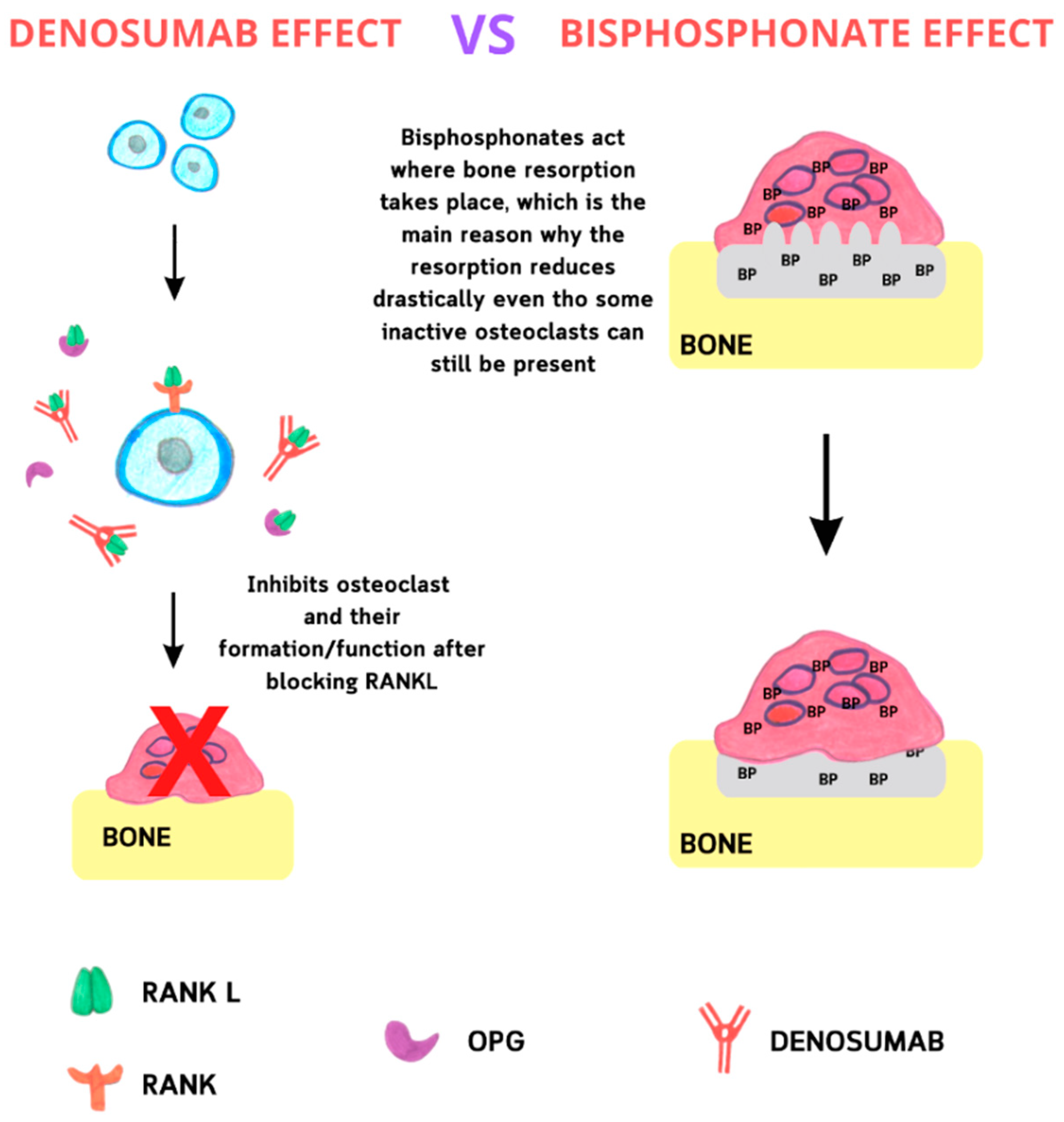
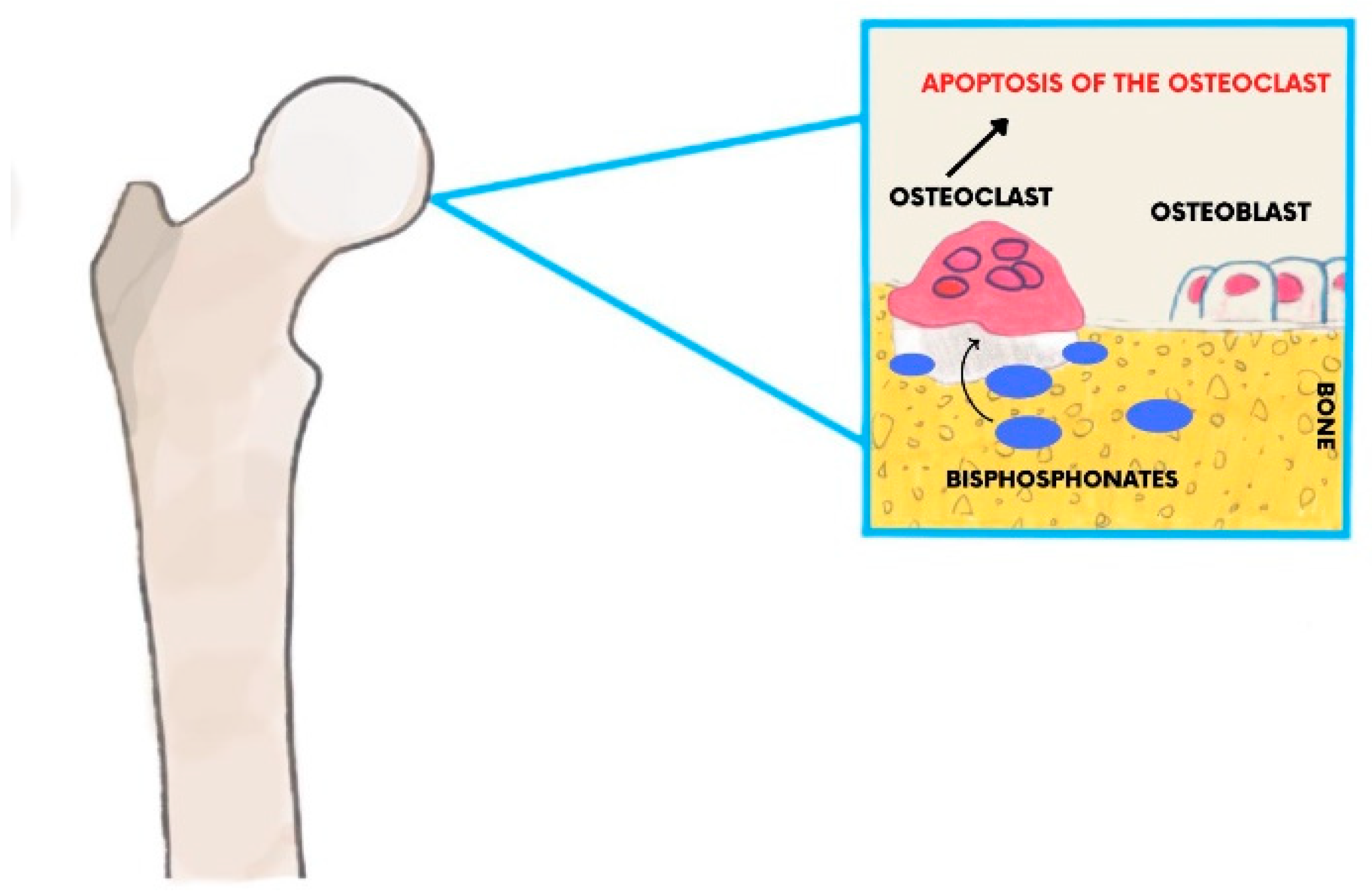
1.4. Mechanism of Action
1.5. Risk Factors Associated with MRONJ
1.6. Local Causal Factors
1.7. Staging
- Stage 0—Clinical symptoms and nonspecific radiological signs without exposure of the bone;
- Stage I—Exposed bone <2 cm with or without pain;
- Stage II—Exposed bone between 2 and 4 cm with pain responsive to nonsteroidal anti-inflammatory drugs (NSAIDs);
- Stage III—Exposed bone >4 cm with pain not responsive to NSAIDs + complications (fistulae, maxillary sinus, or inferior alveolar nerve involvement) [21].
1.8. Actual Practice Guideline
2. Materials and Methods
2.1. Protocol
2.2. Data Sources and Search Strategy
2.3. Inclusion and Exclusion Criteria
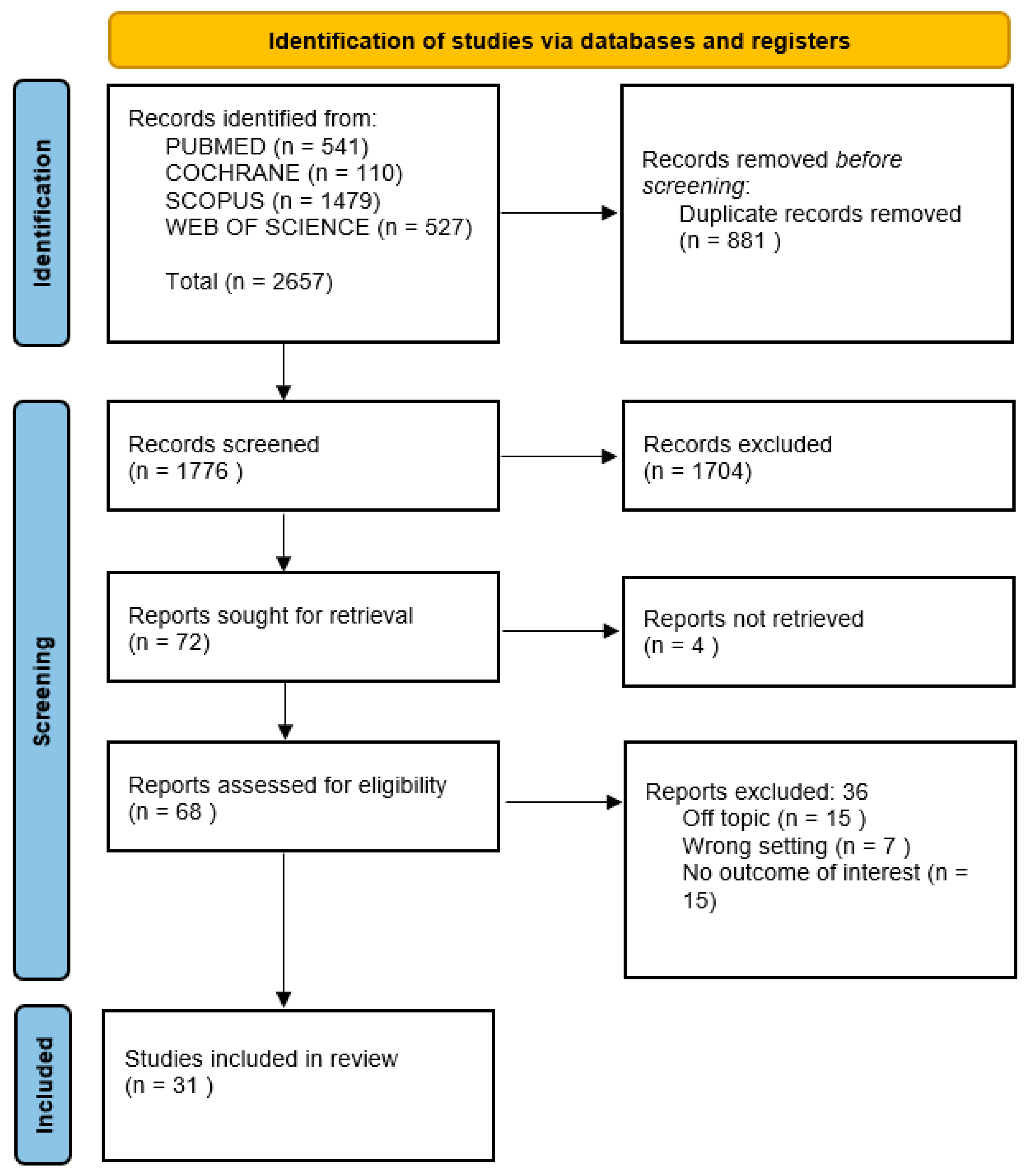
2.4. Study Selection and Characteristics
3. Results
4. Discussion
4.1. Medical Treatment
4.1.1. Antiseptic Therapy
4.1.2. Antibiotic Therapy
4.1.3. Pain Relief Therapy
4.1.4. Teriparatide Therapy
4.1.5. Pre- and Postsurgery Pharmacological Protocols
4.2. Laser Therapy
4.3. Minimally Invasive Surgery: Debridement
4.4. Surgical Resection
4.5. Fluorescence-Guided Bone Surgery
4.6. Platelet-Rich Plasma (PRP), Platelet-Rich Fibrin (PRF), Concentrated Growth Factor (CGF), and Piezosurgery (PZ)
4.7. Vascular Endothelial Growth Factor (VEGF) and Hyaluronic Acid (HA)
4.8. Ozone Terapy
5. Case Reports
5.1. Case Report 1
5.2. Case Report 2
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAOMS | American Association of Oral and Maxillofacial Surgeons |
| ARONJ | Antiresorptive agent-related osteonecrosis of the jaw |
| ARAs | Antiresorptive agents |
| APC | Autologous platelet concentrates |
| BRONJ | Bisphosphonate-related osteonecrosis of the jaw |
| BPs | Bisphosphonates |
| BFF | Buccal fat flap |
| CRP | C reactive protein |
| CONJ | Chemo-osteonecrosis of the jaws |
| CGF | Concentrated growth factor |
| CT | Conservative treatment |
| CTX | C-terminal telopeptide of type 1 collagen |
| DB | Denosumab |
| DRONJ | Denosumab-related osteonecrosis of the jaws |
| FDG PET-CT | Fluorodeoxyglucose positron emission tomography with computed tomography |
| HA | Hyaluronic acid |
| HBO | Hyperbaric oxygen; IPR: inflammatory, proliferative, remodeling |
| LLLT | Low level laser therapy |
| MRONJ | Medication-related osteonecrosis of the jaws |
| MMF | Mylohyoid muscle flap |
| NBPs | Non-aminobisphosphonates |
| NSAIDs | Nonsteroidal anti-inflammatory drugs |
| N.R. | Not reported |
| OHIP-G14 | Oral health impact factor-g14 |
| ONJ | Osteonecrosis of the jaws |
| OPG | Osteoprotegerin |
| ORN | Osteoradionecrosis |
| PR | Periosteal reaction |
| PZ | Piezosurgery |
| PRF | Platelet rich fibrin |
| PRP | Platelet-rich plasma |
| P | Prospective |
| RCT | Randomized clinical trial |
| RANK | Reactive activator of nuclear κb |
| R | Retrospective |
| ST | Surgical treatment |
| TKIs | Tyrosine kinase inhibitors |
| VAS | Visual analog scale |
| VEGF | Vascular endothelial growth factor |
References
- Dodson, T.B. The Frequency of Medication-Related Osteonecrosis of the Jaw and Its Associated Risk Factors. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Ramaglia, L.; Guida, A.; Iorio-Siciliano, V.; Cuozzo, A.; Blasi, A.; Sculean, A. Stage-Specific Therapeutic Strategies of Medication-Related Osteonecrosis of the Jaws: A Systematic Review and Meta-Analysis of the Drug Suspension Protocol. Clin. Oral Investig. 2018, 22, 597–615. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L. Reply: AAOMS Position Paper on Medication-Related Osteonecrosis of the Jaws-2022 Update. Diagnostic Milestones, Doubts, and Perspectives on MRONJ. J. Oral Maxillofac. Surg. 2022, 80, 1724. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 328 Diseases and Injuries for 195 Countries, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosella, D.; Papi, P.; Giardino, R.; Cicalini, E.; Piccoli, L.; Pompa, G. Medication-Related Osteonecrosis of the Jaw: Clinical and Practical Guidelines. J. Int. Soc. Prev. Community Dent. 2016, 6, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udagawa, N.; Koide, M.; Nakamura, M.; Nakamichi, Y.; Yamashita, T.; Uehara, S.; Kobayashi, Y.; Furuya, Y.; Yasuda, H.; Fukuda, C.; et al. Osteoclast Differentiation by RANKL and OPG Signaling Pathways. J. Bone Miner. Metab. 2021, 39, 19–26. [Google Scholar] [CrossRef]
- Aghaloo, T.L.; Kang, B.; Sung, E.C.; Shoff, M.; Ronconi, M.; Gotcher, J.E.; Bezouglaia, O.; Dry, S.M.; Tetradis, S. Periodontal Disease and Bisphosphonates Induce Osteonecrosis of the Jaws in the Rat. J. Bone Miner. Res. 2011, 26, 1871–1882. [Google Scholar] [CrossRef] [Green Version]
- Abtahi, J.; Agholme, F.; Sandberg, O.; Aspenberg, P. Bisphosphonate-Induced Osteonecrosis of the Jaw in a Rat Model Arises First after the Bone Has Become Exposed. No Primary Necrosis in Unexposed Bone. J. Oral Pathol. Med. 2012, 41, 494–499. [Google Scholar] [CrossRef]
- Marx, R.E. Pamidronate (Aredia) and Zoledronate (Zometa) Induced Avascular Necrosis of the Jaws: A Growing Epidemic. J. Oral Maxillofac. Surg. 2003, 61, 1115–1117. [Google Scholar] [CrossRef]
- Favot, C.L.; Forster, C.; Glogauer, M. The Effect of Bisphosphonate Therapy on Neutrophil Function: A Potential Biomarker. Int. J. Oral Maxillofac. Surg. 2013, 42, 619–626. [Google Scholar] [CrossRef]
- Zhang, Q.; Atsuta, I.; Liu, S.; Chen, C.; Shi, S.; Shi, S.; Le, A.D. IL-17-Mediated M1/M2 Macrophage Alteration Contributes to Pathogenesis of Bisphosphonate-Related Osteonecrosis of the Jaws. Clin. Cancer Res. 2013, 19, 3176–3188. [Google Scholar] [CrossRef] [Green Version]
- Roelofs, A.J.; Jauhiainen, M.; Mönkkönen, H.; Rogers, M.J.; Mönkkönen, J.; Thompson, K. Peripheral Blood Monocytes Are Responsible for Gammadelta T Cell Activation Induced by Zoledronic Acid through Accumulation of IPP/DMAPP. Br. J. Haematol. 2009, 144, 245–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, B.J.; Hellstein, J.W.; Jacobsen, P.L.; Kaltman, S.; Mariotti, A.; Migliorati, C.A. American Dental Association Council on Scientific Affairs Expert Panel on Bisphosphonate-Associated Osteonecrosis of the Jaw Updated Recommendations for Managing the Care of Patients Receiving Oral Bisphosphonate Therapy: An Advisory Statement from the American Dental Association Council on Scientific Affairs. J. Am. Dent. Assoc. 2008, 139, 1674–1677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American Association of Oral and Maxillofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws-2022 Update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef]
- Lasseter, K.C.; Porras, A.G.; Denker, A.; Santhanagopal, A.; Daifotis, A. Pharmacokinetic Considerations in Determining the Terminal Elimination Half-Lives of Bisphosphonates. Clin. Drug Investig. 2005, 25, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Cardwell, C.R.; Abnet, C.C.; Cantwell, M.M.; Murray, L.J. Exposure to Oral Bisphosphonates and Risk of Esophageal Cancer. JAMA 2010, 304, 657–663. [Google Scholar] [CrossRef] [Green Version]
- Lacey, D.L.; Boyle, W.J.; Simonet, W.S.; Kostenuik, P.J.; Dougall, W.C.; Sullivan, J.K.; San Martin, J.; Dansey, R. Bench to Bedside: Elucidation of the OPG-RANK-RANKL Pathway and the Development of Denosumab. Nat. Rev. Drug. Discov. 2012, 11, 401–419. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.; Gralow, J.; Marx, R.E.; Hoff, A.O.; Schubert, M.M.; Huryn, J.M.; Toth, B.; Damato, K.; Valero, V. Practical Guidelines for the Prevention, Diagnosis, and Treatment of Osteonecrosis of the Jaw in Patients with Cancer. J. Oncol. Pract. 2006, 2, 7–14. [Google Scholar] [CrossRef]
- Bone, H.G.; Bolognese, M.A.; Yuen, C.K.; Kendler, D.L.; Wang, H.; Liu, Y.; San Martin, J. Effects of Denosumab on Bone Mineral Density and Bone Turnover in Postmenopausal Women. J. Clin. Endocrinol. Metab. 2008, 93, 2149–2157. [Google Scholar] [CrossRef] [Green Version]
- Wessel, J.H.; Dodson, T.B.; Zavras, A.I. Zoledronate, Smoking, and Obesity Are Strong Risk Factors for Osteonecrosis of the Jaw: A Case-Control Study. J. Oral Maxillofac. Surg. 2008, 66, 625–631. [Google Scholar] [CrossRef] [Green Version]
- Favia, G.; Tempesta, A.; Limongelli, L.; Crincoli, V.; Maiorano, E. Medication-Related Osteonecrosis of the Jaws: Considerations on a New Antiresorptive Therapy (Denosumab) and Treatment Outcome after a 13-Year Experience. Int. J. Dent. 2016, 2016, 1801676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Advisory Task Force on Bisphosphonate-Related Ostenonecrosis of the Jaws. American Association of Oral and Maxillofacial Surgeons Position Paper on Bisphosphonate-Related Osteonecrosis of the Jaws. J. Oral Maxillofac. Surg. 2007, 65, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Assael, L.A.; Landesberg, R.; Marx, R.E.; Mehrotra, B. American Association of Oral and Maxillofacial Surgeons Position Paper on Bisphosphonate-Related Osteonecrosis of the Jaws—2009 Update. J. Oral Maxillofac. Surg. 2009, 67, 2–12. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons Position Paper on Medication-Related Osteonecrosis of the Jaw—2014 Update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Hayashida, S.; Soutome, S.; Yanamoto, S.; Fujita, S.; Hasegawa, T.; Komori, T.; Kojima, Y.; Miyamoto, H.; Shibuya, Y.; Ueda, N.; et al. Evaluation of the Treatment Strategies for Medication-Related Osteonecrosis of the Jaws (MRONJ) and the Factors Affecting Treatment Outcome: A Multicenter Retrospective Study with Propensity Score Matching Analysis. J. Bone Miner. Res. 2017, 32, 2022–2029. [Google Scholar] [CrossRef] [Green Version]
- Schiodt, M.; Vadhan-Raj, S.; Chambers, M.S.; Nicolatou-Galitis, O.; Politis, C.; Coropciuc, R.; Fedele, S.; Jandial, D.; Zhang, J.; Ma, H.; et al. A Multicenter Case Registry Study on Medication-Related Osteonecrosis of the Jaw in Patients with Advanced Cancer. Support Care Cancer 2018, 26, 1905–1915. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, T.; Asai, K.; Fukuhara, S.; Uozumi, R.; Bessho, K. Effectiveness of Surgery and Hyperbaric Oxygen for Antiresorptive Agent-Related Osteonecrosis of the Jaw: A Subgroup Analysis by Disease Stage. PLoS ONE 2021, 16, e0244859. [Google Scholar] [CrossRef]
- Kaibuchi, N.; Hoshi, K.; Yamazaki, A.; Miyamoto-Sangu, N.; Akagi, Y.; Okamoto, T. The Progress of Medication-Related Osteonecrosis of the Jaw with Conservative Initial Treatment: A 12-Year Retrospective Study of 129 Patients. Bone Rep. 2021, 14, 101072. [Google Scholar] [CrossRef]
- Yoshida, T.; Watanabe, T.; Akizuki, S.; Okishio, Y.; Fujikawa, N.; Mori, A.; Fukuhara, S.; Asai, K.; Bessho, K. Adverse Events Caused by the Discontinuation of Anti-Resorptive Agents during Treatment for Anti-Resorptive Agent-Related Osteonecrosis of the Jaw: A Single-Center Cohort Study. J. Oral Maxillofac. Surg. Med. Pathol. 2021, 33, 115–119. [Google Scholar] [CrossRef]
- Favia, G.; Tempesta, A.; Limongelli, L.; Crincoli, V.; Maiorano, E. Medication-Related Osteonecrosis of the Jaw: Surgical or Non-Surgical Treatment? Oral Dis. 2018, 24, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Hadaya, D.; Soundia, A.; Freymiller, E.; Grogan, T.; Elashoff, D.; Tetradis, S.; Aghaloo, T.L. Nonsurgical Management of Medication-Related Osteonecrosis of the Jaws Using Local Wound Care. J. Oral Maxillofac. Surg. 2018, 76, 2332–2339. [Google Scholar] [CrossRef]
- Wei, L.-Y.; Kok, S.-H.; Lee, Y.-C.; Chiu, W.-Y.; Wang, J.-J.; Cheng, S.-J.; Chang, H.-H.; Lee, J.-J. Prognosis of Medication-Related Osteonecrosis of the Jaws in Metastatic Prostate Cancer Patients. Oral Dis. 2022, 28, 182–192. [Google Scholar] [CrossRef]
- Osaka, R.; Kato, H.; Hamada, Y.; Fujimoto, Y.; Mizusawa, N.; Watanabe, D.; Kaneko, A. Clinicostatistical Analyses of Medication-Related Osteonecrosis of the Jaws (MRONJ): Evaluation of the Treatment Method and Prognosis. Oral Sci. Int. 2021, 18, 184–192. [Google Scholar] [CrossRef]
- Ristow, O.; Rückschloß, T.; Bodem, J.; Berger, M.; Bodem, E.; Kargus, S.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Double-Layer Closure Techniques after Bone Surgery of Medication-Related Osteonecrosis of the Jaw-A Single Center Cohort Study. J. Cranio-Maxillofac. Surg. 2018, 46, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Coropciuc, R.G.; Grisar, K.; Aerden, T.; Schol, M.; Schoenaers, J.; Politis, C. Medication-Related Osteonecrosis of the Jaw in Oncological Patients with Skeletal Metastases: Conservative Treatment Is Effective up to Stage 2. Br. J. Oral Maxillofac. Surg. 2017, 55, 787–792. [Google Scholar] [CrossRef] [Green Version]
- El-Rabbany, M.; Lam, D.K.; Shah, P.S.; Azarpazhooh, A. Surgical Management of Medication-Related Osteonecrosis of the Jaw Is Associated With Improved Disease Resolution: A Retrospective Cohort Study. J. Oral Maxillofac. Surg. 2019, 77, 1816–1822. [Google Scholar] [CrossRef]
- Sánchez-Gallego Albertos, C.; Del Castillo Pardo de Vera, J.-L.; Viejo Llorente, A.; Cebrián Carretero, J.-L. Medication Related Osteonecrosis of the Jaws (MRONJ): Factors Related to Recurrence after Treatment with Surgery and Platelet Rich Plasma (PRP) Placement. Med. Oral Patol. Oral Cir. Bucal 2021, 26, e684–e690. [Google Scholar] [CrossRef]
- Akashi, M.; Wanifuchi, S.; Iwata, E.; Takeda, D.; Kusumoto, J.; Furudoi, S.; Komori, T. Differences between Osteoradionecrosis and Medication-Related Osteonecrosis of the Jaw. Oral Maxillofac. Surg. 2018, 22, 59–63. [Google Scholar] [CrossRef] [Green Version]
- Hallmer, F.; Andersson, G.; Götrick, B.; Warfvinge, G.; Anderud, J.; Bjørnland, T. Prevalence, Initiating Factor, and Treatment Outcome of Medication-Related Osteonecrosis of the Jaw-a 4-Year Prospective Study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 477–485. [Google Scholar] [CrossRef] [Green Version]
- Ristow, O.; Hürtgen, L.; Moratin, J.; Smielowski, M.; Freudlsperger, C.; Engel, M.; Hoffmann, J.; Rückschloß, T. A Critical Assessment of the Medication-Related Osteonecrosis of the Jaw Classification in Stage I Patients: A Retrospective Analysis. J. Korean Assoc. Oral Maxillofac. Surg. 2021, 47, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.; Ristow, O.; Pache, C.; Troeltzsch, M.; Fliefel, R.; Ehrenfeld, M.; Pautke, C. Fluorescence-Guided Surgery for the Treatment of Medication-Related Osteonecrosis of the Jaw: A Prospective Cohort Study. J. Craniomaxillofac. Surg. 2016, 44, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Kojima, Y.; Soutome, S.; Otsuru, M.; Hayashida, S.; Sakamoto, Y.; Sawada, S.; Umeda, M. Factors Exacerbating Clinical Symptoms and CT Findings in Patients with Medication-Related Osteonecrosis of the Jaw Receiving Conservative Therapy: A Multicenter Retrospective Study of 53 Cases. Int. J. Environ. Res. Public Health 2022, 19, 7854. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, T.; Kanai, I.; Basugi, A.; Miyata, Y.; Inoue, M.; Hamada, Y. The Assessment of Surgical and Non-Surgical Treatment of Stage II Medication-Related Osteonecrosis of the Jaw. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e788–e795. [Google Scholar] [CrossRef] [PubMed]
- Blatt, S.; Krüger, M.; Kämmerer, P.W.; Thiem, D.G.E.; Matheis, P.; Eisenbeiß, A.-K.; Wiltfang, J.; Al-Nawas, B.; Naujokat, H. Non-Interventional Prospective Observational Study of Platelet Rich Fibrin as a Therapy Adjunctive in Patients with Medication-Related Osteonecrosis of the Jaw. J. Clin. Med. 2022, 11, 682. [Google Scholar] [CrossRef]
- Ahrenbog, G.; Gottsauner, M.; Meier, J.K.; Ettl, T.; Reichert, T.E.; Klingelhöffer, C. Surgical Treatment of Advanced Medication-Related Osteonecrosis of the Jaws: Comparison of Soft Tissue Closure Techniques and Evaluation of Side Effects. J. Craniomaxillofac. Surg. 2020, 48, 896–901. [Google Scholar] [CrossRef]
- Mamilos, A.; Spörl, S.; Spanier, G.; Ettl, T.; Brochhausen, C.; Klingelhöffer, C. The First Quantitative Histomorphological Analyses of Bone Vitality and Inflammation in Surgical Specimens of Patients with Medication-Related Osteonecrosis of the Jaw. J. Oral Pathol. Med. 2021, 50, 76–84. [Google Scholar] [CrossRef]
- Moll, S.; Mueller, S.; Meier, J.K.; Reichert, T.E.; Ettl, T.; Klingelhöffer, C. Patients’ Quality of Life Improves after Surgical Intervention of Stage III Medication-Related Osteonecrosis of the Jaw. Oral Maxillofac. Surg. 2021, 25, 359–366. [Google Scholar] [CrossRef]
- Soutome, S.; Yanamoto, S.; Sumi, M.; Hayashida, S.; Kojima, Y.; Sawada, S.; Rokutanda, S.; Iwai, H.; Saito, T.; Umeda, M. Effect of Periosteal Reaction in Medication-Related Osteonecrosis of the Jaw on Treatment Outcome after Surgery. J. Bone Miner. Metab. 2021, 39, 302–310. [Google Scholar] [CrossRef]
- Fleisher, K.E.; Pham, S.; Raad, R.A.; Friedman, K.P.; Ghesani, M.; Chan, K.C.; Amintavakoli, N.; Janal, M.; Levine, J.P.; Glickman, R.S. Does Fluorodeoxyglucose Positron Emission Tomography With Computed Tomography Facilitate Treatment of Medication-Related Osteonecrosis of the Jaw? J. Oral Maxillofac. Surg. 2016, 74, 945–958. [Google Scholar] [CrossRef] [Green Version]
- Klingelhöffer, C.; Zeman, F.; Meier, J.; Reichert, T.E.; Ettl, T. Evaluation of Surgical Outcome and Influencing Risk Factors in Patients with Medication-Related Osteonecrosis of the Jaws. J. Craniomaxillofac. Surg. 2016, 44, 1694–1699. [Google Scholar] [CrossRef] [PubMed]
- Hauer, L.; Jambura, J.; Hrusak, D.; Chalupova, M.; Posta, P.; Rusnak, S.; Vyskocil, V. Surgical Therapy for Medication-Related Osteonecrosis of the Jaw in Osteoporotic Patients Treated with Antiresorptive Agents. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2020, 164, 100–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoefert, S.; Yuan, A.; Munz, A.; Grimm, M.; Elayouti, A.; Reinert, S. Clinical Course and Therapeutic Outcomes of Operatively and Non-Operatively Managed Patients with Denosumab-Related Osteonecrosis of the Jaw (DRONJ). J. Craniomaxillofac. Surg. 2017, 45, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Pichardo, S.E.C.; van Merkesteyn, J.P.R. Evaluation of a Surgical Treatment of Denosumab-Related Osteonecrosis of the Jaws. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Beaudouin, S.; Scailteux, L.-M.; Lefeuvre, C.; Gamby, R.; Cairon-Lejeune, S. Jaw Osteonecrosis in Patients Treated with Denosumab 120 Mg with Regular Dental Monitoring: 4-Year Retrospective Study. J. Oral Med. Oral Surg. 2021, 27, 47. [Google Scholar] [CrossRef]
- Ruggiero, S.L. Diagnosis and Staging of Medication-Related Osteonecrosis of the Jaw. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 479–487. [Google Scholar] [CrossRef]
- Francini, F.; Pascucci, A.; Francini, E.; Miano, S.T.; Bargagli, G.; Ruggiero, G.; Petrioli, R. Osteonecrosis of the Jaw in Patients with Cancer Who Received Zoledronic Acid and Bevacizumab. J. Am. Dent. Assoc. 2011, 142, 506–513. [Google Scholar] [CrossRef]
- Khan, A.A.; Morrison, A.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and Management of Osteonecrosis of the Jaw: A Systematic Review and International Consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar] [CrossRef]
- Lončar Brzak, B.; Horvat Aleksijević, L.; Vindiš, E.; Kordić, I.; Granić, M.; Vidović Juras, D.; Andabak Rogulj, A. Osteonecrosis of the Jaw. Dent. J. 2023, 11, 23. [Google Scholar] [CrossRef]
- Yarom, N.; Shapiro, C.L.; Peterson, D.E.; Van Poznak, C.H.; Bohlke, K.; Ruggiero, S.L.; Migliorati, C.A.; Khan, A.; Morrison, A.; Anderson, H.; et al. Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 2270–2290. [Google Scholar] [CrossRef]
- Straub, A.; Stapf, M.; Fischer, M.; Vollmer, A.; Linz, C.; Lâm, T.-T.; Kübler, A.; Brands, R.C.; Scherf-Clavel, O.; Hartmann, S. Bone Concentration of Ampicillin/Sulbactam: A Pilot Study in Patients with Osteonecrosis of the Jaw. Int. J. Environ. Res. Public Health 2022, 19, 14917. [Google Scholar] [CrossRef] [PubMed]
- Haviv, Y.; Geller, Z.; Mazor, S.; Sharav, Y.; Keshet, N.; Zadik, Y. Pain Characteristics in Medication-Related Osteonecrosis of the Jaws. Support Care Cancer 2021, 29, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Morishita, K.; Yamada, S.-I.; Kawakita, A.; Hashidume, M.; Tachibana, A.; Takeuchi, N.; Ohbayashi, Y.; Kanno, T.; Yoshiga, D.; Narai, T.; et al. Treatment Outcomes of Adjunctive Teriparatide Therapy for Medication-Related Osteonecrosis of the Jaw (MRONJ): A Multicenter Retrospective Analysis in Japan. J. Orthop. Sci. 2020, 25, 1079–1083. [Google Scholar] [CrossRef] [PubMed]
- Sim, I.-W.; Borromeo, G.L.; Tsao, C.; Hardiman, R.; Hofman, M.S.; Papatziamos Hjelle, C.; Siddique, M.; Cook, G.J.R.; Seymour, J.F.; Ebeling, P.R. Teriparatide Promotes Bone Healing in Medication-Related Osteonecrosis of the Jaw: A Placebo-Controlled, Randomized Trial. J. Clin. Oncol. 2020, 38, 2971–2980. [Google Scholar] [CrossRef]
- Liu, J.; Mattheos, N.; Deng, C.; Su, C.; Wang, Z.; Luo, N.; Tang, H. Management of Medication-Related Osteonecrosis of Jaw: Comparison between Icariin and Teriparatide in a Rat Model. J. Periodontol. 2021, 92, 149–158. [Google Scholar] [CrossRef]
- Hayashida, S.; Yanamoto, S.; Fujita, S.; Hasegawa, T.; Komori, T.; Kojima, Y.; Miyamoto, H.; Shibuya, Y.; Ueda, N.; Kirita, T.; et al. Drug Holiday Clinical Relevance Verification for Antiresorptive Agents in Medication-Related Osteonecrosis Cases of the Jaw. J. Bone Miner. Metab. 2020, 38, 126–134. [Google Scholar] [CrossRef]
- Campisi, G.; Bedogni, A.; Fusco, V. Raccomandazioni Clinico-Terapeutiche Sull’osteonecrosi delle Ossa Mascellari (ONJ) Farmaco-Relata e sua Prevenzione; New Digital Press: Palermo, Italy, 2020; ISBN 978-88-550-9147-3. [Google Scholar]
- Zheng, Y.; Dong, X.; Chen, S.; He, Y.; An, J.; Liu, M.; He, L.; Zhang, Y. Low-Level Laser Therapy Prevents Medication-Related Osteonecrosis of the Jaw-like Lesions via IL-1RA-Mediated Primary Gingival Wound Healing. BMC Oral Health 2023, 23, 14. [Google Scholar] [CrossRef]
- Gurav, S.; Dholam, K.P.; Singh, G.P. Treatment of Refractory Medicine Related Osteonecrosis of Jaw With Piezosurgical Debridement and Autologous Platelet Rich Fibrin: Feasibility Study. J. Craniofac. Surg. 2022, 33, e226–e230. [Google Scholar] [CrossRef]
- Contaldo, M.; Luzzi, V.; Ierardo, G.; Raimondo, E.; Boccellino, M.; Ferati, K.; Bexheti-Ferati, A.; Inchingolo, F.; Di Domenico, M.; Serpico, R.; et al. Bisphosphonate-Related Osteonecrosis of the Jaws and Dental Surgery Procedures in Children and Young People with Osteogenesis Imperfecta: A Systematic Review. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 556–562. [Google Scholar] [CrossRef]
- Eckardt, A.M.; Lemound, J.; Lindhorst, D.; Rana, M.; Gellrich, N.-C. Surgical Management of Bisphosphonate-Related Osteonecrosis of the Jaw in Oncologic Patients: A Challenging Problem. Anticancer Res. 2011, 31, 2313–2318. [Google Scholar] [CrossRef]
- Huang, H.; Zhao, N.; Li, Q.; Qiao, Q.; Zhang, J.; Guo, C.; Guo, Y. The Therapeutic Effectiveness Using Fluorescence-Guided Surgery for MRONJ. Biomed. Res. Int. 2022, 2022, 1650790. [Google Scholar] [CrossRef]
- Yoshiga, D.; Nakamichi, I.; Yamashita, Y.; Yamamoto, N.; Yamauchi, K.; Nogami, S.; Kaneuji, T.; Mitsugi, S.; Tanaka, K.; Kataoka, Y.; et al. Prognosis Factors in the Treatment of Bisphosphonate-Related Osteonecrosis of the Jaw-Prognostic Factors in the Treatment of BRONJ. J. Clin. Exp. Dent. 2014, 6, e22–e28. [Google Scholar] [CrossRef]
- Ristow, O.; Nehrbass, D.; Zeiter, S.; Arens, D.; Moratin, J.; Pautke, C.; Hoffmann, J.; Freudlsperger, C.; Otto, S. Differences between Auto-Fluorescence and Tetracycline-Fluorescence in Medication-Related Osteonecrosis of the Jaw—A Preclinical Proof of Concept Study in the Mini-Pig. Clin. Oral Investig. 2020, 24, 4625–4637. [Google Scholar] [CrossRef] [PubMed]
- Sarkarat, F.; Kalantar Motamedi, M.H.; Jahanbani, J.; Sepehri, D.; Kahali, R.; Nematollahi, Z. Platelet-Rich Plasma in Treatment of Zoledronic Acid-Induced Bisphosphonate-Related Osteonecrosis of the Jaws. Trauma Mon. 2014, 19, e17196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohn, D.-S.; Heo, J.-U.; Kwak, D.-H.; Kim, D.-E.; Kim, J.-M.; Moon, J.-W.; Lee, J.-H.; Park, I.-S. Bone Regeneration in the Maxillary Sinus Using an Autologous Fibrin-Rich Block with Concentrated Growth Factors Alone. Implant. Dent. 2011, 20, 389–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsani, E.; Bonazza, V.; Buffoli, B.; Nocini, P.F.; Albanese, M.; Zotti, F.; Inchingolo, F.; Rezzani, R.; Rodella, L.F. Beneficial Effects of Concentrated Growth Factors and Resveratrol on Human Osteoblasts In Vitro Treated with Bisphosphonates. Biomed. Res. Int. 2018, 2018, 4597321. [Google Scholar] [CrossRef] [Green Version]
- Ehrenfest, D.; Bielecki, T.; Mishra, A.; Borzini, P.; Inchingolo, F.; Sammartino, G.; Rasmusson, L.; Everts, P. In Search of a Consensus Terminology in the Field of Platelet Concentrates for Surgical Use: Platelet-Rich Plasma (PRP), Platelet-Rich Fibrin (PRF), Fibrin Gel Polymerization and Leukocytes. Curr. Pharm. Biotechnol. 2011, 13, 1131–1137. [Google Scholar] [CrossRef] [Green Version]
- Dohan Ehrenfest, D.M.; Bielecki, T.; Jimbo, R.; Barbé, G.; Del Corso, M.; Inchingolo, F.; Sammartino, G. Do the Fibrin Architecture and Leukocyte Content Influence the Growth Factor Release of Platelet Concentrates? An Evidence-Based Answer Comparing a Pure Platelet-Rich Plasma (P-PRP) Gel and a Leukocyte- and Platelet-Rich Fibrin (L-PRF). Curr. Pharm. Biotechnol. 2012, 13, 1145–1152. [Google Scholar] [CrossRef]
- Mijiritsky, E.; Assaf, H.D.; Kolerman, R.; Mangani, L.; Ivanova, V.; Zlatev, S. Autologous Platelet Concentrates (APCs) for Hard Tissue Regeneration in Oral Implantology, Sinus Floor Elevation, Peri-Implantitis, Socket Preservation, and Medication-Related Osteonecrosis of the Jaw (MRONJ): A Literature Review. Biology 2022, 11, 1254. [Google Scholar] [CrossRef]
- Wisniewska, L.M.; Dohan Ehrenfest, D.M.; Galindo-Moreno, P.; Segovia, J.D.; Inchingolo, F.; Wang, H.-L.; Fernandes-Cruz, M. Molecular, Cellular and Pharmaceutical Aspects of Biomaterials in Dentistry and Oral and Maxillofacial Surgery. An Internationalization of Higher Education and Research Perspective. Curr. Pharm. Biotechnol. 2017, 18, 10–18. [Google Scholar] [CrossRef]
- Del Corso, M.; Vervelle, A.; Simonpieri, A.; Jimbo, R.; Inchingolo, F.; Sammartino, G.; Dohan Ehrenfest, D.M. Current Knowledge and Perspectives for the Use of Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Oral and Maxillofacial Surgery Part 1: Periodontal and Dentoalveolar Surgery. Curr. Pharm. Biotechnol. 2012, 13, 1207–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsani, E.; Buffoli, B.; Bonazza, V.; Brunelli, G.; Monini, L.; Inchingolo, F.; Ballini, A.; Rezzani, R.; Rodella, L.F. In Vitro Effects of Concentrated Growth Factors (CGF) on Human SH-SY5Y Neuronal Cells. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Bonazza, V.; Borsani, E.; Buffoli, B.; Parolini, S.; Inchingolo, F.; Rezzani, R.; Rodella, L.F. In Vitro Treatment with Concentrated Growth Factors (CGF) and Sodium Orthosilicate Positively Affects Cell Renewal in Three Different Human Cell Lines. Cell Biol. Int. 2018, 42, 353–364. [Google Scholar] [CrossRef] [PubMed]
- Rusilas, H.; Balčiūnaitė, A.; Žilinskas, J. Autologous Platelet Concentrates in Treatment of Medication Related Osteonecrosis of the Jaw. Stomatologija 2020, 22, 23–27. [Google Scholar]
- Dohan Ehrenfest, D.M.; Bielecki, T.; Del Corso, M.; Inchingolo, F.; Sammartino, G. Shedding Light in the Controversial Terminology for Platelet-Rich Products: Platelet-Rich Plasma (PRP), Platelet-Rich Fibrin (PRF), Platelet-Leukocyte Gel (PLG), Preparation Rich in Growth Factors (PRGF), Classification and Commercialism. J. Biomed. Mater. Res. A 2010, 95, 1280–1282. [Google Scholar] [CrossRef]
- Qiao, J.; An, N.; Ouyang, X. Quantification of Growth Factors in Different Platelet Concentrates. Platelets 2017, 28, 774–778. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Sammartino, G.; Charrier, J.-B. Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Human Cell Cultures: Growth Factor Release and Contradictory Results. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 418–421; author reply 421–422. [Google Scholar] [CrossRef]
- Aljohani, S.; Fliefel, R.; Ihbe, J.; Kühnisch, J.; Ehrenfeld, M.; Otto, S. What Is the Effect of Anti-Resorptive Drugs (ARDs) on the Development of Medication-Related Osteonecrosis of the Jaw (MRONJ) in Osteoporosis Patients: A Systematic Review. J. Craniomaxillofac. Surg. 2017, 45, 1493–1502. [Google Scholar] [CrossRef]
- Simonpieri, A.; Del Corso, M.; Vervelle, A.; Jimbo, R.; Inchingolo, F.; Sammartino, G.; Dohan Ehrenfest, D.M. Current Knowledge and Perspectives for the Use of Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Oral and Maxillofacial Surgery Part 2: Bone Graft, Implant and Reconstructive Surgery. Curr. Pharm. Biotechnol. 2012, 13, 1231–1256. [Google Scholar] [CrossRef]
- Giudice, A.; Barone, S.; Giudice, C.; Bennardo, F.; Fortunato, L. Can Platelet-Rich Fibrin Improve Healing after Surgical Treatment of Medication-Related Osteonecrosis of the Jaw? A Pilot Study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 390–403. [Google Scholar] [CrossRef]
- Asaka, T.; Ohga, N.; Yamazaki, Y.; Sato, J.; Satoh, C.; Kitagawa, Y. Platelet-Rich Fibrin May Reduce the Risk of Delayed Recovery in Tooth-Extracted Patients Undergoing Oral Bisphosphonate Therapy: A Trial Study. Clin. Oral Investig. 2017, 21, 2165–2172. [Google Scholar] [CrossRef]
- Adell, R.; Eriksson, B.; Lekholm, U.; Brånemark, P.I.; Jemt, T. Long-Term Follow-up Study of Osseointegrated Implants in the Treatment of Totally Edentulous Jaws. Int. J. Oral Maxillofac. Implants 1990, 5, 347–359. [Google Scholar]
- Lopez-Jornet, P.; Sanchez Perez, A.; Amaral Mendes, R.; Tobias, A. Medication-Related Osteonecrosis of the Jaw: Is Autologous Platelet Concentrate Application Effective for Prevention and Treatment? A Systematic Review. J. Craniomaxillofac. Surg. 2016, 44, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Gallesio, G.; Mozzati, M. Autologous Platelet Concentrates for Bisphosphonate-Related Osteonecrosis of the Jaw Treatment and Prevention. A Systematic Review of the Literature. Eur. J. Cancer 2015, 51, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Curi, M.M.; Cossolin, G.S.I.; Koga, D.H.; Zardetto, C.; Christianini, S.; Feher, O.; Cardoso, C.L.; dos Santos, M.O. Bisphosphonate-Related Osteonecrosis of the Jaws--an Initial Case Series Report of Treatment Combining Partial Bone Resection and Autologous Platelet-Rich Plasma. J. Oral Maxillofac. Surg. 2011, 69, 2465–2472. [Google Scholar] [CrossRef] [PubMed]
- Bocanegra-Pérez, S.; Vicente-Barrero, M.; Knezevic, M.; Castellano-Navarro, J.M.; Rodríguez-Bocanegra, E.; Rodríguez-Millares, J.; Pérez-Plasencia, D.; Ramos-Macías, A. Use of Platelet-Rich Plasma in the Treatment of Bisphosphonate-Related Osteonecrosis of the Jaw. Int. J. Oral Maxillofac. Surg. 2012, 41, 1410–1415. [Google Scholar] [CrossRef] [PubMed]
- Oneto, P.; Zubiry, P.R.; Schattner, M.; Etulain, J. Anticoagulants Interfere With the Angiogenic and Regenerative Responses Mediated by Platelets. Front. Bioeng. Biotechnol. 2020, 8, 223. [Google Scholar] [CrossRef] [Green Version]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.J.; Mouhyi, J.; Gogly, B. Platelet-Rich Fibrin (PRF): A Second-Generation Platelet Concentrate. Part I: Technological Concepts and Evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Charrier, J.-B. Selecting a Relevant in Vitro Cell Model for Testing and Comparing the Effects of a Choukroun’s Platelet-Rich Fibrin (PRF) Membrane and a Platelet-Rich Plasma (PRP) Gel: Tricks and Traps. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 409–411; author reply 411–413. [Google Scholar] [CrossRef]
- Miron, R.J.; Zucchelli, G.; Pikos, M.A.; Salama, M.; Lee, S.; Guillemette, V.; Fujioka-Kobayashi, M.; Bishara, M.; Zhang, Y.; Wang, H.-L.; et al. Use of Platelet-Rich Fibrin in Regenerative Dentistry: A Systematic Review. Clin. Oral Investig. 2017, 21, 1913–1927. [Google Scholar] [CrossRef]
- Nørholt, S.E.; Hartlev, J. Surgical Treatment of Osteonecrosis of the Jaw with the Use of Platelet-Rich Fibrin: A Prospective Study of 15 Patients. Int. J. Oral Maxillofac. Surg. 2016, 45, 1256–1260. [Google Scholar] [CrossRef]
- Inchingolo, F.; Cantore, S.; Dipalma, G.; Georgakopoulos, I.; Almasri, M.; Gheno, E.; Motta, A.; Marrelli, M.; Farronato, D.; Ballini, A.; et al. Platelet Rich Fibrin in the Management of Medication-Related Osteonecrosis of the Jaw: A Clinical and Histopathological Evaluation. J. Biol. Regul. Homeost. Agents 2017, 31, 811–816. [Google Scholar] [PubMed]
- Yüce, M.O.; Adalı, E.; Işık, G. The Effect of Concentrated Growth Factor (CGF) in the Surgical Treatment of Medication-Related Osteonecrosis of the Jaw (MRONJ) in Osteoporosis Patients: A Randomized Controlled Study. Clin. Oral Investig. 2021, 25, 4529–4541. [Google Scholar] [CrossRef]
- Lin, S.-L.; Wu, S.-L.; Tsai, C.-C.; Ko, S.-Y.; Chiang, W.-F.; Yang, J.-W. The Use of Solid-Phase Concentrated Growth Factors for Surgical Defects in the Treatment of Dysplastic Lesions of the Oral Mucosa. J. Oral Maxillofac. Surg. 2016, 74, 2549–2556. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, R.; Young, H.; Patel, D.; Kwok, J. The Role of Piezoelectric Surgery and Platelet-Rich Fibrin in Treatment of ORN and MRONJ: A Clinical Case Series. Oral Surg. 2018, 11, 136–143. [Google Scholar] [CrossRef]
- Giudice, A.; Antonelli, A.; Muraca, D.; Fortunato, L. Usefulness of Advanced-Platelet Rich Fibrin (A-PRF) and Injectable-Platelet Rich Fibrin (i-PRF) in the Management of a Massive Medication-Related Osteonecrosis of the Jaw (MRONJ): A 5-Years Follow-up Case Report. Indian J. Dent. Res. 2020, 31, 813–818. [Google Scholar] [CrossRef]
- Pavlíková, G.; Foltán, R.; Horká, M.; Hanzelka, T.; Borunská, H.; Sedý, J. Piezosurgery in Oral and Maxillofacial Surgery. Int. J. Oral Maxillofac. Surg. 2011, 40, 451–457. [Google Scholar] [CrossRef]
- Danza, M.; Guidi, R.; Carinci, F. Comparison between Implants Inserted into Piezo Split and Unsplit Alveolar Crests. J. Oral Maxillofac. Surg. 2009, 67, 2460–2465. [Google Scholar] [CrossRef]
- Blus, C.; Szmukler-Moncler, S.; Giannelli, G.; Denotti, G.; Orrù, G. Use of Ultrasonic Bone Surgery (Piezosurgery) to Surgically Treat Bisphosphonate-Related Osteonecrosis of the Jaws (BRONJ). A Case Series Report with at Least 1 Year of Follow-Up. Open Dent. J. 2013, 7, 94–101. [Google Scholar] [CrossRef]
- Patel, V.; Patel, D.; McGurk, M.; Sproat, C.; Kwok, J. Flapless Piezoelectric Surgery in the Management of Jaw Necrosis–a Case Series. Oral Surg. 2017, 10, 228–234. [Google Scholar] [CrossRef]
- Sharma, D.; Hamlet, S.; Petcu, E.; Ivanovski, S. Animal Models for Bisphosphonate-Related Osteonecrosis of the Jaws--an Appraisal. Oral Dis. 2013, 19, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Allegra, A.; Alonci, A.; Penna, G.; Granata, A.; Nastro Siniscalchi, E.; Oteri, G.; Loddo, S.; Teti, D.; Cicciù, D.; De Ponte, F.S.; et al. Bisphosphonates Induce Apoptosis of Circulating Endothelial Cells in Multiple Myeloma Patients and in Subjects with Bisphosphonate-Induced Osteonecrosis of the Jaws. Acta Haematol. 2010, 124, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.F.; Hussein, A.I.; Al-Awadhi, B.A.; Hogan, D.E.; Matsubara, H.; Al-Alq, Z.; Fitch, J.; Andre, B.; Hosur, K.; Gerstenfeld, L.C. Vascular Development during Distraction Osteogenesis Proceeds by Sequential Intramuscular Arteriogenesis Followed by Intraosteal Angiogenesis. Bone 2012, 51, 535–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eastgate, J.A.; Symons, J.A.; Wood, N.C.; Grinlinton, F.M.; di Giovine, F.S.; Duff, G.W. Correlation of Plasma Interleukin 1 Levels with Disease Activity in Rheumatoid Arthritis. Lancet 1988, 2, 706–709. [Google Scholar] [CrossRef]
- Carlevaro, M.F.; Cermelli, S.; Cancedda, R.; Descalzi Cancedda, F. Vascular Endothelial Growth Factor (VEGF) in Cartilage Neovascularization and Chondrocyte Differentiation: Auto-Paracrine Role during Endochondral Bone Formation. J. Cell Sci. 2000, 113 Pt 1, 59–69. [Google Scholar] [CrossRef]
- Pushalkar, S.; Li, X.; Kurago, Z.; Ramanathapuram, L.V.; Matsumura, S.; Fleisher, K.E.; Glickman, R.; Yan, W.; Li, Y.; Saxena, D. Oral Microbiota and Host Innate Immune Response in Bisphosphonate-Related Osteonecrosis of the Jaw. Int. J. Oral Sci. 2014, 6, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.S.; Thompson, A.Y.; Heidaran, M.A.; Poser, J.W.; Spiro, R.C. An Osteoconductive Collagen/Hyaluronate Matrix for Bone Regeneration. Biomaterials 1999, 20, 1097–1108. [Google Scholar] [CrossRef]
- Laurent, T.C.; Laurent, U.B.; Fraser, J.R. Functions of Hyaluronan. Ann. Rheum. Dis. 1995, 54, 429–432. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; Cantore, S.; Capodiferro, S.; Grassi, F.R. Esterified Hyaluronic Acid and Autologous Bone in the Surgical Correction of the Infra-Bone Defects. Int. J. Med. Sci. 2009, 6, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Sharma, D.; Hamlet, S.; Vaquette, C.; Petcu, E.B.; Ramamurthy, P.; Ivanovski, S. Local Delivery of Hydrogel Encapsulated Vascular Endothelial Growth Factor for the Prevention of Medication-Related Osteonecrosis of the Jaw. Sci. Rep. 2021, 11, 23371. [Google Scholar] [CrossRef]
- Li, Y.; Toole, B.P.; Dealy, C.N.; Kosher, R.A. Hyaluronan in Limb Morphogenesis. Dev. Biol. 2007, 305, 411–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Experimental-Morphological Study of the Anti-Inflammatory Action of Ozone-Perfluorane Complex Application. Available online: https://pubmed.ncbi.nlm.nih.gov/18454111/ (accessed on 12 February 2023).
- Agrillo, A.; Petrucci, M.T.; Tedaldi, M.; Mustazza, M.C.; Marino, S.M.F.; Gallucci, C.; Iannetti, G. New Therapeutic Protocol in the Treatment of Avascular Necrosis of the Jaws. J. Craniofac. Surg. 2006, 17, 1080–1083. [Google Scholar] [CrossRef] [PubMed]
- Agrillo, A.; Ungari, C.; Filiaci, F.; Priore, P.; Iannetti, G. Ozone Therapy in the Treatment of Avascular Bisphosphonate-Related Jaw Osteonecrosis. J. Craniofac. Surg. 2007, 18, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Agrillo, A.; Sassano, P.; Rinna, C.; Priore, P.; Iannetti, G. Ozone Therapy in Extractive Surgery on Patients Treated with Bisphosphonates. J. Craniofac. Surg. 2007, 18, 1068–1070. [Google Scholar] [CrossRef] [PubMed]
- Petrucci, M.T.; Gallucci, C.; Agrillo, A.; Mustazza, M.C.; Foà, R. Role of Ozone Therapy in the Treatment of Osteonecrosis of the Jaws in Multiple Myeloma Patients. Haematologica 2007, 92, 1289–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ripamonti, C.I.; Cislaghi, E.; Mariani, L.; Maniezzo, M. Efficacy and Safety of Medical Ozone (O(3)) Delivered in Oil Suspension Applications for the Treatment of Osteonecrosis of the Jaw in Patients with Bone Metastases Treated with Bisphosphonates: Preliminary Results of a Phase I-II Study. Oral Oncol. 2011, 47, 185–190. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Articles screening strategy | KEYWORDS: (denosumab OR bevacizumab OR adalimumab OR romosozumab) AND osteonecrosis AND (treatment OR therapy) AND jaw |
| Boolean Indicators: (“A” AND “B”) | |
| Timespan: from 8 January 2006 to 8 January 2023 | |
| Electronic Database: PubMed, Cochrane, Scopus, Web of Science, and Embase |
| Authors (Year) | Study Design | MRONJ-Stage (n. Patients) | N. Total Patients (n. Lesions) and Type of Primary Disease (n. Patients) | Average Age (Years) | Types of Antiresorptive Drugs (n. Patients) and Duration of Therapy (Months, Years) | Description of Treatment (n. Patients) | Follow-Up (Months) | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Hayashida, S. (2017) [26] | R | I and II (356) III (71) | 427 Neoplasms (236) Osteoporosi (191) |
CT: 72.7 ± 10.7 ST: 73.2 ± 10.3 |
DB (107) BP (320) for 28.8 months | CT (236): antiseptic mouth rinse, systemic antimicrobial agent, or debridement. ST (191): conservative surgery, removal of only the necrotic bone; extensive surgery, removal of the necrotic and surrounding bone; marginal mandibulectomy or partial maxillectomy. | 15 months | Better outcome in low-dose antiresorptive agent and ST. Better outcome of extensive ST surgery vs. CT. According to multivariate analysis, 4 variables are significantly correlated with treatment outcome: high-dose administration of an antiresorptive agent, serum albumin level, discontinuing drug, and surgical treatment. |
| Schiodt. et al. (2017) [27] | P | I (86) II (191) III (34) N.R. (9) | 327 Neoplasms (327) | 67 | DB (63) for 15.7 months DB + BP (69) for 40 months BP (196) for 26.2 months | ST (102, 31%): debridement, sequestromy, resection with or without jaw reconstruction, curettage, and teeth extraction. CT (300, 92%): antibiotics, oral rinses, analgesics, and antifungal/antimycotic. | 11 months | Patients exposed to both DB and BP did not present with higher proportions of stage III ONJ or severe symptoms. Rates of associated local oral risk factors (such as tooth extractions) were similar in patients with combined exposure to DB and BP vs. those exposed to single agent antiresorptive. Patients that discontinued antiresorptive treatment between baseline and 3 months had a higher percentage of stage III MRONJ |
| Watanabe (2021) [28] | R | II (206) III (46) | 252 Neoplasms (133) Osteoporosis (119) | 71.2 ± 9.9 |
DB (46) for 81.7 months BP (206) for 18.3 months | 138 (54.8%) underwent surgery, and 143 (56.7%) received HBO therapy. | ≥3 months | In the univariable analysis, therapeutic effect of surgery in both stage II and III vs. therapeutic effect of HBO in stage II. In the multivariable analysis for stage II, stronger association with healing of extensive surgery vs. conservative surgery. ≥46 sessions of HBO therapy less associated with healing vs. non-HBO therapy. |
| Favia (2016) [21] | R | I: 23 Ii: 187 III: 101 | 244 (322) Neoplasms (172) Osteoporotic (72) | N.R. | DB (13) DB + BP (3) BP (228) | ST based on the dimensional staging Stage I: surgical debridement; stage II: small open-access surgery with piezosurgery of bone margins; stage III: wide open-access surgery with extensive bone resection and piezosurgery of bone margins. | 16 months | Dmab-MRONJ is in stage II or III, requiring a more or less invasive surgical approach. Complete clinical and radiological healing in 86.9% of lesions, recurrence in 13.1% recurred (in patients who could not interrupt chemotherapy, steroids, and/or antiresorptive drugs). |
| Kaibuchi (2021) [29] | R | I (26) II (76) III (27) | 129 Neoplasm (72) Osteoporosis (57) | 74.3 ±11.5 | DB (40) BP (89) | CT (71): mouth rinse (saline or povidone-iodine) and systemic antibiotics CT + ST (58): removal of sequestrum | 60 months | Cure rate higher in patients with osteoporosis vs. in those with cancer and in patients who had separation of sequestrum vs. in those who did not. |
| Yoshida T. et al. (2021) [30] | R | I (13) II (91) III (19) | 123 osteoporotis: (123) | 75.1 ± 8.4 | DB (11) for 8.9 months BP (112) for 91.1 months | ST: 82 (66.7%) CT: 41 (33%) | >3 months | ARONJ is frequently located in the mandible (55.3%), and the most frequent initiating event is periodontitis (42.3%). The most common type of ARONJ is BRONJ (91.1%). Most patients continued the ARA therapy (80.5%). No significant difference in the healing rates between the continued group and discontinued group. |
| Favia (2018) [31] | R | I (11 lesions) II (65 lesions) III (55 lesions) | 106 (131) Neoplasm (95) Osteporosis (36) |
ST: 70.2 CT: 71 | DB (20) DB + BP (7) BP (103) | ST (85 patients, 107 lesions): perioperative antibiotics, surgical removal of the necrotic bone, from simple surgical debridement for smaller MRONJ to extensive bone resection for larger lesions. CT (21 patients, 24 lesions): chlorhexidine, periodic dental checks, systemic antibiotic, monthly low-level laser therapy, and removal of bone sequestrum. | 12 months | Complete healing in all the surgically treated lesions showed, except for 13.5% of the lesions (from stage III to stage I). Stabilization without complete healing in all the lesions with conservative treatment |
| Hadaya (2018) [32] | R | I (47) II (32) III (4) | 106 Neoplasm (89) Osteoporosis (34) | 71.7 | DB (17) BP (98) for 5.5, 3.7, and 4.8 years | Local wound care: mechanical vigorous debridement and cleaning of exposed bone, oral antibacterial solution (chlorhexidine), and antibiotics. | 24 months | Complete disease resolution in 71% of lesions, disease improvement in 22%. Association of wound care score with disease resolution and time to resolution. No effect on resolution of demographics, anatomic site, condition, and type and time of antiresorptive treatment. |
| Wei et al. (2022) [33] | R | I (29) II and III (87) | 95 (122) Prostatic cancer (95) | 75.17 ± 8.49 | DB (42) DB + BP (17) BP (57) for 18 months | Stage I: conservative treatment with chlorhexidine mouth rinse. Stage II: chlorhexidine mouth rinse, Antibiotics, and/or analgesics. Stage III: superficial debridement, sequestrectomy, or bone resection. | 12 months | Cumulative response rate of patients treated with DB is 70.5%. DB, pretreatment level of CTX > 150 pg/mL, and anemia are independent prognostic factors of MRONJ in a multivariate analysis. |
| Osaka (2021) [34] | R | I (15) II (51) III (22) | 88 Neoplasms (15) Osteoporosis (73) | 80.5 ± 6.7 | DB: 28 BP: 60 (for 49.1± 33.4) | CT: antimicrobial mouthwash, systemic antimicrobials, or debridement of bony sequestra. ST: Conservative surgery: removal of necrotic bone area. Extensive surgery: removal of the necrotic and surrounding bone, marginal mandibulectomy, or partial maxillectomy. | 23 months | According to univariate analysis, 3 variables significantly correlated with prognoses: sex, dosage, and the treatment method. According to multivariate analysis, 2 variables significantly correlated with the prognosis: high-dose administration of an antiresorptive agent. |
| Ristow (2018) [35] | R | I (31) II (26) III (11) | 87 (104) Neoplasms (79) Osteoporosis (8) | 66.25± 9.58 | DB (33) DB + BP (12) BP (42) for 50.37 ± 32.55 months | Mylohyoideus muscle flap (MMF) for the lower jaw: 57 patients Pedicled buccal fat flap (BFF) for the upper jaw; 30 patients | 8 months | Mucosal integrity in 88.0% (44/50) of patients in the MMF group and 93.1% (27/29) of patients in the BFF group. No serious side effects were reported. Better outcome of stage I and II vs. stage III. |
| Coropciuc (2017) [36] | R | I (57) II (47) III (5) | 79 (109) Neoplasms (79) | 70 | DB (43) BP (36) | ST: minimally invasive approaches (sequestrectomy, debridement of soft tissue, and application of leucocyte and PRF) CT: oral rinses and antibiotics | ≤24 months | Complete healing and resolution of disease in 38/57 stage I lesions, 30/47 stage II lesions, and 3/5 stage III lesions. Improvement of symptoms in 16/47 stage II lesions and 2/5 stage III lesions. Fifteen of the stage I lesions and one of the stage II lesions failed to respond. |
| El-Rabbany (2019) [37] | R | I (15) II (46) III (17) | 78 Neoplasms (12) ( Osteoporosi (66) | 77.2 | DB (17) for 5 years BP (61) for 5 years | ST (56): debridement, curettage, sequestrectomy, cauterization, and resection. CT (22): local and/or systemic antimicrobial therapy, hyperbaric oxygen therapy, pentoxifylline, and teriparatide. | ST: 15.5 months CT: 11 months | Disease resolution in 39 ST patients (70%) vs. 8 CT patients (36%). ST was associated with disease resolution vs. CT alone, after adjustment for age, duration of antiresorptive or antiangiogenic therapy, whether the antiresorptive or antiangiogenic agents were used for oncologic purposes, and the stage of MRONJ at initial presentation. |
| Sánchez-Gallego Albertos (2021) [38] | R | II (4) II (52) III (14) | 70 Neoplasms (36) Osteoporosis (34) | 50–70 | DB (10) BP (60) for 6–12 months | Surgical treatment: resection of necrotic bone, sequestrae and refreshing bone margins with a drill, extraction of the teeth if they were near the necrotic bone, and PRP placement. | 2–52 months | More recurrence (18.6%) in breast cancer patients, smokers, and patients that had been administered zoledronic acid. Smoke is the only independent risk factor. |
| Akashi (2018) [39] | R | I (17) II (28) III (15) | 61 MRONJ Neoplasms (28) Osteporosis (33) 27 ORN |
74 MRONJ 68 ORN |
DB (10) DB + BP (10) BP (41) | CT (14) Minimal debridement (1) ST (1): resection with or without reconstruction. | N.R. | In MRONJ group: higher median age, higher nr. of females, use of steroids, history of pain, periosteal reaction, and tooth extraction. Minimal debridement was significantly performed in the MBROJ group. Surgical resection was performed in the ORN group. |
| Hallmer F. et al. (2018) [40] | P | I (10) II (36) III (9) | 55 (55) Neoplasms (24) Osteoporosis (31) | 63.6 (M)- 73.1 (F) | DB (12) DB + BP (11) BP (32) | ST was sequestrectomy in patients without progressive bone disease or block resection patients with progressive bone disease with ongoing bone destruction. | 15.8 months | Prevalence of MRONJ is 3.64% in those on high-dose DB. Periodontal disease preceded development of MRONJ in 41 patients. Remission or healing in 80% of patients treated with sequestrectomy and in 92.5% of patients treated with block resection. |
| Ristow O et al. (2021) [41] | R | I: 86 | 55 (86) Neoplasm (46) Osteoporosis (9) |
68.2 ± 8.5 (F) 72.5 ± 10.4 (M) | BP (24) DB (25) DV + BP (5) for 49.3 ± 41.5 months | Surgical treatment: VELscope system Vx. Bone resection performed until the bright fluorescence of healthy bone was observed. Visible bone group (46 lesions): bone visibly exposed to the oral cavity. Probable bone group (40 lesions): could be probed to bone through the sinus tract. | ≤8 week | Intraoperatively, the necrotic lesions were significantly larger vs. preoperative mucosal lesions in both groups. There is a significant but very weak relationship between the extent of the mucosal lesions and the necrotic bone area. |
| Otto Sven (2016) [42] | P | I (4) II (42) III (8) | 54 Oncologic (45) Osteoporotic (9) | 71.4 ± 9.2 | DB (3) DB + BP (47) BP (4) for 46.3 months | Fluorescence-guided surgery: complete removal of necrotic bone, monitored using the visually enhanced lesion scope (Velscope), followed by smoothening sharp bony edges and meticulous wound closure. | 12.9 months | Intact mucosa in absence of exposed bone, pain, or signs of infection in 47/54 patients (87%) and in 56/65 lesions (86.2%) after first surgery. In 4 patients with 6 lesions, a second fluorescence-guided surgery was necessary. In total, 51 of 54 patients (94.4%) and 62 of 65 lesions (95.4%) showed complete mucosal healing. |
| Kojima Y. (2022) [43] | R | I (9) II (30) III (14) | 53 Neoplasms (33) Osteoporosis (22) | 74.9 ± 11.9 | DB (16) DB + BP (5) BP (32) for 47.0 ± 33.9 months | CT: oral hygiene guidance, antibacterial mouthwash, local lavage, administration of oral antibiotics, removal of mobile segments of bony sequestrum, and extraction of symptomatic teeth. | 729 ± 494 days | Clinical symptoms of 15 (28.3%) disappeared or improved while worsening was observed in 6 (11.3%). Enlargement of the osteolytic lesion occurred in 17 (32.1%) patients. CT is successful in 12 (22.6%) patients and unsuccessful in 41 patients (77.4%). Patients with stage III MRONJ have worse outcomes. The MRONJ stage and primary disease are not associated with the enlargement of osteolysis on the radiological images. A periosteal reaction on radiological examination is correlated with poor comprehensive treatment outcomes. |
| Eguchi (2017) [44] | R | II (52) | 52 Neoplasm (35) Osteoporosis (17) | CT: 74.8 ± 10.3 ST: 72.3 ± 11.3 | DB +/− BP (38) BP (14) | CT (24): debridement, systemic antibiotics, analgesics, and incisional drainages. ST (28): necrotic bone resection. | 6 months | CT: success in 8/24 pts (33.3%) ST: success in 25/28 pts (89.3%) |
| Blatt (2022) [45] | P | I (41) II (10) III (1) | 52 Neoplasm (52) | 71.5 ± 8.6 | N.R. | Arm A: resection of necrotic bone and fistulas; sufficient, vascularized, and mechanically stable wound coverage. Arm B: surgical treatment + PRF membrane on the decorticated bone before covering. | 6 weeks | Dehiscence and mucosal integrity after surgery in 16 cases (30.76%). No significant differences in VAS score, PWAT score, and IPR wound healing score. |
| Ahrenbog (2020) [46] | P | III | 44 Neoplasms (37) Osteporosis (7) | 68.1 | DB (4) DB + BP (8) BP (32) for 56.4 months | ST: removal of the resected bone, sharp bone edges, and the surface were smoothed till visible bleeding was reached. Afterward, wound closure was performed by using different techniques (mylohyoid muscle flap and buccal fat flap). | 13.2 months | Relapses in 12 cases and mucosal integrity in 38. Cases treated with the muscle or fat flap showed better results regarding the recurrence rate and soft tissue healing. Pain level was reduced significantly. Partial hypoesthesia of the lip arose in 18 cases. |
| Mamilos (2021) [47] | P | III (44) | 44 Neoplasm (22) Osteoporosis (22) | 68.1 | DB (4) DB + BP (8) BP (32) | ST: necrotic bone area resection or continuity resection of the mandibular. Analysis of CRP and leukocytes at baseline. | 13.2 months | The stage of chronic inflammation is correlated with the amount of vital bone and the success of surgery. If acute inflammation is dominant, chronic inflammation areas are found less, while necrotic areas are observed more. The risk of relapses, wound healing disorders, and the level of CRP are elevated if acute inflammation is severe or moderate. |
| Moll (2021) [48] | P | III (43) | 43 Neoplasm (36) Osteoporosis (7) | 68 | DB (13) DB + BP (9) BP (39) for ≥63/<63 months | Surgical treatment: necrotic bone area resection, perioperative, and antimicrobial mouth rinse with chlorhexidine. | 21.86 weeks | Significant improvement of EORTC QoL-H&N35 and the Oral Health Impact Factor-G14 (OHIP-G14) questionnaire |
| Soutome (2020) [49] | R | II (18) III (20) | 38 Neoplasms (17) Osteoporosis (21) | 74.3 |
DB (14) BP (24) for 4 years | 38 MRONJ patients with PR Type 1: new bone is formed parallel to the mandible, and no gap was evident between the mandible and new bone; type 2: new bone is formed parallel to the mandible, and a gap was evident between them; type 3: an irregular shape. Segmental mandibulectomy (9) Marginal mandibulectomy (29) | ≥3 months | Inflammatory tissue in the area visualized as a gap on CT at histological examinations. Presence of bacteria in the type 2 or type 3 PR at bacteriological examination. Complete cure in 21 of 38 (55.3%) patients, lower than the cure rate of 73.4% in 143 patients without PR. Cure rate lower in cases with type 3 PR or with persistent osteolysis. |
| Fleisher (2016) [50] | R | II (31) III (3) | 31 (33) Neoplasms (31) | 64 |
DB (10) DB + BP (3) BP (18) for 47 months | ST: marginal resection with a saw or bur and osteotome to resect sequestra, necrotic bone, reactive bone, and clinically uninvolved bone that was identified by FDG uptake. Low-risk group (type A): 22 patients with activity limited to the alveolus, torus, and/or basal bone superior to the mandibular canal. High-risk group (type B): 11 patients with type A FDG activity with extension inferior to the mandibular canal. | 6.6 months | Treatment of type A MRONJ lesions was more successful than treatment of type B MRONJ lesions. 7 of the type B failures were successfully retreated by segmental resection and reconstruction. |
| Klingelhöffer et al. (2016) [51] | P | I (34) II (36) III (6) | 29 Neoplasms (33) Osteoporosis (4) Rheumatoid arthritis (3) | 70.9 | 20/20 | Preoperatory antibiotics and ST | 55 weeks | Long-term maintenance of the mucosal closure in 27.6% of patients. Stage II patients decreased to stage I in 81% after surgery, and stage III patients improved in 83% of cases. Stage I patients profited only in 38% by surgical intervention. MRONJ recurrence after surgery is associated with extended preoperative MRONJ duration. MRONJ of the upper jaw seems prognostically more favorable. |
| Hauer (2020) [52] | R | I (3) II (24) III (5) | 26 Osteoporosis (26) | 73.4 | DB (8) DB + BP (4) BP (16) for 73.1 months | ST: radical removal of necrotic bone was performed by resection with the borders in nonvital bone, followed by removal of residual osteonecrosis by rotary burr into the viable bleeding bone margins and under VELscope control. In lesions with sequestration, the sequestrectomy is performed, and the remaining necrotic bone is then radically removed by rotary burr. | 20.5 months | Complete healing was observed in all patients, in 9% of cases by secondary intention, in the mean period of 6 weeks. |
| Hoefert et al. (2017) [53] | R | I (1) II (10) III (6) | 17 Neoplasms (16) Osteoporosi (1) | 68.5 ± 12.0 | DB 120 mg (17) DB 60 mg (2) for 19.7 ± 10.5 months | Major ST (5): sequestrectomy, bone smoothing, tension-free tissue coverage, and drainage. Minor ST (1): palatal sequestrectomy and soft tissue closure. CT: (10): surface debridement, local rinses, and intermittent antibiotics. | 348 ± 329 days | Pain at the first visit in 47% of patients, of which 24% had pressure-like pain. The majority of MRONJ are at sites of dental prostheses-induced pressure sores (41%) or dental extractions (35%). Complete healing is significant in patients treated with major ST (80%) vs. CT (20%). DB is discontinued in 60% of nonoperative patients and major ST patients with no effect on healing. Histologic findings exhibit fewer osteocyte lacunae, and micro-CT reveals trabecular thickening. |
| Pichardo (2016) [54] | R | II (2) III (9) | 11 Neoplasms (7) OsteoporosiS (4) | 72.6 |
DB: 6 DB + BP: 5 For 17 months | ST: debridement with cauterization of the bone + antimicrobial treatment. | 16.4 | Healing in 9 patients |
| Beaudouin (2021) [55] | R | I (6) | 6 Neoplasm (6) | 66.5 | DB (6) | Surgical treatment: necrotic bone area reSection 5–9 months after Dmab withdrawal. Conservative treatment: oral hygiene, antibacterial mouthwashes, systemic antibiotic therapy, and not wearing overlying dentures. | 23.5 months | Dmab was stopped in MRONJ patients, with favorable outcomes for 3 cases and stabilization in 4 cases. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, A.M.; Malcangi, G.; Ferrara, I.; Patano, A.; Viapiano, F.; Netti, A.; Azzollini, D.; Ciocia, A.M.; de Ruvo, E.; Campanelli, M.; et al. MRONJ Treatment Strategies: A Systematic Review and Two Case Reports. Appl. Sci. 2023, 13, 4370. https://doi.org/10.3390/app13074370
Inchingolo AM, Malcangi G, Ferrara I, Patano A, Viapiano F, Netti A, Azzollini D, Ciocia AM, de Ruvo E, Campanelli M, et al. MRONJ Treatment Strategies: A Systematic Review and Two Case Reports. Applied Sciences. 2023; 13(7):4370. https://doi.org/10.3390/app13074370
Chicago/Turabian StyleInchingolo, Angelo Michele, Giuseppina Malcangi, Irene Ferrara, Assunta Patano, Fabio Viapiano, Anna Netti, Daniela Azzollini, Anna Maria Ciocia, Elisabetta de Ruvo, Merigrazia Campanelli, and et al. 2023. "MRONJ Treatment Strategies: A Systematic Review and Two Case Reports" Applied Sciences 13, no. 7: 4370. https://doi.org/10.3390/app13074370