
Preoperative Prediction of Optimal Femoral Implant Size by Regularized Regression on 3D Femoral Bone Shape
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Preprocessing
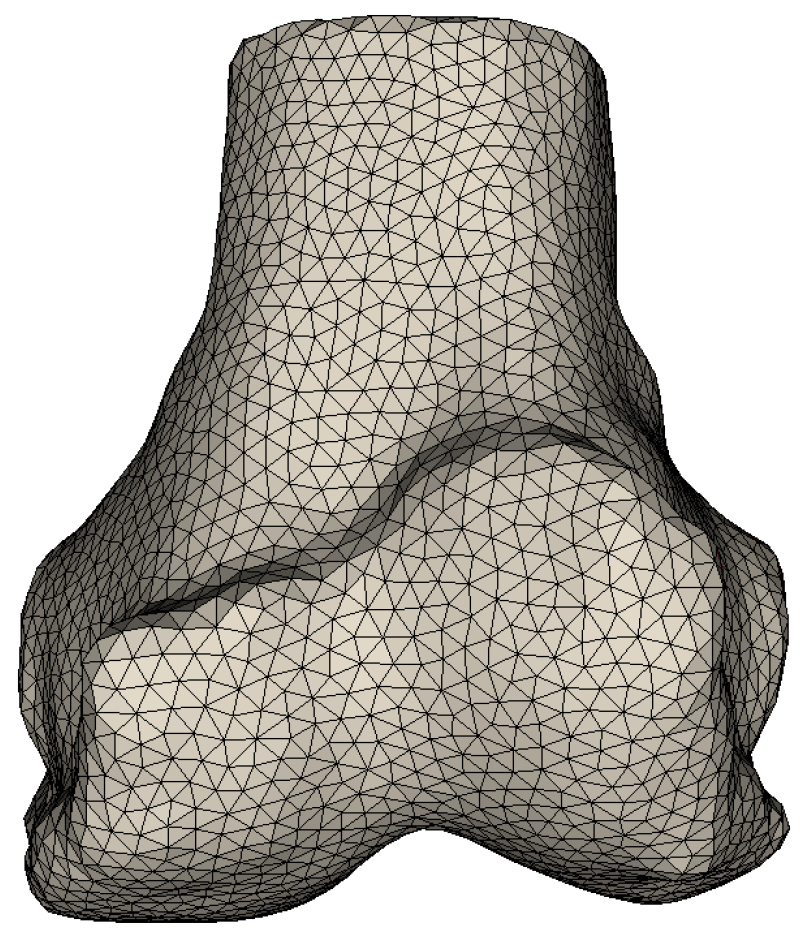
2.2. Hypergraph Representation of a Triangular Mesh
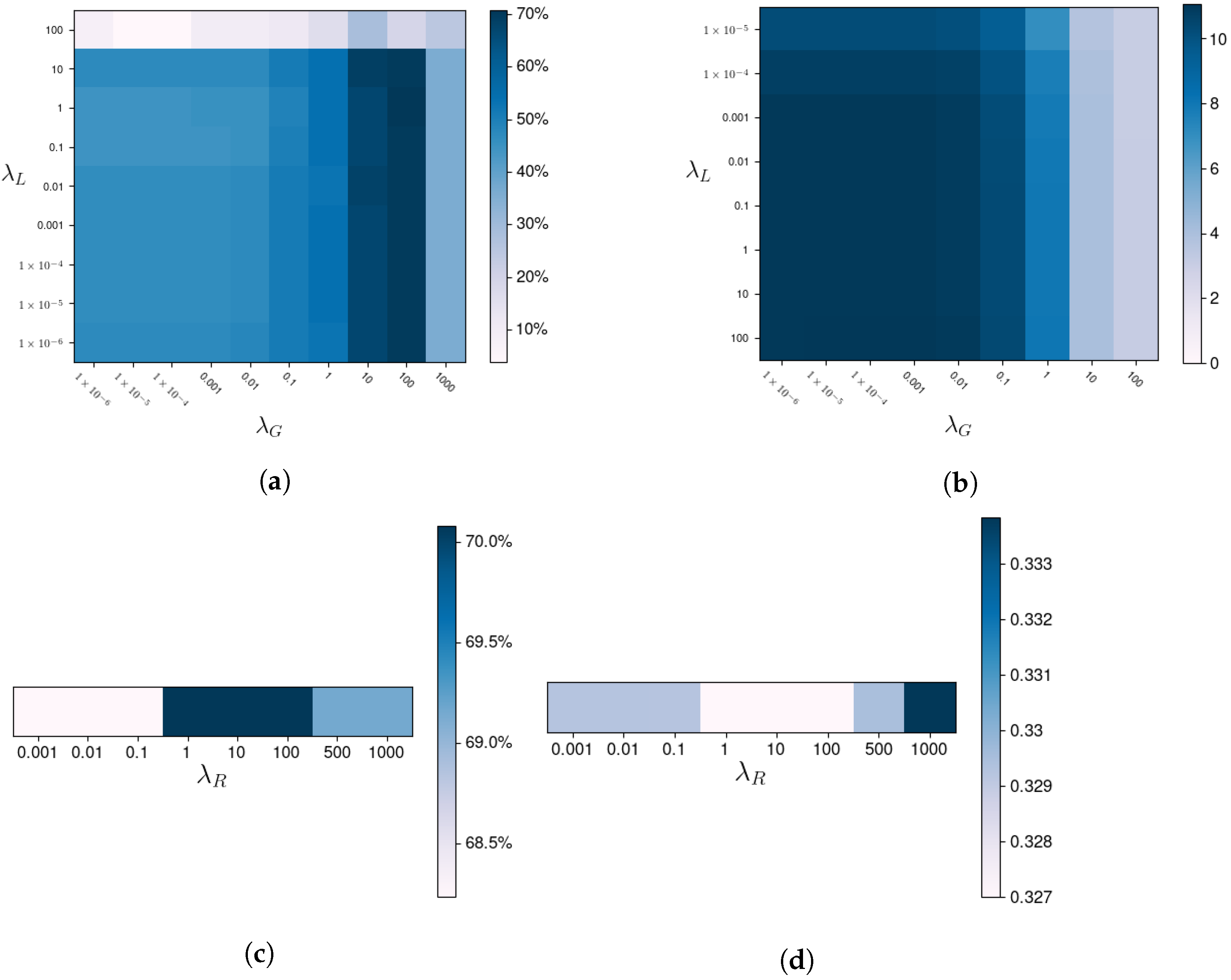
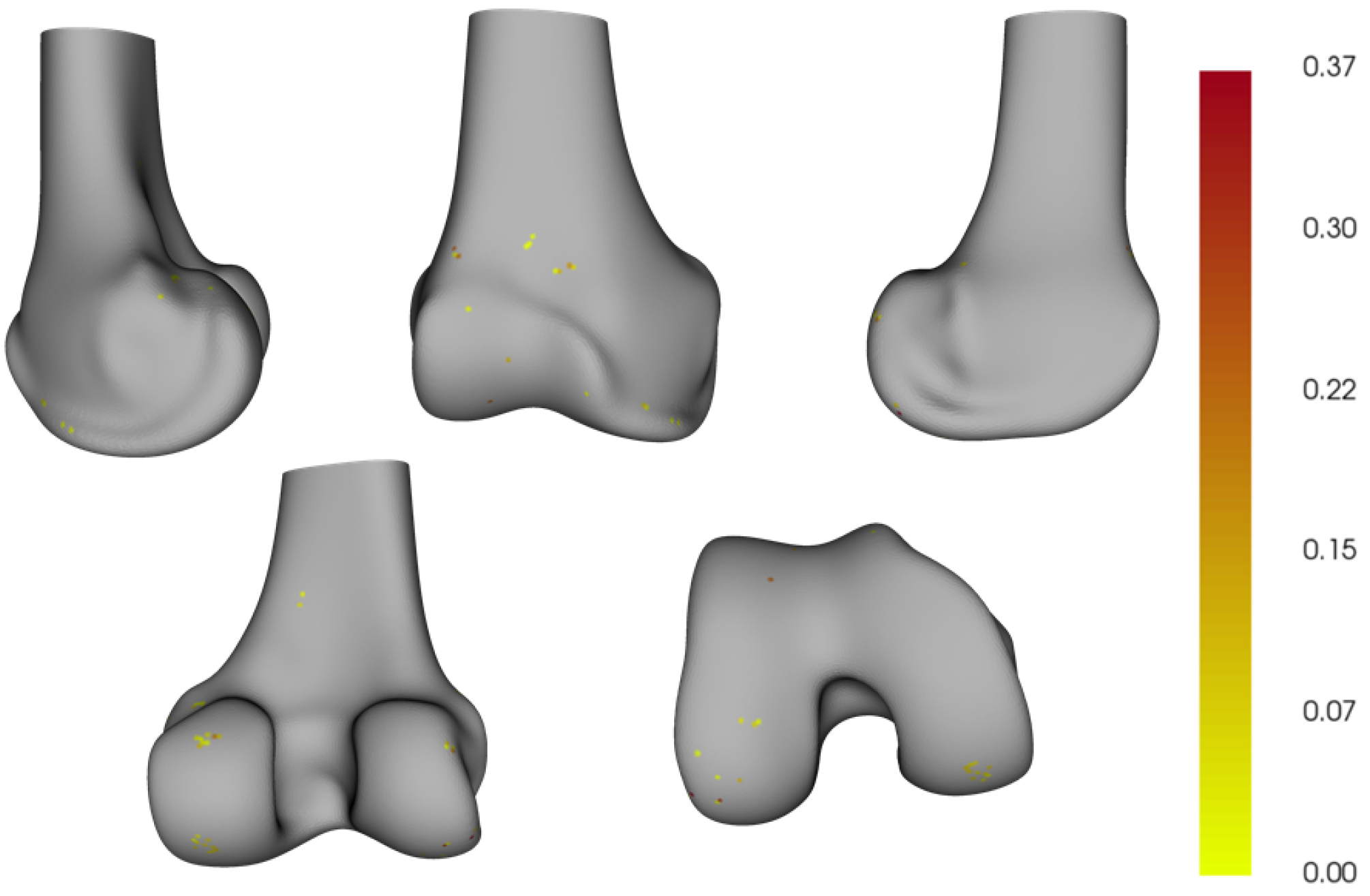
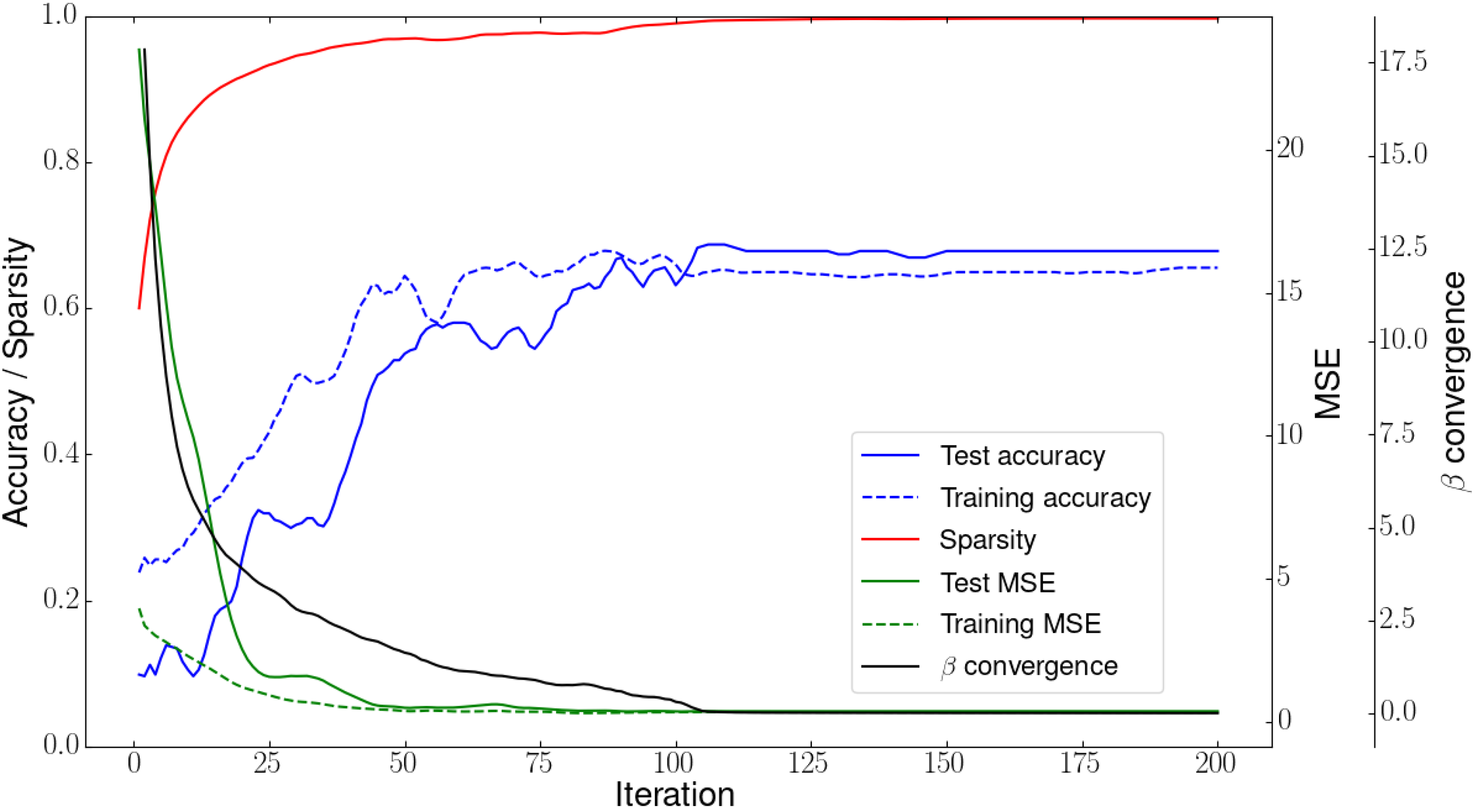
2.3. Hypergraph Regularized Group Lasso
| Algorithm 1: Hypergraph regularized group Lasso. |
 |
2.4. Baseline Method
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bourne, R.B.; Chesworth, B.M.; Davis, A.M.; Mahomed, N.N.; Charron, K.D.J. Patient Satisfaction after Total Knee Arthroplasty: Who is Satisfied and Who is Not? Clin. Orthop. Relat. Res. 2010, 468, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, S.J.; Murphy, M.P.; Schiffman, C.J.; Hopkinson, W.J.; Brown, N.M. Demographic data is more predictive of component size than digital radiographic templating in total knee arthroplasty. Knee Surg. Relat. Res. 2020, 32, 63. [Google Scholar] [CrossRef] [PubMed]
- Trickett, R.W.; Hodgson, P.; Forster, M.C.; Robertson, A. The reliability and accuracy of digital templating in total knee replacement. J. Bone Jt. Surg. Br. Vol. 2009, 91, 903–906. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.G.; Purtill, J.J. Accuracy of digital templating in total knee arthroplasty. Am. J. Orthop. 2012, 41, 510–512. [Google Scholar] [PubMed]
- Unnanuntana, A.; Arunakul, M.; Unnanuntana, A. The accuracy of preoperative templating in total knee arthroplasty. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2007, 90, 2338–2343. [Google Scholar]
- Pietrzak, J.R.T.; Rowan, F.E.; Kayani, B.; Donaldson, M.J.; Huq, S.S.; Haddad, F.S. Preoperative CT-Based Three-Dimensional Templating in Robot-Assisted Total Knee Arthroplasty More Accurately Predicts Implant Sizes than Two-Dimensional Templating. J. Knee Surg. 2019, 32, 642–648. [Google Scholar] [CrossRef]
- Ettinger, M.; Claassen, L.; Paes, P.; Calliess, T. 2D versus 3D templating in total knee arthroplasty. Knee 2016, 23, 149–151. [Google Scholar] [CrossRef]
- Schotanus, M.G.M.; Schoenmakers, D.A.L.; Sollie, R.; Kort, N.P. Patient-specific instruments for total knee arthroplasty can accurately predict the component size as used peroperative. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 3844–3848. [Google Scholar] [CrossRef]
- Mahoney, O.M.; Kinsey, T. Overhang of the Femoral Component in Total Knee Arthroplasty: Risk Factors and Clinical Consequences. J. Bone Jt.-Surg.-Am. Vol. 2010, 92, 1115–1121. [Google Scholar] [CrossRef]
- Tibesku, C.O. 15 The Problem of Under-or Oversizing of Total Knee Replacement. In The Unhappy Total Knee Replacement: A Comprehensive Review and Management Guide; Springer: Cham, Switzerland, 2015; pp. 175–184. [Google Scholar]
- Trainor, S.; Collins, J.; Mulvey, H.; Fitz, W. Total Knee Replacement Sizing: Shoe Size Is a Better Predictor for Implant Size than Body Height. Arch. Bone Jt. Surg. 2018, 6, 100–104. [Google Scholar]
- Lachiewicz, P.F.; Henderson, R.A. Patient-specific Instruments for Total Knee Arthroplasty. J. Am. Acad. Orthop. Surg. 2013, 21, 513–518. [Google Scholar] [CrossRef]
- MacDessi, S.J.; Jang, B.; Harris, I.A.; Wheatley, E.; Bryant, C.; Chen, D.B. A comparison of alignment using patient specific guides, computer navigation and conventional instrumentation in total knee arthroplasty. Knee 2014, 21, 406–409. [Google Scholar] [CrossRef]
- Liu, Z.; Wu, S.; Jin, S.; Ji, S.; Liu, Q.; Lu, S.; Cheng, L. Investigating Pose Representations and Motion Contexts Modeling for 3D Motion Prediction. IEEE Trans. Pattern Anal. Mach. Intell. 2023, 45, 681–697. [Google Scholar] [CrossRef]
- Liu, H.; Liu, M.; Li, D.; Zheng, W.; Yin, L.; Wang, R. Recent Advances in Pulse-Coupled Neural Networks with Applications in Image Processing. Electronics 2022, 11, 3264. [Google Scholar] [CrossRef]
- Kunze, K.N.; Polce, E.M.; Patel, A.; Courtney, P.M.; Levine, B.R. Validation and performance of a machine-learning derived prediction guide for total knee arthroplasty component sizing. Arch. Orthop. Trauma Surg. 2021, 141, 2235–2244. [Google Scholar] [CrossRef]
- Sershon, R.A.; Courtney, P.M.; Rosenthal, B.D.; Sporer, S.M.; Levine, B.R. Can Demographic Variables Accurately Predict Component Sizing in Primary Total Knee Arthroplasty? J. Arthroplast. 2017, 32, 3004–3008. [Google Scholar] [CrossRef]
- Sershon, R.A.; Li, J.; Calkins, T.E.; Courtney, P.M.; Nam, D.; Gerlinger, T.L.; Sporer, S.M.; Levine, B.R. Prospective Validation of a Demographically Based Primary Total Knee Arthroplasty Size Calculator. J. Arthroplast. 2019, 34, 1369–1373. [Google Scholar] [CrossRef]
- Bhowmik-Stoker, M.; Scholl, L.Y.; Khlopas, A.; Sultan, A.A.; Sodhi, N.; Moskal, J.T.; Mont, M.A.; Teeny, S.M. Accurately Predicting Total Knee Component Size without Preoperative Radiographs. Surg. Technol. Int. 2018, 33, 337–342. [Google Scholar]
- Ren, A.N.; Neher, R.E.; Bell, T.; Grimm, J. Using Patient Demographics and Statistical Modeling to Predict Knee Tibia Component Sizing in Total Knee Arthroplasty. J. Arthroplast. 2018, 33, 1732–1736. [Google Scholar] [CrossRef]
- Naylor, B.H.; Butler, J.T.; Kuczynski, B.; Bohm, A.R.; Scuderi, G.R. Can Component Size in Total Knee Arthroplasty Be Predicted Preoperatively?—An Analysis of Patient Characteristics. J. Knee Surg. 2022. [Google Scholar] [CrossRef]
- Blevins, J.L.; Rao, V.; Chiu, Y.f.; Lyman, S.; Westrich, G.H. Predicting implant size in total knee arthroplasty using demographic variables. Bone Jt. J. 2020, 102, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Lambrechts, A.; Wirix-Speetjens, R.; Maes, F.; Van Huffel, S. Artificial Intelligence Based Patient-Specific Preoperative Planning Algorithm for Total Knee Arthroplasty. Front. Robot. AI 2022, 9, 899349. [Google Scholar] [CrossRef] [PubMed]
- Clemmensen, L.; Hastie, T.; Witten, D.; Ersbøll, B. Sparse Discriminant Analysis. Technometrics 2011, 53, 406–413. [Google Scholar] [CrossRef] [Green Version]
- Lorensen, W.E.; Cline, H.E. Marching cubes: A high resolution 3D surface construction algorithm. ACM SIGGRAPH Comput. Graph. 1987, 21, 163–169. [Google Scholar] [CrossRef]
- Van Dijck, C.; Wirix-Speetjens, R.; Jonkers, I.; Vander Sloten, J. Statistical shape model-based prediction of tibiofemoral cartilage. Comput. Methods Biomech. Biomed. Eng. 2018, 21, 568–578. [Google Scholar] [CrossRef]
- Amberg, B.; Romdhani, S.; Vetter, T. Optimal Step Nonrigid ICP Algorithms for Surface Registration. In Proceedings of the 2007 IEEE Conference on Computer Vision and Pattern Recognition, Minneapolis, MI, USA, 17–22 June 2007; pp. 1–8. [Google Scholar] [CrossRef]
- Roth, V.; Fischer, B. The Group-Lasso for generalized linear models: Uniqueness of solutions and efficient algorithms. In Proceedings of the 25th International Conference on Machine Learning, ICML ’08, Helsinki, Finland, 5–9 July 2008; pp. 848–855. [Google Scholar] [CrossRef]
- Hastie, T.R.; Wainwright, M. Statistical Learning with Sparsity: The Lasso and Generalizations; Chapman & Hall/CRC: Boca Raton, FL, USA, 2015. [Google Scholar]
- Ma, X.; Liu, W.; Li, S.; Tao, D.; Zhou, Y. Hypergraph p-Laplacian Regularization for Remotely Sensed Image Recognition. IEEE Trans. Geosci. Remote Sens. 2019, 57, 1585–1595. [Google Scholar] [CrossRef] [Green Version]
- Zou, H.; Hastie, T. Regularization and Variable Selection via the Elastic Net. J. R. Stat. Soc. Ser. 2005, 67, 301–320. [Google Scholar] [CrossRef] [Green Version]
- Nesterov, Y.E. A method for solving the convex programming problem with convergence rate O (1/k⌃ 2). Dokl. Akad. Nauk SSSR 1983, 269, 543–547. [Google Scholar]
- Duff, I.S.; Grimes, R.G.; Lewis, J.G. Sparse matrix test problems. ACM Trans. Math. Softw. 1989, 15, 62043. [Google Scholar] [CrossRef]
- Stamiris, D.; Gkekas, N.K.; Asteriadis, K.; Stamiris, S.; Anagnostis, P.; Poultsides, L.; Sarris, I.; Potoupnis, M.; Kenanidis, E.; Tsiridis, E. Anterior femoral notching ≤ 3 mm is associated with increased risk for supracondylar periprosthetic femoral fracture after total knee arthroplasty: A systematic review and meta-analysis. Eur. J. Orthop. Surg. Traumatol. 2022, 32, 383–393. [Google Scholar] [CrossRef]
- Ambellan, F.; Tack, A.; Ehlke, M.; Zachow, S. Automated segmentation of knee bone and cartilage combining statistical shape knowledge and convolutional neural networks: Data from the Osteoarthritis Initiative. Med. Image Anal. 2019, 52, 109–118. [Google Scholar] [CrossRef]
- Schoenmakers, D.A.L.; Theeuwen, D.M.J.; Schotanus, M.G.M.; Jansen, E.J.P.; van Haaren, E.H.; Hendrickx, R.P.M.; Kort, N.P. High intra- and inter-observer reliability of planning implant size in MRI-based patient-specific instrumentation for total knee arthroplasty. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 573–578. [Google Scholar] [CrossRef] [Green Version]
- Seaver, T.; McAlpine, K.; Garcia, E.; Niu, R.; Smith, E.L. Algorithm based automatic templating is less accurate than manual digital templating in total knee arthroplasty. J. Orthop. Res. 2020, 38, 1472–1476. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Scanner | GE OptimaTM MR450w |
| Field strength | 1.5 T |
| Scan type | 3D |
| Scan direction | Sagittal |
| Sequence | Fat saturated T1 spoiled gradient echo |
| Slice thickness | 1 mm |
| Pixel size | 0.4 mm |
| Study | Absolute Accuracy | +1/−1 Size Accuracy | Modality |
|---|---|---|---|
| Trickett et al. 2009 [3] | 48% | 98% | 2D: X-ray |
| Miller et al. 2012 [4] | 64% | 100% | 2D: X-ray |
| Unnanuntana et al. 2007 [5] | 50.4% | 97.3% | 2D: X-ray |
| Pietrzak et al. 2019 [6] | 52.9% | - | 2D: X-Ray |
| Ettinger et al. 2016 [7] | 59.6% | 97.9% | 2D: X-ray |
| Pietrzak et al. 2019 [6] | 96.6% | - | 3D: CT |
| Ettinger et al. 2016 [7] | 100% | 100% | 3D: MRI |
| Schotanus et al. 2016 [8] | 93.9% | - | 3D: MRI |
| Study | Absolute Accuracy | +1/−1 Size Accuracy | Modality |
|---|---|---|---|
| Seaver et al. 2020 [37] | 19.2% | 51.2% | 2D: X-ray |
| Trainor et al. 2018 [11] | 56% | 99% | Shoe size |
| Sershon et al. 2017 [17] | - | 85–95% (implant dependent) | Demographics |
| Bhowmik-Stoker et al. 2018 [19] | - | 94% | Demographics |
| Sershon et al. 2019 [18] | - | 76% | Demographics |
| Blevins et al. 2020 [22] | - | 94.4% | Demographics |
| Wallace et al. 2020 [2] | 43.7% | 90.1% | Demographics |
| Kunze et al. 2021 [16] | 48.4% | 95% | Demographics |
| Naylor et al. 2022 [21] | - | 83.09% | Demographics |
| Lambrechts et al. 2022 [23] | 82.2% | - | 3D: MRI |
| Manufacturer’s default plan | 23.1% | 99.11% | 3D: MRI |
| Shape coefficient regression | 58.93% | 98.21% | 3D: MRI |
| Hypergraph regularized group lasso | 70.08% | 99.11% | 3D: MRI |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambrechts, A.; Van Dijck, C.; Wirix-Speetjens, R.; Vander Sloten, J.; Maes, F.; Van Huffel, S. Preoperative Prediction of Optimal Femoral Implant Size by Regularized Regression on 3D Femoral Bone Shape. Appl. Sci. 2023, 13, 4344. https://doi.org/10.3390/app13074344
Lambrechts A, Van Dijck C, Wirix-Speetjens R, Vander Sloten J, Maes F, Van Huffel S. Preoperative Prediction of Optimal Femoral Implant Size by Regularized Regression on 3D Femoral Bone Shape. Applied Sciences. 2023; 13(7):4344. https://doi.org/10.3390/app13074344
Chicago/Turabian StyleLambrechts, Adriaan, Christophe Van Dijck, Roel Wirix-Speetjens, Jos Vander Sloten, Frederik Maes, and Sabine Van Huffel. 2023. "Preoperative Prediction of Optimal Femoral Implant Size by Regularized Regression on 3D Femoral Bone Shape" Applied Sciences 13, no. 7: 4344. https://doi.org/10.3390/app13074344