

Digital Occlusion Analysis after Orthodontic Treatment: Capabilities of the Intraoral Scanner and T-Scan Novus System

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
- -
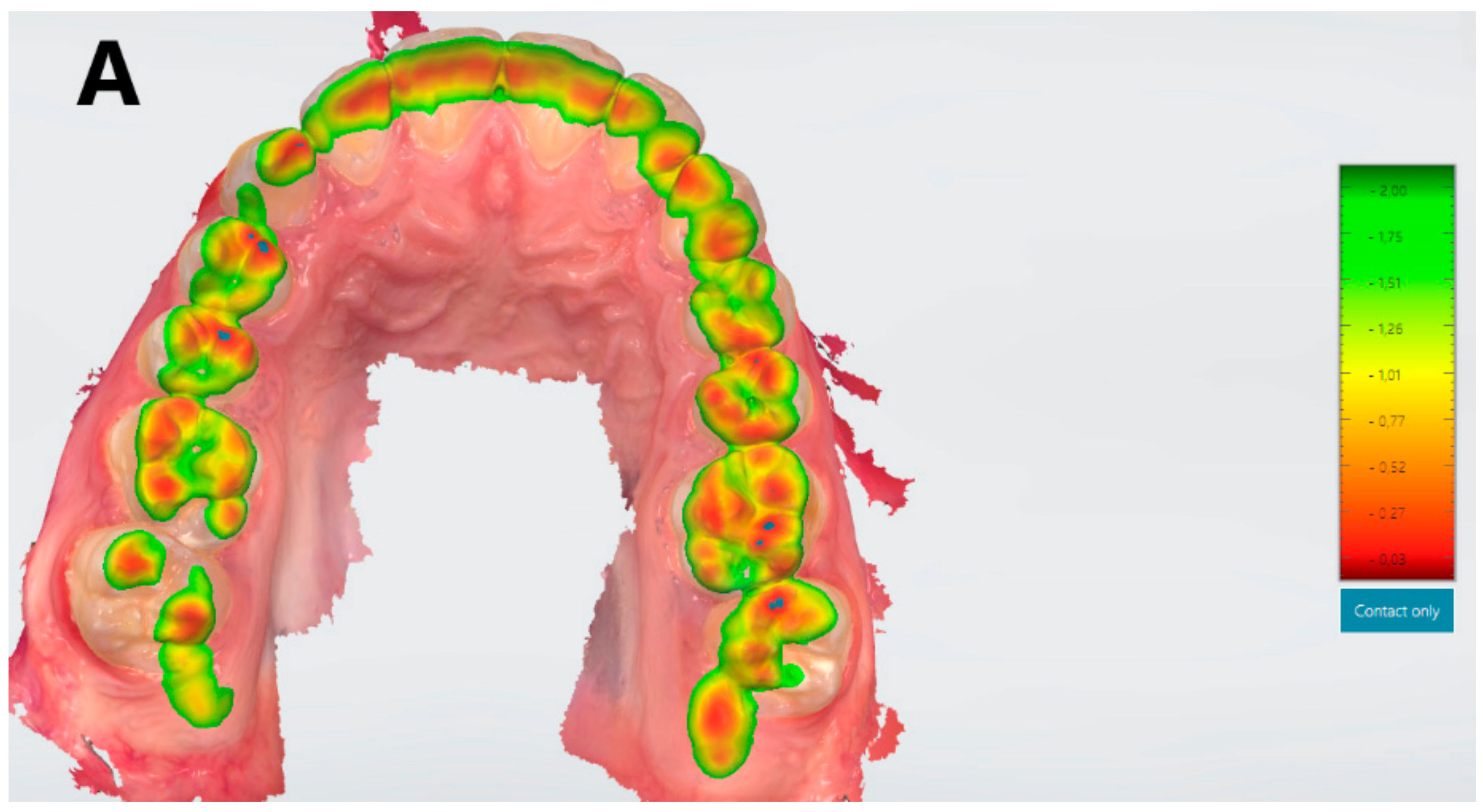
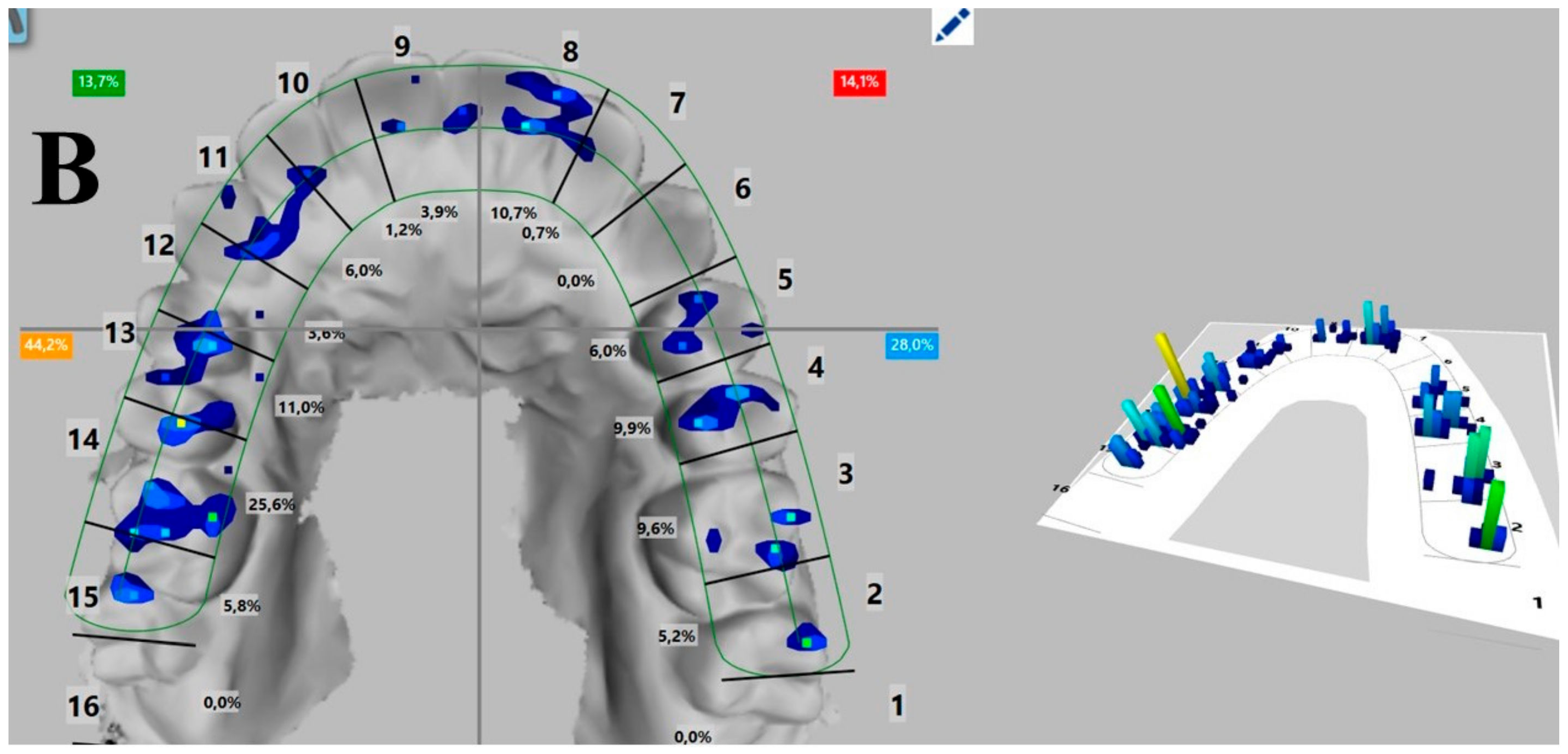
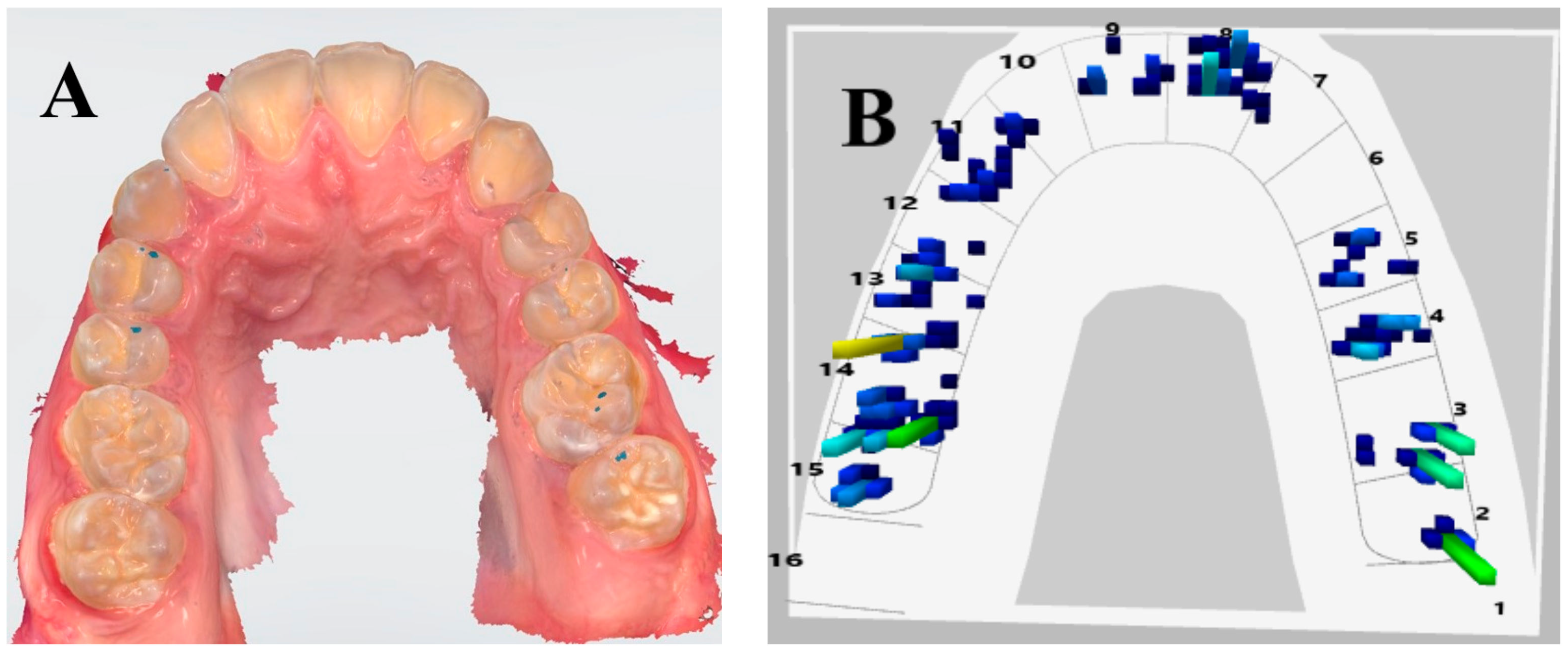
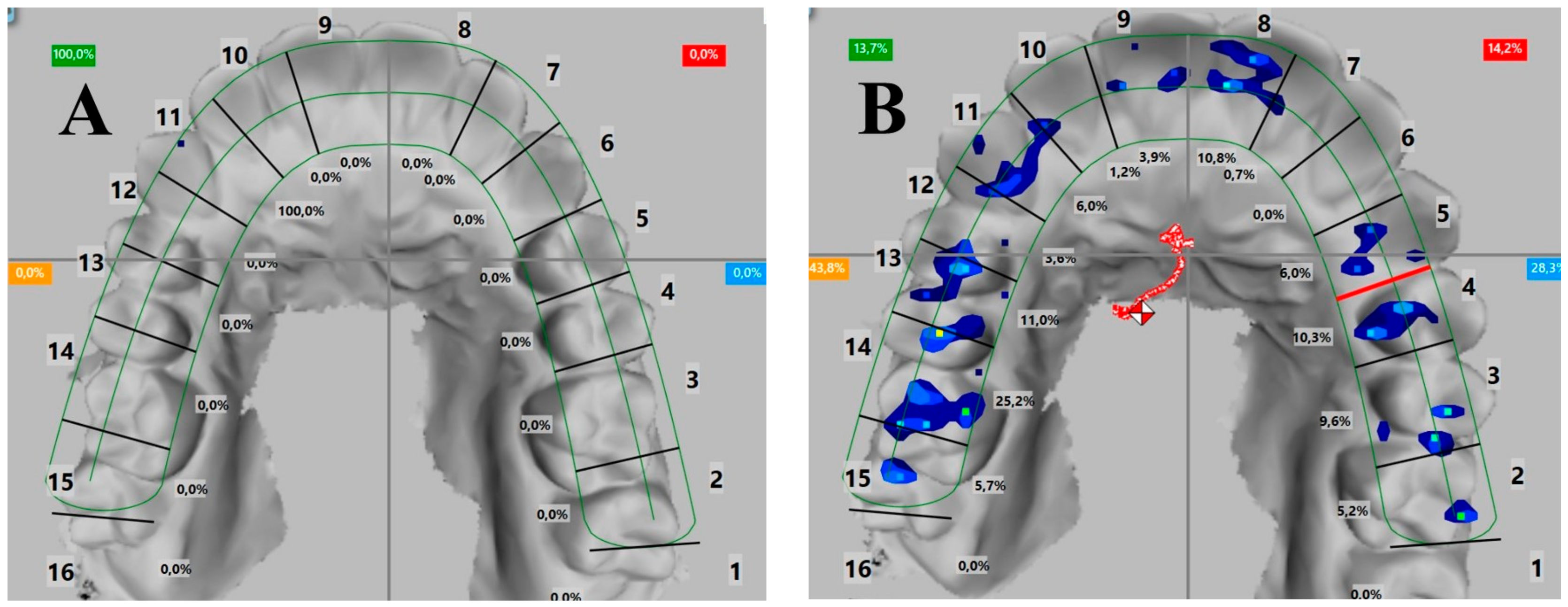
- The tight contact of tooth 13 according to the 3Shape system is the first contact according to the T-Scan system;
- -
- The tight contact of tooth 14 according to the 3Shape system is moderately strong (light blue marking) according to the T-Scan system;
- -
- The tight contact of tooth 15 according to the 3Shape system is the strongest (yellow marking) according to the T-Scan system;
- -
- The tight contacts of teeth 26 and 27 according to the 3Shape system are moderately strong (green marking) according to the T-Scan system;
- -
- All contacts in the 3Shape system have the same markings, but the difference between them can be analyzed only by the T-Scan system;
- -
- The percentage distribution of the strength of the contacts in the dental arch on the single teeth or on the quadrants can be visualized only by the T-Scan system;
- -
- The T-Scan system generates a video and shows the sequence and strength of the contacts in great detail, combined with the movement of the lower jaw;
- -
- The T-Scan system notes occlusion and disocclusion times, which are important parameters in the examination and treatment of patients with parafunction;
- -
- The movement of the lower jaw and its direction and shape can also be documented only through the T-Scan system.


- -
- Male, 17 years old, right frontal zone 32.6%, left distal zone 67.4%;
- -
- Female, 26 years old, left frontal zone 41.2%, left distal zone 58.8%.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Zone | Male (N = 15) | Female (N = 17) | ||
|---|---|---|---|---|
| Mean ± SD | Number of Cases | Mean ± SD | Number of Cases | |
| Right distal zone | 46.67 ± 1.65 | 7 | 47.06 ± 1.78 | 8 |
| Right frontal zone | 6.67 ± 0.23 | 1 | 5.88 ± 0.34 | 1 |
| Left frontal zone | 6.67 ± 0.23 | 1 | 0 ± 0.12 | 0 |
| Left distal zone | 40.00 ± 1.52 | 6 | 47.06 ± 1.78 | 8 |
4. Discussion
Research Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TMJ | temporomandibular joint |
| TMD | temporomandibular disorders |
| MBT system | McLaughlin, Bennett, Trevisi (by the names of the creators) |
| CBCT | cone beam computed tomography |
| JMT | jaw motion tracking |
References
- Zimmermann, M.; Mehl, A.; Mörmann, W.H.; Reich, S. Intraoral scanning systems—A current overview. Int. J. Comput. Dent. 2015, 18, 101–129. [Google Scholar]
- Patzelt, S.B.; Lamprinos, C.; Stampf, S.; Att, W. The time efficiency of intraoral scanners: An in vitro comparative study. J. Am. Dent. Assoc. 2014, 145, 542–551. [Google Scholar] [CrossRef] [Green Version]
- Aswani, K.; Wankhade, S.; Khalikar, A.; Deogade, S. Accuracy of an intraoral digital impression: A review. J. Indian Prosthodont. Soc. 2020, 20, 27. [Google Scholar] [CrossRef]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imburgia, M.; Logozzo, S.; Hauschild, U.; Veronesi, G.; Mangano, C.; Mangano, F.G. Accuracy of four intraoral scanners in oral implantology: A comparative in vitro study. BMC Oral Health 2017, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Ting-Shu, S.; Jian, S. Intraoral digital impression technique: A review. J. Prosthodont. 2015, 24, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Kaewbuasa, N.; Ongthiemsak, C. Effect of different arch widths on the accuracy of three intraoral scanners. J. Adv. Prosthodont. 2021, 13, 205. [Google Scholar] [CrossRef] [PubMed]
- Button, H.; Kois, J.C.; Barmak, A.B.; Zeitler, J.M.; Rutkunas, V.; Revilla-León, M. Scanning accuracy and scanning area discrepancies of intraoral digital scans acquired at varying scanning distances and angulations among 4 different intraoral scanners. J. Prosthet. Dent. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Bedrossian, E.A.; Bedrossian, E.; Kois, J.C.; Revilla-León, M. Use of an optical jaw-tracking system to record mandibular motion for treatment planning and designing interim and definitive prostheses: A dental technique. J. Prosthet. Dent. 2022, in press. [Google Scholar] [CrossRef]
- Revilla-León, M.; Zeitler, J.M.; Kois, J.C. Digital maxillomandibular relationship and mandibular motion recording by using an optical jaw tracking system to acquire a dynamic virtual patient. J. Prosthet. Dent. 2022, in press. [Google Scholar] [CrossRef]
- Revilla-León, M.; Fernández-Estevan, L.; Barmak, A.B.; Kois, J.C.; Pérez-Barquero, J.A. Accuracy of the maxillomandibular relationship at centric relation position recorded by using 3 different intraoral scanners with or without an optical jaw tracking system: An in vivo pilot study. J. Dent. 2023, 132, 104478. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Kau, C.H.; Liao, L.; Kinderknecht, K.; Ow, A.; Abou Saleh, T. The use of a dynamic real-time jaw tracking device and cone beam computed tomography simulation. Ann. Maxillofac. Surg. 2016, 6, 113. [Google Scholar] [PubMed] [Green Version]
- Mahony, D. Refining occlusion with muscle balance to enhance long-term orthodontic stability. J. Clin. Pediatr. Dent. 2005, 29, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Davies, S.J.; Gray RM, J.; Sandler, P.J.; O’Brien, K.D. Orthodontics and occlusion. Br. Dent. J. 2001, 191, 539–549. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, R.P.; Bennett, J.C. Evolution of treatment mechanics and contemporary appliance design in orthodontics: A 40-year perspective. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 654–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Littlewood, S.J.; Kandasamy, S.; Huang, G. Retention and relapse in clinical practice. Aust. Dent. J. 2017, 62, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Heymann, G.C.; Grauer DA, N.; Swift, E.J., Jr. Contemporary approaches to orthodontic retention. J. Esthet. Restor. Dent. 2012, 24, 83–87. [Google Scholar] [CrossRef]
- Al-Moghrabi, D.; Littlewood, S.J.; Fleming, P.S. Orthodontic retention protocols: An evidence-based overview. Br. Dent. J. 2021, 230, 770–776. [Google Scholar] [CrossRef]
- Bibona, K.; Shroff, B.; Best, A.M.; Lindauer, S.J. Factors affecting orthodontists’ management of the retention phase. Angle Orthod. 2014, 84, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Devi, S.; Nallaswamy, D.; Venugopalan, S. Prosthetic Occlusal Analyzers—A Comprehensive Review. Int. J. Dent. Oral Sci. 2021, 8, 3550–3554. [Google Scholar]
- Babu, R.R.; Nayar, S.V. Occlusion indicators: A review. J. Indian Prosthodont. Soc. 2007, 7, 170. [Google Scholar]
- Carey, J.; Craig, M.; Kerstein, R.B.; Radke, J. Determining a relationship between applied occlusal load and articulation paper mark area. Open Dent. J. 2007, 1, 1–7. [Google Scholar] [CrossRef]
- Available online: https://www.tekscan.com/products-solutions/systems/t-scan-novus (accessed on 9 February 2023).
- Cerna, M.; Ferreira, R.; Zaror, C.; Navarro, P.; Sandoval, P. Validity and reliability of the T-Scan® III for measuring force under laboratory conditions. J. Oral Rehabil. 2015, 42, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Solaberrieta, E.; Etxaniz, O.; Otegi, J.R.; Brizuela, A.; Pradies, G. Customized procedure to display T-Scan occlusal contacts. J. Prosthet. Dent. 2017, 117, 18–21. [Google Scholar] [CrossRef]
- Kerstein, R.B. Current applications of computerized occlusal analysis in dental medicine. Gen. Dent. 2001, 49, 521–530. [Google Scholar] [PubMed]
- Fraile, C.; Ferreiroa, A.; Romeo, M.; Alonso, R.; Pradíes, G. Clinical study comparing the accuracy of interocclusal records, digitally obtained by three different devices. Clin. Oral Investig. 2021, 26, 4663–4668. [Google Scholar] [CrossRef]
- Buduru, S.; Mesaros, A.; Talmaceanu, D.; Baru, O.; Ghiurca, R.; Cosgarea, R. Occlusion in the digital era: A report on 3 cases. Med. Pharm. Rep. 2019, 92 (Suppl. S3), S78. [Google Scholar] [CrossRef]
- Kerstein, R.B. The Evolution of the T-Scan I System From 1984 to the Present Day T-Scan 10 System. In Handbook of Research on Clinical Applications of Computerized Occlusal Analysis in Dental Medicine; IGI Global: Hershey, PA, USA, 2020; pp. 1–54. [Google Scholar]
- Ayuso-Montero, R.; Mariano-Hernandez, Y.; Khoury-Ribas, L.; Rovira-Lastra, B.; Willaert, E.; Martinez-Gomis, J. Reliability and validity of T-scan and 3d intraoral scanning for measuring the occlusal contact area. J. Prosthodont. 2020, 29, 19–25. [Google Scholar] [CrossRef]
- Shopova, D.; Yordanova, M.; Yordanova, S. The Digital Impression As An Initial Unit Of Modern Dental Medicine-Literature Review. Knowl.-Int. J. 2020, 38, 797–801. [Google Scholar]
- Shopova, D.; Bakova, D.; Yordanova, M.; Yordanova, S. Teledentistry Methods In Orthodontics And Prosthetic Dentistry During COVID-19 Pandemic. Knowl.-Int. J. 2021, 49, 667–672. [Google Scholar]
- Reddy, L.K.V.; Madithati, P.; Narapureddy, B.R.; Ravula, S.R.; Vaddamanu, S.K.; Alhamoudi, F.H.; Minervini, G.; Chaturvedi, S. Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 1920. [Google Scholar] [CrossRef]
- Ron, B.V.; Cisneros, V.M.; Troncoso, P.P.; Tates, M.R.; Lalvay, E.A.; Bajaña, L.C.; Balladares, A.O. Monitoring of awake bruxism by intelligent app. F1000Research 2022, 11, 479. [Google Scholar]
- Komali, G.; Ignatius, A.V.; Srivani, G.S.; Anuja, K. T-scan system in the management of temporomandibular joint disorders–A review. J. Indian Acad. Oral Med. Radiol. 2019, 31, 252–256. [Google Scholar]
- Haralur, S.B. Digital Evaluation of Functional Occlusion Parameters and their Association with Temporomandibular Disorders. J. Clin. Diagn. Res. 2013, 7, 1772–1775. [Google Scholar] [CrossRef]
- Minervini, G.; Mariani, P.; Fiorillo, L.; Cervino, G.; Cicciù, M.; Laino, L. Prevalence of temporomandibular disorders in people with multiple sclerosis: A systematic review and meta-analysis. CRANIO® 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Del Mondo, D.; Russo, D.; Cervino, G.; D’Amico, C.; Fiorillo, L. Stem cells in temporomandibular joint engineering: State of art and future persectives. J. Craniofacial Surg. 2022, 33, 2181–2187. [Google Scholar] [CrossRef]
- Dimova-Gabrovska, M.I. Protocol for clinical articulation of complete dentures in maximum intercuspation. Stomatologiia 2019, 98, 45–49. [Google Scholar] [CrossRef]
- Dimitrova, D.; Andreeva, R.; Dimova-Gabrovska, M. Application of aesthetic crowns in children patients. Varna Med. Forum 2018, 7, 141–145. [Google Scholar] [CrossRef]
- Dimova-Gabrovska, M.; Dimitrova, D.; Mitronin, V.A. Removable prosthetic treatment in children-literature review. J. IMAB–Annu. Proceeding Sci. Pap. 2018, 24, 2172–2176. [Google Scholar] [CrossRef] [Green Version]
- Trpevska, V.; Kovacevska, G.; Benedeti, A.; Jordanov, B. T-Scan III system diagnostic tool for digital occlusal analysis in orthodontics–a modern approach. Prilozi 2014, 35, 155–160. [Google Scholar] [CrossRef] [Green Version]
- Koval, S.; Kerstein, R.; Radke, J. Characteristics of static and excursive occlusal parameters in subjects seeking orthodontic treatment using t-scan 9 digital occlusal analysis. Adv. Dent. Technol. Tech. 2021, 3, 87–99. [Google Scholar]
- Doh, R.M.; Kim, J.E.; Nam, N.E.; Shin, S.H.; Lim, J.H.; Shim, J.S. Evaluation of Dimensional Changes during Postcuring of a Three-Dimensionally Printed Denture Base According to the Curing Time and the Time of Removal of the Support Structure: An In Vitro Study. Appl. Sci. 2021, 11, 10000. [Google Scholar] [CrossRef]
- Vitale, M.C.; Gallo, S.; Pascadopoli, M.; Alcozer, R.; Ciuffreda, C.; Scribante, A. Local anesthesia with SleeperOne S4 computerized device vs traditional syringe and perceived pain in pediatric patients: A randomized clinical trial. J. Clin. Pediatr. Dent. 2023, 47, 82–90. [Google Scholar]
- Su, T.S.; Sun, J. Comparison of repeatability between intraoral digital scanner and extraoral digital scanner: An in-vitro study. J. Prosthodont. Res. 2015, 59, 236–242. [Google Scholar] [CrossRef]
- Lee, S.J.; Kim, S.W.; Lee, J.J.; Cheong, C.W. Comparison of intraoral and extraoral digital scanners: Evaluation of surface topography and precision. Dent. J. 2020, 8, 52. [Google Scholar] [CrossRef]
- Qadeer, S.; Yang, L.; Sarinnaphakorn, L.; Kerstein, R.B. Comparison of closure occlusal force parameters in post-orthodontic and non-orthodontic subjects using T-Scan® III DMD occlusal analysis. CRANIO® 2016, 34, 395–401. [Google Scholar] [CrossRef]
- Thumati, P. Digital analysis of occlusion using T-Scan III in orthodontics. J. Indian Orthod. Soc. 2016, 50, 196–201. [Google Scholar] [CrossRef]
- Morsy, N.; El Kateb, M. Accuracy of intraoral scanners for static virtual articulation: A systematic review and meta-analysis of multiple outcomes. J. Prosthet. Dent. 2022, in press. [Google Scholar] [CrossRef]
- Cohen-Levy, J. Orthodontic T-Scan Applications. Handb. Res. Comput. Occlusal Anal. Technol. Appl. Dent. Med. 2015, 523–561. [Google Scholar] [CrossRef] [Green Version]
- Cohen-Levy, J. Orthodontic Monitoring and Case Finishing With the T-Scan System. Handb. Res. Clin. Appl. Comput. Occlusal Anal. Dent. Med. 2020, 1057–1124. [Google Scholar] [CrossRef] [Green Version]
- Shopova, D.; Mladenov, K. Case Report: A digital workflow in the treatment of bruxism in a young patient. F1000Research 2022, 10, 894. [Google Scholar] [CrossRef]
- Shopova, D.; Bozhkova, T.; Yordanova, S.; Yordanova, M. Case Report: Digital analysis of occlusion with T-Scan Novus in occlusal splint treatment for a patient with bruxism. F1000Research 2021, 10, 915. [Google Scholar] [CrossRef]
- Dimova-Gabrovska, M. Algorithm for computerized analysis of static, dynamic and functional occlusion in patients with bruxism and bruxomania. Comptes Rendus De L’Académie Bulg. Des Sci. 2019, 72, 259–266. [Google Scholar]
- Park, H.R.; Park, J.M.; Chun, Y.S.; Lee, K.N.; Kim, M. Changes in views on digital intraoral scanners among dental hygienists after training in digital impression taking. BMC Oral. Health 2015, 15, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liczmanski, K.; Stamm, T.; Sauerland, C.; Blanck-Lubarsch, M. Accuracy of intraoral scans in the mixed dentition: A prospective non-randomized comparative clinical trial. Head Face Med. 2020, 16, 1–7. [Google Scholar] [CrossRef]
- Christopoulou, I.; Kaklamanos, E.G.; Makrygiannakis, M.A.; Bitsanis, I.; Perlea, P.; Tsolakis, A.I. Intraoral scanners in Orthodontics: A critical review. Int. J. Environ. Res. Public Health 2022, 19, 1407. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Jabbal, R.; Bindra, S.; Aggarwal, S.; Jain, R. T-Scan a digital pathway to occlusal perfection: A review. Ann. Prosthodon. Restor. Dent. 2015, 1, 32–35. [Google Scholar]



| Extractions | Impacted Teeth | ||||
|---|---|---|---|---|---|
| No | Yes | No | Yes | ||
| Angel_class | Angle Class I | 12 | 6 | 12 | 6 |
| Angle Class II | 6 | 8 | 8 | 6 | |
| Total | 18 | 14 | 20 | 12 | |
| Type of System Comparative Indicator | Trios Intraoral Scan (3Shape System) | T-Scan Novus (Tekscan) |
|---|---|---|
| Occlusal map | Yes | Yes |
| Distance between the upper and lower jaws | Yes | No |
| Strength of the contacts | No | Yes |
| Contact distribution on each tooth (in%) | No | Yes |
| Sequence of the contacts | No | Yes |
| First contact | No | Yes |
| Maximum bite force | No | Yes |
| Maximum intercuspation | No | Yes |
| Occlusion | Virtual articulator with possible and probable movements | Video of real movements, dynamic occlusion |
| Scheme of lower jaw movement | No | Yes |
| Occlusion and disocclusion times | No | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shopova, D.; Bakova, D.; Yordanova, S.; Yordanova, M.; Uzunov, T. Digital Occlusion Analysis after Orthodontic Treatment: Capabilities of the Intraoral Scanner and T-Scan Novus System. Appl. Sci. 2023, 13, 4335. https://doi.org/10.3390/app13074335
Shopova D, Bakova D, Yordanova S, Yordanova M, Uzunov T. Digital Occlusion Analysis after Orthodontic Treatment: Capabilities of the Intraoral Scanner and T-Scan Novus System. Applied Sciences. 2023; 13(7):4335. https://doi.org/10.3390/app13074335
Chicago/Turabian StyleShopova, Dobromira, Desislava Bakova, Svetlana Yordanova, Miroslava Yordanova, and Todor Uzunov. 2023. "Digital Occlusion Analysis after Orthodontic Treatment: Capabilities of the Intraoral Scanner and T-Scan Novus System" Applied Sciences 13, no. 7: 4335. https://doi.org/10.3390/app13074335