
Feature Analysis of Predictors Affecting the Nidus Obliteration of Linear Accelerator-Based Radiosurgery for Arteriovenous Malformations Using Explainable Predictive Modeling

Abstract
:1. Introduction
2. Materials and Methods
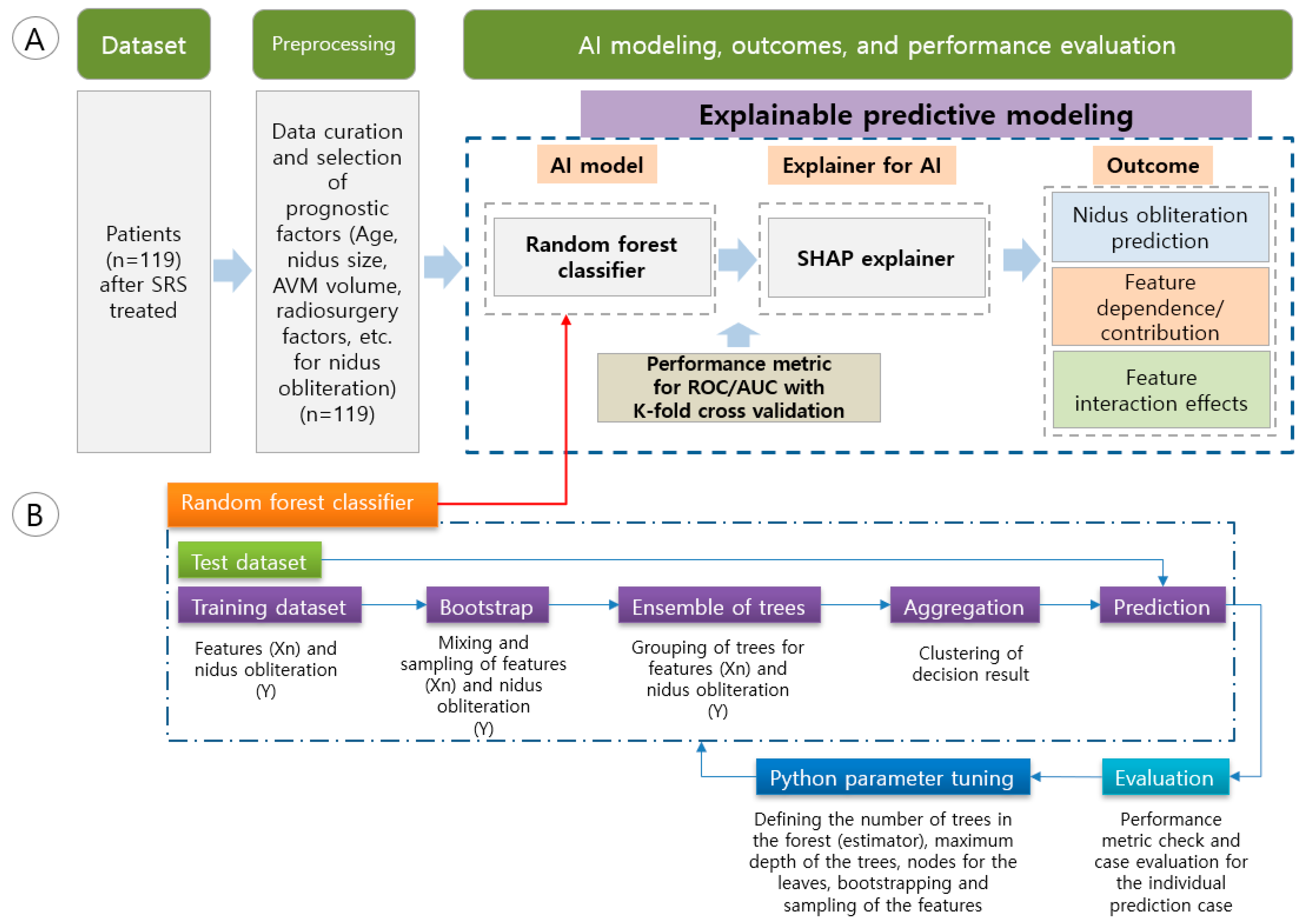
2.1. Patient Dataset
2.2. Explainable Predictive Modeling
2.3. Performance Metric and Programming Environment
3. Results
3.1. Patient Characteristics Analysis
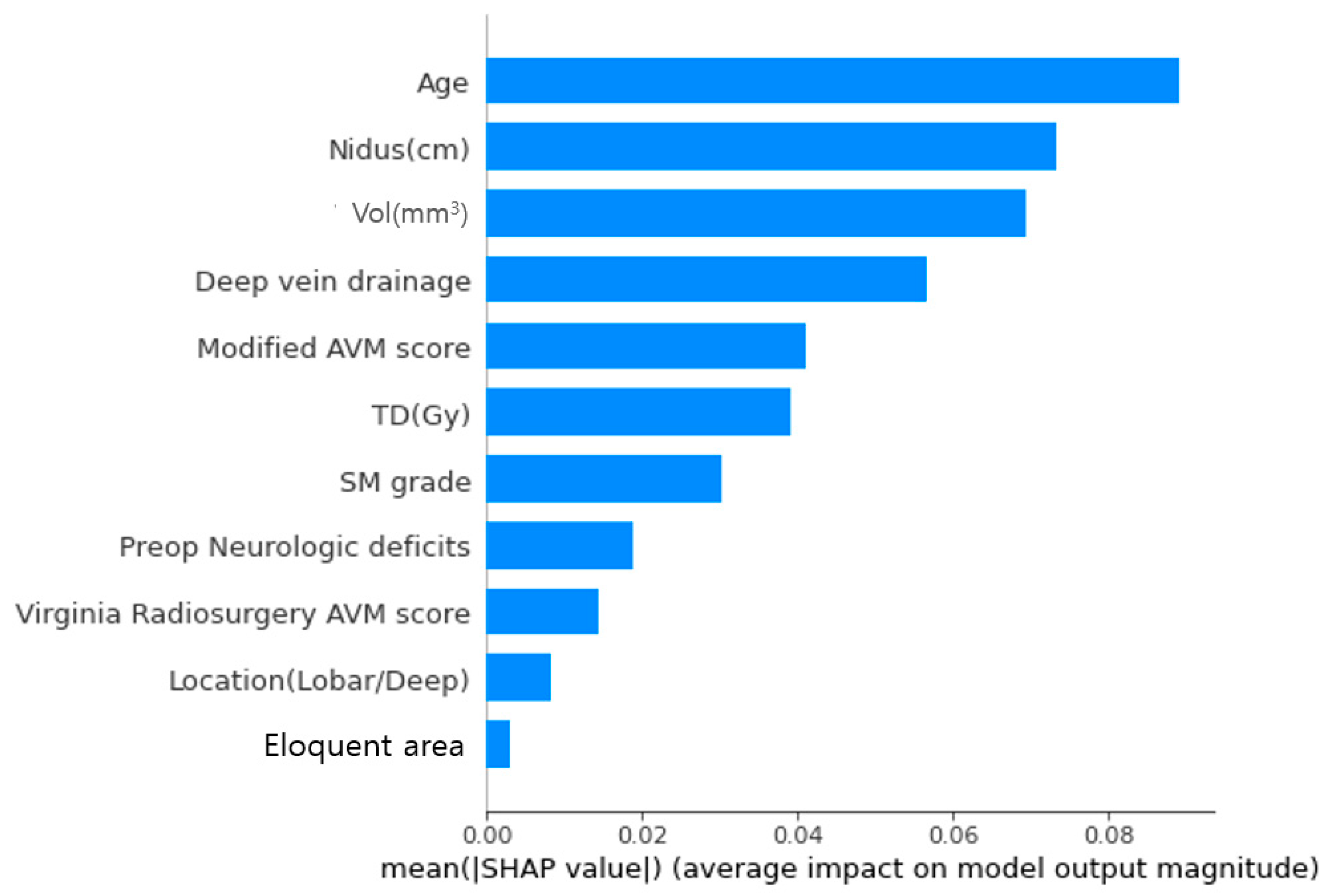
3.2. Importance of Factor Contributions to Prediction of Nidus Obliteration
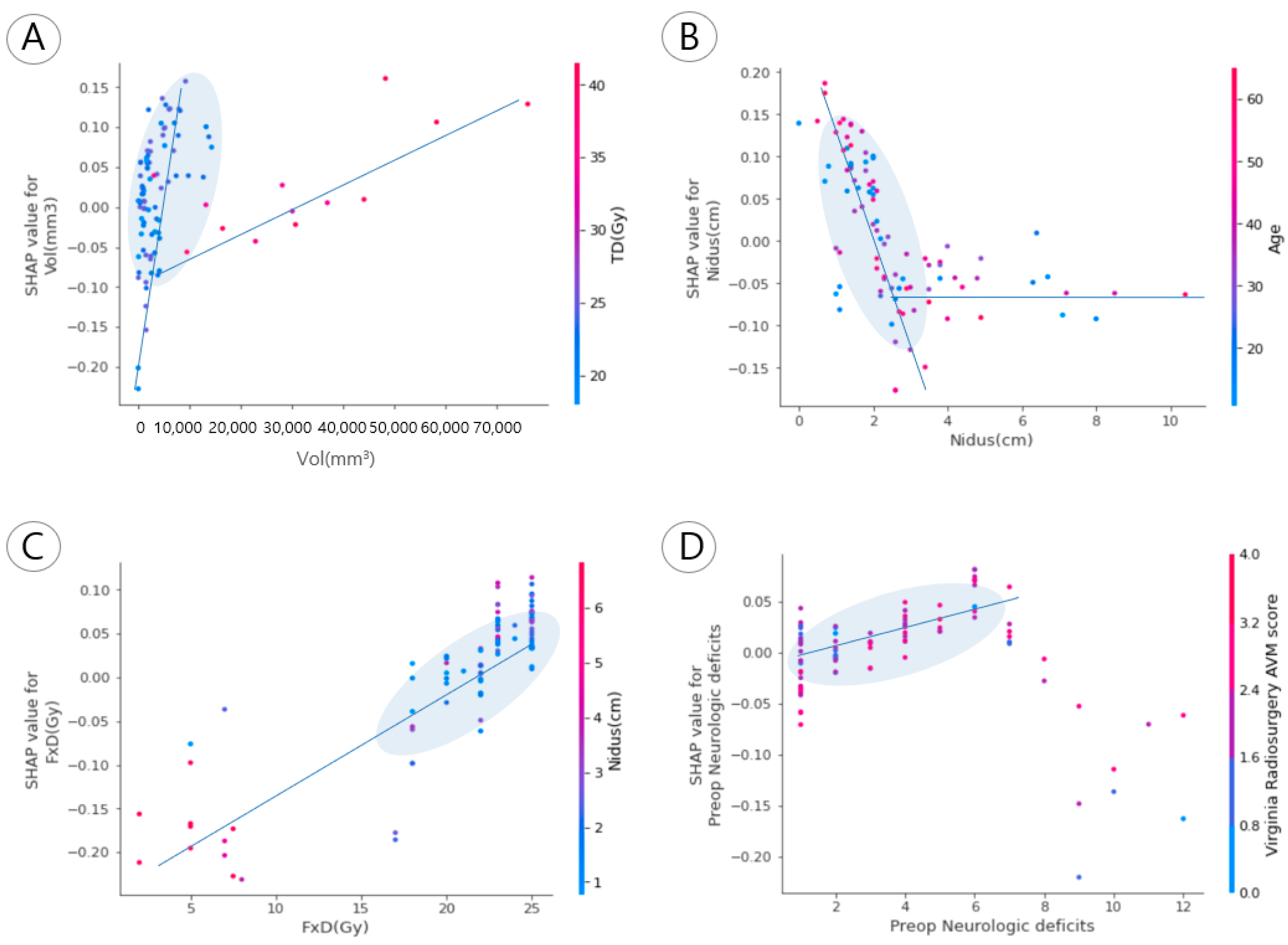
3.3. Correlations between Prognostic Factors and Nidus Obliteration
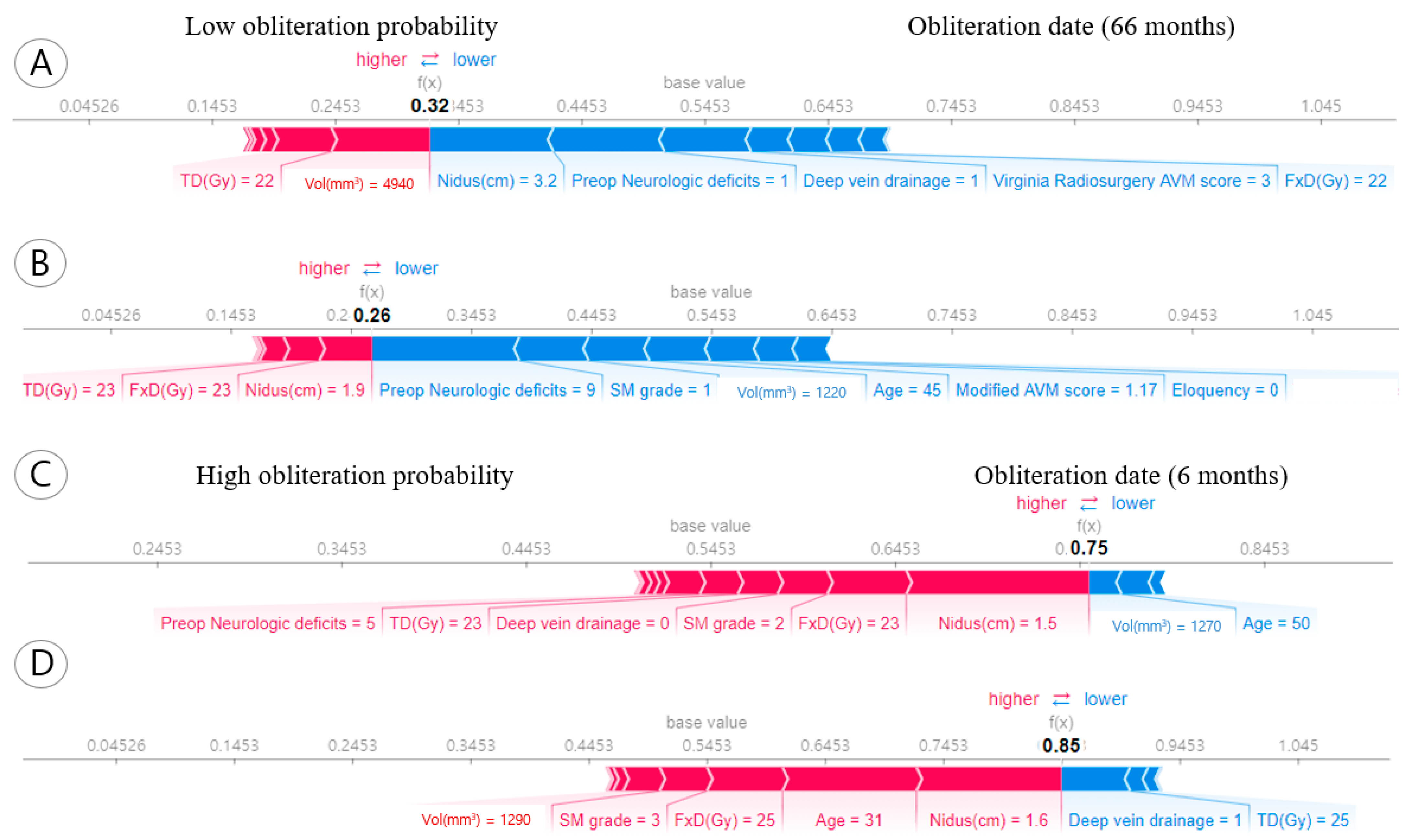
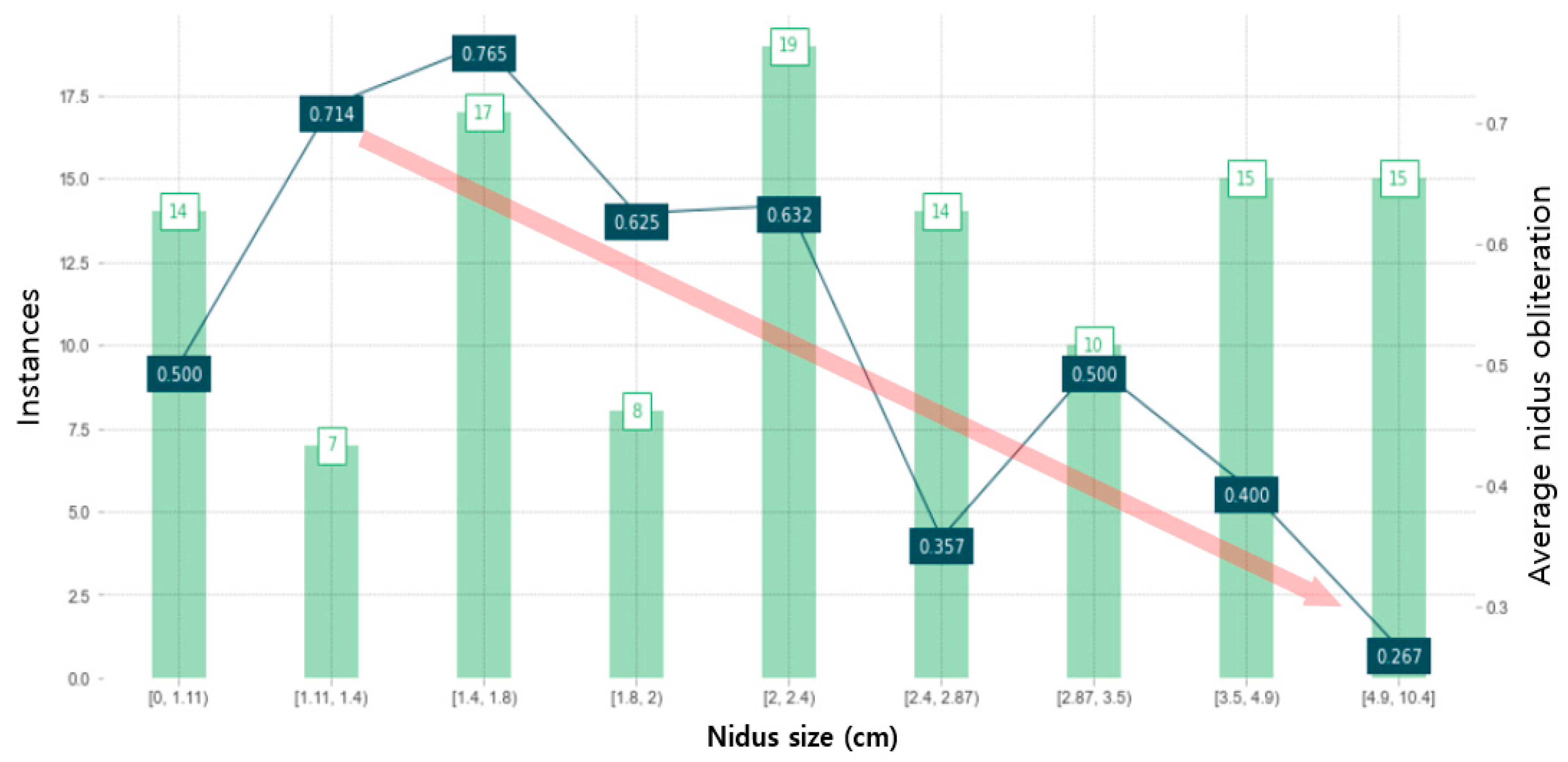
3.4. Individual Obliteration Probability of the Prognostic Factors
3.5. Partial Dependent Analysis for Nidus Obliteration
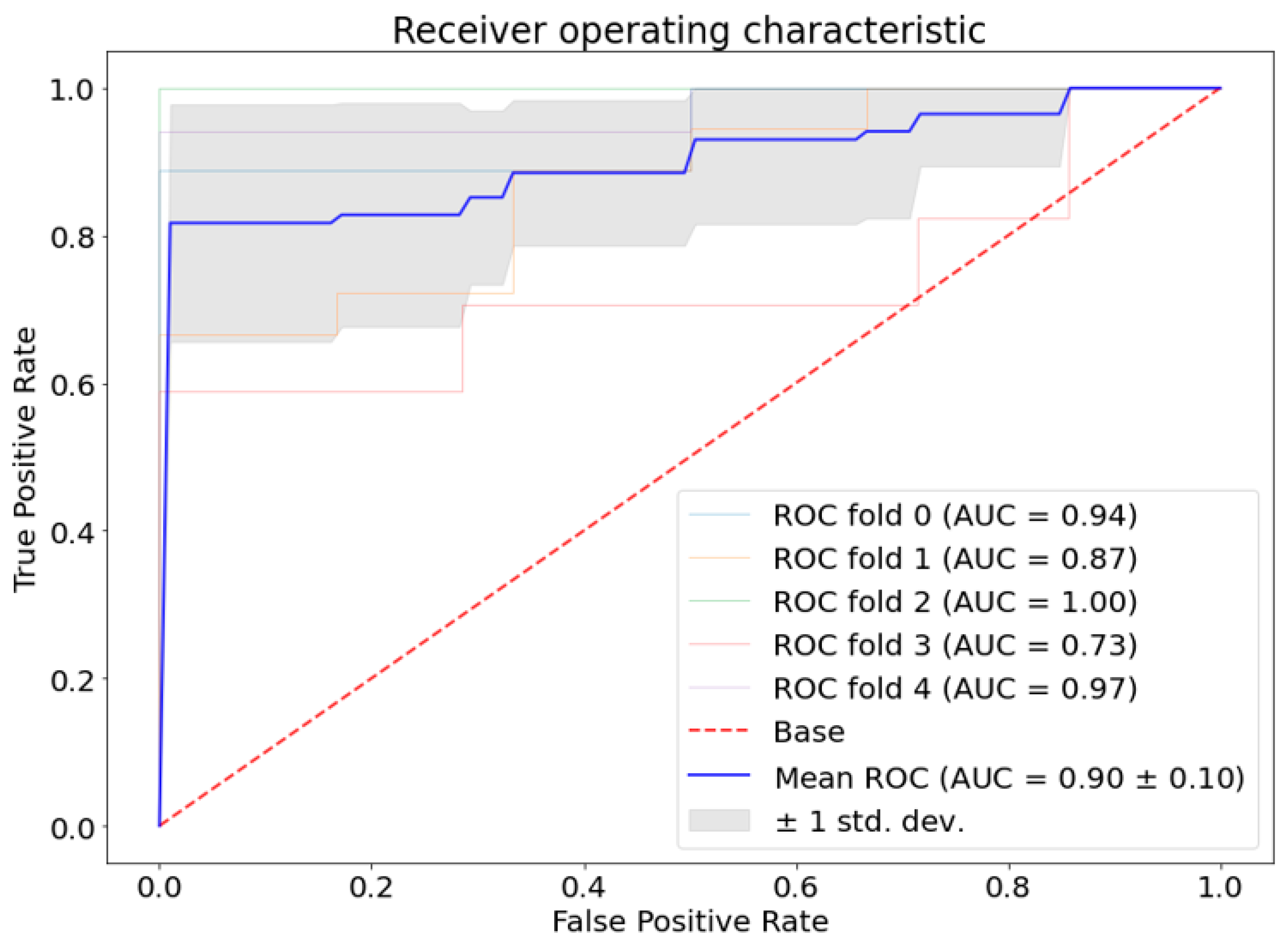
3.6. Performance Metric
4. Discussion
4.1. Prognostic Factors for Arteriovenous Malformation in Radiosurgery
4.2. Need for Explainable AI Methodology
4.3. Limitation of input Data for Machine Learning Model
4.4. Expansion of Model Selection for the Outcome Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lunsford, L.D.; Kondziolka, D.; Flickinger, J.C.; Bissonette, D.J.; Jungreis, C.A.; Maitz, A.H.; Horton, J.A.; Coffey, R.J. Stereotactic radiosurgery for arteriovenous malformations of the brain. J. Neurosurg. 1991, 75, 512–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steiner, L. Stereotaxic radiosurgery for cerebral arteriovenous malformations. Acta Chir. Scand. 1972, 138, 459–464. [Google Scholar] [PubMed]
- Daou, B.J.; Palmateer, G.; Thompson, B.G.; Maher, C.O.; Hayman, J.A.; Lam, K.L.; Wahl, D.R.; Kim, M.; Pandey, A.S. Stereotactic radiosurgery for brain arteriovenous malformations: Evaluation of obliteration and review of associated predictors. J. Stroke Cerebrovasc. Dis. 2020, 29, 104863. [Google Scholar] [CrossRef] [PubMed]
- da Costa, L.; Wallace, M.C.; Ter Brugge, K.G.; O’Kelly, C.; Willinsky, R.A.; Tymianski, M. The natural history and predictive features of hemorrhage from brain arteriovenous malformations. Stroke 2009, 40, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, A.; Pile-Spellman, J.; Stapf, C.; Sciacca, R.; Faulstich, A.; Mohr, J.; Schumacher, H.; Mast, H. Risk of endovascular treatment of brain arteriovenous malformations. Stroke 2002, 33, 1816–1820. [Google Scholar] [CrossRef]
- Sahlein, D.H.; Mora, P.; Becske, T.; Huang, P.; Jafar, J.J.; Connolly, E.S.; Nelson, P.K. Features predictive of brain arteriovenous malformation hemorrhage: Extrapolation to a physiologic model. Stroke 2014, 45, 1964–1970. [Google Scholar] [CrossRef] [Green Version]
- Stapf, C.; Mast, H.; Sciacca, R.; Choi, J.; Khaw, A.; Connolly, E.; Pile-Spellman, J.; Mohr, J. Predictors of hemorrhage in patients with untreated brain arteriovenous malformation. Neurology 2006, 66, 1350–1355. [Google Scholar] [CrossRef]
- Pollock, B.E.; Flickinger, J.C.; Lunsford, L.D.; Maitz, A.; Kondziolka, D. Factors associated with successful arteriovenous malformation radiosurgery. Neurosurgery 1998, 42, 1239–1244. [Google Scholar] [CrossRef]
- Maruyama, K.; Kondziolka, D.; Niranjan, A.; Flickinger, J.C.; Lunsford, L.D. Stereotactic radiosurgery for brainstem arteriovenous malformations: Factors affecting outcome. J. Neurosurg. 2004, 100, 407–413. [Google Scholar] [CrossRef]
- Friedman, W.A.; Bova, F.J.; Bollampally, S.; Bradshaw, P. Analysis of factors predictive of success or complications in arteriovenous malformation radiosurgery. Neurosurgery 2003, 52, 296–308. [Google Scholar] [CrossRef]
- Ding, D.; Xu, Z.; Yen, C.-P.; Starke, R.M.; Sheehan, J.P. Radiosurgery for cerebral arteriovenous malformations in elderly patients: Effect of advanced age on outcomes after intervention. World Neurosurg. 2015, 84, 795–804. [Google Scholar] [CrossRef]
- Börcek, A.Ö.; Çeltikçi, E.; Aksoğan, Y.; Rousseau, M.J. Clinical outcomes of stereotactic radiosurgery for cerebral arteriovenous malformations in pediatric patients: Systematic review and meta-analysis. Neurosurgery 2019, 85, E629–E640. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.; Maruyama, K.; Kurita, H.; Kawamoto, S.; Tago, M.; Terahara, A.; Morita, A.; Ueki, K.; Takakura, K.; Kirino, T. Analysis of nidus obliteration rates after gamma knife surgery for arteriovenous malformations based on long-term follow-up data: The University of Tokyo experience. J. Neurosurg. 2004, 101, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oermann, E.K.; Rubinsteyn, A.; Ding, D.; Mascitelli, J.; Starke, R.M.; Bederson, J.B.; Kano, H.; Lunsford, L.D.; Sheehan, J.P.; Hammerbacher, J. Using a machine learning approach to predict outcomes after radiosurgery for cerebral arteriovenous malformations. Sci. Rep. 2016, 6, 21161. [Google Scholar] [CrossRef] [Green Version]
- Meng, X.; Gao, D.; He, H.; Sun, S.; Liu, A.; Jin, H.; Li, Y. A machine learning model predicts the outcome of SRS for residual arteriovenous malformations after partial embolization: A real-world clinical obstacle. World Neurosurg. 2022, 163, e73–e82. [Google Scholar] [CrossRef] [PubMed]
- Saggi, S.; Winkler, E.A.; Ammanuel, S.G.; Morshed, R.A.; Garcia, J.H.; Young, J.S.; Semonche, A.; Fullerton, H.J.; Kim, H.; Cooke, D.L. Machine learning for predicting hemorrhage in pediatric patients with brain arteriovenous malformation. J. Neurosurg. Pediatr. 2022, 30, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Tjoa, E.; Guan, C. A survey on explainable artificial intelligence (xai): Toward medical xai. IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 4793–4813. [Google Scholar] [CrossRef]
- Arrieta, A.B.; Díaz-Rodríguez, N.; Del Ser, J.; Bennetot, A.; Tabik, S.; Barbado, A.; García, S.; Gil-López, S.; Molina, D.; Benjamins, R. Explainable Artificial Intelligence (XAI): Concepts, taxonomies, opportunities and challenges toward responsible AI. Inf. Fusion 2020, 58, 82–115. [Google Scholar] [CrossRef] [Green Version]
- Gunning, D.; Stefik, M.; Choi, J.; Miller, T.; Stumpf, S.; Yang, G.-Z. XAI—Explainable artificial intelligence. Sci. Robot. 2019, 4, eaay7120. [Google Scholar] [CrossRef] [Green Version]
- Mavroidis, P.; Theodorou, K.; Lefkopoulos, D.; Nataf, F.; Schlienger, M.; Karlsson, B.; Lax, I.; Kappas, C.; Lind, B.K.; Brahme, A. Prediction of AVM obliteration after stereotactic radiotherapy using radiobiological modelling. Phys. Med. Biol. 2002, 47, 2471. [Google Scholar] [CrossRef]
- Pollock, B.E.; Storlie, C.B.; Link, M.J.; Stafford, S.L.; Garces, Y.I.; Foote, R.L. Comparative analysis of arteriovenous malformation grading scales in predicting outcomes after stereotactic radiosurgery. J. Neurosurg. 2017, 126, 852–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheth, S.A.; Potts, M.B.; Sneed, P.K.; Young, W.L.; Cooke, D.L.; Gupta, N.; Hetts, S.W. Angiographic features help predict outcome after stereotactic radiosurgery for the treatment of pediatric arteriovenous malformations. Child Nerv. Syst. 2014, 30, 241–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senders, J.T.; Staples, P.C.; Karhade, A.V.; Zaki, M.M.; Gormley, W.B.; Broekman, M.L.; Smith, T.R.; Arnaout, O. Machine learning and neurosurgical outcome prediction: A systematic review. World Neurosurg. 2018, 109, 476–486.e471. [Google Scholar] [CrossRef]
- Rodríguez-Pérez, R.; Bajorath, J. Interpretation of machine learning models using shapley values: Application to compound potency and multi-target activity predictions. J. Comput. Aided Mol. Des. 2020, 34, 1013–1026. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Graf, E.; Schmoor, C.; Sauerbrei, W.; Schumacher, M. Assessment and comparison of prognostic classification schemes for survival data. Stat. Med. 1999, 18, 2529–2545. [Google Scholar] [CrossRef]
- Potts, M.B.; Sheth, S.A.; Louie, J.; Smyth, M.D.; Sneed, P.K.; McDermott, M.W.; Lawton, M.T.; Young, W.L.; Hetts, S.W.; Fullerton, H.J. Stereotactic radiosurgery at a low marginal dose for the treatment of pediatric arteriovenous malformations: Obliteration, complications, and functional outcomes. J. Neurosurg. Pediatr. 2014, 14, 187–200. [Google Scholar] [CrossRef] [Green Version]
- Karlsson, B.; Lax, I.; Söderman, M. Risk for hemorrhage during the 2-year latency period following gamma knife radiosurgery for arteriovenous malformations. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 1045–1051. [Google Scholar] [CrossRef]
- Ding, D.; Starke, R.M.; Kano, H.; Lee, J.Y.; Mathieu, D.; Pierce, J.; Huang, P.P.; Feliciano, C.; Rodriguez-Mercado, R.; Almodovar, L. Stereotactic radiosurgery for Spetzler-Martin Grade III arteriovenous malformations: An international multicenter study. J. Neurosurg. 2017, 126, 859–871. [Google Scholar] [CrossRef] [Green Version]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine learning in medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef]
- Alanazi, H.O.; Abdullah, A.H.; Qureshi, K.N. A critical review for developing accurate and dynamic predictive models using machine learning methods in medicine and health care. J. Med. Syst. 2017, 41, 69. [Google Scholar] [CrossRef]
- Sidey-Gibbons, J.A.; Sidey-Gibbons, C.J. Machine learning in medicine: A practical introduction. BMC Med. Res. Methodol. 2019, 19, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bzdok, D.; Krzywinski, M.; Altman, N. Machine learning: Supervised methods. Nat. Methods 2018, 15, 5. [Google Scholar] [CrossRef] [PubMed]
- Marx, V. Machine learning, practically speaking. Nat. Methods 2019, 16, 463–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raju, B.; Jumah, F.; Ashraf, O.; Narayan, V.; Gupta, G.; Sun, H.; Hilden, P.; Nanda, A. Big data, machine learning, and artificial intelligence: A field guide for neurosurgeons. J. Neurosurg. 2020, 1, 2688. [Google Scholar] [CrossRef] [PubMed]
- Celtikci, E. A systematic review on machine learning in neurosurgery: The future of decision-making in patient care. Turk. Neurosurg. 2018, 28, 167–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchlak, Q.D.; Esmaili, N.; Leveque, J.-C.; Farrokhi, F.; Bennett, C.; Piccardi, M.; Sethi, R.K. Machine learning applications to clinical decision support in neurosurgery: An artificial intelligence augmented systematic review. Neurosurg. Rev. 2020, 43, 1235–1253. [Google Scholar] [CrossRef] [Green Version]
- Staartjes, V.E.; Stumpo, V.; Kernbach, J.M.; Klukowska, A.M.; Gadjradj, P.S.; Schröder, M.L.; Veeravagu, A.; Stienen, M.N.; van Niftrik, C.H.; Serra, C. Machine learning in neurosurgery: A global survey. Acta Neurochir. 2020, 162, 3081–3091. [Google Scholar] [CrossRef]
- Cohen-Gadol, A.A.; Pollock, B.E. Radiosurgery for arteriovenous malformations in children. J. Neurosurg. Pediatr. 2006, 104, 388–391. [Google Scholar] [CrossRef]
- Riva, D.; Pantaleoni, C.; Devoti, M.; Lindquist, C.; Steiner, L.; Giorgi, C. Radiosurgery for cerebral AVMs in children and adolescents: The neurobehavioral outcome. J. Neurosurg. 1997, 86, 207–210. [Google Scholar] [CrossRef]
- Kondziolka, D.; Lunsford, D.; Flickinger, J.C. Stereotactic radiosurgery in children and adolescents. Pediatr. Neurosurg. 1990, 16, 219–221. [Google Scholar] [CrossRef] [PubMed]
- Clement-Colmou, K.; Roualdes, V.; Martin, S.-A.; Josset, S.; Desal, H.; Campion, L.; Thillays, F. Dynamic conformal arc radiosurgery for arteriovenous malformations: Outcome and influence of clinical and dosimetrical data. Radiother. Oncol. 2017, 123, 251–256. [Google Scholar] [CrossRef]
- Minniti, G.; Clarke, E.; Lanzetta, G.; Osti, M.F.; Trasimeni, G.; Bozzao, A.; Romano, A.; Enrici, R.M. Stereotactic radiosurgery for brain metastases: Analysis of outcome and risk of brain radionecrosis. Radiat. Oncol. 2011, 6, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boldrini, L.; Bibault, J.-E.; Masciocchi, C.; Shen, Y.; Bittner, M.-I. Deep learning: A review for the radiation oncologist. Front. Oncol. 2019, 9, 977. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Unit or Sub-Category | Instance (%) or Mean ± SD |
|---|---|---|
| Age | years | 34 ± 13 |
| Age ≤ 18 | years | 26 (21.85%) |
| Sex | Male | 82(68.91%) |
| Female | 37(31.09%) | |
| Previous rupture | Yes | 64 (53.78%) |
| No | 55 (46.22%) | |
| Prior embolization | Yes | 6 (5.04%) |
| No | 113 (94.96%) | |
| AVM Location | Lobar | 60 (50.42%) |
| Deep | 59 (49.58%) | |
| SM grade | 1 | 14 (11.76%) |
| 2 | 39 (32.77%) | |
| 3 | 43 (36.13%) | |
| 4 | 15 (12.61%) | |
| 5 | 8 (6.72%) | |
| Median score | 3 | |
| AVM Volume | mm3 | Mean 7163 (IQR Q1: 1190, Q3: 7140, min: 64, max: 15,600) |
| Virginia radiosurgery AVM score | 0 | 4 (3.36%) |
| 1 | 24 (20.17%) | |
| 2 | 46 (38.66%) | |
| 3 | 40 (33.61%) | |
| 4 | 5 (4.20%) | |
| Modified AVM score | Median score | 2.05 |
| Deep vein drainage | Yes | 51 (42.86%) |
| No | 68 (57.14%) | |
| FD | Gy | 20.28 ± 6.49) |
| Fx | Sx | 102 (85.71%) |
| Fx | 17 (14.29%) | |
| TD | Gy | 25.74 ± 8.58 |
| Dmax | Gy | 30.02 ± 9.83 |
| Nidus size | cm | 2.75 ± 1.78 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.H.; Sohn, M.-J. Feature Analysis of Predictors Affecting the Nidus Obliteration of Linear Accelerator-Based Radiosurgery for Arteriovenous Malformations Using Explainable Predictive Modeling. Appl. Sci. 2023, 13, 4267. https://doi.org/10.3390/app13074267
Kim KH, Sohn M-J. Feature Analysis of Predictors Affecting the Nidus Obliteration of Linear Accelerator-Based Radiosurgery for Arteriovenous Malformations Using Explainable Predictive Modeling. Applied Sciences. 2023; 13(7):4267. https://doi.org/10.3390/app13074267
Chicago/Turabian StyleKim, Kwang Hyeon, and Moon-Jun Sohn. 2023. "Feature Analysis of Predictors Affecting the Nidus Obliteration of Linear Accelerator-Based Radiosurgery for Arteriovenous Malformations Using Explainable Predictive Modeling" Applied Sciences 13, no. 7: 4267. https://doi.org/10.3390/app13074267